
Abstract
Background
Identify the objectives and the instructional design of undergraduate endodontics in dental schools in Saudi Arabia.
Methods
The online questionnaire was developed from an original survey conducted in the United Kingdom. The questionnaire was modified for purpose of the study and the region of interest. Then it was directed and emailed to the undergraduate endodontic program directors in twenty-six dental schools in Saudi Arabia. The results were analyzed using descriptive statistics and the Chi-square and Fisher’s exact tests.
Results
The response rate was 96.15%. The number of credit hours for preclinical endodontic courses was up to four credit hours (84%). Students were clinically trained to do vital pulp therapies (92%), root canal treatment (100%), and root canal retreatment (68%). The majority of dental schools define the minimum clinical requirements (92%). Practical and clinical competency exams were used to evaluate students' performance (92% and 84% respectively). The students were trained to treat cases of minimal (52%) to moderate complexity (48%). Endodontic treatment consent and difficulty assessment form were used by 32% and 60% of dental schools respectively. There was no significant difference in the instructional design between public and private dental schools (P > 0.05).
Conclusion
The endodontic undergraduate objectives were to graduate competent clinicians who acquired basic science of endodontics and who know their limitations as it is necessary for a safe general dental practice. The use of endodontic treatment consent and case difficulty assessment should be wisely considered in clinical training.
Similar content being viewed by others
Background
Periodontium health is an essential component of overall body health [1,2,3]. Root canal treatment (RCT) has proven to be effective in restoring the health of the supporting periodontium in non-vital teeth [4,5,6]. Moreover, endodontic treatment can help prevent the development of apical lesions in vital cases [5,6,7].
General dentists are often the first-line practitioners who provide endodontic interventions for patients in need [8, 9]. Unfortunately, the quality of RCT in cross-sectional studies is often described as inadequate or substandard [10,11,12,13,14]. Possible causes were the complexity of root canal procedures or the graduation of inexperienced practitioners [15, 16]. Fortunately, the introduction of modern technologies, instruments, and materials such as nickel-titanium rotary files and bioceramic sealers made RCT procedures simpler and more predictable for general practitioners [15, 17,18,19,20,21].
Ideally, the undergraduate student should master case selection, become competent in using modern techniques for RCT, and have adequate clinical experience before graduation. Thankfully, these educational objectives are permissible when international treatment standards and guidelines are being followed in a well-designed dental curriculum. The Commission of Dental Accreditation (CODA), the Association of Dental Education in Europe (ADEE), and the European Society of Endodontology (ESE) recommended competency-based education in a comprehensive clinical care environment [15, 22, 23]. Furthermore, an endodontic difficulty assessment form or tool has been developed to help guide students and general dentists in case selection [24,25,26].
The Ministry of Education outlines the national qualification framework for the dental specialty in Saudi Arabia. This framework was made to meet the demand for nationally and internationally qualified Saudi dental graduates [27]. Saudi dental graduates are expected to provide high-quality services inside the country and complete their studies or work abroad. Competency-based education is integral to the academic curriculum because it measures and verifies the attainment of intended program learning outcomes [28]. Finally, dental graduates have to commit to a lifelong journey of continuing education and meet the requirements for Saudi licensure registration [29]. However, studies found that Saudi students were not confident in doing steps of RCT or in managing endodontic emergencies [30,31,32]. A similar finding was also reported internationally which signifies the importance of well-designed undergraduate endodontic curricula [33,34,35].
Knowledge about the quality of undergraduate endodontic education for dental practitioners in Saudi Arabia is obscure due to the absence of national observational studies. Therefore, this study aimed to investigate the endodontic course directors' main objectives from undergraduate endodontic education in dental schools of Saudi Arabia. Furthermore. The study will explore the instructional design of endodontic education that course directors followed to meet their objectives.
Material and method
The study was exempt from ethical approval by the institutional review board at Princess Nourah Bint Abdulrahman University (IRB log number: 20–016). The questionnaire was developed from a previous survey made in the United Kingdom [36] and modified to suit the region of interest and the study objectives. The modified questionnaire was written in the English language and piloted on a convenient sample of endodontic faculty. Comments about wording sentences, abbreviations, and punctuations were reviewed and discussed. The suggested changes were considered in the final version of the questionnaire.
The online questionnaire (SurveyMonkey, Momentive, CA, USA) started with a clarification of study objectives, assurance of confidentiality, and consent for participation. The first question was the type of school sector, followed by a question about the program director's objectives in the undergraduate endodontic program. There were eleven questions related to the instructional design of endodontic education (Table 1). All the questions required an answer before complete submission. The newly developed questionnaire was internally piloted and tested for readability and modified accordingly.
A list of all the public and private dental schools in Saudi Arabia was obtained from the Ministry of Education, and the emails of the Deans were obtained from the Saudi Dental Education Society. The Deans were initially contacted with the objectives of the study and to obtain their consent for participation. Then they were requested to email the questionnaire to the undergraduate endodontic program director, who will answer the questions on behalf of the dental school. The responses were analyzed using JMP statistical software (SAS Institute, NC, USA) and the data were summarized using descriptive statistics. The Chi-square and Fisher’s exact tests were used to statically determine the relationship between the collected categorical data and the type of dental school. The level of significance was P ≤ 0.05.
Results
Twenty-five out of the twenty-six dental schools answered the questionnaire resulting in a 96.15% response rate. The number of participating public dental schools was 18 (72%) and seven private dental schools (28%). The program directors' objectives of undergraduate endodontic education were collectively summarized into three main objectives. The first objective is to acquaint students with the basic science of endodontics such as histology, microbiology, pathology, anatomy, and radiology. The second objective was to prepare a dental graduate who is competent in endodontic diagnosis, treatment planning, and management of simple root canal treatments, traumatic dental injuries, and emergencies. They also emphasized that every graduate is aware of the importance of recall and knows how to evaluate the success of their intervention. The third objective was to follow endodontic international standards and guidelines in preparing graduates, and equip them with the ability to recognize the limitation of their skills and experience in managing difficult cases and the necessity of referral in these situations.
The answers to several instructional design questions and their statistical association to the type of dental school are presented in Table 2. The students spend four credit hours or less in preclinical endodontic training (84%), where they are trained using natural teeth (96%). In the clinical setting, students are allowed to mainly treat anterior teeth (100%), premolars (100%), and first molars (92%). Only 36% of the programs train students to treat second molars. Moreover, students are trained to do vital pulp therapy and root canal treatment. However, none of the schools allow students to do apical surgery and only two schools train students to do pulp regeneration. Few schools require students to use a special endodontic treatment consent (32%) and the same applies to using the endodontic difficulty assessment form (40%) (Table 2). Students are allowed to treat simple and moderately difficult cases only.
All of the undergraduate endodontic programs cover the following topics in their teaching: Root canal anatomy and pulp histology (100%), pulp pathology and endodontic microbiology (100%), endodontic radiology (100%), endodontic materials (100%), root canal treatment (100%). Moreover, the majority of dental schools are teaching vital pulp therapy (84%), root canal treatment of immature teeth with necrotic pulp (88%), root canal re-treatment (88%), endodontic surgery (84%), endodontic regeneration (80%), restoration of root-filled teeth (92%), bleaching of endodontically treated teeth (72%), dental trauma (84%), endodontic emergency (92%). There are four dental schools (16%) that mentioned other topics such as endodontic diagnosis and differential diagnosis, case selection and treatment planning, visual aids for diagnosis, endo-perio relationship, resorption, endodontic pain management, rotary files, magnification, and endodontic advancement. The Chi-square and Fisher’s exact tests reveled no significant assosiations between the type of the instructional design and the type of dental schools (P > 0.05).
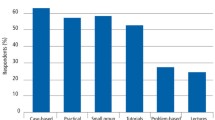
The majority of the dental schools (92%) required students to pass a preclinical practical competency before commencing clinical training. The students have to pass a preclinical root canal treatment competency on anterior teeth (36%), premolars (32%), and molars (24%) before the beginning of clinical training. Four dental schools mentioned that the preclinical competency exam was both on anterior and premolar teeth. One school conducted three preclinical competency exams using plastic teeth, one on an anterior tooth, premolar, and molar. For clinical competency exams, most schools performed them on either anterior teeth (56%), premolars (44%), or both (16%). Clinical competency exams on molars were less emphasized compared to other teeth types (28%). One school stated that their competency exam involved asking the student to complete root canal treatment of a single canal system in one visit.
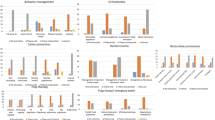
The majority of dental schools (92%) request students to complete a minimum number of endodontic requirements before graduation. Only two schools do not define the number nor the type of their requirements (8%). The minimum number of root canal treatments required before graduation is presented in Fig. 1. Single canal systems were frequently requested. The students usually have to complete up to three to six cases before graduation. Few dental schools ask their students to complete RCT of ten single canals (12%). Comparable findings were found in the two canals system in which few schools requested ten teeth (8%). Requirements involving three to four canal systems, however, were less than three teeth in most dental schools (68%) (Fig. 2). One school asked dental students to collect procedural points instead of defining the number or the type of procedures. In this model, the students will aim to collect procedural points that will allow them to reach the minimum number of points requested for their level of education in each dental specialty. The weight of the procedural points is adjusted according to the number of canals or the difficulty of the procedure. For example, multiple canals are given more weight than a single canal. Interestingly, one school additionally requested two cases of retreatment before graduation.

Percentage of dental schools that use anterior, premolar and molar teeth in competency exams in preclinical and clinical training

Percentage of dental schools according to the minimum number of root canal treatments required from dental students per canal anatomy
Discussion
The objectives of the undergraduate endodontic program directors were to graduate competent practitioners who know the basic science of endodontics and who are competent in the diagnosis and management of simple endodontic cases. They also emphasized the importance of case selection to prevent malfeasance. Undergraduate students attend less than four credit hours of preclinical endodontic courses in which they are trained to do root canal treatment on natural teeth. In the clinical setting, most schools allowed students to do RCT on single, as well as, multiple canal systems except the second molar. Moreover, students are trained to do vital pulp therapy and RCT in simple and moderately difficult cases. The majority of dental students have a competency-based assessment in preclinical and clinical training. The students usually graduate after completing a minimum number of requirements in simple or moderately difficult cases. Unfortunately, the students are not consistently using the endodontic difficulty assessment forms and not signing a special endodontic treatment consent.
The endodontic undergraduate objectives are aligned with the European Society of Endodontology (ESE) and the Australian and New Zealand Academy of Endodontists undergraduate endodontic curriculum guidelines [37, 38]. The ESE and ADEE assume that dental students should be trained to be competent in RCT of uncomplicated single and multi-rooted teeth [5, 39, 40]. The Ministry of Health in Saudi Arabia expects qualified general dentists to be competent in RCT of anterior teeth, and mandates they refer treatment of posterior teeth to the endodontist after performing only necessary emergency intervention [41]. However, Saudi students are being trained to do RCT on all teeth types except for second molars. Moreover, the Saudi students are trained to treat cases of minimal to moderate level of complexity. Several studies found that undergraduate students were least confident in treating the molars among other teeth groups [31,32,33, 35, 42, 43]. Interestingly, the quality of RCT done in the Saudi public health sector was better than in the Saudi private sector and even better than some of the internationally reported findings [10]. One possible reason is that the general dentist in the Saudi public sector is more likely to follow the Ministry of Health recommendation and refer posterior teeth to an endodontist. The quality of RCT was reported to be significantly lower in molars [13]. The same finding was also reported studying the quality of RCT among undergraduate dental students [39, 40, 44]. Therefore, RCT of molars can become the objective of graduate training in the absence of sufficient time or resources to achieve satisfactory results in undergraduate training.
The Canadian and American endodontic case difficulty assessment form was developed to help dental practitioners to evaluate case complexity which will help them decide whether to treat or refer the case. Cases of high difficulty were defined as being clinically challenging for the most experienced practitioners. RCT of second molars and retreatments were regarded as high in difficulty [45]. The students were allowed to treat second molars in 36% of dental schools and perform retreatment in 68% of the dental schools. Also, the students were allowed to engage in the treatment of moderately complex cases. Case selection was one of the objectives of the undergraduate endodontic training. However, 40% of dental schools did not use any difficulty assessment form in clinical training. Tanalp et al. suggest that students are less confident in treating complex cases because they tend to refer these cases to postgraduate residents [35]. However, students perceived endodontic treatment as one of the most stressful dental procedures [46]. Because the endodontic procedure includes many steps such as local anesthesia administration, rubber dam isolation, and caries removal [46]. In addition to the endodontic access and root canal negotiation that requires multiple radiographs for assessment and completion of RCT visit. The management of patient anxiety and pain, post-operative pain, and endodontic flare-up may add another burden to undergraduate students [35]. Observation studies found that the quality of RCT and the endodontic treatment outcomes were less predictable in complex cases [35, 40, 44, 47, 48]. Therefore, it's probably best to refer these challenging cases to a specialist who can conveniently dedicate expertise, time, and resources to manage and follow these cases closely.
The students
Competency-based education focuses on preparing dental students for professional life after graduation [49,50,51,52]. The laboratory practical exams, clinical competencies, and procedural requirements are methods used to assess competency [53]. The majority of dental schools in Saudi Arabia require students to pass a clinical competency exam and to complete a minimum number of procedural requirements. In a clinical competency exam, students carefully select their competency cases to pass the test. Then the faculty will assess the dental student's ability to provide adequate RCT independently [53]. The quality of RCT will be assessed according to international treatment standards. Therefore, students during this process will carefully practice case difficulty assessment and will realize the importance of case selection. Standardization of clinical circumstances can be improved by providing a clear description of suitable clinical cases [54]. For example, the clinical competency exam should be on an uncomplicated single canal in the anterior region.
The number of procedural requirements is different among Saudi dental schools. Currently, there is no sound evidence that supports the need to repeat a clinical dental procedure a certain number of times before approaching competency [55]. ESE used to recommend twenty natural teeth including extracted teeth as a minimum requirement for dental graduation [56]. Experiential learning theory can be used to support the importance of procedural requirements because it suggests that students learn best from experience [57]. Moreover, Self-efficacy was a positive predictor of dental academic performance [58]. The dental students' perception of self-efficacy was connected to their clinical experience [59]. Furthermore, students' endodontic self-efficacy improved as they performed more RCT [43]. However, those students endodontic self-efficacy declined in molars and retreatments [43].
Unexpectedly, Chamber observed that the learning curve in dental school was flat [55]. The possible explanation was that students aimed to perform best to pass grading criteria rather than gain dental experience. Moreover, he criticized the arbitrary practice of setting the procedural requirements numbers [55]. There is a need for further studies that explore the benefits of this practice and that guide educators in the decision-making process. Procedural requirements were regarded as an unethical practice [53]. Moreover, dental students found procedural requirements stressful [60]. Dental students in Saudi Arabia reported a high level of stress during their clinical training [61, 62]. Endodontic procedure particularly was one of the most stressful clinical events in dental training [46]. Thoughtfully, endodontic education guidelines in Australia and New Zealand extended the duration of comprehensive inter-disciplinary clinical care to at least two years [38]. However, the exact number and type of teeth were not determined since it depends on patient availability [38]. Hence, emphasizing the duration of clinical training rather than the number and type of teeth could be beneficial and less stressful for dental students [38].
Few dental schools did not select practical exams or clinical requirements as assessment criteria. Alternatives and adjunctive techniques that were suggested to assess competency are portfolios, objective structured clinical examination (OSCE), triple jump exams, and longitudinal and daily evaluation [54]. However, these assessment techniques were not investigated in this study.
Dental schools in Saudi Arabia don’t use endodontic consent for treatment consistently. General treatment consent might not clarify the possible emerging endodontic complications such as failure to achieve local anesthesia, post-operative pain, ledge, or broken instrument. Moreover, endodontic treatment consent is a valuable tool that would reinforce students' need for careful case assessment and treatment discussion with the patient. Finally, endodontic consent would set the treatment expectations for the patients and allow them to make informed dental decisions [63].
Most of the endodontic topics were covered which was similar to the findings of the United Kingdom and Spain [36, 64]. Fortunately, 96% of preclinical training was on natural teeth. Preclinical training on natural teeth is recommended since it's more challenging and realistic [65, 66]. Alternative options to natural teeth have been explored in the literature [65, 66]. The public and private schools had a similar approach to the instructional design of undergraduate endodontics in Saudi Arabia. One possible explanation is that the sample size for both of these schools was small to detect actual differences between them. Since the statistical findings were highly susceptible to type II error, the results have to be carefully interpreted.
The development of national guidelines for undergraduate endodontic education is recommended since it will improve the alliance among Saudi dental schools. Moreover, national guidelines would combine up-to-date evidence in best practices in education and endodontics. These guidelines will help undergraduate program directors to make key decisions that will enhance the training and performance of dental graduates. Finally, further research is needed to explore the best teaching and assessment methods to ensure endodontic competency, specifical topics such as the learning curve in endodontics and the requirements number.
Conclusion
The undergraduate endodontic objectives are aligned with European endodontic guidelines. Saudi students are trained to do vital pulp therapy and RCT on mild to moderately complex cases. Procedural requirements and competency clinical exams are used to assess competency in the majority of dental schools. Endodontic treatment consent and difficulty assessment form are not consistently used. The development of national guidelines for undergraduate endodontic education is recommended.
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Abbreviations
- RCT:
-
Root canal treatment
- CODA:
-
The Commission of Dental Accreditation
- ADEE:
-
Association of Dental Education in Europe
- ESE:
-
European Society of Endodontology
- OSCE:
-
Objective structured clinical examination
References
An GK, Morse DE, Kunin M, Goldberger RS, Psoter WJ. Association of radiographically diagnosed apical periodontitis and cardiovascular disease: a hospital records-based study. J Endod. 2016;42:916–20.
Gomes MS, Blattner TC, Sant’ Ana Filho M, Grecca FS, Hugo FN, Fouad AF, et al. Can apical periodontitis modify systemic levels of inflammatory markers? A systematic review and meta-analysis. J Endod. 2013;39:120–17.
Segura-Egea JJ, Martín-González J, Castellanos-Cosano L. Endodontic medicine: connections between apical periodontitis and systemic diseases. Int Endod J. 2015;48:933–51.
Ng YL, Mann V, Gulabivala K. Outcome of secondary root canal treatment: a systematic review of the literature. Int Endod J. 2008;41:1026–46.
Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - Part 2. Influence of clinical factors. Int Endod J. 2008;41:6–31.
Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: Systematic review of the literature - Part 1. Effects of study characteristics on probability of success. Int Endod J. 2007;40:921–39.
Aguilar P, Linsuwanont P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod. 2011;37:581–7.
Alrahabi M, Ahmad MS. Knowledge regarding technical aspects of non-surgical root canal treatment in Al-Madinah Al-Munawarah private dental centers. Saudi Endod J. 2015;5:155–60.
Dietz GC, Dietz GC. The endodontist and the general dentist. Dent Clin North Am. 1992;36:459–71.
Al-Obaida MI, Alwehaiby KM, Al-Hindi OH, Merdad K, Al-Madi EM. Radiographic evaluation of the technical quality of root canal filling in Riyadh government and private hospitals. Saudi Endod J. 2020;10:194–8.
Alrahabi M, Younes HB. A cross-sectional study of the quality of root canal treatment in Al-Madinah Al-Munawwarah. Saudi Endod J. 2016;6:31–5.
Boucher Y, Matossian L, Rilliard F, Machtou P. Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. Int Endod J. 2002;35:229–38.
Chueh LH, Chen SC, Lee CM, Hsu YY, Pai SF, Kuo ML, et al. Technical quality of root canal treatment in Taiwan. Int Endod J. 2003;36:416–22.
Di Filippo G, Sidhu SK, Chong BS. Apical periodontitis and the technical quality of root canal treatment in an adult sub-population in London. Br Dent J. 2014;216:E22–E22.
Koch M, Wolf E, Tegelberg Å, Petersson K. Effect of education intervention on the quality and long-term outcomes of root canal treatment in general practice. Int Endod J. 2015;48:680–9.
Qualtrough AJE. Undergraduate endodontic education: What are the challenges? Br Dent J. 2014;216:361–4.
Abu-Tahun I, El-Ma’aita A, Khraisat A. Satisfaction of undergraduate students at University of Jordan after root canal treatment of posterior teeth using rotary or hand preparation. Aust Endod J. 2016;42:66–72.
Dahlström L, Molander A, Reit C. The impact of a continuing education programme on the adoption of nickel-titanium rotary instrumentation and root-filling quality amongst a group of Swedish general dental practitioners. Eur J Dent Educ. 2015;19:23–30.
Koch K, Brave D. Bioceramic technology – the game changer in endodontics. Practice. 2009:13–7.
Koch K, Brave D. The increased use of bioceramics in endodontics. Dentaltown. 2009:39–43.
Chybowski EA, Glickman GN, Patel Y, Fleury A, Solomon E, He J. Clinical outcome of non-surgical root canal treatment using a single-cone technique with endosequence bioceramic sealer: a retrospective analysis. J Endod. 2018;44:941–5.
Levin L, Halperin-Sternfeld M. Tooth preservation or implant placement: a systematic review of long-term tooth and implant survival rates. J Am Dent Assoc. 2013;144:1119–33.
Commission on Dental Accreditation Accreditation Standards For Dental Education Programs. Commission on Dental Accreditation (CODA). Coda.org. 2018. https://www.ada.org/en/coda. Accessed 8 Jul 2021.
Essam O, Boyle EL, Whitworth JM, Jarad FD. The Endodontic Complexity Assessment Tool (E-CAT): a digital form for assessing root canal treatment case difficulty. Int Endod J. 2021;54:1189–99.
Haug SR, Solfjeld AF, Ranheim LE, Bårdsen A. Impact of case difficulty on endodontic mishaps in an undergraduate student clinic. J Endod. 2018;44:1088–95.
Ree MH, Timmerman MF, Wesselink PR. An evaluation of the usefulness of two endodontic case assessment forms by general dentists. Int Endod J. 2003;36:545–55.
National Commission for Academic Accreditation. National Qualifications Framework for Higher Education in the Kingdom of Saudi Arabia. 2009. https://www.mu.edu.sa/sites/default/files/National%20Qualifications%20Framework%20for%20HE%20in%20KSA.pdf. Accessed 8 Jul 2021.
Education and Training Evaluation Commission. Standards for Program Accreditation. 2018.
Saudi Commission for Health Specialties. Regulations and Requirements. 2017. https://www.scfhs.org.sa/en/registration/Regulation/Pages/default.aspx. Accessed 8 Jul 2021.
Alrahabi M. The confidence of undergraduate dental students in Saudi Arabia in performing endodontic treatment. Eur J Dent. 2017;11:17–21.
Javed MQ, Khan AM, Bhatti UA. Evaluation of undergraduate dental students self-perceived confidence level regarding endodontic procedures: a questionnaire survey. Saudi Endod J. 2021;11:228.
Shoaib B, Khawaja Z, Oteibi A Al, Asiri L, Wasifre A Al, Anizi M Al. The problems of endodontic treatment facing undergraduate students. J Appl Dent Med Sci. 2019;5:1–9.
Davey J, Bryant ST, Dummer PMH. The confidence of undergraduate dental students when performing root canal treatment and their perception of the quality of endodontic education. Eur J Dent Educ. 2015;19:229–34.
Luz LB, Grock CH, Oliveira VF, Bizarro L, Ardenghi TM, Ferreira MBC, et al. Self-reported confidence and anxiety over endodontic procedures in undergraduate students—Quantitative and qualitative study. Eur J Dent Educ. 2019;23:482–90.
Tanalp J, Güven EP, Oktay I. Evaluation of dental students′ perception and self-confidence levels regarding endodontic treatment. Eur J Dent. 2019;07:218–24.
Al Raisi H, Dummer PMH, Vianna ME. How is Endodontics taught? A survey to evaluate undergraduate endodontic teaching in dental schools within the United Kingdom. Int Endod J. 2019;52:1077–85.
De Moor R, Hülsmann M, Kirkevang LL, Tanalp J, Whitworth J. Undergraduate curriculum guidelines for endodontology. Int Endod J. 2013;46:1105–14.
Sadr A, Rossi-Fedele G, Love RM, George R, Parashos P, Wu MCY, et al. Revised guidelines for the endodontic education of dentistry students in Australia and New Zealand (FEBRUARY 2021). Aust Endod J. 2021;47:327–31 (J Aust Soc Endodontology Inc).
Eleftheriadis GI, Lambrianidis TP. Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. Int Endod J. 2005;38:725–34.
Unal GC, Kececi AD, Kaya BU, Tac AG. Quality of root canal fillings performed by undergraduate dental students. Eur J Dent. 2019;05:324–30.
Saudi Ministry of Health. Regulations of Dental Services in Saudi Ministry of Health. Saudi Ministry of Health; 2004. https://www.moh.gov.sa/Ministry/Rules/Pages/default.aspx. Accessed 15 Jul 2021.
Barakat RM, Matoug-Elwerfelli M, Almohareb RA, Balto HA. Influence of preclinical training on root canal treatment technical quality and confidence level of undergraduate dental students. Int J Dent. 2021;2021:9920280.
Baaij A, Özok AR, Vӕth M, Musaeus P, Kirkevang L-L. Self-efficacy of undergraduate dental students in Endodontics within Aarhus and Amsterdam. Int Endod J. 2020;53:276–84.
Barrieshi-Nusair KM, Al-Omari MA, Al-Hiyasat AS. Radiographic technical quality of root canal treatment performed by dental students at the Dental Teaching Center in Jordan. J Dent. 2004;32:301–7.
American Association of Endodontists. AAE Endodontic Case Difficulty Assessment Form. 2021 Mar 2. 2019. https://www.aae.org/specialty/wp-content/uploads/sites/2/2019/02/19AAE_CaseDifficultyAssessmentForm.pdf. Accessed 2 Mar 2021.
Mocny-Pachońska K, Doniec RJ, Wójcik S, Sieciński S, Piaseczna NJ, Duraj KM, et al. Evaluation of the most stressful dental treatment procedures of conservative dentistry among polish dental students. Int J Environ Res Public Health. 2021;18:4448.
De Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, et al. Treatment outcome in endodontics: the Toronto study—Phase 4: initial treatment. J Endod. 2008;34:258–63.
Imura N, Pinheiro ET, Gomes BPFA, Zaia AA, Ferraz CCR, Souza-Filho FJ. The outcome of endodontic treatment: a retrospective study of 2000 cases performed by a specialist. J Endod. 2007;33:1278–82.
Chambers DW. Competency-based dental education in context. Eur J Dent Educ. 1998;2:8–13.
Chambers D. Competencies: a new view of becoming a dentist. J Dent Educ. 1994;58:342–5.
Chambers D, Glassman P. A primer on competency-based evaluation. J Dent Educ. 1997;61:651–66.
Chuenjitwongsa S, Oliver RG, Bullock AD. Competence, competency-based education, and undergraduate dental education: a discussion paper. Eur J Dent Educ. 2018;22:1–8.
Albino JEN, Young SK, Neumann LM, Kramer GA, Andrieu SC, Henson L, et al. Assessing dental students’ competence: best practice recommendations in the performance assessment literature and investigation of current practices in predoctoral dental education. J Dent Educ. 2008;72:1405–35.
Kramer GA, Albino JEN, Andrieu SC, Hendricson WD, Henson L, Horn BD, et al. Dental student assessment toolbox. J Dent Educ. 2009;73:12–35.
Chambers D. Learning curves: what do dental students learn from repeated practice of clinical procedures? J Dent Educ. 2012;76:291–302.
Löst C. Undergraduate curriculum guidelines for endodontology. Int Endod J. 2001;34:574–80.
Sharlanova V. Experiential learning. Trakia J Sci. 2004;2:36–9.
Mafla AC, Divaris K, Herrera-López HM, Heft MW. Self-efficacy and academic performance in colombian dental students. J Dent Educ. 2019;83:697–705.
Watters AL, Stabulas-Savage J, Toppin JD, Janal MN, Robbins MR. Incorporating experiential learning techniques to improve self-efficacy in clinical special care dentistry education. J Dent Educ. 2015;79:1016–23.
Alzahem AM, Van Der Molen HT, Alaujan AH, Schmidt HG, Zamakhshary MH. Stress amongst dental students: a systematic review. Eur J Dent Educ. 2011;15:8–18.
Al-Sowygh ZH. Academic distress, perceived stress and coping strategies among dental students in Saudi Arabia. Saudi Dent J. 2013;25:97–105.
Al-Sowygh ZH, Alfadley AA, Al-Saif MI, Al-Wadei SH. Perceived causes of stress among Saudi dental students. King Saud Univ J Dent Sci. 2013;4:7–15.
Selbst AG. Understanding informed consent and its relationship to the incidence of adverse treatment events in conventional endodontic therapy. J Endod. 1990;16:387–90.
Segura-Egea JJ, Zarza-Rebollo A, Jiménez-Sánchez MC, Cabanillas-Balsera D, Areal-Quecuty V, Martín-González J. Evaluation of undergraduate Endodontic teaching in dental schools within Spain. Int Endod J. 2021;54:454–63.
Bitter K, Gruner D, Wolf O, Schwendicke F. Artificial versus natural teeth for preclinical endodontic training: a randomized controlled trial. J Endod. 2016;42:1212–7.
Decurcio DA, Lim E, Chaves GS, Nagendrababu V, Estrela C, Rossi-Fedele G. Pre-clinical endodontic education outcomes between artificial versus extracted natural teeth: a systematic review. Int Endod J. 2019;52:1153–61.
Acknowledgements
Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2022R162), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Funding
Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2022R162), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Author information
Authors and Affiliations
Contributions
F.A and R.B study conception and design; F.A, E.A, L.A and A.A data collection: F.A, R.B and R.A; analysis and interpretation of results; F.A, R.B and R.A draft manuscript preparation; All authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was waived by the institutional review board in Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia (IRB log number: 20–016) since the research involved survey procedures that collect existing data and documents in a manner that human subjects can not be identified directly or indirectly. Written informed consent was obtained from each of the participants. The anonymity of participants was guaranteed and all of the participants voluntarily participated in the study. All methods were performed following the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Algahtani, F.N., Barakat, R.M., Almohareb, R.A. et al. The objectives and instructional design of undergraduate endodontic program: multicenter cross-sectional study in Saudi Arabia. BMC Med Educ 22, 486 (2022). https://doi.org/10.1186/s12909-022-03548-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-022-03548-8