
Abstract
Background
Medical students face significant psychological stress, impacting their academic performance and well-being. The Systematic Assessment for Resilience (SAR) framework is designed to enhance resilience and mitigate stress among medical students, addressing the need for interventions within the assessment system in medical education. The aim of this study was to evaluate the implementation of SAR framework on medical students’ resilience, anxiety, depression, burnout, and academic stress.
Methods
This study employed a quasi-experimental design with pre- and post-testing. It involved the training of course coordinators in implementing the SAR framework and its integration into the daily learning activities. Fourth-year medical students were assessed before and after the intervention using standardized measures of resilience, anxiety, depression, burnout, and academic stress. Data were analyzed using quantitative methods and thematic analysis for qualitative feedback.
Results
Post-intervention, students demonstrated a significant increase in resilience scores (p < 0.001) and a notable decrease in measures of anxiety, depression, and academic stress (p < 0.001). The burnout types were also statistically different (p < 0.001) except client-related burnout (p > 0.05). Qualitative feedback of the course coordinators highlighted an improved learning environment, increased coping strategies, and a more supportive academic culture.
Conclusion
The SAR framework significantly contributes to enhancing medical students’ resilience and reducing psychological distress. Its implementation suggests a promising approach to fostering a supportive educational environment that not only addresses the psychological challenges faced by medical students but also enhances their academic performance and overall well-being. Further research is warranted to explore the long-term impacts of SAR across different medical education contexts.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Medical students perceive medical school as a demanding environment due to the nature and magnitude of the curriculum’s contents [1] and the pressure of numerous assessments that influence important decisions in their lives [2]. Systematic reviews and meta-analyses reveal alarming figures regarding the extent to which medical students suffer from stress and its consequences, such as anxiety and depression [3,4,5]. It has been found that 30% of medical students suffer from stress, anxiety, or depression [5,6,7]. Other studies have reported even higher rates of these problems (70%) [8, 9]. Chronic stress aggravates other undesirable problems, such as poor academic performance, poor peer relationships, academic dishonesty, depression, and even sleep and eating disorders [10, 11]. Additionally, chronic stress is connected to drug addiction, alcoholism, and suicide [3,4,5]. It has been found that doctors who suffer stress throughout their undergraduate education may develop a negative attitude toward their profession that could threaten patient care [5,6,7].
Based on these facts, it is sensible to identify the causes of stress and to implement interventions to alleviate this burden. Multiple studies have found that tests and exams are among the most identified causes [4, 5, 12, 13]. Consequently, several interventions have been implemented to combat what is known in the literature as test anxiety [7, 14]. In their systematic review, Soares and Woods [15] summarized several studies on test anxiety reduction and found a lack of collaboration between the identified interventions and the school site, which impeded the maximum benefit of intervention and the desired outcomes. Furthermore, the identified studies focus on a single aspect of the problem without addressing a solid theoretical framework or a holistic perspective on other factors that influence the situation [15]. Consequently, it has become vital to seek comprehensive approaches that incorporate both individual and systemic (organizational) factors [4, 5]. With the expansion of resilience research, medical educators are increasingly interested in identifying interventions that foster resilience among medical students [3, 16, 17].
Resilience is a construct that cultivates a variety of characteristics necessary for adapting to the dynamic changes of life and maintaining well-being [18]. Resilience is no longer viewed as a set of inherited traits that enable an individual to overcome life’s challenges and adversities; rather, it is viewed as a dynamic process and an acquired trait, meaning that it can be taught and fostered [19, 20]. Despite varying definitions of resilience, the general and agreed definition is the individual’s capacity to deal with and overcome adversity appropriately and effectively that boosts well-being [4, 18, 21,22,23,24]. Accordingly, resilient students are those who can maintain their abilities and continue to grow despite academic and life obstacles [3, 25,26,27]. According to related literature, resilience can be fostered by working on multiple levels. The first level begins with internal factors, which means advancing the psychological process in the face of adversity and enhancing what are called “internal traits” [28]. The second level involves exposing individuals to simulated adversities and providing them with opportunities for reflection [21, 29]. The third level derives from the extent of institutional or organizational efforts to provide protective factors and fertile resources (external protective factors) to equip individuals with the necessary protective factors to overcome life’s adversities [28, 30].
In their recent research, Wadi et al. developed a framework for fostering resilience through the process of student assessment [31]. This framework is called the Systematic Assessment for Resilience (SAR) framework and encompasses numerous guidelines for fostering resilience and enhancing its four constructs: (1) self-control, in which students should be able to govern themselves and face adversity; (2) management, which describes the students’ ability to use available resources effectively to overcome obstacles; (3) engagement, which highlights the students’ ability to be involved and committed to pursuing challenges with perseverance; and (4) growth, which reflects the students’ ongoing development to face future challenges. The four constructs work together in a cycle to promote resilience through five phases of assessment: (i) direction, which focuses on improving the candidate’s understanding of the assessment’s scope and procedure; (ii) preparation, which emphases enhancing candidates’ cognitive, mental, and psychomotor readiness to optimize assessment performance; (iii) experience, which helps enhance the formative assessment component; (iv) examiner focus, which deals with improving examiner behavior to increase candidate performance and decrease candidate anxiety; and (v) student reflection, which encourages self-review [31]. The SAR framework presents a comprehensive approach that promises to foster a learning environment in medical schools that supports mental well-being and cultivates resilience in medical students. Therefore, this study aims to evaluate the impact of the SAR framework implementation on enhancing resilience and reducing anxiety, depression, and academic-related stress among medical students.
Methods
Study setting
The study was conducted at the University of Sharjah, College of Medicine (UoS-CoM), which offers a six-year MBBS program delivered in three phases: Phase I is the foundation year and Phase II is the pre-clerkship phase, which includes years 1, 2, and 3. This is followed by Phase III, a clerkship phase, that comprises years 4 and 5. In the clerkship phase, students receive clinical training in various departments in public and private hospitals in Sharjah. Year 4 consists of four clinical rotations (10 weeks each) in the four major divisions of Medicine, Surgery, Pediatrics, and Obstetrics & Gynecology, while in Year 5, the rotations include medicine and surgery sub-specialties such as Neurology, Dermatology, Cardiology, Nephrology, ENT, and Ophthalmology, as well as Family Medicine and Psychiatry [32].
Study population
-
1)
Students.
For logistical considerations, Year 4 students were selected as study participants. All 149 fourth-year medical students registered for the academic year 2021–2022 at UoS-CoM were invited to participate in this study.
-
2)
Course coordinators.
Eight Year 4 course coordinators, responsible for planning courses, organizing educational events, facilitating bedside training in teaching hospitals, and managing learning materials in the learning management system, were invited to participate in the study.
Eligibility criteria of participants
For students, only those who participated in both the pre- and post-stages of the study will be included in the analysis of the results. As for course coordinators, only those who agree to participate in the in-depth interview will be included in the analysis of results.
Study design
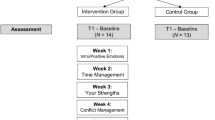
The study used a quasi-experimental design with one group pre- and post-test [33]. The decision to opt for a single-group design was driven by ethical considerations, as randomizing student participants into intervention and control groups posed ethical concerns related to potential unequal benefits [33]. Additionally, the feasibility of maintaining the integrity of training materials among course coordinators in the target group further supported the choice of a single-group pre-test and post-test design [34].
The design begins with training all course coordinators on how to use the SAR framework as a daily practice in their respective clerkships and then measuring its effect on students before and after its implementation. Furthermore, in-depth interviews were conducted with the course coordinators (Fig. 1). The purpose of this qualitative phase was to gain insights into the perceptions of the SAR guidelines among medical teachers, as well as to assess the feasibility and applicability of these guidelines in the clinical setting.
Study intervention
The intervention began with a training session on how to utilize and implement the SAR framework, which was completed before the clerkship rotation began. It was a five-hour online training workshop provided by Microsoft Teams for fourth-year medical educators (Appendix I). The course coordinators were informed that SAR consists of guidelines that promote resilience throughout the various phases of assessment, from planning to implementation to evaluation. Participants were given a group activity consisting of a list of SAR guidelines presented in the form of a series of yes-or-no questions regarding how to apply the SAR guidelines (Appendix II). To facilitate the effective implementation of the guidelines, they were tabulated, and each was accompanied by an example of how and when to use it (Appendix III). In addition, the participants were supported/monitored through ongoing online communication (WhatsApp group, online meetings, email reminders) to discuss and clarify any concerns regarding SAR guidelines. They were not required to implement all of the framework’s guidelines; rather, they were free to decide which guidelines were feasible and applicable to their clerkships. As a result, all students received the intervention, which was tailored based on the guidelines implemented by their course coordinators.
Data collection
Quantitative data
Quantitative data were gathered from Year 4 medical students whose course coordinators implemented the SAR guidelines in their respective courses. Before starting their respective clerkship rotations, all students were invited to complete the study’s measurement instruments through a Google form, distributed to them via their official email addresses. Four tools were used: (1) the Medical Professionals Resilience Scale (MeRS) to measure resilience, (2) the academic-related stressors (ARS) part of the Medical Students Stressor Questionnaire (MSSQ), (3) the depression and anxiety parts of the Depression and Anxiety Stress Scale (DASS), and (4) the Copenhagen Burnout Inventory (CBI). Appendix IV contains full details of study tools and how they were scored, however, a general overview of these tools is described below.
The Medical Professionals Resilience Scale (MeRS) [35] measures four domains of resilience based on the integrated resilience model [36]: control, resourcefulness, involvement, and growth dimensions. The MeRS is a valid and reliable scale with a Cronbach’s alpha of 0.914 [35]. It presents 37 items to rank according to a four-point Likert scale (1 Strongly disagree, 2 Disagree, 3 Agree, and 4 Strongly agree). Six items assess the domain of control, which refers to medical professionals’ ability to remain calm and composed in the face of adversity, four assess resourcefulness—the ability to use available resources to overcome adversity—twelve assess commitment, and fifteen assess growth capability and resilience following adversity.
The Medical Student Stress Questionnaire (MSSQ) [37] contains 40 items covering six dimensions of stress unique to medical students—academic stressors, interpersonal stressors, teaching and learning stressors, social stressors, drive/desire stressors, and group activity stressors. The questionnaire is based on a four-point Likert scale and has a good level of validity and reliability, with a Cronbach’s alpha of 0.95 in the initial study [37], and its reliability has been consistently upheld across various contexts and cultures [38, 39]. For the purpose of this study, only the items measuring academic-related stressors (ARS) were used.
The Depression, Anxiety, and Stress Scale (DASS-21) [40] is a widely used screening tool that utilizes a tripartite approach to assess three dimensions of emotional states: depression (low positive affect), anxiety (physiological hyperarousal), and stress (negative affect) [41]. Each dimension of the DASS-21 contains seven items. The respondents were asked to consider how much each statement applied to them in the previous week and rank each statement accordingly. A score of 0 means Did not apply to me at all, 1 = Applied to some degree or some of the time, 2 = Applied to me to a considerable degree or a good part of time, 3 = Applied to me very much or most of the time). DASS-21 has an overall Cronbach’s alpha of 0.93 [40] in the original study. This reliability has been mirrored in its global application [42].
The Copenhagen Burnout Inventory (CBI) [43] is a self-reporting inventory comprised of 19 items that assess personal-, work-, and client-related burnout. The personal-related burnout domain has six items and assesses respondents’ levels of physical and psychological fatigue or exhaustion independent of their work. The work-related burnout domain contains seven items and assesses respondents’ levels of physical and psychological fatigue or exhaustion as a result of their employment. The client-related burnout domain has six items and assesses the respondent’s bodily and psychological weariness or fatigue as a result of their clients. Client is a broad term that encompasses individuals, such as students, customers, and patients. In accordance with the CBI guide, the phrase “client-related burnout” should be used when referring to the sample’s participants, and this domain will henceforth be referred to as shown. It has been confirmed using Cronbach’s alpha values of 0.85 to 0.87 for each domain [43], the reliability of the instrument has been consistently evident in various studies utilizing the CBI [44].
For the purpose of analyzing and matching students’ responses in pre- and post-intervention, students were asked to include a distinct number in both surveys to facilitate the matching of pre- and post-intervention responses without compromising confidentiality.
Qualitative data
Qualitative data were collected at the end of the clinical courses via in-depth interviews with the course coordinators. The interview was conducted in person and recorded for verbatim transcription and analysis. Figure 1 is a flow chart illustrating the steps of the study.

Study flowchart
Data analysis
Quantitative data
Initially, each participant’s pre- and post-intervention data were matched, and descriptive and inferential analyses were conducted using SPSS 23 with a 95% confidence interval and a significance level of 0.05. Based on the majority of measurement tools, the responses were calculated as means and standard deviations (SD). The paired t-test was used to compare the means of pre- and post-intervention results among students. McNemar test was used to analyze the difference of burnout cases pre- and post-intervention. Additionally, the Pearson correlation coefficient was used for pre- and post-intervention measurements to evaluate study parameters.
Qualitative data
Braun and Clark’s six-phase thematic analysis method was used for the analysis of the transcripts of the interviews [45]. In the first step (data familiarization phase), the authors familiarized themselves with the data transcribed verbatim from the audio recordings, assigned pseudonyms to all identifiable individuals, and cross-checked the transcript against the audio recordings. In the second step (generating initial codes), the authors imported the transcript into Atlas.Ti (version 7.9) and began identifying open codes across the dataset, including the participants’ own words (in vivo) or a descriptor for their experience. Next, in the third step (searching for themes), the authors sought themes by combining several related codes to generate overarching themes. Then in the fourth step, reviewing the themes, the authors reviewed the themes and their coherence with the related quotes and defined and named the themes (fifth step) to write the report. Finally, as the sixth step, the authors wrote the report.
To ensure the trustworthiness of qualitative data, the researchers employed Guba’s four criteria: credibility, transferability, dependability, and confirmability [46]. Credibility (akin to internal validity) was enhanced through prolonged engagement during interview, ensuring participants fully expressed their experiences, and member checking, which involved validating summaries of discussion with participants “on the spot”. Transferability (comparable to external validity) was facilitated by providing detailed descriptions in the methodology section of the study’s context and participants, enhancing the applicability of findings across different settings. Dependability was secured through a code-recode strategy, involving periodic reevaluation of data coding to verify consistency. Lastly, confirmability was established by creating an audit trail, documenting the research process and analysis, thus offering a transparent record for external examination.
Results
After matching students’ pre-and post-intervention responses, 78 students of 149 had participated in both phases. The characteristics of the students are shown in Table 1.
Pre- and post-intervention scores of the measured parameters were compared for all students. Collectively, the mean differences in resilience (as a global score), as well as its underlying four constructs, showed negative values, indicating a significant increase in these parameters after the intervention, whereas the difference in the mean scores of depression, anxiety, and academic-related stressors showed positive values, indicating a significant reduction of these parameters after the intervention. There were statistically significant differences between the mean scores for all parameters (Table 2).
The analysis of student burnout pre- and post-intervention revealed significant shifts in two categories of burnout (Table 3). For personal-related burnout, all 21 participants initially classified as non-cases remained unchanged, highlighting the intervention’s stability in non-affected individuals. Conversely, 12 participants previously identified as cases transitioned to non-cases, showcasing a notable positive change (p-value < 0.001). In the realm of work-related burnout, while 25 non-cases maintained their status, 11 cases shifted to non-cases, underscoring the intervention’s effectiveness (p-value = 0.001). However, in client-related burnout, although a shift was observed with 6 moving from case to non-case, this change was not statistically significant (p-value = 0.289) (Table 3).
The correlation matrix presented in Table 4 reveals substantial associations among the study variables pre- and post-intervention. Global resilience and its four domains consistently showed strong, positive correlations in both assessments. Depression, anxiety, and academic-related stress (ARS) were positively correlated with various burnout types. Inversely, global resilience and its subcomponents negatively correlated with these psychological stress indicators, suggesting that higher resilience is linked to lower levels of depression, anxiety, and stress.
Qualitative analysis of in-depth interviews
In-depth interviews were conducted with five course coordinators who agreed to participate to offer their perceptions of the SAR framework and its guidelines. Interviews were conducted through an online platform, each lasting around 35 min. The qualitative analysis of the interviews revealed the themes shown in Table 5. Generally, all coordinators acknowledged the feasibility of implementing the SAR framework with their educational practices; for example, briefing the students about assessments, sharing the assessment rubrics with the students, implementing formative assessment and mock exams, providing supporting material about coping and study skills, encouraging peer and self-assessment, and orienting the examiners to create a less stressful environment during the exams. Concerning observed effectiveness, the coordinators stated that they noticed that students in the intervention were generally self-assured and were enjoying the rotation compared to other batches. Regarding the challenges faced with the SAR after its implementation, one coordinator expressed that some strategies could not be done without official approval from the curriculum committee; for instance, introducing collaborative assessment and open book exams. Almost all the coordinators emphasized that components included in the SAR framework should be obligatory as part of educational practices.
Discussion
In contrast to other resilience interventions aimed at enhancing resilience at the individual level that use interventions with a limited perspective, the current study utilized a holistic approach to foster resilience as an integral part of daily assessment practices among medical students in their clinical years. Consequently, the purpose of applying the SAR framework is to sustain and foster resilience as part of the organization’s educational process [17, 47]. The efficacy of the intervention was verified by measuring its impact on students’ psychological parameters (resilience, academic stress, anxiety, depression, and burnout), as well as by ascertaining the perspective of medical educators who used the framework. The analysis of psychological measurements yielded statistically significant results, and the qualitative analysis of the educators’ perspectives reported positive feedback. Below, we discuss the results based on study measurement tools and support the quantitative results with qualitative findings obtained from the participating educators.
Resilience
The current study revealed that applying the SAR framework improved resilience significantly, reflecting the dramatic effect of SAR as an intervention. These findings can be explained from three aspects: (i) the approach of the SAR intervention, (ii) the nature of the guidelines, and (iii) the specific resilience measurement tool.
The SAR intervention approach is holistic and integrative. It incorporates resilience principles at multilevel steps across different stages of assessment, while simultaneously employing various preventive measures to counteract the opposite effect of anti-resilience constructs, particularly anxiety and stress. Indeed, the SAR framework utilized Huey and Palaganas [3] recommendation to combine organizational and individual factors to promote resilience in an HPE context. Furthermore, SAR promotes resilience at all stages of assessment: before, during, and after. The SAR guidelines aim to improve students’ protective factors during pre-assessment so that they can pursue the assessment with adequate resources and preparation. It has been demonstrated that providing students with adequate protective factors improves resilience [48]. During the assessment, the SAR guidelines aim to gradually expose students to uncertainty and difficulty through formative assessment or mock exams, so that they will engage in adversity but with support (feedback) to help them overcome difficulties and achieve their goals [49, 50]. They will eventually develop confidence and belief in their own abilities (self-efficacy) [51, 52]. As a result, they will be able to face similar struggles in the future [36]. The SAR framework provides opportunities for self-reflection following assessment. Students evaluate their performance based on constructive feedback, reformulate their goals [52, 53], and benefit from the experience (growth and transformation) to face future challenges [53].
The nature of SAR guidelines is to make them part of daily practice as checklists facilitating their use. Checklists act as reminders of the most crucial steps that even highly qualified professionals might forget [54]. It has been demonstrated that using checklists is an easy and effective way to boost both individual and group performance [55]. Besides using checklists, SAR provides fertile resources explaining how every guideline can be applied. The courses’ coordinators acknowledged that they were pleasantly surprised by the way SAR could be integrated into assessment practice. They also commented on the richness of the provided resources, which facilitated the use of SAR in their practice, and the positive feedback they received from students (Table 5). Therefore, SAR can be described as a proactive and supportive framework for promoting resilience [56].
The last point supporting these findings was the result of a specific resilience measurement tool, the Medical Professionals Resilience Scale (MeRS) [35]. This tool was created based on the integrated resilience model [57]. The MeRS has specific items measuring a particular resilience construct. Even though this tool was validated for practicing doctors [35], the uniqueness of the items in measuring four resilience constructs—control, resourcefulness, involvement, and growth—supported its use in the current study. Several systematic reviews have recommended that using a specific measurement tool in resilience intervention is crucial for validating the intervention’s effectiveness [19, 58, 59].
Contrasting the current findings with previous research in terms of study design and the relationship between assessment and resilience is worthwhile. In terms of using an experimental design, the current study is comparable with certain studies identified in the systematic review that was done by Cleary, Kornhaber [58] in which numerous interventional studies using single-arm pre- and post-intervention measurement were very effective in promoting resilience among health professionals, and comparable with the findings of Kunzler, Helmreich [59] meta-analysis which found that several randomized controlled trials were very effective in promoting resilience among health professionals.
Regarding those studies’ attempts to explain the relationship between assessment and resilience, Berg and Pietrasz [60] used experiential classroom exercises (competitive activities) to help students develop resilience. Similarly, Clipa et al. [16] found that students’ resilience increases when they practice formative assessment, which reduces test anxiety. Although both studies have the same findings, the intervention proposed in the current study was developed based on a solid evidence-based framework [31].
The current findings are consistent with those of Liu et al. [61], who found that resilience mediated the relationship between emotion regulation and test anxiety and discovered that developing resilience improves emotional regulation, which automatically lowers test anxiety. The current study used SAR as an intervention not only to promote resilience but also to enhance emotional regulation. The employed approach targeted individual and environmental levels at various stages of assessment: pre-, during, and post-assessment to improve emotion regulation. The SAR contains guidelines focusing on emotion regulation, such as “advising students on exam skills” and “providing strategies for students to reduce test anxiety.” These guidelines principally aim to mitigate anxiety, thus fostering resilience. Cobbinah and Amoako [62] used a non-experimental study design to show that the assessment promotes resilience by causing students to manage and cope well with academic stress caused by “the assessment” without support and guidance, whereas the current study used an empirical study design (quasi-experimental) and designed a comprehensive assessment framework to promote resilience proactively. The current study provided protective factors (resources for assessment direction and preparation). These resources serve as enablers for achieving resilience and equip students with the resources they need to face adversity. In the absence of these resources, resilience will not grow. This works in the same way that adequate nutrition does after vaccination. Nutrition strengthens the immune system in the face of the vaccine [50, 63].
Academic-related stress
The implementation of SAR significantly reduced academic stress, reflecting the effectiveness of the framework in improving psychological health. Obtaining this result may be due to the approach of the SAR framework. It adopts the implications of the transactional stress model of Lazarus and Folkman [64] and incorporates sets of guidelines at various levels to counteract stress and nurture the coping mechanisms of medical students. According to this model [64], there are three stages of stress development: (1) primary appraisal, influenced by stress antecedents; (2) secondary appraisal, influenced by stress mediators; and (3) reappraisal, influenced by stress consequences. Primary appraisal is the process by which an individual evaluates an event and decides whether it is positive, threatening (negative), or irrelevant [64]. This is influenced by personality traits (such as social evaluative trait anxiety, self-efficacy, and optimism) and environmental factors (such as the test atmosphere, the amount of social support available, and the nature of the cognitive task) [65]. The SAR framework encourages the personal traits and environment toward the positive side. It enhances self-efficacy and optimism through the frequency of formative assessment and feedback so that the students will acquire self-regulatory learning, which in turn enhances self-efficacy and optimism. Regarding the environment, it guides course coordinators to enrich the test environment with multiple factors to reduce the sources of test anxiety. The secondary appraisal appears if a negative event occurs. In this phase, the process starts when a person evaluates the resources available to deal with a situation. When a loss occurs, harm appraisal occurs. When a person anticipates harm, threat appraisal occurs; when they are confident in their ability to meet the demand of an event, challenge appraisal occurs [64]. Zeidner [65] described this psychological process as a stress mediator. The SAR framework was designed to empower the psychological process (stress mediators) so that the individual will have enough ability to appraise the harm event and overcome the loss if it occurs. This characteristic is the core of resilience [19, 30]. Reappraisal occurs when new information or resources for dealing with an event become available. It is a continuous reevaluation of the event [64, 66] influenced by individual characteristics and coping strategies [65]. The SAR is also designed to provide avenues for reappraisal and to strengthen personal characteristics and coping strategies in advance.
Another point to elucidate the findings is that the stress measurement instrument is primarily focused on academic-related stressors (ARS). ARS items are very specific to stressors arising from the academic context [37]. Because the SAR framework aims to promote resilience and simultaneously counteract other anti-resilience factors such as academic stress, the results are expected. The result is comparable with the randomized controlled trial (RCT) conducted by Yusoff and Esa [67], in which the same tool was used but the intervention was different. It was a workshop enhancing coping skills in the face of adversities. The current study utilized a holistic approach through daily practice of assessment and curriculum delivery. The SAR framework provides a range of advice on how to overcome test anxiety, how to manage time, and how to study properly (Appendix III). All these skills were utilized as system-built approaches not only to foster resilience but also to enhance the protective factors of students and enhance medical teachers’ ability to provide a safe and healthy academic environment [48]. Notably, the medical educators reported a remarkable change in the students’ behavior exemplified by their favorable attitude toward the academic environment (Table 5).
Comparing the current findings with those of other studies that used resilience-focused intervention demonstrates that resilience intervention has an enduring effect on stress that can persist for six months after intervention [19, 58, 59, 68]. The current study adds to this body of evidence by providing another empirical finding to support the nexus between reducing academic stress and improving resilience through assessment practice.
Nevertheless, the current study contradicts the findings of Lo et al. [69], who found that psychological interventions did not affect stress but that cognitive-behavioral, relaxation, and mindfulness interventions may improve the mental health of health profession students. The current study combines psychoeducation and cognitive interventions by providing students with useful links to a variety of resources based on these approaches and advising them to use them.
Anxiety
A significant reduction in anxiety symptoms was observed in the current study. This was not unexpected, as the intervention incorporates multiple components that not only reduce test anxiety and the negative impact of assessment but also reduce other anxieties arising from the burden of studying medicine, while simultaneously fostering self-efficacy, a strong predictor of resilience [51, 70].
The guidelines provide medical educators with several practical tips for students to overcome academic challenges, including exam-taking strategies and self-care techniques, as well as advice on reducing test anxiety [71].
The current findings provide additional evidence for earlier systematic reviews [3, 58, 59] that discovered a significant effect of resilience interventions in lowering anxiety among HPE students and practitioners. The current study, however, diverges from the findings of Lo et al. [69], who found that while cognitive-behavior, relaxation, and mindfulness interventions may improve the mental health of health professional students, psychoeducational interventions did not affect stress. The SAR framework encompasses guidelines targeting these previous aspects and provides students with helpful links to a range of resources based on these approaches (Appendix III).
Depression
The current study found that depressive symptoms decreased significantly after implementing SAR guidelines. The improvement in depressive symptoms may be attributed to the design of the SAR framework, which enhances resilience at multiple levels (personal and environmental) throughout the various assessment stages (pre, during, and post) [3, 50]. The SAR framework’s “assessment preparation” and “student reflection” guidelines aim to improve personal assessment behavior (Appendix III). During SAR implementation, students were advised to prepare thoroughly for the exam and were given strategies for improving self-care and reducing test anxiety. Furthermore, the other SAR guidelines, particularly “assessment direction” and “assessment experience,” focus on the assessment organizational process to boost motivation and self-efficacy. These can lead to a reduction in “rumination,” a cognitive response style that consists of a vicious cycle of ruminating on negative thoughts [72]. Regarding this quantitative finding, course coordinators supported it by observing and reporting that mental health improved after SAR implementation (Table 5).
The current study is comparable to a randomized controlled trial confined to a single medical school in which researchers used a workshop-based intervention to promote the mental health of students, and the results demonstrated a significant reduction in depressive symptoms [67]. Furthermore, this study is consistent with Kunzler, Helmreich [59] systematic review, which found that resilience interventions result in improving depression with a low effect size. It is worth noting that the systematic review by Cleary, Kornhaber [58] revealed that some interventional studies improved depression, but not resilience. They attributed this outcome to the nature of the intervention, which focused on specific psychological problems, such as depression, while ignoring other crucial constructs, such as resilience. The current intervention addressed both concepts—depression and resilience—demonstrating its strength as a comprehensive and holistic approach.
Burnout
Three types of burnout were measured in the current study—personal, work (academic), and client (patients). Personal and work-related (academic) burnout were significantly reduced by the use of SAR guidelines, which is consistent with the findings of two RCTs that found a significant decline in burnout following resilience intervention [73, 74]. This could be explained by the reciprocal mediating effect between resilience and burnout [4, 75, 76]. Moreover, the SAR guidelines were intended to improve personal and occupational factors (academic environment). SAR includes several guidelines aimed at personal factors, such as self-efficacy and motivation, as well as guidelines aimed at mitigating the negative effects of the academic environment, particularly the exam-related environment (Appendix III). As a result of implementing the SAR guidelines (personal and academic environment), resilience increased while burnout declined.
The factor that contributes to burnout reduction is the use of SAR guidelines at the process and organizational levels of an assessment (pre, intra, and post). Multiple meta-analyses have found that organizationally targeted interventions have a greater effect size than individually targeted interventions [8, 77,78,79]. This further supports the argument that burnout is likelier to be caused by organizational deficiencies than by individual factors [8, 77]. This effect is clearly described by medical educators who observed that students were significantly more engaged in clinical rotations when SAR was utilized than in rotations when it was not (Table 5).
Client-related burnout did not differ significantly between pre- and post-intervention measures. This could be explained by the fact that participants who had just begun their clinical rotation lacked the full authority to interact with patients and make clinical decisions. These actions were performed by clinicians, so students were not yet exposed to hospital-related burnout [8, 10].
Correlation among study tools
The correlation analysis of study tools in pre- and post-intervention elucidates the dynamic interplay between resilience and psychological stress indicators such as depression, anxiety, stress, and burnout among participants before and after the intervention. We discovered a significant negative correlation between resilience and these indicators, highlighting resilience’s critical role in protecting against psychological distress. Such findings are consistent with prior research by Hayat, Choupani [51], Putwain, Becker [80], which suggest that enhancing resilience can significantly mitigate the adverse effects of stress, anxiety, and depression.
The practical implications of these insights are profound. They suggest that interventions aimed at bolstering resilience may be effective strategies for reducing psychological distress. In educational settings, this could translate to a resilience-built-in system designed to equip students with coping mechanisms, thereby enhancing their well-being and academic performance.
Regarding the strong correlation of anxiety, depression, stress, and burnout that was noticed in this study, a previous systematic review by Koutsimani, Montgomery [78] found that such psychological constructs are highly correlated even when using different scales.
Nevertheless, the current study has several strengths, one of which is that it used an experimental design with pre- and post-intervention evaluations. The timing of the study intervention was optimal, as it occurred in the middle of the academic year when stress levels were at their peak [7]. This underscores its effectiveness. Moreover, it was evident that these guidelines are user-friendly and self-explanatory. In addition to providing a system-integrated approach to promoting resilience, the study also includes tools for assessing resilience levels along with other counteracting factors.
On the other hand, the study has some limitations. One of these is that a comparative control group is impractical because preventing intervention leakage cannot be guaranteed in a single-institution study. Additional research that includes a control group is necessary to evaluate the efficacy of the SAR framework. Another challenge was that follow-up measurements were not conducted due to logistical constraints. After implementing the intervention, multiple measurements should be taken in a future study. Additionally, qualitative feedback was gathered from five course coordinators, rendering the sample size insufficient for achieving saturation in a qualitative study. Future research should aim to include an acceptable sample size for the qualitative evaluation of the study. Finally, it was limited to a single institution and the sample size is small; further study including multicenter research with large sample size is suggested.
Based on the findings of the current study, the researchers propose several recommendations. First, it is strongly recommended that the SAR guidelines be incorporated into medical and HPE curricula daily due to their clarity, practicability, and feasibility. Teachers in the medical and HPE fields should be encouraged to utilize them and be provided training to ensure their proper application. Second, in the “new normal” following the COVID-19 pandemic and the massive transformations it occasioned, nearly all medical schools have adopted blended learning. It is feasible to apply the SAR framework with this modification. E-learning platforms are fertile ground for employing SAR guidelines and their associated resources, and students would have unlimited access to them. Additionally, these resources are simple to expand and update regularly. Finally, the nature of SAR guidelines is not limited to medical and HPE students; they can be applied to students in other disciplines in higher education, and even to students in secondary and elementary schools.
Conclusion
Resilience is a crucial attribute for students in the medical and health professions as it fosters the traits that graduates need to face future adversities. The current study presents a distinctive intervention using a quasi-experimental design with one group pre- and post-test for fostering resilience while simultaneously practicing the assessment. It uses what is called systematic assessment for resilience (SAR) to enhance resilience through a holistic approach across multiple levels. Comparing the results of pre- and post-intervention measurements yielded astounding results and showed significant improvement in resilience and a significant reduction in counteracting psychological parameters, such as stress, anxiety, depression, and burnout; thus, this study provides evidence-based guidance on how to promote resilience within an educational setting. By using this novel approach, the SAR framework, this research opens a new horizon for nurturing the mental well-being of future doctors who will provide better healthcare services to ensure patient safety. Future research is needed to monitor the impact of the SAR framework over time and broaden the scope of the intervention by including other HPE fields and students in higher education.
Data availability
Please email the corresponding author for a link to the de-identified datasets. However, due to privacy concerns, the in-depth interview transcripts are unavailable to the general public.
Abbreviations
- ARS:
-
Academic Related Stressors
- CBI:
-
Copenhagen Burnout Inventory
- CI:
-
Confidence interval
- DASS-21:
-
Depression, Anxiety and Stress Scale 21
- df:
-
Degree of freedom
- DOCEE:
-
Direct Observation of the Clinical Examination Encounter
- HPE:
-
Health Professions Education
- IQR:
-
Inter Quartile Range
- MeRS:
-
Medical Professionals Resilience Scale
- MSSQ:
-
Medical Students Stressor Questionnaire
- RCT:
-
Randomized Control Trials
- SAR:
-
Systematic Assessment for Resilience
- SD:
-
Standard deviation
- SPSS:
-
Statistical Package for Social Sciences
References
Slavin SJ, Schindler DL, Chibnall JT. Acad Med. 2014;89(4). https://doi.org/10.1097/ACM.0000000000000166. Medical Student Mental Health 3.0: Improving Student Wellness Through Curricular Changes.
Banks J, Smyth E. Your whole life depends on it’: academic stress and high-stakes testing in Ireland. J Youth Stud. 2015;18(5):598–616. https://doi.org/10.1080/13676261.2014.992317.
Huey CWT, Palaganas JC. What are the factors affecting resilience in health professionals? A synthesis of systematic reviews. Med Teach. 2020;42(5):550–60. https://doi.org/10.1080/0142159X.2020.1714020.
Yusoff MSB. Promoting resilience and minimizing burnout. In: Marcus A, Henning CU, Krägeloh R, Dryer F, Moir R, Hill B AG, editors. Wellbeing in Higher Education: cultivating a healthy lifestyle among Faculty and Students. New York: Routledge; 2018. pp. 82–105.
Moir F, Yielder J, Sanson J, Chen Y. Depression in medical students: current insights. Adv Med Educ Pract. 2018;9:323–33. https://doi.org/10.2147/AMEP.S137384.
Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of Depression, anxiety, and other indicators of psychological distress among U.S. and Canadian Medical Students. Acad Med. 2006;81(4):354–73. https://doi.org/10.1097/00001888-200604000-00009.
Yusoff MSB. Interventions on medical students’ psychological health: a meta-analysis. J Taibah Univ Med Sci. 2014;9(1):1–13. https://doi.org/10.1016/j.jtumed.2013.09.010.
Erschens R, Keifenheim KE, Herrmann-Werner A, Loda T, Schwille-Kiuntke J, Bugaj TJ, et al. Professional burnout among medical students: systematic literature review and meta-analysis. Med Teach. 2019;41(2):172–83. https://doi.org/10.1080/0142159X.2018.1457213.
Mao Y, Zhang N, Liu J, Zhu B, He R, Wang X. A systematic review of depression and anxiety in medical students in China. BMC Med Educ. 2019;19(1):327. https://doi.org/10.1186/s12909-019-1744-2.
Frajerman A, Morvan Y, Krebs M-O, Gorwood P, Chaumette B. Burnout in medical students before residency: a systematic review and meta-analysis. Eur Psychiatry. 2019;55:36–42. https://doi.org/10.1016/j.eurpsy.2018.08.006.
Ribeiro ÍJS, Pereira R, Freire IV, de Oliveira BG, Casotti CA, Boery EN. Stress and quality of life among University students: a systematic literature review. Health Professions Educ. 2018;4(2):70–7. https://doi.org/10.1016/j.hpe.2017.03.002.
Chisholm-Burns MA, Berg-Poppe P, Spivey CA, Karges-Brown J, Pithan A. Systematic review of noncognitive factors influence on health professions students’ academic performance. Adv Health Sci Educ. 2021. https://doi.org/10.1007/s10459-021-10042-1.
Ragab EA, Dafallah MA, Salih MH, Osman WN, Osman M, Miskeen E, et al. Stress and its correlates among medical students in six medical colleges: an attempt to understand the current situation. Middle East Curr Psychiatry. 2021;28(1):75. https://doi.org/10.1186/s43045-021-00158-w.
Wadi M, Yusoff MSB, Abdul Rahim AF, Lah NAZN. Factors affecting test anxiety: a qualitative analysis of medical students’ views. BMC Psychol. 2022;10(1):8. https://doi.org/10.1186/s40359-021-00715-2.
Soares D, Woods K. An international systematic literature review of test anxiety interventions 2011–2018. Pastoral Care Educ. 2020;1–24. https://doi.org/10.1080/02643944.2020.1725909.
Clipa O, Duca DS, Padurariu G. Test anxiety and student resilience in the context of School Assessment. Revista Romaneasca Pentru Educatie Multidimensionala. 2021;13(1Sup1):299–314. https://doi.org/10.18662/rrem/13.1Sup1/397.
Wadi MM, Rahim AFA, Yusoff MSB. Infusing resilience into Assessment system. Educ Med J. 2020;12(1):1–5. https://doi.org/10.21315/eimj2020.12.1.1.
Schwarz S. Resilience in psychology: a critical analysis of the concept. Theory Psychol. 2018;28(4):528–41. https://doi.org/10.1177/0959354318783584.
Chmitorz A, Kunzler A, Helmreich I, Tüscher O, Kalisch R, Kubiak T, et al. Intervention studies to foster resilience – a systematic review and proposal for a resilience framework in future intervention studies. Clin Psychol Rev. 2018;59:78–100. https://doi.org/10.1016/j.cpr.2017.11.002.
Joyce S, Shand F, Tighe J, Laurent SJ, Bryant RA, Harvey SB. Road to resilience: a systematic review and meta-analysis of resilience training programmes and interventions. BMJ open. 2018;8(6):e017858. https://doi.org/10.1136/bmjopen-2017-017858.
Garcia-Dia MJ, DiNapoli JM, Garcia-Ona L, Jakubowski R, O’Flaherty D. Concept analysis: resilience. Arch Psychiatr Nurs. 2013;27(6):264–70. https://doi.org/10.1016/j.apnu.2013.07.003.
Lee JH, Nam SK, Kim AR, Kim B, Lee MY, Lee SM. Resilience: a meta-analytic approach. J Couns Dev. 2013;91(3):269–79. https://doi.org/10.1002/j.1556-6676.2013.00095.x.
Windle G. What is resilience? A review and concept analysis. Reviews Clin Gerontol. 2011;21(2):152–69. https://doi.org/10.1017/S0959259810000420.
Yusoff MSB. What does it take to Minimise Burnout and Build Resilience of Healthcare Learners? In: Sky WHY, editor. Preparing Healthcare Learners for a changing World. Hong Kong: University of Hong Kong; 2019.
Ye W, Strietholt R, Blömeke S. Academic resilience: underlying norms and validity of definitions. Educational Assess Evaluation Account. 2021;33(1):169–202. https://doi.org/10.1007/s11092-020-09351-7.
García-Crespo FJ, Fernández-Alonso R, Muñiz J. Academic resilience in European countries: the role of teachers, families, and student profiles. PLoS ONE. 2021;16(7):e0253409. https://doi.org/10.1371/journal.pone.0253409.
Martin A. Motivation and academic resilience: developing a model for Student Enhancement. Australian J Educ. 2002;46(1):34–49. https://doi.org/10.1177/000494410204600104.
Richardson GE. The metatheory of resilience and resiliency. J Clin Psychol. 2002;58(3):307–21. https://doi.org/10.1002/jclp.10020.
Luthar SS, Cicchetti D, Becker B. The Construct of Resilience: a critical evaluation and guidelines for future work. Child Dev. 2000;71(3):543–62. https://doi.org/10.1111/1467-8624.00164.
Sanderson B, Brewer M. What do we know about student resilience in health professional education? A scoping review of the literature. Nurse Educ Today. 2017;58:65–71. https://doi.org/10.1016/j.nedt.2017.07.018.
Wadi MM, Yusoff MSB, Taha MH, Shorbagi S, Nik Lah NAZ, Abdul Rahim AF. The framework of systematic Assessment for Resilience (SAR): development and validation. BMC Med Educ. 2023;23(1):213. https://doi.org/10.1186/s12909-023-04177-5.
University of Sharjah. BACHELOR OF MEDICINE AND BACHELOR OF SURGERY (MBBS). https://www.sharjah.ac.ae/en/academics/Colleges/Medicine/Pages/Bachelor-of-Medicine-and-Bachelor-of-Surgery.aspx 2022 [.
Creswell JW. Experimental desgins. Educational Research: planning, conducting, and evaluating quantitative and qualitative research. England: Pearson Education; 2012.
Tavakol M, Sandars J. Quantitative and qualitative methods in medical education research: AMEE Guide 90: part I. Med Teach. 2014;36(9):746–56. https://doi.org/10.3109/0142159X.2014.915298.
Rahman MA, Yusoff MSB, Roslan NS, Mohammad JA-M, Ahmad A. Development and validation of the medical professionals resilience scale. BMC Health Serv Res. 2021;21(1):482. https://doi.org/10.1186/s12913-021-06542-w.
Wadi M, Nordin NI, Roslan NS, Celina T, Yusoff MSB. Reframing Resilience Concept: insights from a Meta-synthesis of 21 resilience scales. Educ Med J. 2020;12(2). https://doi.org/10.21315/eimj2020.12.2.2.
Yusoff MSB, Rahim AFA, Yaacob MJ. The development and validity of the Medical Student Stressor Questionnaire (MSSQ). ASEAN Journal of Psychiatry. 2010;11(1):231-5. https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=4c7e3c6a2948bd424adec12e067eb1b9cd4d8f58
Dagani J, Buizza C, Ferrari C, Ghilardi A. Psychometric validation and cultural adaptation of the Italian medical student stressor questionnaire. Curr Psychol. 2022;41(6):4132–40. https://doi.org/10.1007/s12144-020-00922-x.
Jayarajah U, Lakmal K, Athapathu A, Jayawardena AJ, de Silva V. Validating the Medical Students’ Stressor Questionnaire (MSSQ) from a Sri Lankan medical faculty. J Taibah Univ Med Sci. 2020;15(5):344–50. https://doi.org/10.1016/j.jtumed.2020.08.003.
Zanon C, Brenner RE, Baptista MN, Vogel DL, Rubin M, Al-Darmaki FR, et al. Examining the dimensionality, reliability, and Invariance of the Depression, anxiety, and stress Scale–21 (DASS-21) across eight countries. Assessment. 2020;28(6):1531–44. https://doi.org/10.1177/1073191119887449.
Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression anxiety stress scales (DASS) with the Beck Depression and anxiety inventories. Behav Res Ther. 1995;33(3):335–43. https://doi.org/10.1016/0005-7967(94)00075-U.
Bibi A, Lin M, Zhang XC, Margraf J. Psychometric properties and measurement invariance of Depression, anxiety and stress scales (DASS-21) across cultures. Int J Psychol. 2020;55(6):916–25. https://doi.org/10.1002/ijop.12671.
Kristensen TS, Borritz M, Villadsen E, Christensen KB. The Copenhagen Burnout Inventory: a new tool for the assessment of burnout. Work Stress. 2005;19(3):192–207. https://doi.org/10.1080/02678370500297720.
Moser CM, Tietbohl-Santos B, Arenas DL, Xavier A, Ornell F, Borges RB, et al. Psychometric properties of the Brazilian Portuguese version of the Copenhagen Burnout Inventory (CBI) in healthcare professionals. Trends Psychiatry Psychother. 2023;45:e20210362. https://doi.org/10.47626/2237-6089-2021-0362.
Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Res Psychol. 2006;3(2):77–101. https://doi.org/10.1191/1478088706qp063oa.
Guba EG. Criteria for assessing the trustworthiness of naturalistic inquiries. ECTJ. 1981;29(2):75–91. https://doi.org/10.1007/BF02766777.
Rogers D. Which educational interventions improve healthcare professionals’ resilience? Med Teach. 2016;38(12):1236–41. https://doi.org/10.1080/0142159X.2016.1210111.
Fletcher D, Sarkar M, Psychological, Resilience. Eur Psychol. 2013;18(1):12–23. https://doi.org/10.1027/1016-9040/a000124.
Martin AJ, Marsh HW. Academic buoyancy: towards an understanding of students’ everyday academic resilience. J Sch Psychol. 2008;46(1):53–83. https://doi.org/10.1016/j.jsp.2007.01.002.
Howe A, Smajdor A, Stöckl A. Towards an understanding of resilience and its relevance to medical training. Med Educ. 2012;46(4):349–56. https://doi.org/10.1111/j.1365-2923.2011.04188.x.
Hayat A, Choupani H, Dehsorkhi H. The mediating role of students’ academic resilience in the relationship between self-e cacy and test anxiety. J Educ Health Promotion. 2021;10(1):297. https://doi.org/10.4103/jehp.jehp_35_21.
Panadero E, Broadbent J, Boud D, Lodge JM. Using formative assessment to influence self- and co-regulated learning: the role of evaluative judgement. Eur J Psychol Educ. 2019;34(3):535–57. https://doi.org/10.1007/s10212-018-0407-8.
Nicol D. The power of internal feedback: exploiting natural comparison processes. Assess Evaluation High Educ. 2021;46(5):756–78. https://doi.org/10.1080/02602938.2020.1823314.
Gawande A. The Checklist Manifesto: how to get things right. New York: Metropolitan Books; 2009.
Boritz JE, Timoshenko LM. On the Use of checklists in auditing: a Commentary. Curr Issues Auditing. 2014;8(1):C1–25. https://doi.org/10.2308/ciia-50741.
Jones E, Priestley M, Brewster L, Wilbraham SJ, Hughes G, Spanner L. Student wellbeing and assessment in higher education: the balancing act. Assess Evaluation High Educ. 2020;1–13. https://doi.org/10.1080/02602938.2020.1782344.
Wadi M, Nordin NI, Syazni N, Roslan TC, Yusoff MSB. Reframing Resilience Concept: insights from a Meta-synthesis of 21 resilience scales. Educ Med J. 2020;12(2):3–22. https://doi.org/10.21315/eimj2020.12.2.2.
Cleary M, Kornhaber R, Thapa DK, West S, Visentin D. The effectiveness of interventions to improve resilience among health professionals: a systematic review. Nurse Educ Today. 2018;71:247–63. https://doi.org/10.1016/j.nedt.2018.10.002.
Kunzler AM, Helmreich I, Chmitorz A, König J, Binder H, Wessa M et al. Psychological interventions to foster resilience in healthcare professionals. Cochrane Database Syst Reviews. 2020(7). https://doi.org/10.1002/14651858.CD012527.pub2.
Berg P, Pietrasz C. Turning Classroom failure into Student Success: the value of integrating Resiliency Building activities in the Academic Classroom. Manage Teach Rev. 2017;2(4):299–311. https://doi.org/10.1177/2379298117710780.
Liu Y, Pan H, Yang R, Wang X, Rao J, Zhang X, et al. The relationship between test anxiety and emotion regulation: the mediating effect of psychological resilience. Ann Gen Psychiatry. 2021;20(1):40. https://doi.org/10.1186/s12991-021-00360-4.
Cobbinah A, Amoako I. Hidden curriculum: the impact of Assessment on Students’ Self-regulated learning and resilience. Can J Educational Social Stud. 2021;1(2):29–42. https://doi.org/10.53103/cjess.v1i2.13.
Martin AJ, Marsh HW. Academic resilience and academic buoyancy: multidimensional and hierarchical conceptual framing of causes, correlates and cognate constructs. Oxf Rev Educ. 2009;35(3):353–70. https://doi.org/10.1080/03054980902934639.
Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer; 1984.
Zeidner M. Test anxiety: the state of the art. New York: Kluwer Academic; 1998.
Smith RJ, Arnkoff DB, Wright TL. Test anxiety and academic competence: a comparison of alternative models. J Couns Psychol. 1990;37(3):313–21. https://doi.org/10.1037/0022-0167.37.3.313.
Yusoff MSB, Esa AR. A DEAL-based intervention for the reduction of depression, denial, self-blame and academic stress: a randomized controlled trial. J Taibah Univ Med Sci. 2015;10(1):82–92. https://doi.org/10.1016/j.jtumed.2014.08.003.
Yusufov M, Nicoloro-SantaBarbara J, Grey NE, Moyer A, Lobel M. Meta-analytic evaluation of stress reduction interventions for undergraduate and graduate students. Int J Stress Manage. 2019;26(2):132. https://doi.org/10.1037/str0000099.
Lo K, Waterland J, Todd P, Gupta T, Bearman M, Hassed C, et al. Group interventions to promote mental health in health professional education: a systematic review and meta-analysis of randomised controlled trials. Adv Health Sci Educ. 2018;23(2):413–47. https://doi.org/10.1007/s10459-017-9770-5.
von der Embse N, Jester D, Roy D, Post J. Test anxiety effects, predictors, and correlates: a 30-year meta-analytic review. J Affect Disord. 2018;227:483–93. https://doi.org/10.1016/j.jad.2017.11.048.
Poorman SG, Mastorovich ML, Gerwick M. Interventions for test anxiety: how Faculty can help. Teach Learn Nurs. 2019;14(3):186–91. https://doi.org/10.1016/j.teln.2019.02.007.
Nolen-Hoeksema S. Responses to depression and their effects on the duration of depressive episodes. J Abnorm Psychol. 1991;100(4):569. https://doi.org/10.1037/0021-843X.100.4.569.
Mache S, Baresi L, Bernburg M, Vitzthum K, Groneberg D. Being prepared to work in Gynecology Medicine: evaluation of an intervention to promote junior gynecologists professionalism, mental health and job satisfaction. Arch Gynecol Obstet. 2017;295(1):153–62. https://doi.org/10.1007/s00404-016-4223-6.
Lanz JJ. Evidence-based resilience intervention for nursing students: a Randomized Controlled Pilot Trial. Int J Appl Posit Psychol. 2020;5(3):217–30. https://doi.org/10.1007/s41042-020-00034-8.
García-Izquierdo M, Ríos-Risquez MI, Carrillo-García C, Sabuco-Tebar, EdlÁ. The moderating role of resilience in the relationship between academic burnout and the perception of psychological health in nursing students. Educational Psychol. 2018;38(8):1068–79. https://doi.org/10.1080/01443410.2017.1383073.
Cheng J, Zhao YY, Wang J, Sun YH. Academic burnout and depression of Chinese medical students in the pre-clinical years: the buffering hypothesis of resilience and social support. Psychol Health Med. 2020;25(9):1094–105. https://doi.org/10.1080/13548506.2019.1709651.
Panagioti M, Panagopoulou E, Bower P, Lewith G, Kontopantelis E, Chew-Graham C, et al. Controlled interventions to reduce burnout in Physicians: a systematic review and Meta-analysis. JAMA Intern Med. 2017;177(2):195–205. https://doi.org/10.1001/jamainternmed.2016.7674.
Koutsimani P, Montgomery A, Georganta K. The Relationship between Burnout, Depression, and anxiety: a systematic review and Meta-analysis. Front Psychol. 2019;10(284). https://doi.org/10.3389/fpsyg.2019.00284.
West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;388(10057):2272–81. https://doi.org/10.1016/S0140-6736(16)31279-X.
Putwain DW, Becker S, Symes W, Pekrun R. Reciprocal relations between students’ academic enjoyment, boredom, and achievement over time. Learn Instruction. 2018;54:73–81. https://doi.org/10.1016/j.learninstruc.2017.08.004.
Acknowledgements
Authors extend the deepest gratitude to the clerkship courses’ coordinators who participated in this study, dedicating their valuable time and providing essential insights that significantly enriched our research. Their cooperation and enthusiastic engagement were crucial in the successful completion of the data collection process. We also wish to thank the students at the College of Medicine, University of Sharjah, for their active participation and contributions. Their involvement was instrumental in enhancing the depth and breadth of our study. This work could not have been accomplished without the collective efforts of all parties involved.
Funding
This research is part of a larger project supported by Fundamental Research Grant Scheme (FRGS: 203.PPSP.6171219), Ministry of Education, Malaysia.
Author information
Authors and Affiliations
Contributions
Each author has a substantial contribution in this paper. MW, MSBY, and AS initiated the research idea and wrote the research proposal. MW established the training program for the medical teachers. AS, SS and MHT collected data pre and post the training. MW and MHT analyze data. MW initiated writing the paper. Both MW and AS has refined the paper. MHT, SS and MSBY reviewed it carefully before submission.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study has received ethical approval (no. REC-21-11-03) from the Research Ethics Committee of the University of Sharjah, which followed the Belmont Report and Helsinki Declaration. All participants signed a written informed consent form containing clear information about the study’s purpose, methods, and secure data handling. They were also informed that they could withdraw from the study verbally or in writing. The standard rules for privacy and confidentiality were followed when conducting the study. Anonymity was maintained for participants for Year 4 clerkship rotations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wadi, M., Shorbagi, A., Shorbagi, S. et al. The impact of the Systematic Assessment for Resilience (SAR) framework on students’ resilience, anxiety, depression, burnout, and academic-related stress: a quasi-experimental study. BMC Med Educ 24, 506 (2024). https://doi.org/10.1186/s12909-024-05444-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-024-05444-9