
Abstract
Background
Emotional intelligence (EI) is a predictive factor of academic success in undergraduate Doctor of Medicine (MD) programs. Although some research suggests a positive association between EI and academic success in MD programs, other research reports neither an association nor a negative correlation between the two variables. The current study aimed to resolve these contradictory findings by conducting a systematic review and a meta-analysis using research from 2005 to 2022.
Methods
Data were analyzed using a multilevel modeling approach to (a) estimate the overall relationship between EI and academic success in MD programs and (b) determine whether the mean effect size varies according to country (United States vs. non-United States countries), age, EI test, EI task nature (ability-based vs. trait-based), EI subscales, and academic performance criteria (grade point average vs. examinations).
Results
Findings from 20 studies (m = 105; N = 4,227) indicated a positive correlation between EI and academic success (r = .13, 95% CI [.08, – .27], p < .01). Moderator analyses indicated that the mean effect size significantly varied according to EI tests and EI subscales. Moreover, three-level multiple regression analyses showed that between-study variance explained 29.5% of the variability in the mean effect size, whereas within-study variance explained 33.5% of the variability in the mean effect.
Conclusions
Overall, the current findings show that EI is significantly, albeit weakly, related to academic success in MD programs. Medical researchers and practitioners can therefore focus on integrating EI-related skills into the MD curriculum or target them through professional development training and programs.
Similar content being viewed by others


Background
Which factors predict academic success in undergraduate medical programs? While some students perform well in Doctor of Medicine (MD) programs, others fail to complete their studies or struggle in their MD journey. Moreover, the current competencies and expectations of undergraduate medical students differ from those of the last 20 to 30 years [1], which highlights the significance of revising the admission criteria for such programs [2]. Numerous research studies in medical education have evaluated the admission criteria as determinants of academic success for MD students. Over the last two decades, medical education researchers have attempted to test the association between academic success and factors, such as metacognitive awareness [3, 4], motivation [5*, 6, 7], coping strategy [8, 9], learning style [10, 11], educational environment [12], critical thinking [13, 14], and Emotional Intelligence (EI) [15*, 16*, 17]. In this study, we have comprehensively investigated EI as the variable of interest.
Although the notion of EI was first discussed by Edward Thorndike in the 1920s when he conceptualized intelligence as a multidimensional rather than unidimensional construct, including mechanical, abstract, and social intelligence, it was Salovey and Mayer’s seminal work that contributed to the systematic and scientific study of EI [18]. Since then, other theories and models of EI such as Bar-On’s model [19] and Goleman’s model [20] have been introduced. EI has been extensively researched in different fields including sports, education, music, and medicine [21,22,23,24]. It is increasingly becoming important in the medical profession because success in this field is not only determined by knowledge and academic excellence but also the acquisition of EI-related skills such as empathy, communication, interpersonal sensitivity, and emotion recognition [16*]. Doctors manage different kinds of patients with varying socioeconomic status, and diverse case severity that range from mild to critical illnesses, which requires an understanding of patients’ emotions, ability to demonstrate empathy, and in some instances, communicate bad news in a professional way.
Interest in studying the association between EI and academic success in MD programs arose in the first decade of the twenty-first century. Notably, a literature review on the predictors of academic success in medical schools revealed that EI is one of the most studied variables, with three systematic reviews published on this topic [17, 25, 26]. One of the major findings of these systematic reviews was that primary studies reported contradictory findings. For instance, Singh, Kulkarni, and Gupta [17] reported that eight studies concluded that EI has a positive impact on academic success, two studies showed nonsignificant associations between EI and academic success, and 11 studies showed a negative relationship between EI and academic success. A similar conclusion was reached by Arora et al. [25] and Cook, Cook, and Hilton [26]. Although systematic reviews offer valuable source information for researchers regarding the effectiveness of an intervention, the difference between two or more groups for a specific variable, and the association between different factors, they do not provide quantitative and reliable results. Therefore, one of the objectives of the current study is to synthesize the effect sizes stemming from primary studies using a multilevel meta-analysis approach to clarify the nature and magnitude of the relationship between EI and academic success in MD programs. The second objective is to identify factors that may contribute to the contradictory findings in primary studies (see Table 1).
The next section sheds light on possible sources of inconsistency in the primary research based on reviewing the literature on the association between EI and academic success.
Sources of inconsistency and the need for a quantitative synthesis
Previous meta-analyses on EI provide some explanations for the inconsistent findings in the primary studies. These include culture or country, age, gender, EI tests, EI subscales, and EI task nature (ability-based vs trait-based assessments; [21, 46, 47]). These factors have been recognized in previous studies that assessed the association between EI and academic success in MD programs (see Table 1). For example, Brannick et al. [33*] reported that there was no significant correlation between a trait-based EI scale (Wong and Lu EI Scale; WLEIS) and academic performance, while an ability-based EI test (i.e., Mayer–Salovey–Caruso Emotional Intelligence Test; MSCEIT) was significantly correlated with academic performance. By contrast, some studies identified a significant relationship between academic performance and some of the EI subscales (e.g., optimism, awareness of emotions, and attention to feelings), no significant correlations were observed between academic performance and other EI subscales (e.g., [16*, 35*]). This study deviates from previous literature in its definition of academic success. While some studies assessed academic success using students’ grade point average (GPA; [30*, 31*, 33*]), others used unit/achievement tests (e.g., Austin et al. [23*]; Chew, Zain, and Hassan [32*]; Rajasingam et al. [37*]). Therefore, in addition to the advantage of using a multilevel meta-analysis in addressing the nested data (e.g., unit and finaltest scores are nested in/within GPA), the difference in academic performance criteria was included as a possible moderator that could explain the variability in the mean effect. The effect of culture on EI variance has also been recognized [48]. The current study included works that represented 10 countries in four different continents (North America, Europe, Asia, and Australia; see Table 1). Finally, some studies showed a link between EI and age [49, 50]. All the above factors were considered in the current study to possibly explain the variability in the mean effect size.
Research questions
Based on the above literature review, this study aims to answer the following research questions:
-
1.
What is the nature and magnitude of the relationship between EI and academic success in undergraduate medical programs?
-
2.
Do moderators such as country, age, EI test, EI task nature, EI subscale, and academic performance criteria explain the variability in reported results in previous studies on the relationship between EI and academic success in undergraduate medical programs?
Methods
Search strategy
Potential studies were identified by searching the following databases: ScienceDirect, ProQuest Central, ProQuest Digital Dissertation, Academic Search Complete, ERIC, Access Medicine, Medline, and PsycINFO up to December 2022. The following keywords were searched in the titles and abstracts: (“emotional intelligence”) AND (“medical students” OR “medical school”) AND (“academic success” OR “performance” OR “GPA”). Moreover, the authors reviewed the reference lists of the three systematic reviews conducted on the same topic [17, 25, 26]. This search resulted in locating 180 works. After eliminating duplicates, we obtained 123 items (113 journal articles, 7 reports, 1 magazine, 1 conference material, and 1 dissertation).
Selection process
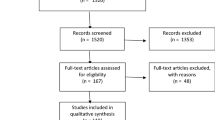
Research studies were selected according to PRISMA guidelines [51]. Five criteria were applied to these 123 works: First, only articles written in English were included. Second, they must report sufficient statistics to calculate the effect size (Pearson’s r). Third, they must examine the association between EI as assessed by several well-known EI tests and scales and academic success/achievement defined in terms of GPA or achievement examination(s). Fourth, the search included both published and unpublished works; however, only one dissertation was found, which was excluded because it assessed the relationship between EI and leadership [52]. Finally, we only included studies that were conducted with undergraduate medical students pursuing their MD program. All studies conducted on graduate medical students or nursing students were excluded [53, 54]. Applying these criteria brought the number down to 20 studies published between January 2005Footnote 1 to December 2021 (see Fig. 1).

Flowchart for selection of studies
Data collection
A coding book, which included information about the study variables and the special code for each level of categorical variables, was created (see Table 2). The first and second authors met to discuss the coding and clarify any issues before starting the independent coding in the coding sheet. In addition to coding the study moderators, the two coders independently retrieved the effect size (i.e., Pearson correlation) and the sample size associated with it. A column for notes was included for the coders to make any comments. The two-way interclass correlation coefficient was high (r = 0.93 [55]). All cases with disagreement were individually revisited and resolved by consensus. The data are available on request from the authors.
Effect size calculation and statistical analyses
All included studies reported the Pearson product-moment correlation coefficient (r). As the Pearson correlation is not normally distributed, each effect size was converted to Fisher’s z (see Borenstein and Hedges [56] for transformation equations/formulas).
As most of the studies reported more than one effect size (e.g., an effect size per EI subscale or for each EI test), a three-level meta-analysis approach was adopted, which also considered the various assessments of academic performance. Level 1 referred to the sampling error, Level 2 referred to the between-studies variance, and Level 3 referred to the across-studies variance. All multilevel analyses were conducted using SAS® Studio. The full codes for running analyses can be found in Van den Noortgate et al. [57]. The equations for the full model (without adding moderators) and the full model (where all moderators are included) can be found in Konstantopoulos [58].
Heterogeneity analysis
There are several methods for estimating heterogeneity in meta-analyses including Q, I 2, and T 2 statistics. In the current study, both Q and I 2 statistics were computed. The Q-statistic follows a chi-squared distribution with degrees of freedom equal to the number of effect sizes/studies minus 1, and it is defined as “the sum of squared deviations of each observed effect from the mean effect on a standardized scale” [59]. I 2-statistic refers to the proportion of the observed variance. The equations for calculating the Q- and I 2-statistic are presented in Borenstein et al. [59].
Assessing publication bias
Three methods of assessing publication bias were used in this study: the funnel plot, Egger’s test, and the Begg and Mazumdar correlation test. The funnel plot is a visual representation, which assumes that in the absence of publication bias, the mean effect size is expected to be the same in small and in large studies [60]. Egger’s test is a parametric test that assesses the funnel plot asymmetry based on linear regression analysis. A significant t-test result indicates that publication bias may exist. Finally, Begg and Mazumdar’s test is a nonparametric correlation test that assesses whether there is a relationship between the study size and effect size [61].
Results
Figure 2 shows the funnel plot for precision. Egger’s regression test was not significant, b = -0.59, SE = 0.67, p = 0.18. In addition, Begg and Mazumdar’s correlation test was not significant, τ = -0.02, zτ = 0.41, p = 0.34. These results show that publication bias did not affect the results.

Funnel plot of precision by Fisher’s z
The effect size values ranged between -0.21 and 0.51. To estimate the mean effect size, results from 20 studies (m = 105; N = 4,227) indicated that, overall, there is a significant positive correlation between EI and academic success, r = 0.13, 95% CI [0.08, – 0.27], p < 0.01. The within-study variance (Level-2) as well as the between-study variance (Level-3) were both statistically significant (Level-2 = 0.005, SE = 0.002, z = 1.70, p = 0.04; Level-3 = 0.006, SE = 0.001, z = 3.29, p < 0.001). Level 3 explained 29.5% of the variability in the mean effect, whereas Level 2 explained 33.5%. Together, Levels 2 and 3 explained 63% of the variability in the mean effect. As expected, a high heterogeneity was observed, Q(105) = 375.48, p < 0.001, I 2 = 72.04.
Moderator analysis showed that the mean effect size significantly varied according to the EI test, Q(3) = 42.93, p < 0.001, and EI subscale, Q(3) = 18.87, p = 0.04, whereas EI task nature [Q(1) = 0.71, p = 0.40], country [Q(1) = 3.08, p = 0.08], and academic performance criterion [Q(1) = 0.38, p = 0.54] did not significantly explain variability in the mean effect (Table 3). The EI test and EI subscale explained 34% of the variability in the mean effect. Age was treated as a continuous variable, and the results showed that age did not significantly explain variability in the mean effect, b = 0.011, SE = 0.007, p = 0.17 (see Fig. 3). As Table 3 shows, the EQ-i test was highly correlated with academic success compared with other EI tests, and the perceiving emotions subscale was highly associated with academic performance compared with other EI subscales.

Regression of Fisher’s z on age
Discussion
The first objective of the current meta-analysis was to test whether EI predicts academic success in MD programs. The three-level multilevel analysis showed that EI is weakly related to academic success in MD programs (r = 0.13; 62). It is interesting and surprising that many studies were devoted to investigating such an association. In fact, to the best of our knowledge, there are no MD programs that explicitly teach medical students how to be emotionally intelligent. Therefore, the assumption that academic performance as assessed by different achievement tests in preclinical and clinical years is related to perceiving emotions, understanding emotions, emotional management, and other EI skills might be unrealistic and not based on a solid rationale. To summarize, these pre-clerkship phase tests of the MD program have very little, if anything, to do with EI. Nevertheless, such an interest in EI in medical training has implications. Although EI represents an important skill or set of skills crucial for all careers/jobs, it is especially relevant in health professions wherein many doctors while dealing with patients require EI for optimal health care delivery. Even those who do not often deal with such challenges require EI skills. We tend to prefer doctors who understand us, show empathy, reduce anxiety, and help us stay optimistic. Therefore, although our findings are based on correlational analysis and do not allow us to draw inferences based on the current study’s findings, we highly recommend that EI skills be explicitly embedded in the MD competency framework. The EI learning outcomes could be achieved either by infusing EI skills into the curriculum or through special training modules. Such a recommendation is supported by Cherry et al. [62] who conducted a critical review of EI in medical education and concluded that “EI-based education may be able to contribute to the teaching of professionalism and communication skills in medicine” (p. 468). Roth et al. discusses practical methods for teaching EI in medical education [63].
A distinction must be made between trait and behavioral EI models because such a distinction has implications on the interpretation of grades achieved in academic courses versus those achieved in clinical settings. While trait EI model predicted the performance of dental graduate students in the Dental Admission Test (DAT) in the first two years in classroom-based didactic courses, the behavioral model of EI predicted grades in the third- and fourth-year clinic-based assessment by dental faculty. Conversely, DAT, the dental school equivalent of MCAT, did not predict grades in the third and fourth years, and behavioral EI did not predict grades in the first two years [64]. Therefore, any interpretation of EI and academic grades of learners, more so in health professions, must consider the EI model used. Nevertheless, the relationship between EI and performance is likely more relevant to the behavioral, interpersonal, and professional aspects of performance than the academic or technical aspects of performance.
Antagonistic neural networks underly differentiated leadership roles in medicine [65]. Analytic processes, including problem solving, emanate from a dominant neural network called the Task Positive Network. However, human interactive processes and openness to new ideas and emotions emanate from the Default Mode Network. These two networks are antagonistic [66]. Given these neural underpinnings, academic grades are not a suitable performance measure of EI in medical school or in the practice of medicine. In addition, there are cross-cultural differences in the EI- scores of medical students [67,68,69].
The second objective of the current study was to test whether the mean effect size varied based on several moderators (see Table 2). Moderator analyses showed that EI tests and EI subscales significantly explained 34% of the variability in the mean effect. Specifically, EI and academic performance are highly related when a trait-based self-report assessment (i.e., EQ-i) is being used compared with an ability-based EI test (i.e., MSCEIT and Schutte Self-Report Emotional Intelligence Test. This is in line with previous studies that showed a weak correlation between ability-based EI tests and trait-based EI scales [21, 70, 71]. Moreover, according to O’Connor et al. [72] “People are not always good judges of their emotion-related abilities and tendencies” (p. 4). Another general disadvantage of self-report assessments is their susceptibility reporting untrue information. However, the correlation between the EQ-i test and academic performance was still weak (r = 0.14). Finally, moderator analysis showed that the EI subscale moderator significantly explained some of the variability in the mean effect. The highest correlation was found for skill in perceiving emotions (r = 0.20) followed by facilitating emotions (r = 0.13) and understanding emotions (r = 0.11). Such a finding indicates that when the ability-based EI test is used with undergraduate medical students (more specifically, the MSCEIT), perceiving emotions best predicts academic performance compared with the other MSCEIT branches.
An important aspect to be considered while interpreting EI in predicting academic success in medical school pertains to the evaluation methods employed to measure academic success. EI affects the major competencies expected of graduating doctors, such as communication skills and professionalism. While there are only a few quality outcomes of these measures, possible outcomes include Objective Structured Clinical Evaluation, faculty ratings, and disciplinary action records. The complexity of evaluating these outcomes may require a 360-degree approach to capture an appropriate level of mastery. Notably, the World Federation of Medical Education as well as MD accreditation commissions have explicitly stated standards and indicators to evaluate these domains. Future studies may focus on these issues to further refine the concept of success in medical school that translates into professional success in medical practice as well.
Two limitations are worth mentioning regarding the current study. First, although performing a meta-analysis study with approximately 15 studies is acceptable [73], researchers in the current study were limited by the small number of effect sizes for some levels of moderators. As Table 3 shows, some levels of moderators consisted of less than 10 effect sizes, which might limit the generalizability of some findings. Second, owing to language limitations, only studies published in English were included. Our search showed that 15 related studies that were published in other languages, which we could not include in our study owing to language limitations.
Conclusions
We conclude with the following recommendations: (a) As our findings showed that EI and academic success are weakly related, researchers and practitioners in the medical field may want to include EI related skills into the MD curriculum or to target EI skills through professional development training/programs; (b) medical education researchers may shift their focus from correlational to experimental studies where EI is explicitly targeted [62] to ensure that MD graduate have the skills to understand others’ emotions and feelings, show empathy to their patients, control, evaluate, and manage their emotions, and use other EI skills effectively in healthcare delivery.
Availability of data and materials
Data available upon request from the first author.
Notes
This is the date of the first published study that met the inclusion criteria. There was no restriction for the year of publication.
Abbreviations
- EI:
-
Emotional intelligence
- MD:
-
Doctor of Medicine
- MSCEIT:
-
Mayer–Salovey–Caruso Emotional Intelligence Test
- TMMS:
-
Trait Meta Mood Scale (TMMS)
- CPX:
-
Comprehensive clinical performance
- PE:
-
Physical examination
- DAT:
-
Dental Admission Test
- GPA:
-
Grade point average
- UMAT:
-
Undergraduate Medicine and Health Sciences Admission Test
- TER:
-
Tertiary Entrance Rank
- WLEIS:
-
Wong and Law Emotional Intelligence Scale
- STEU:
-
Situational Test of Emotional Understanding
- STEM:
-
Situational Test of Emotion Management
- ASICS:
-
Academic Success Inventory for College Students
- EQ-i:
-
Bar-On Emotional Quotient Inventory
- TEIQue:
-
Trait Emotional Intelligence Questionnaire
- CGPA:
-
Cumulative grade point average
- MBBS:
-
Bachelor of Medicine, Bachelor of Surgery
References
References marked with an asterisk indicate studies included in the meta-analysis.
Vanderbilt AA, Perkins SQ, Muscaro MK, Papadimos TJ, Baugh RF. Creating physicians of the 21st century: assessment of the clinical years. Adv Med Educ Pract. 2017;8:395–8.
Fielding S, Tiffin PA, Greatrix R, Lee AJ, Patterson F, Nicholson S, et al. Do changing medical admissions practices in the UK impact on who is admitted? An interrupted time series analysis. BMJ Open. 2018;8: e023274.
Akbarilakeh M, Sharifi¬Fard TS. The relationship between metacognitive awareness and academic success of medical students at Shahid Beheshti University of Medical Sciences. J Med Educ Dev. 2021;16:199–206.
Ullah S, Ullah S, Parvez P, Sheikh GA. Assessment of medical students’ metacognitive awareness of reading strategies and its relation with academic performance: a cross sectional study at Aziz Fatima Medical and Dental College. Faisalabad J Univ Med Dent Coll. 2020;11:1–8.
* Altwijri S, Alotaibi A, Alsaeed M, Alsalim A, Alatiq A, Al-Sarheed S, et al. Emotional intelligence and its association with academic success and performance in medical students. Saudi J Med Med Sci. 2021;9:31–7.
Wu H, Li S, Zheng J, Guo J. Medical students’ motivation and academic performance: the mediating roles of self-efficacy and learning engagement. Med Educ Online. 2020;25:1742964.
Yun H, Kim S, Chung EK. Exploring the structural relationships between medical students’ motivational regulation, cognitive learning, and academic performance in online learning. Korean J Med Educ. 2021;33:115–24.
Banerjee Y, Akhras A, Khamis AH, Alsheikh-Ali A, Davis D. Investigating the relationship between resilience, stress-coping strategies, and learning approaches to predict academic performance in undergraduate medical students: protocol for a proof-of-concept study. JMIR Res Protoc. 2019;8: e14677.
Mahmood M, Afzal MT, Malik AR, Butt AUA, Khan MS, Waseem MH. Association of stress coping strategies and leisure time physical activity with academic performance in medical students. J Rawalpindi Med Coll. 2021;25:48–54.
Amin NAM, Nizman NIM, Zainal ZN, Muhamad MA, Manan NA, Samad NA. Learning style and academic erformance among linical years’ medical students. Malays J Med Health Sci. 2021;17(Suppl 11):8–12.
Hernández-Torrano D, Ali S, Chan C-K. First year medical students’ learning style preferences and their correlation with performance in different subjects within the medical course. BMC Med Educ. 2017;17:131.
Javaeed A, Ishtiaq K, Nawaz A, Khan SH, Shabbir Z, Ghauri SK. Assessment of the relationship between the educational environment and academic performance of undergraduate medical students of Azad Kashmir. J Pak Med Assoc. 2022;72:243–7.
Chang C, Colón-Berlingeri M, Mavis B, Laird-Fick HS, Parker C, Solomon D. Medical student progress examination performance and its relationship with metacognition, critical thinking, and self-regulated learning strategies. Acad Med. 2021;96:278–84.
Shakurnia A, Fazelinia T, Khajeali N. The trend of critical thinking disposition in medical students and its relationship with their academic performance. J Educ Health Promot. 2021;10:479.
* Humphrey-Murto S, Leddy JJ, Wood TJ, Puddester D, Moineau G. Does emotional intelligence at medical school admission predict future academic performance? Acad Med. 2014;89:638–43.
* Libbrecht N, Lievens F, Carette B, Côté S. Emotional intelligence predicts success in medical school. Emotion. 2014;14:64–73.
Singh N, Kulkarni S, Gupta R. Is emotional intelligence related to objective parameters of academic performance in medical, dental, and nursing students: a systematic review. Educ Health (Abingdon). 2020;33:8–12.
Salovey P, Mayer JD. Emotional intelligence Imagin Cogn Pers. 1990;9:185–211.
Bar-On R. The Bar-On model of emotional-social intelligence (ESI). Psicothema. 2006;18(Suppl):13–25.
Goleman D. Emotional Intelligence. Bantam 10th Anniversary Hardcover Ed. New York: Bantam Books; 2006.
Abdulla Alabbasi AM, Ayoub AE, Ziegler A. Are gifted students more emotionally intelligent than their non-gifted peers? A meta-analysis High Ability Stud. 2021;32:189–217.
Arribas-Galarraga S, Cecchini JA, Luis-De-Cos I, Saies E, Luis-De CG. Influence of emotional intelligence on sport performance in elite canoeist. J Hum Sport Exer. 2020;15:772–82.
* Austin EJ, Evans P, Goldwater R, Potter V. A preliminary study of emotional intelligence, empathy and exam performance in first year medical students. Pers Individ Dif. 2005;39:1395–405.
Kaschub M. Defining emotional intelligence in music education. Arts Educ Policy Rev. 2002;103:9–15.
Arora S, Ashrafian H, Davis R, Athanasiou T, Darzi A, Sevdalis N. Emotional intelligence in medicine: a systematic review through the context of the ACGME competencies. Med Educ. 2010;44:749–64.
Cook CJ, Cook CE, Hilton TN. Does emotional intelligence influence success during medical school admissions and program matriculation?: a systematic review. J Educ Eval Health Prof. 2016;13:40.
* Stratton TD, Elam CL, Murphy-Spencer AE, Quinlivan SL. Emotional intelligence and clinical skills: preliminary results from a comprehensive clinical performance examination. Acad Med. 2005;80(10) Suppl:S34–7.
* Austin EJ, Evans P, Magnus B, O’Hanlon K. A preliminary study of empathy, emotional intelligence and examination performance in MBChB students. Med Educ. 2007;41:684–9.
* Carr SE. Emotional intelligence in medical students: does it correlate with selection measures? Med Educ. 2009;43:1069–77.
* Fallahzadeh H. The relationship between emotional intelligence and academic achievement in medical science students in Iran. Procedia Soc Behav Sci. 2011;30:1461–6.
* Leddy JJ, Moineau G, Puddester D, Wood TJ, Humphrey-Murto S. Does an emotional intelligence test correlate with traditional measures used to determine medical school admission? Acad Med. 2011;86(10) Suppl:S39–41.
* Chew BH, Zain AMd, Hassan F. Emotional intelligence and academic performance in first and final year medical students: a cross-sectional study. BMC Med Educ. 2013;13:44.
* Brannick MT, Grichanik M, Nazian SJ, Wahi MM, Goldin SB. Emotional intelligence and medical school performance: a prospective multivariate study. Med Sci Educ. 2013;23:628–36.
* Shah CJ, Sanisara M, Mehta HB, Vaghela HM. The relationship between emotional intelligence and academic achievement in medical undergraduate. Int J Res Med Sci. 2014;2:59–61.
* Naeem N, van der Vleuten C, Muijtjens AM, Violato C, Ali SM, Al-Faris EA, et al. Correlates of emotional intelligence: results from a multi-institutional study among undergraduate medical students. Med Teach. 2014;36(Suppl 1):S30–5.
* Radfar S, Aghaie M, Motashaker-Arani M, Noohi S, Saburi A. Evaluation of emotional intelligence and its relation to the academic achievement in medical students. Thrita J Med Sci. 2013;1:113–9.
* Rajasingam U, Suat-Cheng P, Aung T, Dipolog-Ubanan G, Wei WK. Assessing the relationship between perceived emotional intelligence and academic performance of medical students. AIP Conf Proc. 2014;1635:854–8.
* Nath S, Ghosh S, Das S. Relation between intelligence, emotional intelligence, and academic performance among medical interns. Open J Psychiatry Allied Sci. 2015;6:96–100.
* Holman MA, Porter SG, Pawlina W, Juskewitch JE, Lachman N. Does emotional intelligence change during medical school gross anatomy course? Correlations with students’ performance and team cohesion. Anat Sci Educ. 2016;9:143–9.
* Aithal AP, Kumar N, Gunasegeran P, Sundaram SM, Rong LZ, Prabhu SP. A survey-based study of emotional intelligence as it relates to gender and academic performance of medical students. Educ Health (Abingdon). 2016;29:255–8.
* Johar N, Ehsan N, Khan MA. Association of emotional intelligence with academic performance of medical students. Pak Armed Forces Med J. 2019;69:455–9.
* Gore AD, Jadhav EA. A study analyzing the relationship of emotional intelligence to academic success assessment and stress, depression, anxiety of medical students. Al Ameen J Med Sci. 2021;14:217–24.
Bar-On R. The Bar-On Emotional Quotient Inventory (EQ-i): rationale, description and summary of psychometric properties. In: Geher G, editor. Measuring emotional intelligence: common ground and controversy. Hauppauge: Nova Science Publishers; 2004. p. 115-45
Mayer JD, Caruso DR, Salovey P. The ability model of emotional intelligence: principles and updates. Emot Rev. 2016;8:290–300.
Schutte NS, Malouff JM, Hall LE, Haggerty DJ, Cooper JT, Golden CJ, et al. Development and validation of a measure of emotional intelligence. Pers Individ Dif. 1998;25:167–77.
Ogurlu U. A meta-analytic review of emotional intelligence in gifted individuals: a multilevel analysis. Pers Individ Dif. 2021;171:1–11.
Sánchez-Álvarez N, Berrios Martos MP, Extremera N. A meta-analysis of the relationship between emotional intelligence and academic performance in secondary education: a multi-stream comparison. Front Psychol. 2020;11:1517.
Lim N. Cultural differences in emotion: differences in emotional arousal level between the East and the West. Integr Med Res. 2016;5:105–9.
Chen Y, Peng Y, Fang P. Emotional intelligence mediates the relationship between age and subjective well-being. Int J Aging Hum Dev. 2016;83:91–107.
Sliter M, Chen Y, Withrow S, Sliter K. Older and (emotionally) smarter? Emotional intelligence as a mediator in the relationship between age and emotional labor strategies in service employees. Exp Aging Res. 2013;39:466–79.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA statement. BMJ. 2009;339: b2535.
Reyes-Dominguez P. The relationship between emotional intelligence and leadership on organizational excellence. Unpublished Doctoral Dissertation. ProQuest. p. 3363978; 2008.
Cheshire MH, Strickland HP, Carter MR. Comparing traditional measures of academic success with emotional intelligence scores in nursing students. Asia Pac J Oncol Nurs. 2015;2:99–106.
Doherty EM, Cronin PA, Offiah G. Emotional intelligence assessment in a graduate entry medical school curriculum. BMC Med Educ. 2013;13:38.
McGraw KO, Wong SP. Forming inferences about some intraclass correlation coefficients. Psychol Methods. 1996;1:30–46.
Borenstein M, Hedges LV. Effect size for meta-analysis. In: Cooper H, Hedges LV, Valentine JC, editors. The handbook of research synthesis and meta-analysis. 3rd ed. New York: Russell Publishing Sage Foundation; 2019. p. 207–43.
Van den Noortgate W, López-López JA, Marín-Martínez F, Sánchez-Meca J. Meta-analysis of multiple outcomes: a multilevel approach. Behav Res Methods. 2015;47:1274–94.
Konstantopoulos S. Fixed effects and variance components estimation in three-level meta-analysis. Res Synth Methods. 2011;2:61–76.
Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to meta-analysis. 2nd ed. Chichester: Wiley; 2021.
Hunter JE, Schmidt FL. Methods of Meta-analysis: correcting error and bias in research findings. 3rd ed. New York: Sage Publications, Inc; 2015.
Vevea JL, Coburn K, Sutton A. Publication bias. In: Cooper H, Hedges LV, Valentine JC, editors. The handbook of research synthesis and meta-analysis. 3rd ed. New York: Russell Publishing Sage Foundation; 2019. p. 383-429
Cherry MG, Fletcher I, O’Sullivan H, Dornan T. Emotional intelligence in medical education: a critical review. Med Educ. 2014;48:468–78.
Roth CG, Eldin KW, Padmanabhan V, Friedman EM. Twelve tips for the introduction of emotional intelligence in medical education. Med Teach. 2019;41:746–9.
Victoroff KZ, Boyatzis RE. What is the relationship between emotional intelligence and dental student clinical performance? J Dent Educ. 2013;77:416–26.
White BAA, Cola PA, Boyatzis RE, Quinn JF. Editorial: Emotionally intelligent leadership in medicine. Front Psychol. 2022;13:999184. doi:103389/psyg.2022.999184
Boyatzis RE, Rochford K, Jack AI. Antagonistic neural networks underlying differentiated leadership roles. Front Hum Neurosci. 2014;8:114. https://doi.org/10.3389/fnhum.2014.00114.
Abe K, Niwa M, Fujisaki K, Suzuki Y. Associations between emotional intelligence, empathy and personality of Japanese medical students. BMC Med Educ. 2018;18:47. https://doi.org/10.1186/s12909-018-1165-7.
Scholz U, Gutiérrez Doña B, Sud S, Schwarzer R. Is general self-efficacy a universal construct? Eur J Psycol Assess. 2002;18:242–51. https://doi.org/10.1027//1015-5759.18.3.242.
Bandura A. Self-efficacy: toward a unifying theory of behavioral changes. Psychol Rev. 1977;84:191–215. https://doi.org/10.1037//0033-295x.84.2.191.
Goldenberg I, Matheson K, Mantler J. The assessment of emotional intelligence: a comparison of performance-based and self-report methodologies. J Pers Assess. 2006;86:33–45.
Zeidner M, Shanizinovich I, Matthews G, Roberts RD. Assessing emotional intelligence in gifted and non-gifted high school students: outcomes depend on the measure. Intelligence. 2005;33:369–91.
O’Connor PJ, Hill A, Kaya M, Martin B. The measurement of emotional intelligence: a critical review of the literature and recommendations for researchers and practitioners. Front Psychol. 2019;10:1116.
Lipsey MW, Wilson DB. Practical meta-analysis. New York: Sage Publications, Inc; 2001.
Borenstein M. Heterogeneity in meta-analysis. In: Cooper H, Hedges LV, Valentine JC, editors. The handbook of research synthesis and meta-analysis. 3rd ed. New York: Russell Publishing Sage Foundation; 2019. p. 453-68
Cohen J. Statistical power analysis for the behavioral sciences. New York: Routledge; 1988.
Acknowledgements
Not applicable.
Institutional review board statement
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conceptualization, A. Alabbasi; methodology, A. Alabbasi and F.A. Alabbasi; writing, A. Alabbasi and R. Sequeira; review and editing, A. AlSaleh., R. Sequeira, and A. Alansari; Analyses, A. Alabbasi. All authors have read and agreed to the current version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alabbasi, A.M.A., Alabbasi, F.A., AlSaleh, A. et al. Emotional intelligence weakly predicts academic success in medical programs: a multilevel meta-analysis and systematic review. BMC Med Educ 23, 425 (2023). https://doi.org/10.1186/s12909-023-04417-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-023-04417-8