
Abstract
Background
Reducing delays along the acute stroke pathway significantly improves clinical outcomes for acute ischemic stroke patients eligible for reperfusion treatments. The economic impact of different strategies reducing onset to treatment (OTT) is crucial information for stakeholders in acute stroke management. This systematic review aimed to provide an overview on the cost-effectiveness of several strategies to reduce OTT.
Methods
A comprehensive literature search was conducted in EMBASE, PubMed, and Web of Science until January 2022. Studies were included if they reported 1/ stroke patients treated with intravenous thrombolysis and/or endovascular thrombectomy, 2/ full economic evaluation, and 3/ strategies to reduce OTT. The Consolidated Health Economic Evaluation Reporting Standards statement was applied to assess the reporting quality.
Results
Twenty studies met the inclusion criteria, of which thirteen were based on cost-utility analysis with the incremental cost-effectiveness ratio per quality-adjusted life year gained as the primary outcome. Studies were performed in twelve countries focusing on four main strategies: educational interventions, organizational models, healthcare delivery infrastructure, and workflow improvements. Sixteen studies showed that the strategies concerning educational interventions, telemedicine between hospitals, mobile stroke units, and workflow improvements, were cost-effective in different settings. The healthcare perspective was predominantly used, and the most common types of models were decision trees, Markov models and simulation models. Overall, fourteen studies were rated as having high reporting quality (79%-94%).
Conclusions
A wide range of strategies aimed at reducing OTT is cost-effective in acute stroke care treatment. Existing pathways and local characteristics need to be taken along in assessing proposed improvements.
Similar content being viewed by others


Background
Worldwide, stroke is the second leading cause of death and the most common cause of permanent disability, resulting in huge societal and economic burdens related to long-term care, rehabilitation, and productivity loss [1, 2]. Acute ischemic stroke (AIS) represents the majority of stroke patients, and reperfusion treatments like intravenous thrombolysis (IVT) and endovascular thrombectomy (EVT) have shown to be effective in improving functional outcomes. Both treatments are highly time-dependent, with IVT effective up to 4.5 h after symptom onset and EVT within 6 h [3, 4]. For selected patients suspected of a large vessel occlusion (LVO), EVT has shown to be effective even up to 24 h [5]. Importantly, shorter time from onset to treatment (OTT) with IVT or EVT is associated with better functional outcomes [6,7,8].
Due to the time dependency of reperfusion treatments, multiple strategies or interventions have been proposed to reduce time delays along the acute stroke pathway. Examples include educational interventions to create awareness among citizens to contact emergency services immediately following symptom onset [9], a mobile stroke unit that brings IVT to the patient instead of transporting the patients to the nearest IVT capable facility [9], telemedicine solutions for expert opinion at a distance [10], and workflow improvements including inter-hospital patients transfer, teamwork and feedback on performance [9, 11]. In addition, direct transport of acute stroke patients suspected of LVO from the onset scene to a comprehensive stroke center based on prehospital triage instruments [12] is a promising alternative organizational model, which could decrease the OTT time for patients eligible for EVT [13].
While several strategies have been developed to reduce time to reperfusion treatments, less is known about their cost-effectiveness. As stroke incidence and its burden on society are expected to increase [14], evidence generated by economic evaluations of these strategies will support policymakers, clinicians, and other stakeholders in deciding how to allocate scarce resources whilst optimizing clinical outcomes for patients. Therefore, the aim of this study is to systematically review the cost-effectiveness of strategies directed at reducing time to reperfusion treatments for AIS patients.
Methods
Search strategy and study selection
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [15]. The search strategy was constructed by the first two authors (C.P.N. and W.J.M). Three electronic databases (EMBASE, MEDLINE/ Pubmed, and Web of Science) were searched to identify relevant articles published between January 2010 to January 2022. The search strategy was based on the PICOS format: The population (P) were ‘stroke’ patients, the intervention (I) ‘EVT or IVT’ and ‘reducing time-to-treatment’, and the outcome (O) was ‘incremental cost-effectiveness ratio’ (ICER). Comparators (C) and study design (S) were not included to maximize records retrieved. Our eligibility criteria were: (1) stroke patients treated with IVT and/or EVT, (2) full economic evaluation was performed (i.e., cost-effectiveness, cost-utility, or cost–benefit analysis), and (3) strategies or interventions that aim to reduce time to treatment or increasing the proportion of eligible patients for treatment due to time delay reduction. Papers were excluded if: (1) articles published before 2010; (2) articles not written in English, and (3) reviews, protocol papers, conference abstracts, letters to editors, or case reports. All identified records from three databases were stored in Endnote® X8 software [16]. Details of the search strategy are reported in the Supplementary Information (Appendix 1). In addition, a manual cross-reference of selected papers was performed to include more relevant papers.
Study selection, data extraction, and quality assessment were performed independently by two reviewers (C.P.N. and W.J.M.). Disagreements were discussed between reviewers until a consensus was reached. Discrepancies were resolved by consulting a third reviewer (M.M.H.L.).
Data extraction and analysis
The following information was extracted from the selected papers independently by two reviewers (C.P.N. and W.J.M): country of origin, strategies including intervention, comparator, type of economic evaluation, effectiveness measurement, model type (i.e. Markov model, decision tree or other), economic perspective, time horizon, discount rate, reference year of cost, outcomes including incremental costs, incremental effectiveness and an ICER. An economic evaluation was stratified by type of strategy or intervention and compared with the same effectiveness measurement. An ICER was calculated by dividing the different costs by the different effectiveness of two strategies. The strategy or intervention was considered cost-effective if an ICER was less than the willingness-to-pay threshold mentioned in the study. In case specific willingness-to-pay thresholds were not stated in the study, the recommended threshold of one Gross Domestic Product (GDP) per capita was used according to the World Health Organization for cost-effectiveness studies [17]. The strategy or intervention was dominant if the strategy resulted in higher effectiveness (i.e., QALY) and less costs than the comparator. In case data were insufficient or unclear for data analysis, additional information was requested by contacting the corresponding author of individual papers.
Quality assessment
For quality assessment, the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) guideline [18] was used, scoring a total of 24 criteria. Papers were classified into three categories: high (75.0% or more), medium (from 50.0% to 74.9%) and low quality (less than 50.0%) [19, 20].
Results
Study selection
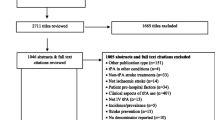
The initial literature search resulted in 1,790 records (Fig. 1). After removing duplicates, 1,294 articles were screened on title and abstract independently by both reviewers, and 36 articles were considered relevant for the full-text review. Of these articles, 18 articles were excluded because of missing outcome measures (n = 1), missing time to treatment variables (n = 13), missing full economic evaluation (n = 2) and data duplication between articles (n = 2). Two additional articles were identified when an additional search in Pubmed, EMBASE, and Web of Science was conducted until January 9th 2022. Ultimately, 20 studies were included.

PRISMA flow chart
Study characteristics
The majority of economic evaluations were conducted in high-income countries, and only one study was performed in an upper-middle-income country (China) [21]. Five studies were based in the United States [22,23,24,25,26], one study in Canada [27], 10 studies in Europe [28,29,30,31,32,33,34,35,36,37], one study in Japan [38], one study in Singapore [39], and one study in Australia [40]. The type of interventions varied across studies, including educational interventions [23, 34, 39], organizational models [22, 24,25,26,27, 30,31,32, 36, 38, 40], healthcare delivery infrastructure [29, 33, 35], and workflow improvement [28, 34]. An overview of all study characteristics is provided in Table 1.
The majority of studies applied cost-utility analysis (n = 14) with quality-adjusted life year (QALY) (n = 13) [21,22,23, 26,27,28,29,30, 32, 34, 36, 38, 39] and disability-adjusted life year (DALY) (n = 1) [40] as the primary outcome of effectiveness. Two studies reported cost-effectiveness based on the IVT rate [29, 30], one study based on the number of home discharges [20], one study based on three outcome variables, including the IVT rate within three hours from symptom onset, OTT time, and door-to-needle time [25], and one study based on door-to-needle time, and death averted [37]. One study analyzed the cost–benefit of the used strategy [31].
Most economic evaluations conducted a model-based approach, while two studies were trial-based analyses [32, 37]. Simulation modeling was applied in six studies [25, 29, 30, 33, 38, 40], decision tree analytic modeling was used in four studies [24, 26, 34, 35], the use of a decision tree and a Markov model was adopted in four studies [21, 27, 28, 36], and two studies used a Markov model [22, 23]. Additionally, one study used a population-level systems dynamics model [39], and one study did not report a clear model [31].
Economic evaluations were analyzed from various perspectives containing a healthcare payer or payer perspective (n = 7) [26, 27, 29, 32, 36, 37, 39], a hospital or healthcare provider perspective (n = 3) [24, 35, 40], a national health service viewpoint (n = 2) [28, 34], a societal perspective (n = 3) [21,22,23], a policy maker viewpoint (n = 1) [33] and a government perspective (n = 1) [38]. Hence, most of studies included medical service costs, such as ambulance transportation, hospitalization, outpatient visits, rehabilitation, and long-term care. However, only two studies with a societal perspective reported indirect costs (productivity loss) [21, 23]. In three studies, no perspective was mentioned. One study included health care costs (ambulance service, treatment costs, bed day, nursing home, residential care home, assisted living facility, and carer visiting) [30], and two studies considered intervention costs and costs of different functional status after stroke [25, 31].
Time horizons ranged from 90 days to a lifetime. Seven studies used a 5-year horizon [23, 24, 29, 30, 32, 37, 40], and six studies employed a lifetime perspective [22, 25, 27, 28, 34, 36]. A ninety-day horizon was used in one study [26]. Discount rates were reported in 13 studies ranging from 1.5% to 5.0% [21,22,23,24,25, 27, 28, 32, 34, 36, 38,39,40]. Seven studies did not report any discount rate. Of those, the discount rate was not applicable for three studies due to a short time horizon of 90 days or 12 months [26, 31, 35].
Quality of studies
Total CHEERS scores, along with percentage scores of included studies, are presented in Table 2. Fourteen studies were assessed as high quality (ranging from 79.2% to 93.8%) and six studies as medium quality (ranging from 66.7% to 72.9%). There were no studies that were assessed as low quality. The assessment on each item of the CHEERS statement is described in the Supplementary Information (Fig. S1).
Results of economic evaluation
Included studies were categorized into four main groups based on the type of interventions: (1) educational interventions, (2) organizational models, (3) healthcare delivery infrastructure, and (4) workflow improvements (see Table 3).
Educational interventions
Three studies assessed the cost-utility of educational interventions to reduce time delays to treatment in AIS patients [23, 34, 39]. Topics varied across studies, including public campaigns, interactive interventions for patients (i.e. educational materials, medical alert bracelets, and in-hospital interactive group sessions), and training staff of general practitioner offices. Irrespective of the type of intervention, all educational interventions were cost-effective as their ICERs were lower than the willingness-to-pay thresholds. One study even demonstrated that educational interventions for both health staff and patients were dominant compared to current practice (higher QALY gained (1.14- 2.26 QALYs) and saving $16,153- $32,305) [34].
Organizational models
Over half of the selected studies (12/20) performed economic evaluations on organizational models. Different strategies were considered, including studies on telemedicine solutions between stroke centers and community hospitals [21, 22, 24,25,26], in-ambulance telemedicine [36], mobile stroke units [31, 32, 40], a combination of mothership model and drip-and-ship model with alternative transportation modes (ground or air) [27], prehospital redirection of patients to regional IVT center instead of local stroke units [30], and a mobile interventionist [38]. Most of these studies (11 out of 12) reported that interventions were cost-effective or dominant (higher QALY gained and saving costs) [22, 24,25,26,27, 30,31,32, 36, 40]. However, one Japanese study reporting on the use of a mobile interventionist showed that this approach was only cost-effective in a specific region (i.e. Kamikawachubu area in Hokkaido). In Hokkaido, the ICER of mobile interventionists was higher than the threshold of $48,146 in other areas [38].
Healthcare delivery infrastructure
Three economic evaluations reported interventions related to the regional healthcare delivery infrastructure for acute stroke care, such as introducing new EVT centers [29], upgrading hospitals to IVT-capable stroke care centers [33, 35] and centralization of acute stroke care treatment [33]. Effectiveness was measured as the percentage of the IVT rate in two studies. Within these studies, the ICER ranged from $56 to $660 per one percentage increase in the IVT rate [33, 35]. One study showed that adding new EVT-capable centers in their region gained an additional 213 QALYs and saved £2,870,000 compared to the current situation [29].
Workflow improvement
Three studies assessed economic evaluations of workflow improvements [28, 34, 37]. Implementing a quality improvement project, including streamlining stroke care pathway and simulation-based training, produced an additional $29 per minute door-to-needle time reduction and $10,543 per death averted [37]. One study evaluated inter-hospital transfer by helicopter emergency medical service compared to ground emergency medical service, which appeared cost-effective at the threshold of £30,000 per QALY [28]. Another study demonstrated that an immediate computed tomography (CT) scan strategy, in which the CT scanner was moved closer to the emergency department, was dominant when compared to current practice [34].
The ICERs of studies reporting QALYs (n = 13) [21,22,23, 26,27,28,29,30, 32, 34, 36, 38, 39] were assessed as a proportion of country GDP per capita (Fig. 2). Cross-study analysis indicated that the strategies of educational interventions, organizational models, healthcare delivery infrastructure, and workflow improvement were highly cost-effective with the ICER less than one times GDP per capita (ranging from -1.58 to 0.85 times GDP per capita) in 11 studies. Stevens et al. showed that the educational interventions in the US exceeded one times GDP (1.05 to 1.49 times GDP per capita). However, organizational models in Japan were not considered cost-effective in most of regions with the ICERs ranging from 2.25 to 40.89 times GDP per capita.

ICERs compared to country GDP per capita
Three studies had more than 1 intervention (3 interventions in Bayer’s study, 2 interventions in Stevens’ study, 3 interventions in Ramos’ study); 1 intervention in 7 regions in Morii’s study. ICER: incremental cost-effectiveness ratio.
The majority of included studies (18/20) performed sensitivity analysis. Of these studies, probabilistic sensitivity analysis was conducted in seven studies. More information on the sensitivity analyses is summarized in the Supplementary Information (Table 1).
Discussion
Principal findings
To our knowledge, this is the first systematic review on the cost-effectiveness of strategies aimed to reduce OTT time for AIS patients. Twenty studies met the eligibility criteria and were included in this systematic review. Based on factors associated with time reductions along the acute stroke care pathway [9, 11, 44], we categorized strategies into four groups: educational interventions, organizational models, healthcare delivery infrastructure and workflow improvements. The results of this review demonstrate that all intervention types may be cost-effective or even dominant when compared with current stroke care practices [21,22,23,24,25,26,27,28,29, 31, 34, 36, 39, 40]. Two studies in ‘organizational model’ category [30, 32], in which the willingness to pay threshold was not stated, were deemed cost-effective if the threshold of one GDP per capita was applied [17]. Accordingly, these strategies should be considered as interventions to optimize acute stroke care systems, as they improve functional outcomes for AIS patients and reduce long-term costs of disability after stroke. However, some improvement approaches might be region-specific, as Morii et al. [38] found that a mobile interventionist strategy was cost-effective in only one area (i.e. Kamikawahokubu) while not feasible in other areas due to the close distance between the hub and spoke centers and a relatively low incidence of LVO patients. We could not conclude whether interventions were cost-effective for two studies [33, 35] in the category ‘healthcare delivery infrastructure’ and for one study [37] in the category ‘workflow improvement’ because the primary outcome was not measured in QALYs. In addition, cross-study analysis of studies reporting QALYs showed that all intervention types were highly cost-effective in most of countries (11/13 studies).
In our review, 70% of included studies were classified as high quality based on the CHEERS score. The majority of the studies referred to a cost-utility analysis, in which the study design (i.e. the perspective, time horizon, and models) differed across studies. However, most of studies (16/20) showed that strategies aimed at reducing the OTT time were cost-effective. Although strategies were categorized into four groups, classifying articles was not straightforward because various strategies were simultaneously considered in economic evaluations. For example, Penaloza-Ramos et al. conducted health economic evaluations of seven strategies simultaneously, including health staff training (in the ‘educational intervention’ category) and timely CT scan (in the ‘workflow improvement’ category) [34]. Bayer et al. performed the cost-effectiveness analysis of combining a public information campaign with five other interventions, such as IVT and EVT treatment in the acute stroke unit, out-of-hospital rehabilitation, and secondary prevention. The results showed that combining interventions was the most cost-effective strategy [39].
Policy relevance
Incorporating the cost-effectiveness evidence, apart from the current set-up of regional stroke services, other local factors need to be taken into account before intervening in regional stroke care pathways, such as the incidence of stroke, population density, and geographic location of stroke centers. From a variety of possible improvement strategies, policymakers and other stakeholders will have to identify the ones most favorable in terms of effects and cost implications. For example, the mobile interventionist strategy is cost-effective in the specific area with a high incidence of LVO, more than three-hour travel for patients to a hub (intervention) center, and within one-hour travel for interventionists [38]. Furthermore, Yan et al. identified the optimal strategy in delivering EVT, as the combination of both mothership model and drip-and-ship model based on the geographical location of stroke onset and stroke centers [27]. As such, it can be inferred that multiple organizational models need to be considered in stroke management according to local characteristics.
Strengths and limitations
The strength of our systematic review is in its wide scope, providing a broad range of various strategies to reduce time delay compared with focusing on one or more specific interventions. Additionally, all types of full economic evaluations, with both trial- and model-based analysis, were included in this review. Furthermore, it provides an informative synthesis of the cost-effectiveness evidence for all strategies, enabling better-informed decisions in stroke care, especially in the context of constrained health resources and the ageing population.
Nevertheless, several limitations in the review should be noted. Firstly, direct comparison between strategies was not possible due to heterogeneity across studies, such as setting, effectiveness outcomes, and comparators. Therefore, a ranking and assessment could not be offered. The latter would be difficult, as generic weighing and balancing are impractical without taking region-specific characteristics of the local setting into account. Instead, we offer a narrative synthesis which will help local policymakers to consider their individual options. Another limitation is to include only English papers in the present systematic review. However, no language restriction was applied in our search strategy, and screening title and abstract revealed that non-English articles also met other exclusion criteria. Finally, the results of this review were based on published studies only, thus potentially leading to publication bias.
Future perspective and recommendation
Our study demonstrates the cost-effectiveness of various strategies aiming at reducing OTT, but other organizational strategies are currently lacking a cost-effectiveness perspective. For example, the use of prehospital triage tools to transfer stroke patients directly to the appropriate target hospitals [45] or workflow improvements in which suspected LVO patients are directly transferred to the angiography suite [46] may be efficient solutions to further reduce time delays to EVT initiation. This emphasizes the need of economic evaluations for these strategies.
There is also a notable gap persisting in the cost-effectiveness analysis of strategies reducing OTT time in low- or middle-income countries. In such settings policymakers and health care providers are possibly in the phase of building infrastructure without the opportunity to consider alternative organizational set-ups (i.e. mobile stroke unit, mobile interventionist) [47]. Although stroke remains a major cause of death and disability worldwide, stroke incidence and mortality rates recently have shown to decline in high-income countries due to improvements in primary and secondary prevention as well as in acute reperfusion treatments [48]. However, the trend in low- and middle-income countries is the opposite, resulting in a significant stroke burden in these regions [49]. Given the concerning shift in stroke epidemiology to low- or middle-income countries, important choices lie ahead, even when considering the very basic infrastructure.
Current economic evaluations use healthcare or payer perspectives that do not include indirect costs of post-stroke, such as productivity loss and informal caregiving for stroke patients. However, indirect costs of post-stroke account for approximately 33% of the total economic burden of stroke [50]. There is a remarkable increase worldwide in stroke incidence among younger groups (i.e. less than 65 years old) [51], which is likely to increase the indirect cost of stroke burden. Hence, future studies need to take into account the lack of evidence of societal perspective, and in low-and middle-income countries.
Conclusions
The results of this systematic review show that reported strategies reducing time delay in stroke care services are mostly cost-effective across different settings. While the findings from this review provide mainly positive results, local characteristics and background of regional health care systems should be taken into account.
All authors were involved with the conception and study design. Chi Phuong Nguyen and Willemijn J Maas performed screening records, data extraction, and data analysis. Maarten M H Lahr was the third reviewer. Chi Phuong Nguyen outlined the manuscript. Chi Phuong Nguyen and Willemijn J Maas drafted the manuscript. All authors critically reviewed the entire manuscript and approved the final submission.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Abbreviations
- AIS:
-
Acute ischemic stroke
- CHEERS:
-
Consolidated Health Economic Evaluation Reporting Standards
- DALY:
-
Disability-adjusted life year
- EVT:
-
Endovascular thrombectomy
- GDP:
-
Gross Domestic Product
- ICER:
-
Incremental cost-effectiveness ratio
- IVT:
-
Intravenous thrombolysis
- LVO:
-
Large vessel occlusion
- OTT:
-
Onset to treatment
- QALY:
-
Quality-adjusted life year
References
Krishnamurthi RV, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the global burden of disease study 2017. Neuroepidemiology. 2020;54(2):171–9.
Rajsic S, Gothe H, Borba HH, Sroczynski G, Vujicic J, Toell T, Siebert U. Economic burden of stroke: a systematic review on post-stroke care. Eur J Health Econ : HEPAC : Health Econ Prev Care. 2019;20(1):107–34.
Herpich F, Rincon F. Management of acute ischemic stroke. Crit Care Med. 2020;48(11):1654–63.
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, et al. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. 2018;49(3):e46–110.
Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, Yavagal DR, Ribo M, Cognard C, Hanel RA, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018;378(1):11–21.
Goyal M, Almekhlafi M, Dippel DW, Campbell BCV, Muir K, Demchuk AM, Bracard S, Davalos A, Guillemin F, Jovin TG, et al. Rapid alteplase administration improves functional outcomes in patients with stroke due to large vessel occlusions. Stroke. 2019;50(3):645–51.
Saver JL, Fonarow GC, Smith EE, Reeves MJ, Grau-Sepulveda MV, Pan W, Olson DM, Hernandez AF, Peterson ED, Schwamm LH. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 2013;309(23):2480–8.
Kunz WG, Hunink MG, Almekhlafi MA, Menon BK, Saver JL, Dippel DWJ, Majoie C, Jovin TG, Davalos A, Bracard S, et al. Public health and cost consequences of time delays to thrombectomy for acute ischemic stroke. Neurology. 2020;95(18):e2465–75.
Sharobeam A, Jones B, Walton-Sonda D, Lueck CJ. Factors delaying intravenous thrombolytic therapy in acute ischaemic stroke: a systematic review of the literature. J Neurol. 2021;268(8):2723–34.
Lazarus G, Permana AP, Nugroho SW, Audrey J, Wijaya DN, Widyahening IS. Telestroke strategies to enhance acute stroke management in rural settings: a systematic review and meta-analysis. Brain Behav. 2020;10(10): e01787.
Janssen PM, Venema E, Dippel DWJ. Effect of workflow improvements in endovascular stroke treatment. Stroke. 2019;50(3):665–74.
Duvekot MHC, Venema E, Rozeman AD, Moudrous W, Vermeij FH, Biekart M, Lingsma HF, Maasland L, Wijnhoud AD, Mulder L, et al. Comparison of eight prehospital stroke scales to detect intracranial large-vessel occlusion in suspected stroke (PRESTO): a prospective observational study. Lancet Neurol. 2021;20(3):213–21.
Cabal M, Machova L, Vaclavik D, Jasso P, Holes D, Volny O, Bar M. New prehospital triage for stroke patients significantly reduces transport time of EVT patients without delaying IVT. Front Neurol. 2021;12: 676126.
Wafa HA, Wolfe CDA, Emmett E, Roth GA, Johnson CO, Wang Y. Burden of stroke in Europe: thirty-year projections of incidence, prevalence, deaths, and disability-adjusted life years. Stroke. 2020;51(8):2418–27.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clinical research ed). 2021;372: n71.
EnNoteTM X8 Research Smarter. Quick reference guide for Windows. Clarivate Analytics; 2016. https://endnote.com/wp-content/uploads/m/pdf/en-x8-qrg-windows.pdf.
WHO. Commission on Macroeconomics Health, World Health, Organization. Macroeconomics and health: investing in health for economic development: executive summary/ report of 10.1186/s12913-023-09310-0 the Commission on Macroeconomics and Health. Geneva: World Health Organization; 2021. https://apps.who.int/iris/handle/10665/42463. Accessed 10 Jan 2021.
Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, Augustovski F, Briggs AH, Mauskopf J, Loder E. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)–explanation and elaboration: a report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health : J Int Soc Pharmacoeconomics Outcomes Res. 2013;16(2):231–50.
Mangham-Jefferies L, Pitt C, Cousens S, Mills A, Schellenberg J. Cost-effectiveness of strategies to improve the utilization and provision of maternal and newborn health care in low-income and lower-middle-income countries: a systematic review. BMC Pregnancy Childbirth. 2014;14:243.
Yuniar P, Robinson S, Moorin R, Norman R. Economic evaluation of breast cancer early detection strategies in Asia: a systematic review. Value Health Regional Issues. 2020;21:252–63.
Tan E, Gao L, Tran HN, Cadilhac D, Bladin C, Moodie M. Telestroke for acute ischaemic stroke: A systematic review of economic evaluations and a de novo cost-utility analysis for a middle income country. J Telemed Telecare 2021:1357633x211032407.
Demaerschalk BM, Switzer JA, Xie J, Fan L, Villa KF, Wu EQ. Cost utility of hub-and-spoke telestroke networks from societal perspective. Am J Manag Care. 2013;19(12):976–85.
Stevens ER, Roberts E, Kuczynski HC, Boden-Albala B. Stroke Warning Information and Faster Treatment (SWIFT): cost-effectiveness of a stroke preparedness intervention. Value Health : J Int Soc Pharmacoeconomics Outcomes Res. 2019;22(11):1240–7.
Switzer JA, Demaerschalk BM, Xie J, Fan L, Villa KF, Wu EQ. Cost-effectiveness of hub-and-spoke telestroke networks for the management of acute ischemic stroke from the hospitals’ perspectives. Circ Cardiovasc Qual Outcomes. 2013;6(1):18–26.
Torabi E, Froehle CM, Lindsell CJ, Moomaw CJ, Kanter D, Kleindorfer D, Adeoye O. Monte Carlo simulation modeling of a regional stroke team’s use of telemedicine. Acad Emerg Med Off J Soc Acad Emerg Med. 2016;23(1):55–62.
Whetten J, van der Goes DN, Tran H, Moffett M, Semper C, Yonas H. Cost-effectiveness of Access to Critical Cerebral Emergency Support Services (ACCESS): a neuro-emergent telemedicine consultation program. J Med Econ. 2018;21(4):398–405.
Yan C, Zheng Y, Hill MD, Mann B, Jeerakathil T, Kamal N, Amlani S, Chuck AW. Health technology optimization analysis: conceptual approach and illustrative application. MDM Pol Pract. 2018;3(1):2381468318774804.
Coughlan D, McMeekin P, Flynn D, Ford GA, Lumley H, Burgess D, Balami J, Mawson A, Craig D, Rice S, et al. Secondary transfer of emergency stroke patients eligible for mechanical thrombectomy by air in rural England: economic evaluation and considerations. Emerg Med J : EMJ. 2021;38(1):33–9.
McMeekin P, Flynn D, Allen M, Coughlan D, Ford GA, Lumley H, Balami JS, James MA, Stein K, Burgess D, et al. Estimating the effectiveness and cost-effectiveness of establishing additional endovascular Thrombectomy stroke Centres in England: a discrete event simulation. BMC Health Serv Res. 2019;19(1):821.
McMeekin P, Gray J, Ford GA, Rodgers H, Price CI. Modelling the efficiency of local versus central provision of intravenous thrombolysis after acute ischemic stroke. Stroke. 2013;44(11):3114–9.
Dietrich M, Walter S, Ragoschke-Schumm A, Helwig S, Levine S, Balucani C, Lesmeister M, Haass A, Liu Y, Lossius HM, et al. Is prehospital treatment of acute stroke too expensive? An economic evaluation based on the first trial. Cerebrovasc Dis (Basel, Switzerland). 2014;38(6):457–63.
Gyrd-Hansen D, Olsen KR, Bollweg K, Kronborg C, Ebinger M, Audebert HJ. Cost-effectiveness estimate of prehospital thrombolysis: results of the PHANTOM-S study. Neurology. 2015;84(11):1090–7.
Lahr MM, van der Zee DJ, Luijckx GJ, Vroomen PC, Buskens E. Centralising and optimising decentralised stroke care systems: a simulation study on short-term costs and effects. BMC Med Res Methodol. 2017;17(1):5.
Penaloza-Ramos MC, Sheppard JP, Jowett S, Barton P, Mant J, Quinn T, Mellor RM, Sims D, Sandler D, McManus RJ. Cost-effectiveness of optimizing acute stroke care services for thrombolysis. Stroke. 2014;45(2):553–62.
Pronost M, Benjamin B, Gantzer S, Moulin T. Medico-economic modelling of stroke care with telemedicine. An experience in Franche-Comté. European Research in Telemedicine / La Recherche Européenne en Télémédecine. 2017;6:107–15.
Valenzuela Espinoza A, Devos S, van Hooff RJ, Fobelets M, Dupont A, Moens M, Hubloue I, Lauwaert D, Cornu P, Brouns R, et al. Time gain needed for in-ambulance telemedicine: cost-utility model. JMIR Mhealth Uhealth. 2017;5(11): e175.
Ajmi SC, Kurz MW, Ersdal H, Lindner T, Goyal M, Issenberg SB, Vossius C. Cost-effectiveness of a quality improvement project, including simulation-based training, on reducing door-to-needle times in stroke thrombolysis. BMJ Qual Saf. 2021;31(8):569–78. https://doi.org/10.1136/bmjqs-2021-013398.
Morii Y, Osanai T, Fujiwara K, Tanikawa T, Houkin K, Gu S, Ogasawara K. Analyzing cost-effectiveness of allocating neurointerventionist for drive and retrieve system for patients with acute ischemic stroke. J Stroke Cerebrovasc Dis : J Natl Stroke Assoc. 2021;30(8):105843.
Bayer S, Eom K, Sivapragasam N, Silva DAD, Choon G, Koh H, Tan KB, Ansah JP, Matchar DB. Estimating costs and benefits of stroke management: A population-based simulation model. J Operational Res Soc. 2020;72(9):2122–34.
Kim J, Easton D, Zhao H, Coote S, Sookram G, Smith K, Stephenson M, Bernard S, Parson MW, Yan B, et al. Economic evaluation of the Melbourne mobile stroke unit. Int J Stroke J Int Stroke Soc. 2021;16(4):466–75.
Germany: Gross domestic product (GDP) per capita in current prices from 1986 to 2026. 2014. https://www.statista.com/statistics/295465/germany-gross-domestic-product-per-capita-incurrent-prices. Accessed 12 Oct 2021.
US Dollar to Euro Spot Exchange Rates for 2014. 2014. https://www.exchangerates.org.uk/USD-EUR-spot-exchange-rates-history-2014.html. Accessed 12 Oct 2021.
Gross domestic product per capita in the United Kingdom from 1055 to 2020. 2011.https://www.statista.com/statistics/970672/gdp-per-capita-in-the-uk/. Accessed 12 Oct 2021.
Maas WJ, Lahr MMH, Buskens E, van der Zee DJ, Uyttenboogaart M. Pathway design for acute stroke care in the era of endovascular thrombectomy: a critical overview of optimization efforts. Stroke. 2020;51(11):3452–60.
Ramos A, Guerrero WR. Pérez de la Ossa N: prehospital stroke triage. Neurology. 2021;97(20 Suppl 2):S25-s33.
Requena M, Olivé-Gadea M, Muchada M, Hernández D, Rubiera M, Boned S, Piñana C, Deck M, García-Tornel Á, Díaz-Silva H, et al. Direct to angiography suite without stopping for computed tomography imaging for patients with acute stroke: a randomized clinical trial. JAMA Neurol. 2021;78(9):1099–107.
Pandian JD, William AG, Kate MP, Norrving B, Mensah GA, Davis S, Roth GA, Thrift AG, Kengne AP, Kissela BM, et al. Strategies to improve stroke care services in low- and middle-income countries: a systematic review. Neuroepidemiology. 2017;49(1–2):45–61.
Katan M, Luft A. Global burden of stroke. Semin Neurol. 2018;38(2):208–11.
Ezejimofor MC, Chen YF, Kandala NB, Ezejimofor BC, Ezeabasili AC, Stranges S, Uthman OA. Stroke survivors in low- and middle-income countries: a meta-analysis of prevalence and secular trends. J Neurol Sci. 2016;364:68–76.
Joo H, George MG, Fang J, Wang G. A literature review of indirect costs associated with stroke. J Stroke Cerebrovasc Dis : J Natl Stroke Assoc. 2014;23(7):1753–63.
Gorelick PB. The global burden of stroke: persistent and disabling. Lancet Neurol. 2019;18(5):417–8.
Acknowledgements
The CONTRAST consortium acknowledges the support from the Netherlands Cardiovascular Research Initiative, an initiative of the Dutch Heart Foundation (CVON2015-01: CONTRAST), and from the Brain Foundation Netherlands (HA2015.01.06). The collaboration project is additionally financed by the Ministry of Economic Affairs by means of the PPP Allowance made available by the Top Sector Life Sciences & Health to stimulate public-private partnerships (LSHM17016). This work was funded in part through unrestricted funding by Stryker, Medtronic and Cerenovus. The funding sources were not involved in study design, monitoring, data collection, statistical analyses, interpretation of results, or manuscript writing. We sincerely thank Peter G. Braun, information specialist at the Central Medical Library, University Medical Center Groningen, for his assistance in developing the search strategy. We would also like to thank Katsuhiko Ogasawara and Yasuhiro Morii (Hokkaido University, Hokkaido, Japan) for providing additional information regarding their article.
Funding
The CONTRAST consortium is supported by Netherlands Cardiovascular Research Initiative, an initiative of the Dutch Heart Foundation (CVON2015-01: CONTRAST), by the Brain Foundation Netherlands and powered by Health ~ Holland, Top Sector Life Sciences and receives unrestricted funding from Medtronic and Cerenovus. The collaboration project is additionally financed by the Ministry of Economic Affairs by means of the PPP Allowance made available by the Top Sector Life Sciences & Health to stimulate public–private partnerships.
Author information
Authors and Affiliations
Consortia
Contributions
All authors were involved with the conception and study design. Chi Phuong Nguyen and Willemijn J Maas performed screening records, data extraction, and data analysis. Maarten M H Lahr was the third reviewer. Chi Phuong Nguyen outlined the manuscript. Chi Phuong Nguyen and Willemijn J Maas drafted the manuscript. All authors critically reviewed the entire manuscript and approved the final submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was not required for this systematic review as no individual patient data were used. This systematic review was not registered.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix 1.
Search strategy description. Supplementary Table S1. Sensitivity analysis of included studies. Supplementary Fig. S1. Quality assessment of included studies according to each item of the CHEERS statement. Supplementary Table S2. PRISMA checklist. Supplementary Table S3.PRISMA 2020 for Abstract Checklist.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nguyen, C.P., Maas, W.J., van der Zee, DJ. et al. Cost-effectiveness of improvement strategies for reperfusion treatments in acute ischemic stroke: a systematic review. BMC Health Serv Res 23, 315 (2023). https://doi.org/10.1186/s12913-023-09310-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09310-0