
Abstract
Background
Peer-led tutorials are widely used in medical education to promote practical skills acquisition and support faculty staff. Typically, student tutors are custom trained for this specific task. We investigated whether opening up an existing medical tutor qualification program to other degree programs is successful in terms of acceptance among students, acquisition of tutor-specific and interprofessional competencies, and which factors contribute to success or failure.
Methods
We developed a two-day tutor qualification program and conducted it annually from 2016 to 2020 with medical and other healthcare students. At the end of each course, we administered a written survey in which the participants rated the following items: their attitudes towards interprofessional learning (using the UWE-IP-D Interprofessional Learning Scale), the interprofessional learning setting, the teaching approach, and their competency acquisition (each on a five-point Likert scale; 1 = strongly agree, 5 = strongly disagree). Furthermore, we assessed participants’ qualitative feedback in free-text fields and performed inductive content analyses.
Results
The study participation rate was high (response rate 97%; medical students: n = 75; healthcare students: n = 22). Participants stated high levels of competency acquisition (total M = 1.59, individual items’ M’s ranging from 1.20 to 2.05) and even higher satisfaction with the teaching approach (total M = 1.28, individual items’ M’s ranging from 1.43 to 1.05). Overall satisfaction with the training was M = 1.22; SD = 0.58. No significant differences in ratings were found between the student groups. The qualitative results showed that students appreciated the interprofessional setting and experienced it as enriching. The most positive feedback was found in didactics/teaching methods on role-plays and group work; most suggestions for improvement were found in the area of structure and organisation on breaks and time management.
Conclusions
Opening up an existing medical tutor qualification program to other student groups can be seen as fruitful to teach not only tutor-related aspects but also interprofessional competencies. The results demonstrate the importance of detailed planning that considers group composition and contextual conditions and provides interactive teaching methods to promote interprofessional experiences. This study offers important information about prerequisites and methodological implementation that could be important for the interprofessional redesign of existing training programs.
Similar content being viewed by others


Background
Student tutorial courses represent an essential element within undergraduate medical teaching today. One crucial and widespread setting is near-peer teaching. Experienced and trained students (referred to as tutors) teach small student groups in communication and clinical skills, for example [1,2,3]. Peer teaching has a long history in medical education [4, 5]. One major impetus for implementation was faculty dissatisfaction with large lectures where students played a passive role [6]. Peer teaching programs offer numerous further advantages to traditional faculty-led classes, for example, by addressing the faculty resource problem of providing multiple teachers to lead smaller group sizes for practising hands-on skills [7,8,9,10,11]. Peer-led courses can be as effective as traditional staff-led courses [12,13,14]. When students learn from students who usually have only a few semesters’ head start, a shared knowledge base and experience can be built upon [15]. Since tutors are generally highly motivated and engaged [16] and have high cognitive and social congruence [15], their familiarity with the learner’s current knowledge and learning situation can create a more personal and friendly learning atmosphere. This contributes to deepening and broadening the learners’ practical, cognitive and social skills and thus to quality assurance and professionalism [17]. To achieve these positive effects, both sensitive planning and implementation of tutorial courses and structured and rigorous training of tutors are necessary [18, 19]. A variety of strategies exist to prepare tutors for teaching other students.
Currently, medical education sees a trend towards a needs-adapted training strategy [20] as teaching in the medical program is characterised by a tightly paced curriculum and many competencies to be acquired. The high level of interactivity, examination of one’s role, and generally well-supported tutor training programs make this setting attractive for interprofessional education (IPE). Opening up proven and tailored medical teaching programs to students from other health professions can broaden participants’ horizons but risks weakening the focus on profession-specific competencies. In the field of tutorial courses, there is evidence that well-established monoprofessional approaches can be successfully transformed into interprofessional ones [21].
A fundamental, competency-based reorientation of medical studies in Germany is currently underway, calling for more robust integration of interprofessional teaching programs [22]. The aim is to ensure the quality of future cross-professional patient care [23, 24]. Being educated in an interprofessional setting provides an opportunity for professionals to share skills and knowledge that facilitates the development of shared values and a better understanding of the roles and responsibilities of the other healthcare students [25]. According to the definition given by the Centre for the Advancement of Interprofessional Education, “Interprofessional learning takes place when members or students of two or more professions learn with, from and about each other to improve collaboration and the quality of care and services” [26]. The collaboration for which IPE prepares is more than cooperation since students learn to empower each other in a nurturing and mutually supportive environment to collaborate flexibly and effectively across predetermined professional boundaries [27]. A form of leadership based on joint decision-making is required to ensure good cooperation within an interprofessional team, which poses a challenge to lecturers with traditional, hierarchical role models [28]. Hierarchical gradients between student tutors and student learners are at a minimum [29], and thus tutors and learners gradually build an interactional relationship [30]. Interprofessional peer teaching opens up the possibility of breaking down traditional role patterns. Interprofessional trained student tutors can serve as multipliers and role models for other students and are, therefore, of particular interest for spreading positive interprofessional attitudes. Opening up existing medical tutor qualification programs to other healthcare students could provide new interprofessional learning opportunities.
The following questions guide the study presented here:
-
Do general attitudes differ toward interprofessional learning between tutors from different degree programs and toward other students?
-
How is interprofessional tutor training perceived from the participating students’ point of view? Are there differences between different student groups? How high is participants overall satisfaction?
-
Can the training program’s learning objectives be achieved in an interprofessional setting for all student groups, even though tutors are trained for different tutorials? Are there differences in goal achievement between the student groups?
-
Which teaching methods and conditions contribute to the success or failure of interprofessional tutor training?
Methods
Peer teaching at the Heidelberg Medical Faculty
Medical students
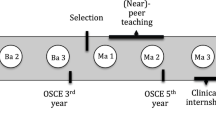
Tutors are firmly integrated into the preclinical study phase at the Heidelberg Medical Faculty. They independently guide small groups of ten to twelve students in the training of medical skills, in particular, taking medical histories, physical examinations and venipuncture. Central coordination was established to successfully implement AaLPlus, the Living Anatomy plus Anamnesis program, to regulate the extensive coordination within the Medical Faculty and the evaluation of the acquired skills [31]. The program sustainably contributes to quality assurance, professionalism, and solving the problem of resources in medical education [32, 33]. As a prerequisite for teaching their younger peers, AaLPlus tutors must complete basic training in didactics/teaching methods and group leadership, as well as additional doctor-patient communication and physical examination training [34]. These modules are part of a longitudinally structured program for tutor qualification, developed at the Heidelberg Medical Faculty based on a needs assessment and implemented in the 2010 summer semester [35]. The program consists of other advanced modules, such as subject-specific training, collegial advice, and reflection on the tutors’ activities. The basic tutor training is conducted annually before the winter semester. The Department of General Practice & Health Services Research at Heidelberg University’s Faculty of Medicine organises the AaLPlus program. It conducts the corresponding tutor qualification program each year before the start of the winter semester.
Healthcare students
Two study programs for healthcare students are also affiliated with this department. The undergraduate bachelor’s degree program in “Interprofessional Health Care” was introduced in 2011. In eight semesters, students can complete an academic degree parallel to vocational training, such as nursing, physiotherapy or speech therapy [36]. In addition, the two-year, full-time Master of Science program in “Health Services Research and Implementation Science” was introduced in 2015. This program is unique because it focuses specifically on healthcare delivery in all settings, e.g., hospitals, primary care, ambulatory practices, and public health organisations [37]. Healthcare students (HCS) acquire basic knowledge of qualitative and quantitative research in both degree programs, but have very different learning backgrounds within the courses. It proved necessary to provide them with supervised sessions to practice scientific skills such as seeking literature and scientific writing. Individual modules, such as Medical English [38, 39], are also conducted interprofessionally, with integrated tutoring.
Developing the interprofessional tutor qualification program
Since the cohorts in both HCS degree programs are relatively small compared to the medical school and no direct experience with the training of tutors was available, the idea of joint tutor training within the Medical Faculty emerged. Moreover, one further aim was to establish additional opportunities for interprofessional learning to address the increasing need for interprofessional collaboration among healthcare professionals [40]. The respective coordinators of the healthcare degree programs and the established medical tutor qualification program first discussed the potential for a joint tutor qualification program in 2015. The medical tutor qualification program coordinators expressed concerns that the study groups could be too diverse and that the tailored tutoring qualification of medical students could be endangered due to the different group compositions and tutoring settings they were to be qualified for. In general, developing a training program for interprofessional student tutors requires excellent care so that students can later conduct tutorials on an equal footing and are accepted equally by all participants [41]. At the same time, all coordinators saw the opportunity to use existing resources and were willing to create interprofessional learning opportunities. Since tutors are role models, positive attitudes towards interprofessional learning and working can positively impact other students. In addition, the acquisition of interprofessional competencies in an interprofessional tutor qualification program makes it easier to establish other interprofessional peer-assisted teaching programs, for example, in communication training or scientific writing. An interprofessional tutor qualification program was developed with internal funding from the Heidelberg Medical Faculty, supported by the State Ministry of Baden-Württemberg for Science, Research and the Arts (“Sonderlinie Medizin” project). Tight curricula and, therefore time constraints necessitated a closely coordinated team of representatives from the participating programs working together to condense relevant content into a joint, comprehensive training program.
First, the multiprofessional trainer team, consisting of a medical educator, a psychologist, a physician, and a social anthropologist, assessed the essential training to identify the module components relevant to all degree programs. The trainers formulated competencies that all participants should acquire (Fig. 1).

Development process and competencies of the interprofessional tutor qualification program
In the next step the trainers reviewed all teaching content to ensure that it was understandable and authentic for the participating students. They transformed role plays and case studies into interprofessional scenarios and avoided profession-specific technical language. After a year-long planning phase, the team conducted a one-day module and evaluated it at the beginning of the 2015 winter semester. Evaluation results showed a high acceptance among the participating students. Based on the evaluation results, the team developed a two-day interprofessional tutor qualification program conducted annually from 2016 onwards. The four trainers prepared and conducted all training sessions, bringing to bear their professional perspectives. Table 1 shows the schedule of the newly designed interprofessional tutor qualification program. Training content and methods were continuously adapted in subsequent years, although the objectives and basic structure have been largely retained.
Data collection and study design
Between October 2016 and October 2020, we asked all participants in the interprofessional tutor qualification program to complete a paper-based questionnaire at the end of the interprofessional course. The questionnaire is comprised of the following sections:
-
1)
Socio-demographic data (age, gender, study program and study semester) was collected to describe the participants.
-
2)
General attitudes toward interprofessional learning were assessed with the Interprofessional Learning scale from the German version of the University of the West of England Interprofessional Questionnaire (UWE-IP-D) [50, 51]. The UWE-IP-D is an established assessment tool used at the University of Heidelberg to evaluate interprofessional learning environments. This questionnaire was validated for the German language in 2017 and was already available at the beginning of our study [52]. The statements of the UWE-IP-D subscale for Interprofessional Learning consists of nine items from 1 (= strongly agree) to 5 (= strongly disagree) with overall scores ranging from 9 to 45. Scores from 9 to 22, 23 to 31, and 32 to 45 indicate positive, neutral and negative attitudes, respectively [51]. We deleted individual UWE-IP-D subscales, if one or more single values were missing.
-
3)
The assessment of the interprofessional setting was conducted on a five-point Likert scale (rating statement: Learning with other professions was successful) and an open-ended question (request: What has contributed to the success/failure of interprofessional learning?).
-
4)
Tutor competency acquisition was assessed with eight rating questions related to the previously established competencies (five-point Likert scale; 1 = strongly agree, 5 = strongly disagree).
-
5)
The teaching approach was assessed with nine rating questions on course design, interaction, satisfaction and overall rating of the training (five-point Likert scale; 1 = strongly agree, 5 = strongly disagree). To gain deeper insight into what contributed to the individual ratings, these two open-ended questions were added: “Which methods/content should definitely be retained?” and “How could the tutor training be improved?”.
Data analyses
The qualitative data in the free-text fields were analysed using a content analytical approach. SZ and AH structured the text material regarding parts of the program that should be kept or improved. First, 88/86 statements for each question were screened and broken up into distinctive topics that the participants referred to in their feedback. Second, all statements were kept as worded and grouped thematically by both researchers independently. Each researcher identified the major themes or program components to which the statements referred and created main categories for each group of statements. Third, the two researchers compared and discussed their categorizations. To grasp the number of participants who expressed a specific feedback, all similar statements were counted and grouped into sub-categories. Both the quantitative description and the sub-categories were double-checked, discussed and refined in an iterative process [53].
We analyzed all quantitative data using IBM’s SPSS statistics (version 27, 2020) with a general significance level set to α = .05. A thorough data screening revealed no missing data, outliers, or nonlinear associations. Most Likert scale items showed floor effects. We computed relevant descriptive statistics and conducted inferential comparisons between medical students’ and healthcare students’ ratings. This mostly required non-parametrical statistics (Mann-Whitney tests and Kruskal-Wallis tests) only the UWE-IP-D scale allowed parametrical comparisons (students’ t-tests and ANOVAs). Since descriptive statistics for ordinal scales are often uninformative and the assumption of continuous latent variables seems plausible, we report means and standard deviations for the Likert scale items. To prevent inflation of false positive rates, we employed the Bonferroni-Holm adjustment for multiple comparisons [54] where necessary.
Results
Sample
A total of 77 students participated in the interprofessional tutor qualification program from October 2016 to October 2020. Seventy-five questionnaires were completed and included in this study (medical students, n = 75; HCS, n = 22; response rate 97%). The compositions of the cohorts and characteristics of the participants are shown in Table 2.
General attitudes towards interprofessional learning
Medical students reported higher values (M = 15.74) than HCS (M = 12.33) on the UWE-IP-D’s Interprofessional Learning Scale, t(60.4) = 4.01, p < .001, (df’s adjusted using Welch’s procedure for unequal variances). Low values indicate higher interest in Interprofessional Learning. Participants’ ratings did not differ across years, F(4, 89) = 1.036, p = .393, n.s. (Fig. 2).

Attitudes toward interprofessional education. Medical students: n = 72; HCS (healthcare students): n = 21
Assessment of the interprofessional setting
Overall, 66 students rated learning with other professions as successful (Likert scale 1 or 2), four students as partially successful (Likert scale 3), and no student as unsuccessful (Likert scale 4 or 5) (M = 1.33; SD = 0.56). The results of the quantitative assessment are shown in Table 3. In the free-text fields, 55 of the students with a positive rating gave reasons for their assessment, and all four students with a neutral rating.
-
1)
The following reasons contributed most frequently to the positive assessment (at least two mentions):
-
2)
Broadening horizons (31): get to know different experiences, exchange different points of view, gain new insights;
-
3)
Participant characteristics (10): participants’ openness, nice people;
-
4)
Trainer leadership behaviour (8): trainers are in charge of selecting the group composition, ensure a good group mix and respond to individual needs;
-
5)
Group factors (7): group composition, mixing the professions within group work;
-
6)
Group atmosphere (7): good group dynamics, excellent atmosphere.
-
7)
Medical students with a neutral rating criticized the low number of students from the other professions (2) and found that the case studies did not always fit their own profession (2).
Competency acquisition
Participants in the three study programs demonstrated good to very good competency acquisition in all areas. Data are shown in Table 4. No dependent variable showed significant differences between medical students and HCS after using Bonferroni-Holm’s adjustment for multiple comparisons [54].
Teaching approach
The teaching approach was consistently rated as very good. Here, too, no dependent variable showed significant differences between medical and other healthcare students after using Bonferroni-Holm’s adjustment for multiple comparisons [54]. Results are shown in Table 5.
In an exploratory analysis we examined potential differences across cohorts on all dependent variables with Kruskal-Wallis tests. After adjusting for multiple comparisons [54], the only significant dependent variable was “Attending the tutor-training was worthwhile” H(4) = 18.795, p < .001; all other variables’ H’s ≤ 14.486, n.s. However, it did not show a consistent trend over time (M2016 = 1.16, M2017 = 1.90, M2018 = 1.31, M2019 = 1.74, M2020 = 1.13).
The open-ended question, “Which methods/content should definitely be retained?” was answered by 90 participants, and the question, “How could the tutor training be improved?” by 86. Results are shown in Table 6.
Many participants commented positively in the free-text fields on the role plays carried out. They could slip into the role of group leaders and participants and reflect on their experiences afterwards. Some wished for more detailed instructions for these role plays. Interactive games and methods were also well received. The majority of the inputs on theories and concepts, such as learning theory [42, 45, 55], theme-centred interaction [49], group dynamics [46], were also described as helpful. Many of the students praised the variety of methods presented to them during the training. Many students also liked the alternating work in small groups and plenum. Some participants would like to have more training content: more role plays, teaching methods, and theoretical input. However, there is also feedback that the amount of theory should be reduced. Some participants commented positively on the training group, mentioning that it was a pleasant atmosphere, and some explicitly said they appreciated its interprofessionality. Some perceived the pedagogical approach of the trainers as learner-centred, individual and supportive and therefore positive. Still, others said that the trainers’ feedback mentality was a bit too pronounced throughout the training. Many participants gave feedback on the training structure, notably that the breaks and time management could be improved (e.g., contradictory feedback regarding break length or frequency, timekeeping) and that the time of the training (in the afternoon) should be changed to the morning.
Discussion
The overarching goal to redesign and implement an existing monoprofessional tutor qualification program to an interprofessional one was successfully achieved. The evaluation generally shows positive results and a high response rate, which points to the participants’ commitment and interest in the further development of teaching.
HCS scored slightly more positive (M = 12.33) on the Interprofessional Learning Scale (UWE-IP-D) than medical students (M = 15.74). This may be due to their familiarity with the theory and practice of interprofessionality. However, medical students are less likely to have the opportunity to learn together with other professions in a guided and systematic way. Overall, the attitudes of all training participants were significantly more positive than in most other studies on interprofessional learning [39, 56,57,58]. Comparably good values were only found regarding an interprofessional training ward [59] and a conversation training course for pre-licensure senior healthcare students [60]. Therefore, collaborative and active learning environments seem to foster interprofessional learning optimally.
Medical students and HCS appreciated the interprofessional setting and pointed out that their horizons were broadened by the exchange with students of other degree programs. This effect is also described in other studies [40, 61]. The willingness of students to engage in a nondiscriminatory exchange with each other even exceeded our expectations. It may have been advantageous that many of the students within the same study program were also unfamiliar before the course began. Also, we decided that participants would get to know each other (with the help of icebreaker exercises) without knowing about their respective memberships in different study programs.
Furthermore, the group composition was carefully designed to be as balanced as possible regarding gender and degree program in all small group exercises. Students mentioned that changing group compositions during the training challenged them to work together in different constellations. However, some students criticised the uneven design about the number of participants from other professions. Medical students, in particular, complained that a higher number of HCS would have facilitated interprofessional learning better.
In terms of teaching methods, students rated the group and role plays particularly positively. Interactive teaching methods have proven effective for interprofessional training in general [62], and role-plays be practical regarding communication skills [63, 64]. Many students particularly welcomed the mix of theory and practice and the exposure to specific concepts. By conveying new content to all participants, a common foundation was created on which the subsequent discussion and work processes were built. As a result, existing subject differences faded at times into the background. The program seemed to transcend subject boundaries: Students no longer seemed to be aware of their different degree programs while solving everyday tasks and slipping into the role of a future tutor. An awareness replaced the perception of differences that all future tutors have similar fears, goals and work processes to shape.
Khalili and Orchard stated that IPE helps to clarify one’s own professional identity and develop a dual identity. An “in-group” status substitutes out-group discrimination, and the professional identity is not lost but broadened, resulting in a “dual identity” [65, 66]. In this context, Khalili et al. stated that interprofessional interaction and critical reflection could cause an increased openness towards interprofessional collaboration. So-called transprofessional role-plays improve compassion and reliability across professions [67]. This study shows that a sense of belonging was developed between the students of the different study groups due to dealing with the new tutor role within role-plays and exchanges.
Most negative comments in free-text fields referred to “structure and organisation” despite our efforts to optimise the break times and the schedule. Evaluations of these topics seem very heterogeneous among the students, which may be due to different contextual conditions such as varying examinations schedules. No one way could be found to satisfy all students equally. However, it is not clear from this study whether the different perceptions regarding time management and feedback would have been equally evident in a monoprofessional setting. This survey also shows that contextual conditions, such as clear task descriptions, comprehensiveness of feedback and communicated time management, can be necessary for the positive evaluation of interprofessional training.
Overall, our study shows that the general attitude toward interprofessional learning and the reported learning achievements did not differ between tutors from different study programs. A multiprofessional trainer team, careful planning, balanced group composition and an interactive approach contribute substantially to the success of an interprofessional training program.
Strengths and limitations
Almost all of the trained tutors in each of the five cohorts participated in the study allowing for a high degree of confidence in the gathered data. However, generalisation to other circumstances is impossible because we conducted the study at a single site. Furthermore, we did not complete a pre-post survey, and a control group was unavailable. Therefore, we cannot safely draw causal conclusions regarding the training’s effect, most importantly, whether didactic skills and positive attitudes toward interprofessional learning were already present before the qualification program. However, our qualitative data strongly suggest a significant positive impact on participants, in line with trainers’ impressions during the training. Another methodological limitation is that the results are based on self-assessments and statements gathered directly after the training. It would be interesting to analyse the long-term influence of interprofessional education on peer teaching and professional practice in a follow-up study.
In addition, we focused on whether opening up an existing program to other student groups was successful. In further studies, we would look more closely at precisely what shapes interprofessional attitudes, how mono-, inter- and transprofessional perceptions change over the course of the training, and what contributes to success.
Conclusion
Overall, transforming an existing monoprofessional tutor qualification program into an interprofessional training program can foster tutor-specific and interprofessional competencies. The success of such training depends on balanced group compositions, contextual conditions and trainers’ leadership behaviour. Role-plays and other interactive teaching methods and opportunities to reflect on one’s future role were particularly suitable for promoting interprofessional exchange up to transprofessional exchange. The results provide important clues about the prerequisites and methodological considerations that could be important for the interprofessional redesign of existing training programs.
Availability of data and materials
The dataset used and analysed during the current study is available as supplementary material.
Abbreviations
- AaLPlus :
-
[Anatomie am Lebenden plus] Living Anatomy plus Anamnesis program
- HCS:
-
Healthcare students
- IPE:
-
Interprofessional education
- UWE-IP-D:
-
German version of the University of the West of England Interprofessional Questionnaire
References
ten Cate O, Durning S. Dimensions and psychology of peer teaching in medical education. Med Teach. 2007;29(6):546–52. https://doi.org/10.1080/01421590701583816.
Secomb J. A systematic review of peer teaching and learning in clinical education. J Clin Nurs. 2008;17(6):703–16. https://doi.org/10.1111/j.1365-2702.2007.01954.x.
Ringel N, Burmann BM, Fellmer-Drueg E, Roos M, Herzog W, Nikendei C, et al. Integrated peer teaching of communication and clinical skills: how to train student tutors? Psychother Psychosom Med Psychol. 2015;65(8):288–95. https://doi.org/10.1055/s-0034-1398549.
Goldschmid B, Goldschmid ML. Peer teaching in higher education: a review. J High Educ. 1976;5(1):9–33. https://doi.org/10.1007/bf01677204.
Moore-West M, Hennessy SA, Meilman PW, O'Donnell JF. The presence of student-based peer advising, peer tutoring, and performance evaluation programs among U.S. medical schools. Acad Med. 1990;65(10):660–1. https://doi.org/10.1097/00001888-199010000-00018.
Whitman NA. Pear teaching: to teach is to learn twice. ASHE-ERIC higher education reports no 4. Washington D.C.: Association for the Study of Higher Education; 1988. ISSN 0884-0040
ten Cate O, Durning S. Peer teaching in medical education: twelve reasons to move from theory to practice. Med Teach. 2007;29(6):591–9. https://doi.org/10.1080/01421590701606799.
Fatmi M, Hartling L, Hillier T, Campbell S, Oswald AE. The effectiveness of team-based learning on learning outcomes in health professions education: BEME guide no. 30. Med Teach. 2013;35(12):e1608–24. https://doi.org/10.3109/0142159X.2013.849802.
Yu TC, Wilson NC, Singh PP, Lemanu DP, Hawken SJ, Hill AG. Medical students-as-teachers: a systematic review of peer-assisted teaching during medical school. Adv Med Educ Pract. 2011;2:157–72. https://doi.org/10.2147/AMEP.S14383.
Dandavino M, Snell L, Wiseman J. Why medical students should learn how to teach. Med Teach. 2009;29(6):558–65. https://doi.org/10.1080/01421590701477449.
Allikmets S, Vink JP. The benefits of peer-led teaching in medical education. Adv Med Educ Pract. 2016;7:329–30. https://doi.org/10.2147/AMEP.S107776.
Lauter J, Branchereau S, Herzog W, Bugaj TJ, Nikendei C. Tutor-led teaching of procedural skills in the skills lab: complexity, relevance and teaching competence from the medical teacher, tutor and student perspective. Z Evid Fortbild Qual Gesundh wesen. 2017;122:54–60. https://doi.org/10.1016/j.zefq.2017.03.005.
Weyrich P, Celebi N, Schrauth M, Moltner A, Lammerding-Koppel M, Nikendei C. Peer-assisted versus faculty staff-led skills laboratory training: a randomised controlled trial. Med Educ. 2009;43(2):113–20. https://doi.org/10.1111/j.1365-2923.2008.03252.x.
Seifert LB, Schaack D, Jennewein L, Steffen B, Schulze J, Gerlach F, et al. Peer-assisted learning in a student-run free clinic project increases clinical competence. Med Teach. 2016;38(5):515–22. https://doi.org/10.3109/0142159X.2015.1105940.
Lockspeiser TM, O’Sullivan P, Teherani A, Muller J. Understanding the experience of being taught by peers: the value of social and cognitive congruence. Adv Health Sci Educ. 2008;13(3):361–72. https://doi.org/10.1007/s10459-006-9049-8.
Bulte C, Betts A, Garner K, Durning S. Student teaching: views of student near-peer teachers and learners. Med Teach. 2007;29(6):583–90. https://doi.org/10.1080/01421590701583824.
Carr SE, Brand G, Wei L, Wright H, Nicol P, Metcalfe H, et al. “Helping someone with a skill sharpens it in your own mind”: a mixed method study exploring health professions students experiences of Peer Assisted Learning (PAL). BMC Med Educ. 2016;16:48. https://doi.org/10.1186/s12909-016-0566-8.
Williams B, Reddy P. Does peer-assisted learning improve academic performance? A scoping review. Nurse Educ Today. 2016;42:23–9. https://doi.org/10.1016/j.nedt.2016.03.024.
Sevenhuysen S, Haines T, Kiegaldie D, Molloy E. Implementing collaborative and peer-assisted learning. Clin Teach. 2016;13(5):325–31. https://doi.org/10.1111/tct.12583.
Alvarez S, Dethleffsen K, Esper T, Horneffer A, Reschke K, Schultz JH. An overview of peer tutor training strategies at German medical schools. Z Evid Fortbild Qual Gesundh wesen. 2017;126:77–83. https://doi.org/10.1016/j.zefq.2017.09.009.
Brem BG, Schaffner N, Schlegel CA, Fritschi V, Schnabel KP. The conversion of a peer teaching course in the puncture of peripheral veins for medical students into an interprofessional course. GMS J Med Educ. 2016;33(2):Doc21. https://doi.org/10.3205/zma001020.
Wissenschaftsrat. Neustrukturierung des Medizinstudiums und Änderung der Approbationsordnung für Ärzte Modellstudiengänge - Empfehlungen der Expertenkommission zum Masterplan Medizinstudium 2020. Köln: Wissenschaftsrat; 2018. Available from: https://www.dgai.de/alle-docman-dokumente/entschliessungen-vereinbarungen/1715-neustrukturierung-des-meddizinstudiums-aenderung-aeappro-expertenkommission/file.html. Accessed 1 Apr 2022.
Kultusministerkonferenz. Masterplan Medizinstudium 2020. Berlin: Kultusministerkonferenz; 2017. Available from: https://www.kmk.org/aktuelles/artikelansicht/masterplan-medizinstudium-2020.html. Accessed 1 Apr 2022.
Gesellschaft für Medizinische Ausbildung e.V. Stellungnahme des Ausschusses Integrative Medizin und Perspektivenpluralismus. Position des Beirats und Vorstands der Gesellschaft für Medizinische Ausbildung (GMA) zum “Masterplan Medizinstudium 2020”. GMS J Med Educ. 2019;36. https://doi.org/10.3205/zma001254.
Interprofessional Education Collaborative Expert Panel. Core competencies for interprofessional collaborative practice: 2016 update. Washington, DC: Interprofessional Education Collaborative Expert Panel; 2016. https://www.aacom.org/docs/default-source/insideome/ccrpt05-10-11.pdf?sfvrsn=77937f97_2. Accessed 1 Apr 2022.
Centre For The Advancement Of Interprofessional Education (CAIPE). 2002. Available from: http://www.caipe.org. Accessed 1 Apr 2022.
Barr H, Gray R, Helme M, Low H, Reeves S. Steering the development of interprofessional education. J Interprof Care. 2016;30(5):549–52. https://doi.org/10.1080/13561820.2016.1217686.
Lingard L, Vanstone M, Durrant M, Fleming-Carroll B, Lowe M, Rashotte J, et al. Conflicting messages: examining the dynamics of leadership on interprofessional teams. Acad Med. 2012;87(12):1762–7. https://doi.org/10.1097/ACM.0b013e318271fc82.
Krautter M, Andreesen S, Kohl-Hackert N, Hoffmann K, Herzog W, Nikendei C. Cross-year peer tutoring on internal medicine wards: results of a qualitative focus group analysis. Adv Med Educ Pract. 2014;5:323–30. https://doi.org/10.2147/AMEP.S65479.
Bianchi M, Ghirotto L, Bagnasco A, Catania G, Zanini M, Aleo G, et al. Tutor and student dyadic interactions in relation to Interprofessional education and clinical care: a constructivist grounded theory study. J Adv Nurs. 2021;77(2):922–33. https://doi.org/10.1111/jan.14643.
Ledig T, Eicher C, Szecsenyi J, Engeser P. AaLplus - ein Anamnese- und Untersuchungskurs für den vorklinischen Studienabschnitt. Z Allgemeinmed. 2014;90(2):76–80. https://doi.org/10.3238/zfa.2014.0076-0080.
Schwill S, Hundertmark J, Fahrbach-Veeser J, Eicher C, Tonchev P, Kurczyk S, et al. The AaLplus near-peer teaching program in family medicine strengthens basic medical skills-a five-year retrospective study. PLoS One. 2020;15(5):e0233748. https://doi.org/10.1371/journal.pone.0233748.
Hundertmark J, Alvarez S, Loukanova S, Schultz JH. Stress and stressors of medical student near-peer tutors during courses: a psychophysiological mixed methods study. BMC Med Educ. 2019;19(1):95. https://doi.org/10.1186/s12909-019-1521-2.
Homberg A, Hundertmark J, Krause J, Brunnee M, Neumann B, Loukanova S. Promoting medical competencies through a didactic tutor qualification programme - a qualitative study based on the CanMEDS Physician Competency Framework. BMC Med Educ. 2019;19(1):187. https://doi.org/10.1186/s12909-019-1636-5.
Fellmer-Drüg E, Drude N, Sator M, Schultz JH, Irniger E, Chur D, et al. Introducing a curricular program culminating in a certificate for training peer tutors in medical education. GMS J Med Educ. 2014;31(2):1–14. https://doi.org/10.3205/zma000911.
Mahler C, Berger SJ, Karstens S, Campbell S, Roos M, Szecsenyi J. Re-profiling today's health care curricula for tomorrow’s workforce: establishing an interprofessional degree in Germany. J Interprof Care. 2015;29(4):386–8. https://doi.org/10.3109/13561820.2014.979980.
Ullrich C, Mahler C, Forstner J, Szecsenyi J, Wensing M. Teaching implementation science in a new master of science program in Germany: a survey of stakeholder expectations. Implement Sci. 2017;12(1):55. https://doi.org/10.1186/s13012-017-0583-y.
Hundertmark J, Homberg A, Alvarez S, Lauber H, Berger S, Büscher C, et al. Practice report / Bericht aus der praxis: tutor training for a peer-assisted interprofessional communication seminar: a work in progress. Z Evid Fortbild Qual Gesundh wesen. 2017;122:61–3. https://doi.org/10.1016/j.zefq.2017.04.003.
Berger S, Mahler C, Krug K, Szecsenyi J, Schultz JH. Evaluation of interprofessional education: lessons learned through the development and implementation of an interprofessional seminar on team communication for undergraduate health care students in Heidelberg - a project report. GMS J Med Educ. 2016;33(2):Doc22. https://doi.org/10.3205/zma001021.
Arnold C, Berger S, Gronewold N, Schwabe D, Götsch B, Mahler C, et al. Exploring early interprofessional socialization: a pilot study of student’s experiences in medical history taking. J Interprof Care. 2020:1–8. https://doi.org/10.1080/13561820.2019.1708872.
Weber T, Hoffmann H. The subjective experience of collaboration in interprofessional tutor teams: a qualitative study. GMS J Med Educ. 2016;33(2):Doc25. https://doi.org/10.3205/zma001024.
Lefrançois GR. Psychologie des Lernens. 5th ed. Berlin: Springer; 2015. ISBN 978-3-642-41971-3
Wahl D, Meyer H, Schlee J, Schubiger A. Wirkungsvoll unterrichten in Schule, Hochschule und Erwachsenenbildung : von der Organisation der Vorkenntnisse bis zur Anbahnung professionellen Handelns. Bad Heilbrunn: Julius Klinkhardt; 2020. ISBN 978-3-7815-2355-5
Jank W, Meyer H. Didaktische Modelle. 13th ed. Berlin: Cornelsen; 2019. ISBN 978-3-589-21566-9
Kolb DA. Experiential learning : experience as the source of learning and development. 2nd ed. Upper Saddle River: Pearson Education LTD; 2014. ISBN 978-0-13-389251-2
Meredith Belbin R. Management teams: why they succeed or fail. 3rd ed: Human Resource Management International Digest. 2011;19(3). https://doi.org/10.1108/hrmid.2011.04419cae.002.
Stahl E. Dynamik in Gruppen: Handbuch der Gruppenleitung. 3rd ed. Weinheim: Beltz; 2012. ISBN 978-3-621-27775-4
Billig M. Kurt Lewin’s leadership studies and his legacy to social psychology: is there nothing as practical as a good theory? Social psychology. JTSB. 2015;45:440–60.
Ruth-Cohn-Institute for TCI - International. Themenzentrierte Interaktion: TZI. Göttingen: Vandenhoeck & Ruprecht; 2017. ISBN 2511-9516
Pollard K, Miers ME, Gilchrist M. Second year scepticism: pre-qualifying health and social care students’ midpoint self-assessment, attitudes and perceptions concerning interprofessional learning and working. J Interprof Care. 2005;19(3):251–68. https://doi.org/10.1080/13561820400024225.
Pollard KC, Miers ME, Gilchrist M. Collaborative learning for collaborative working? Initial findings from a longitudinal study of health and social care students. Health Soc Care Community. 2004;12(4):346–58. https://doi.org/10.1111/j.1365-2524.2004.00504.x.
Mahler C, Berger S, Pollard K, Krisam J, Karstens S, Szecsenyi J, et al. Translation and psychometric properties of the German version of the University of the West of England Interprofessional Questionnaire (UWE-IP). J Interprof Care. 2017;31(1):105–9. https://doi.org/10.1080/13561820.2016.1227964.
Kuckartz U. Qualitative text analysis: a guide to methodes, practice & using software. Los Angeles: Sage; 2014.
Holm S. A simple sequentially rejective multiple test procedure. Scand J Stat. 1979;6(2):65–70.
Reich K. Konstruktivistische Didaktik - Das Lehr- und Studienbuch. 5th ed. Weinheim: Beltz; 2012. ISBN 9783407256898
Kolb S, Vasilakis T, Stein B, Stadelmann J, Munzinger A, Fley G, et al. Attitudes and preferences concerning interprofessional education of first-year students and experienced medical and nursing staff. J Interprof Care. 2017;31(2):164–6. https://doi.org/10.1080/13561820.2017.1283301.
Lochner L, Girardi S, Pavcovich A, Meier H, Mantovan F, Ausserhofer D. Applying interprofessional team-based learning in patient safety: a pilot evaluation study. BMC Med Educ. 2018;18(1):48. https://doi.org/10.1186/s12909-018-1164-8.
Ulrich G, Homberg A, Karstens S, Mahler C. Attitudes towards interprofessional collaboration in young healthcare professionals. J Interprof Care. 2019:1–6. https://doi.org/10.1080/13561820.2019.1597839.
Mink J, Mitzkat A, Krug K, Mihaljevic A, Trierweiler-Hauke B, Gotsch B, et al. Impact of an interprofessional training ward on interprofessional competencies - a quantitative longitudinal study. J Interprof Care. 2020:1–9. https://doi.org/10.1080/13561820.2020.1802240.
Delisle M, Grymonpre R, Whitley R, Wirtzfeld D. Crucial conversations: an interprofessional learning opportunity for senior healthcare students. J Interprof Care. 2016;30(6):777–86. https://doi.org/10.1080/13561820.2016.1215971.
Homberg A, Mink J, Karstens S, Mahler C. Learning about professional theories, models and concepts within an interprofessional seminar for undergraduate healthcare students. JIEP. 2019;17. https://doi.org/10.1016/j.xjep.2019.100272.
Barr H, Ford J, Gray R, Helme M, Hutchings M, Low H, et al. Interprofessional education guidelines: CAIPE: Centre for the Advancement of Interprofessional Education; 2017. 01.11.2020. Available from: https://www.caipe.org/news/guidance-on-global-interprofessional-education-and-collaborative-practice-research
Wershofen B, Heitzmann N, Beltermann E, Fischer MR. Fostering interprofessional communication through case discussions and simulated ward rounds in nursing and medical education: a pilot project. GMS J Med Educ. 2016;33(2):Doc28. https://doi.org/10.3205/zma001027.
Windish DM, Price EG, Clever SL, Magaziner JL, Thomas PA. Teaching medical students the important connection between communication and clinical reasoning. J Gen Intern Med. 2005;20(12):1108–13. https://doi.org/10.1111/j.1525-1497.2005.0244.x.
Khalili H, Orchard C, Laschinger HK, Farah R. An interprofessional socialization framework for developing an interprofessional identity among health professions students. J Interprof Care. 2013;27(6):448–53. https://doi.org/10.3109/13561820.2013.804042.
Khalili H. Interprofessional socialization and dual identity development amongst cross-disciplinary students. Ontario; 2013. Available from: https://mobt3ath.com/uplode/books/book-39277.pdf. Accessed 1 Apr 2022.
Ohta R, Ryu Y, Yoshimura M. Realist evaluation of interprofessional education in primary care through transprofessional role play: what primary care professionals learn together. Educ Prim Care. 2021;32(2):91–9. https://doi.org/10.1080/14739879.2020.1858349.
Acknowledgements
We would like to acknowledge Simone Alvarez, Friederike Böhlen, Johannes Inhoffen and Heike Lauber. They supported the conduction and further development of the program and all students for participating in the evaluation.
Funding
Open Access funding enabled and organized by Projekt DEAL. Funding for the study was received from the State Ministry of Baden-Wuerttemberg for Sciences, Research and the Arts as part of the “Sonderlinie Medizin” project. The funding body was not involved in the study’s design, data collection, analysis, or interpretation of data, nor was it involved in writing the manuscript.
Author information
Authors and Affiliations
Contributions
AH and JH conceived and designed the study; SZ and AH performed qualitative analyses; JH and AH analysed quantitative data. All authors interpreted data and discussed the results. AH drafted the manuscript in close cooperation with JH and SZ. The other authors reviewed the manuscript; CM focused on interprofessional education, JHS focused on medical education, and SL concentrated on structure and coherence. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The project received ethics approval from the Ethics Committee of the Medical Faculty of the University of Heidelberg, no. S-276/2015 before starting the study. All participants received written information in advance about the survey process and the aim of the study. We obtained informed consent from all participants. All participants declared in writing their willingness to participate voluntarily before the start of the study. During the investigation, we assigned de-identified pseudonyms to ensure participants’ privacy and blinding in all quantitative and qualitative analyses. We confirm that all methods were performed by the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
None declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Suplementary Table.
Evaluation Data from the cohorts 2016-2020.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Homberg, A., Ziegler, S., Mahler, C. et al. Opening up a tailored tutor qualification program for medical students to other healthcare students – a mixed-method study. BMC Med Educ 22, 251 (2022). https://doi.org/10.1186/s12909-022-03304-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-022-03304-y