
Abstract
Background
The COVID-19 pandemic has had a significant impact on the education sector, leading to the closure of colleges and schools and disrupting the learning process for an uncertain duration. In response, electronic learning has emerged as a suitable method for continuing the educational process during the lockdown. This study aimed to assess the attitudes, practices, and barriers to e-learning among medical students at Syrian Private University.
Methods
A cross-sectional survey study was conducted at the Faculty of Medicine of the Syrian Private University (SPU) in Damascus, Syria. The study used a convenience sampling approach and was carried out from June 2021 to January 2022. Data were collected using a self-administered questionnaire structured into two sections. The first section included 12 sociodemographic questions. The second section assessed students’ attitudes, practices, and barriers related to e-learning, and consisted of 14 questions on attitudes, 11 questions on practices, and 9 questions on barriers.
Results
Of the 519 participating students, over half (55.1%) exhibited a negative attitude towards e-learning. However, more than 60% reported engaging in e-learning activities such as downloading educational content and participating in virtual study groups. The main barriers identified were unstable internet connections (92.7%) and challenges in communication with educators (82.7%). Bionomical logistic regression revealed that negative attitudes were predicted by housing status, academic year, health status, lack of engagement with colleagues in e-learning practices, and the reported barriers of difficulty adjusting learning style, lack of technical skills, poor communication with educators, limited access to devices, and limited space conducive for studying (P < 0.05).
Conclusion
While medical students at SPU were actively engaged in e-learning, over half held negative attitudes. These negative attitudes were associated with the various barriers that students reported. The findings can inform stakeholders in our institution and other Syrian universities about the challenges of implementing e-learning in medical colleges.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
According to the World Health Organization (WHO), the coronavirus disease (COVID-19) has resulted in over 775 million cases and 6.9 million deaths since its emergence in 2019 [1]. This pandemic, caused by the SARS-CoV-2 virus, has had a profound and wide-ranging impact on global civilization, affecting major sectors like the economy, health, education, and social aspects [2]. The burden of this pandemic was far higher on low-income countries due to limited resources and inadequate health care [3]. In Syria, the pandemic significantly impacted a country that already struggles with a decade of ongoing conflict, affecting all vital sectors, particularly the healthcare system [4].
The global lockdowns were intended as a preventive measure to halt the rapid spread of the virus, though their overall effectiveness was mixed. These unplanned strategies created numerous problems, including a decline in social activities, disruptions to the global economy, challenges to food security, and widespread impacts on education [5]. The lockdown had paused the educational process in all its forms for an undetermined period. University students and researchers have experienced a significant decline in academic progress and have encountered various difficulties during this period. The Syrian community has been severely affected by the lockdown, as it has exacerbated their unmet economic and healthcare needs [6]. In the aspect of higher education, in March 2020, the Higher Education Council (HEC) in Syria implemented a lockdown of all higher education institutions for a duration exceeding two months to prevent the spread of the virus. This decision resulted in disruption to the academic year and had a widespread impact on the teaching and learning process [7].
E-learning has emerged as a concept that facilitates comprehensive learning through technological tools. Nowadays, e-learning plays an essential role in university education and further education. It is also utilized for informal training, providing personalized and socially enhanced learning experiences through the Internet [8]. E-learning in medical education has been well implemented even in its clinical spectrum where technical methods were developed to provide appropriate clinical knowledge such as open online courses, virtual reality environments, virtual patients, and psychomotor skills trainers [9]. E-learning, as a medical teaching method, presents a viable alternative to traditional in-person teaching and can assist in resolving the scarcity of medical doctors and educators, especially during a crisis [10,11,12].
During the abrupt lockdown, e-learning was quickly recognized as an effective method to reengage students in the educational process. However, due to the emergent situation, the implementation of this approach was accelerated without proper planning. This led to various unmet needs and challenges in e-learning. It can be acknowledged that the adoption of e-learning in educational facilities was compelled by the pandemic [13]. The transition to an alternative mode of learning, coupled with the challenges posed by the pandemic and the lockdown, resulted in significant difficulties for both educators and students.
Time constraints, technical skill deficiencies, inadequate infrastructure, a lack of institutional strategies and support, and negative attitudes are some of the main barriers to the development and adoption of e-learning in medical education [14]. These limitations pose a substantial burden, especially for low-income countries. In Syria, The HEC encouraged educational facilities to use alternative teaching methods such as online learning. However, numerous higher education institutions, particularly large public universities, were ill-equipped to implement the HEC’s online education mandate. Insufficient training among teaching staff in these new educational methods was notable. Moreover, students faced insurmountable obstacles such as the absence of necessary equipment, limited internet access, and inadequate support for online programs. Consequently, the Ministry of Higher Education ultimately rescinded the online education mandate, instructing institutions to return to face-to-face teaching after the lockdown and make up for the missed courses [7].
Recent research papers worldwide have extensively focused on assessing the attitudes, practices, and barriers to e-learning among medical students [13]. This is thought to be crucial as the success of this teaching method depends on several factors. The acceptance and accessibility of this approach from the students and teachers are considered the most significant, especially in the context of medical education where accurate healthcare education is vital for proper healthcare services. Notably, during the pandemic, the medical college at the Syrian Private University (SPU) implemented online distance learning for the first time to adapt to the lockdown. However, the impact of this new teaching strategy on students was not previously evaluated. Therefore, this current study aims to assess medical students’ attitudes toward e-learning, evaluate their practices and barriers related to this teaching method, and explore potential predictors of negative attitudes among the participating students.
Methods
Study design, participants, and sample size calculation
From June 2021 to January 2022, a cross-sectional study was conducted at the Faculty of Medicine of the Syrian Private University (SPU) in Damascus, Syria. The study aimed to investigate the use of e-learning tools among medical faculty students from the 1st to the 6th year. Specifically, during the study period, teachers incorporated various e-learning tools, including recorded lectures and online discussions, into their courses. The inclusion criteria for the study were current enrollment at the Syrian Private University and previous exposure to e-learning methods among medical students. It is important to note that some students may have been compelled to withdraw from classes due to the impact of the pandemic. Prior to participation, students were informed that their involvement was voluntary, and all their responses would be recorded anonymously. Additionally, students were informed that their involvement was voluntary, all responses would be recorded anonymously, and they were free to withdraw from the study at any time. The sample size was calculated by using the following single-population proportion formula: n = [(Zα/2)² * P * (1—P)] / d² where Zα/2 = 1.96 at the 95% level of significance, P = Proportion to be estimated = 50%, and d = degree of precision (0.05). The estimated required sample size was 385 students.
Study tool
We used a self-administered Arabic-language questionnaire that was modeled from several published studies [15,16,17]. The first section of the questionnaire contained nine questions about socio-demographic and background information including gender, age, social status, residence, academic year, housing, financial difficulties during the pandemic, level of electricity (e.g., poor, moderate, low quality), and internet connection quality (e.g., High, Good, Acceptable, low). In addition to the same section, 3 added questions about COVID-19, (1) self-reported health assessment, (2) whether they have sufficient knowledge regarding COVID-19, and (3) their source of information regarding COVID-19. The second section consists of 34 questions divided into three parts: attitudes to e-learning (14 of 5-point Likert scale questions), practice evaluation of e-learning (11 of Yes/No questions), and barriers to e-learning (9 of 4-point Likert scale questions).
Questionnaire reliability
The questionnaire was initially prepared in English and then translated into Arabic, the local language, for wider accessibility. To ensure consistency in meaning and concepts, the translated questionnaire was then translated back into English. This translation process was carried out by two healthcare teachers who were responsible for both the translation and review of the final questionnaire. The Research Ethics Committee approved the questionnaire before its implementation. To assess the questionnaire’s clarity, reliability, relevance, and acceptability, a pilot study was conducted. A total of 35 students were invited to participate in the pilot study and provide feedback on the questionnaire. Out of these invitations, 30 students accepted and shared their perceptions. However, it should be noted that this pilot study sample was excluded from the final sample to prevent any potential bias. During the pilot study, any questions that were found to be unclear or that did not adequately cover the study’s concept were modified accordingly, based on the feedback received from the participating students. Cronbach’s alpha test was applied to determine the internal consistency of the questionnaire. The Cronbach’s alpha value of the whole Arabic questionnaire was 0.714. The items were considered to represent an acceptable level of internal consistency [18].
Data collection
The questionnaire was distributed using two methods to ensure a diverse sample and minimize bias. The first method involved using online platforms such as WhatsApp and Telegram, where the questionnaire was shared through a Google Form survey. This approach allowed for chain-referral sampling, where respondents were encouraged to forward the questionnaire to their friends and colleagues. The second method was carried out by a dedicated data collection group under the supervision of the principal investigator. This group was responsible for distributing the questionnaires to students during the intervals between classes. To ensure convenience sampling, the data collection group enlisted the help of external individuals who were asked to voluntarily distribute the questionnaires. These external individuals were provided with comprehensive information about the study’s objectives and methodology, as well as detailed instructions on how to effectively carry out the distribution process.
Statistical analysis
The data collected through face-to-face administration of the questionnaires was integrated into the online questionnaire in Google Forms by the investigators. This integration process involved manually entering the responses from the face-to-face interviews into the corresponding sections of the original online questionnaire. By merging the data obtained from both sources, a unified dataset was created for analysis. We used Statistical Package for Social Sciences version 26.0 (SPSS Inc., Chicago, IL, United States). Frequencies and percentages for categorical and mean with SD for continuous variables. Attitudes were scored as; strongly agree- 1, Agree- 2, Neutral- 3, Disagree- 4, and strongly Disagree- 5, for reversed items (2 items), scores were reversed and computed as strongly agree- 5, Agree- 5, Neutral- 3, Disagree- 2, and strongly Disagree- 1, in dependence of the score means outcome, two levels were adopted, namely; Negative attitude (< 39), and Positive attitude (39< ). Statistical analysis employed chi-square tests to examine negative and positive attitudes. The analysis assessed: (1) demographics and participants’ characteristics, (2) students’ practice evaluation of medical e-learning, (3) and the reported barriers to e-learning. Binomial logistic regression was conducted to identify predictors of a negative attitude (< 39). The Enter method was used to analyze three categories of independent variables with the dependent variable. The Nagelkerke R Square was employed as an indicator of the model’s goodness of fit. P-values < 0.05 were considered statistically significant.
Ethical consideration
The Research Ethics Committee approved the study protocol by the Syrian private university (SPU), faculty of medicine at date (1/5/2021). Informed consent was obtained from every participant before participation. This study did not include participants younger than 18 years old. This study was performed in accordance with the Declaration of Helsinki.
Results
Socio-demographic characteristics
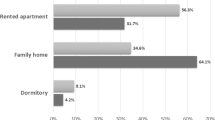
A total of 519 out of 583 (response rate = 89.02%) undergraduate medical students completed the survey. Of them, more than half were females (50.5%). The study participants had a mean age of 21 ± 2.01 years. Approximately 40% of the participants reported experiencing financial difficulties during the pandemic, while 41.8% indicated poor electricity connectivity. Furthermore, over two-thirds of the participants stated that they possessed sufficient knowledge about COVID-19. Social networking pages and groups served as the primary sources of information about COVID-19 for more than 50% of the participants. (Table 1).
Attitudes of participants toward E-learning
Among the 519 students included in the study, more than half of the sample (55.1%) exhibited negative attitudes towards e-learning. Over half of the participants (53.9%) strongly agreed that old devices and poor internet quality hindered their use of e-learning. Just over three-fifths of the participants reported a lack of interaction between students in e-learning. A significant proportion of participants (67.2%) agreed that there was poor communication between lecturers and students in the e-learning environment. The majority of students (69.6%) expressed a preference for direct communication and interaction with lecturers rather than electronic communication. More than half of the sample (52.4%) stated that e-learning is often not preferred due to its potential to increase social isolation. (Table 2).
Practices and barriers of E-learning
Table 3 presents a summary of the participants’ responses concerning the evaluation of e-learning practices and the barriers associated with it. More than half of the respondents reported engaging in various activities related to e-learning: accessing online courses for medical information (15.4%), downloading educational content (64.2%), sharing materials with peers (59.5%), participating in virtual study groups (54.5%), utilizing personal computers for online studying (57.2%), incorporating the internet into their regular academic routines (61.1%), and opting for electronic content over paper formats to save costs (46.6%).
The majority of the participants identified several barriers to e-learning, as shown in Table 3. These included difficulties in adapting to the learning style (87.7%), challenges in maintaining effective communication with educators (82.7%), and unstable internet connections (92.7%). Additionally, over half of the respondents cited specific obstacles such as a lack of technical skills (55.1%), limited access to devices or the internet (55.3%), and limited space to study (68.8%).
Predicted factors of negative attitude towards E-learning
Three binomial logistic regression models were run on three categories of independent variables (Table 4). The initial model examines socio-demographic factors as predictors of the outcome variables, this model was statistically significant, X2 = 46.9, P < 0.001. Of the variation in medical students’ negative attitudes toward e-learning (< 39), this model predicted 11.6% (Nagelkerke R Square). Of the four predictor variables, three were statistically significant (P < 0.05). 2nd and 3rd-year students had two times higher odds of negative attitude compared to those in other academic year categories. Students who live alone demonstrated a twofold higher likelihood of having negative attitudes compared to those living with their families.
The second model examines practices as predicted factors of the negative attitudes, this model was statistically significant, X2 = 42.3, P < 0.001. Of the variation in medical students’ negative attitudes toward E-learning (< 39), this model predicted 10.5% (Nagelkerke R Square). Of the eight predictor variables, only one was statically significant (P < 0.05). students who did not share educational materials with their colleagues have 1.7 times higher odds of having negative attitudes compared to those who did.
The last model examines barriers as predictors of the outcome variables, this model was statistically significant, X2 = 27.5, P < 0.001. Of the variation in medical students’ negative attitudes toward E-learning (< 39), this model predicted 6.9% (Nagelkerke R Square). Students who stated difficulty adjusting learning style, lack of technical skills, poor communication with educators, no device or limited access, and limited space conducive for studying as barriers have 1-1.8 times higher odds of having negative attitudes compared to those who did not.
Discussion
The COVID-19 pandemic abruptly disrupted the educational process, necessitating the rapid adoption of alternative teaching methods, such as e-learning. Many educational institutions found themselves implementing this approach for the first time. E-learning emerged as a convenient means for reintegrating students into the educational process. It can be argued that the pandemic expedited the implementation of e-learning methods without prior planning. Numerous universities in advanced nations adopted e-learning to respond to the epidemic [19]. However, in low-income countries like Syria, switching to e-learning necessitates several adaptations to ensure effective delivery. A technological framework had to be constructed, and educators had to rapidly modify their curriculum. Following the lockdown in Syria, SPU’s response was swift; within a month, a platform featuring audio presentations and WhatsApp groups alongside teachers was built to increase students’ connection with teachers. This study aimed to assess attuited, practices, and barriers towards e-learning among medical students at Syrian Private University. In addition, this study aimed to identify predicted factors of negative attitudes towards the experience of e-learning.
Syrian Private University was one of the few Syrian institutions that implemented e-learning during the pandemic, and this study is the first in Syria to evaluate this experience. The study found that while over half of the respondents were actively engaged in e-learning activities, 55.1% of the surveyed medical students exhibited negative attitudes toward e-learning. Negative attitudes were predicted by several factors, including housing status, academic year, health status, lack of engagement with colleagues in e-learning practices, and the reported barriers of difficulty adjusting learning style, lack of technical skills, poor communication with educators, limited access to devices, and limited space conducive for studying.
While numerous studies in the Middle East have investigated e-learning, offering valuable insights, the findings of this study contrast with some previous research. A previous study in Libya indicated that the medical students exhibited relatively positive attitudes, but over half also showed inadequate e-learning practices [16]. In contrast, a study at King Saud University found most medical students had a positive attitude towards online classes, though 59.6% reported difficulties obtaining explanatory information - a challenge faced by 42% of the sample in this study [20].
A Lebanese study revealed that approximately 39% of the participants reported low satisfaction with this mode of learning [21], while studies in the UAE and Iran reported generally acceptable attitudes toward e-learning [22, 23]. These variations in results may be influenced by the different contexts in which the studies were conducted, as each country has its unique educational system, and infrastructure, which can impact students’ perceptions of e-learning [24]. It is crucial to acknowledge that the current study was conducted in Syria, a country that has experienced severe conflict and crisis, significantly impacting the necessary infrastructure for e-learning. Additionally, the psychological burden faced by Syrian students is an external factor that may have influenced their acceptance and engagement with online education [25]. Although this influence was partially evident in our findings, it is important to note that the study did not directly assess the psychological impact on students through specific measures.
The present study found students living alone were more likely to develop negative attitudes toward e-learning, and over half the participants agreed it contributes to increased social isolation. These results are consistent with findings from other studies. For example, according to a King Saud University study, two-thirds of participants believed that distance learning impeded their ability to meet and collaborate with friends [20], while a Lebanese study revealed that students who preferred online education over in-person education exhibited significantly lower scores in social functioning [21]. Additional research stratified that e-learning led to prolonged social isolation and restricted interaction with peers [26]. However, it is important to note that this study was conducted during the COVID-19 pandemic, a period characterized by lockdowns and limited social activities [27]. Therefore, it may not be entirely accurate to conclude that e-learning is the primary cause of social isolation. Future studies should consider assessing this issue under normal circumstances, outside of emergencies.
Preclinical students in their second and third years demonstrated a higher propensity for negative attitudes towards e-learning. This aligns with a King Saud University study [20], but it contrasts with findings from Iran [23]. Previous research states that preclinical students tend to hold negative attitudes toward online teaching as they believe it restricts their communication, teamwork, brainstorming, critical thinking, ability to orient themselves, and access to support [28]. Recent research recommended that hybrid learning, combining online and in-person methods, is generally considered more effective than online-only approaches [29].
This study identified several key barriers impacting attitudes towards e-learning. Notably, poor communication with educators emerged as a significant issue, as approximately 80% of the sample reported this problem. Additionally, in the King Saud University study, more than half of the participants stated this limitation [20]. Relatedly, In the Sudan study, 24% of students expressed concern regarding the interaction with peers and instructors during online sessions [30]. Qualitative research further indicates issues related to poor communication with educators encompass various aspects, such as ineffective educational feedback, which includes one-sided communication or a lack of two-way communication, deficiency in student-educator interaction, and limited interaction between student and health profession educators across different platforms [31].
Another significant barrier was a lack of technical skills and limited access to devices, reported by over half of the sample. Prior research supports this, with studies of medical students in Egypt finding that 23% reported a lack of internet connection, and 5% reported a lack of devices as barriers to online e-learning [32]. Similarly, a Sudan study revealed that 40% of the sample expressed concerns regarding technical support and only 38% stated good internet quality [30]. In contrast, studies in Libya [16] and King Saud University [20] reported generally good availability of technical resources.
The variations in e-learning barriers across regions can be attributed to a combination of factors. One key factor is the level of technological infrastructure and connectivity in each area. Developed regions are more likely to have reliable and advanced technological infrastructure resulting in fewer barriers related to internet access and quality. Conversely, regions with limited infrastructure or remote areas may face challenges in accessing stable internet connections, leading to higher reported barriers [33]. Students’ access to technological resources and technical support can affect their overall satisfaction with e-learning. Notably, the study findings highlight the significant effect of various barriers on e-learning practices in the context of war-torn Syria. The severe infrastructure challenges caused by the conflict have directly affected the accessibility and reliability of e-learning resources and platforms. Consequently, has hindered students’ ability to fully engage and participate in online education. For instance, the lack of technical skills is considered one of the most significant barriers to e-learning, resulting in a negative impact on the acceptance of this teaching method [34]. This issue is particularly pronounced in the context of Syria, as confirmed by the study findings. The final decision to withdraw online education by the Ministry of Higher Education in Syria reflects the impact of barriers on e-learning practice.
This study identifies significant predictors for negative attitudes toward e-learning. Pinpointing these predictors is crucial as modifying those factors leads to better outcomes when using this educational approach. it is recommended to focus on improving accessibility, user experience, and comprehensive training while fostering a positive learning environment. Implementing these recommendations is anticipated to enhance medical students’ engagement with and positive perception of e-learning.
Limitation
A key limitation of this study is its reliance on self-reported data, particularly for variables such as social status, internet connectivity, and electricity connectivity. Participants’ tendency to provide socially desirable responses may have impacted the study outcomes. One limitation is the lack of clarity in certain survey questions, such as those related to health status and knowledge about the emerging coronavirus pandemic, rated internet and electricity without specifying assessment criteria. Additionally, the predominantly young age group (21–24 years) in the sample might not fully represent the wider student population, and the subgroup analysis based on residence may limit generalizability. Moreover, this study was conducted on university student regardless of their nationality which may affect the generalizability of the study results. Furthermore, the study’s external validity is constrained by its focus on a single private university in Syria, which does not represent the entire educational population. Finally, the use of Google Forms as the data-gathering tool may have introduced potential bias.
Conclusion
While the majority of respondents reported engaging in e-learning activities, more than half of participating medical students showed negative attitudes toward e-learning. These negative attitudes were driven by the barriers to e-learning that were reported.
The findings of this study have important implications for stakeholders within the institution, as well as other universities in Syria, regarding the challenges associated with the adoption of e-learning as an effective teaching approach in medical colleges. it is recommended to raise knowledge and influence attitudes towards e-learning adoption within medical colleges, the university should organize awareness webinars discussing the challenges and benefits of e-learning, featuring expert speakers and interactive sessions. Additionally, specialized training courses should be offered to faculty members, equipping them with knowledge about the benefits of e-learning and practical guidance on its implementation.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- WHO:
-
World Health Organization
- HEC:
-
Higher Education Council
- E-learning:
-
Electronic learning
- COVID-19:
-
coronavirus disease of 2019
- SPSS:
-
The Statistical Package for Social Sciences
- SPU:
-
Syrian Private University
References
WHO COVID-19. dashboard [ https://data.who.int/dashboards/covid19/cases?n=c
Gebru AA, Birhanu T, Wendimu E, Ayalew AF, Mulat S, Abasimel HZ, et al. Global burden of COVID-19: situational analyis and review. Hum Antibodies. 2021;29(2):139–48.
Levin AT, Owusu-Boaitey N, Pugh S, Fosdick BK, Zwi AB, Malani A, et al. Assessing the burden of COVID-19 in developing countries: systematic review, meta-analysis and public policy implications. BMJ Global Health. 2022;7(5):e008477.
Mohsen F, Bakkar B, Armashi H, Aldaher N. Crisis within a crisis, COVID-19 knowledge and awareness among the Syrian population: a cross-sectional study. BMJ Open. 2021;11(4):e043305.
Onyeaka H, Anumudu CK, Al-Sharify ZT, Egele-Godswill E, Mbaegbu P. COVID-19 pandemic: a review of the global lockdown and its far-reaching effects. Sci Prog. 2021;104(2):00368504211019854.
Kakaje A, Mansour S, Ghareeb A. Was a forced lockdown adequate for a country in conflict? A psychological perspective from the Syrian population. Qatar Med J. 2021;2021(1):17.
Mualla W, Mualla K. Higher Education in Syria Post-war and Pandemic: Challenges and Opportunities. 2022. pp. 283–309.
Siemens G, Connectivism. A learning Theory fir the Digital Age. 2005.
Ellaway R, Masters K. AMEE Guide 32: e-Learning in medical education part 1: learning, teaching and assessment. Med Teach. 2008;30(5):455–73.
Jayakumar N, Brunckhorst O, Dasgupta P, Khan MS, Ahmed K. e-Learning in Surgical Education: a systematic review. J Surg Educ. 2015;72(6):1145–57.
Corrêa L, de Campos AC, Souza SC, Novelli MD. Teaching oral surgery to undergraduate students: a pilot study using a web-based practical course. Eur J Dent Educ. 2003;7(3):111–5.
Belfi LM, Dean KE, Bartolotta RJ, Shih G, Min RJ. Medical student education in the time of COVID-19: a virtual solution to the introductory radiology elective. Clin Imaging. 2021;75:67–74.
Aristovnik A, Karampelas K, Umek L, Ravšelj D. Impact of the COVID-19 pandemic on online learning in higher education: a bibliometric analysis. Front Educ. 2023;8.
O’Doherty D, Dromey M, Lougheed J, Hannigan A, Last J, McGrath D. Barriers and solutions to online learning in medical education – an integrative review. BMC Med Educ. 2018;18(1):130.
Baticulon RE, Sy JJ, Alberto NRI, Baron MBC, Mabulay REC, Rizada LGT, et al. Barriers to Online Learning in the Time of COVID-19: a National Survey of Medical students in the Philippines. Med Sci Educ. 2021;31(2):615–26.
Alsoufi A, Alsuyihili A, Msherghi A, Elhadi A, Atiyah H, Ashini A, et al. Impact of the COVID-19 pandemic on medical education: medical students’ knowledge, attitudes, and practices regarding electronic learning. PLoS ONE. 2020;15(11):e0242905.
Olum R, Atulinda L, Kigozi E, Nassozi DR, Mulekwa A, Bongomin F, et al. Medical Education and E-Learning during COVID-19 pandemic: awareness, attitudes, preferences, and barriers among undergraduate medicine and nursing students at Makerere University, Uganda. J Med Educ Curric Dev. 2020;7:2382120520973212.
Ursachi G, Horodnic IA, Zait A. How Reliable are Measurement Scales? External factors with indirect influence on reliability estimators. Procedia Econ Finance. 2015;20:679–86.
Jin YQ, Lin CL, Zhao Q, Yu SW, Su YS. A study on traditional teaching method transferring to E-Learning under the Covid-19 pandemic: from Chinese students’ perspectives. Front Psychol. 2021;12:632787.
Alzamil HA, AlSaleh F, Bin Selayem S, Alhakbany MA. The attitude of King Saud University Medical Students toward Online Distance Learning during the COVID-19 pandemic. Adv Med Educ Pract. 2022;13:1407–16.
Hatem G, Omar CA, Ghanem D, Khachman D, Rachidi S, Awada S. Evaluation of the impact of online education on the health-related quality of life of medical students in Lebanon. 2023;24(3):100812.
Malkawi E, Bawaneh A, Bawaaneh M. campus-off-education-on-uaeu-students-satisfaction-and-attitudes-towards-e-learning-and-virtual-8708. Contemporary Educational Technology. 2020;13:ep283.
Niroumand S, Mastour H, Moodi Ghalibaf A, Shamshirian A, Moghadasin M. Medical Students’ Attitude Toward E-learning During the COVID-19 Pandemic. Shiraz E-Medical J. 2022;23.
Connolly N, Abdalla ME. Impact of COVID-19 on medical education in different income countries: a scoping review of the literature. Med Educ Online. 2022;27(1):2040192.
Tozan O. The impact of the Syrian conflict on the higher education sector in Syria: a systematic review of literature. Int J Educational Res Open. 2023;4:100221.
Rutkowska A, Cieślik B, Tomaszczyk A, Szczepańska-Gieracha J. Mental Health conditions among E-Learning students during the COVID-19 pandemic. Front Public Health. 2022;10.
Walters M, Alonge T, Zeller M. Impact of COVID-19 on Medical Education: perspectives from students. Acad Med. 2022;97(3s):S40–8.
Hanafy SM, Jumaa MI, Arafa MA. A comparative study of online learning in response to the coronavirus disease 2019 pandemic versus conventional learning. Saudi Med J. 2021;42(3):324–31.
Lee BE, Zlotshewer BA, Mayeda RC, Kaplan LI. Impact of online-only instruction on Preclinical Medical Education in the setting of COVID-19: comparative analysis of online-only Vs. hybrid instructions on academic performance and Mental Wellbeing. Med Sci Educ. 2022;32(6):1367–74.
Gismalla MD-A, Mohamed MS, Ibrahim OSO, Elhassan MMA, Mohamed MN. Medical students’ perception towards E-learning during COVID 19 pandemic in a high burden developing country. BMC Med Educ. 2021;21(1):377.
Salarvand S, Mousavi MS, Rahimi M. Communication and cooperation challenges in the online classroom in the COVID-19 era: a qualitative study. BMC Med Educ. 2023;23(1):201.
Mortagy M, Abdelhameed A, Sexton P, Olken M, Hegazy MT, Gawad MA, et al. Online medical education in Egypt during the COVID-19 pandemic: a nationwide assessment of medical students’ usage and perceptions. BMC Med Educ. 2022;22(1):218.
Abbas U, Parveen M, Sahito FS, Hussain N, Munir S. E-learning in medical education: a perspective of pre-clinical medical students from a lower-middle income country. BMC Med Educ. 2024;24(1):162.
Regmi K, Jones L. A systematic review of the factors - enablers and barriers - affecting e-learning in health sciences education. BMC Med Educ. 2020;20.
Acknowledgements
We would like to thank Morphine Team members in Syrian private university (Masa Bytamoni, Ghina Almustafa, Selim Badra, Abdullah Al-Rebdawi, Nour Zuhair Abd Alaal, Malaz Shammout, Asma’ Alnoufi, Rafah Jumaa) who helped in the questionnaire distribution process.
Funding
This project did not receive any funding from any agencies in the public, commercial, or non-profit sectors.
Author information
Authors and Affiliations
Contributions
Mhd Homam Safiah, Mhd Obai Alchallah, Homam Alolabi, Muhammad Omar ElHomsi, and Sham Ataya conceptualized the study, participated in the design, and wrote the study protocol. Mhd Homam Safiah and Khaled Kalalib Al Ashabi performed the statistical analysis and were responsible for the literature search. Muhammad Omar ElHomsi was responsible for the literature search and drafted the manuscript. Fatema Mohsen revised the final draft. Louie Darjazini Nahas supervised the study and revised the draft. All authors read and approved the final draft.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Research Ethics Committee in a Syrian private university. Informed consent was obtained from every participant before participation. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Safiah, M.H., Alchallah, M.O., ElHomsi, M.O. et al. The attitudes of Syrian Private University Medical Students towards E-Learning during the COVID-19 pandemic: a cross-sectional study. BMC Med Educ 24, 826 (2024). https://doi.org/10.1186/s12909-024-05817-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-024-05817-0