
Abstract
Background
Prevention and treatment of stroke are extremely important to reduce the incidence of stroke-related disability and the associated death. This study aimed to investigate the current ability of community doctors in stroke management in the Jinjiang district of Chengdu, China, and the effect of intensive education on stroke prevention and management ability of these doctors.
Methods
A self-designed questionnaire was used to investigate the current status of stroke management by community doctors in the Jinjiang district. Subsequently, a series of intensive stroke management education courses for community doctors was designed according to the relevant guidelines for cerebrovascular accident prevention and treatment in China. All community doctors were trained, and their ability to treat and prevent stroke was reassessed using the self-designed questionnaire.
Results
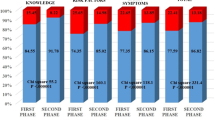
Of the 450 questionnaires issued, 370 (82.2%) and 389 (86.4%) community doctors were enrolled before and after intensive education, respectively. The results showed that only 37.8% of the community doctors in the Jinjiang district knew the guidelines for the prevention and treatment of cerebrovascular diseases, and only 45.9% thought they had stroke management ability. The stroke management ability of community doctors improved after intensive education (p < 0.05), including pre-hospital identification and management of stroke, and management of its risk factors.
Conclusions
The capacity of community doctors in the Jinjiang district of Chengdu is far from meeting the requirements of stroke prevention and treatment. However, the stroke management ability of the community doctors was greatly improved by promoting intensive education.
Similar content being viewed by others


Background
Ischaemic stroke was the cause of approximately 0.73 million deaths in China in 2016, accounting for nearly 40% of deaths from stroke, 70% of new-onset strokes, and 78% of the prevalence of stroke in China [1, 2]. Under the current community medical service model in China, community medical staff plays an important role in the stroke prevention and treatment system [3]. Presently, except for the relatively high quality of community medical staff in Beijing, Shanghai, and other developed areas, the theory and management ability of stroke of community medical staff in other areas are inadequate [4, 5]. A few studies have reported that the prevention and treatment ability of Chinese community doctors require improvement [3,4,5]. Only when these doctors fully grasp the principles of diagnosis and treatment can patients receive the most timely and appropriate treatment. The purpose of this study was to investigate the current standard of stroke management among community doctors in the Jinjiang district of Chengdu, to re-evaluate their ability after intensive education, and to determine the effectiveness of intensive education.
Methods
Sample
We conducted a survey of community doctors from nine communities (Chunxi, Yanshikou, Niushikou, Hongsha, Jinjiang, Lianxin, Wanke, Quan subtree, and Daci temple) in the Jinjiang district of Chengdu (China) from February 2017 to February 2019. According to the method for estimating the minimum sample size of quantitative data recommended by the Chinese Residents of Nutrition and Health Survey in 2002, 450 community doctors in Jinjiang district were considered an appropriate sample number and these doctors were randomly selected. A cluster sampling method was adopted, selecting 50 doctors in each community.
Ethical approval for this study was obtained from the Medical and Health Research Ethics Committee of the Second People’s Hospital of Chengdu, China. Written informed consent was obtained from all the participants. All methods were carried out in accordance with the pertinent literature on prevention and treatment of acute ischemic stroke (AIS) and the Chinese guidelines for the secondary prevention of ischemic stroke and transient ischemic attack (TIA) [6,7,8,9,10,11].
Survey contents
Based on the Chinese guidelines for the prevention and treatment of AIS and the Chinese guidelines for the secondary prevention of ischemic stroke and transient ischemic attack (TIA) [6, 7, 9,10,11], a questionnaire on the current status of stroke management ability of community doctors was designed to conduct a cluster sampling survey among doctors from nine communities in the Jinjiang district. The questionnaire contained 23 questions, which were divided into three main sections:
-
(1).
Basic information: sex, age, education, title, specialty before engaging in community health services, general practitioner education status, time spent performing clinical work, engagement in community health services, among others.
-
(2).
Concepts related to early recognition and emergency treatment for stroke: pre-hospital stroke identification, assessment (including knowledge of stroke warning signs), and processing (awareness of thrombolytic therapy and its time window; airway management; assessment of circulation; monitoring of heart function, inhaled oxygen supply, and blood glucose; establishment of intravenous route; and transfer of patients to the nearest comprehensive stroke center as soon as possible).
-
(3).
Knowledge about secondary stroke prevention: risk factors for stroke; definition and management of TIA; general and ideal goal for target blood pressure, HbA1c, and international normalized ratio levels; and awareness of statin, warfarin, and antiplatelet therapies and their side effects. We conducted stroke health education activities with the theme “understanding stroke” and evaluated the outcome. We designed a series of intensive stroke management education courses for community doctors according to the relevant guidelines for cerebrovascular prevention and treatment in China [6,7,8], including the management of major modifiable risk factors for stroke (hypertension, smoking, diabetes, carotid stenosis, atrial fibrillation, dyslipidemia, lack of physical exercise, unhealthy dietary habits, alcohol consumption, drug abuse, and obesity).
Intensive education was conducted through face-to-face lectures, online education, and the distribution of handouts and information manuals by experts in the area. The doctors were reassessed before and after the intensive education, using the self-designed questionnaire to determine whether the education could improve their stroke management ability.
Statistical analysis
After sorting out the data processing and survey data, the data were entered into the EPIDATA database and then imported into SPSS version 22 (IBM Corp., Armonk, NY, USA) for statistical analysis. Descriptive statistical analysis was used to assess the general characteristics of respondents, identify stroke-related risk factors, identify warning symptoms of stroke, and identify management ability of stroke. Chi-square test was used to analyze the general characteristics of doctors before and after intensive education and the doctors’ knowledge of stroke-related knowledge and management ability of stroke before and after intensive education. Continuous and normally distributed variables were expressed as the mean ± standard deviation, and variables not normally distributed were expressed as medians (interquartile ranges). Categorical data were described as frequencies and percentages. P value less than 0.05 was regarded as statistically significant.
Results
Questionnaire responses
In total, 450 questionnaires were issued before intensive education, 370 of which were returned, indicating a valid response rate of 82.2%. After the intensive education, 450 questionnaires were reissued, 389 of which were returned, indicating a valid response rate of 86.4%.
General information of respondents
In total, 370(82.2%) and 389(86.4%) community doctors were enrolled before and after intensive education, respectively. The general information (sex, age, educational level, professional title, specialty before engaging in community health services, general practitioner education status, education time, clinical experience time, and community service experience time) of the respondents before and after intensive education showed no significant difference between the two groups (Table 1).
Stroke management ability of community doctors before intensive education
The results of our study showed that only 7.0% (26/370) of the community doctors had knowledge of all the five warning symptoms of a sudden stroke, and 34.9% (129/370) did not know any of the symptoms. Furthermore, only 3% (11/370) of the respondents correctly described the pre-hospital management of acute stroke. Although most doctors knew that thrombolysis is the most effective treatment for AIS, less than half [40.3% (149/370)] knew the thrombolytic time window. Only 20.8% (77/370) named four or more risk factors for stroke, and approximately 30% (108/370) were unable to name any. Less than 50% knew how to properly manage the risk factors for stroke, such as hypertension, diabetes, and atrial fibrillation.
Stroke management ability of community doctors after intensive education
After intensive education, 13.1% (51/389) of the community doctors correctly mentioned all five warning symptoms of stroke, while 20.3% (79/389) could not mention any; and 28.0% (109/389) correctly described the pre-hospital management of acute stroke. The proportion of doctors who knew that the most effective treatment for AIS was thrombolytic therapy, along with the knowledge of its time window, increased to 61.0% (214/389). Regarding stroke prevention, 25.2% (98/389) of the community doctors named five risk factors for stroke, which was better than before (P<0.001), while 13.9% (54/389) could not name any. The proportion of community doctors who knew how to properly manage the risk factors for stroke, such as hypertension, diabetes, and atrial fibrillation, was also significantly higher (P<0.001). The results showed that the stroke management ability of community doctors improved after intensive education (Table 2).
Discussion
Previous surveys have reported that the stroke management ability of community doctors in China was low and required immediate improvement [3,4,5, 12, 13]. A study of Botswana’s community physicians also suggested that community physicians may be less likely to contribute to stroke [14]. Our survey found that only 37.8% of community doctors in the Jinjiang District of Chengdu knew the guidelines for the prevention and treatment of cerebrovascular diseases, and only 45.9% thought they had stroke management ability. The results of our study indicated that community doctors in the Jinjiang district of Chengdu lacked the ability to manage the identification and pre-hospital treatment of stroke and the secondary prevention of stroke recurrence.
This is the first study to present results on intensive education of community doctors on stroke prevention and their management ability in stroke treatment. The community doctors are the health advisors of the vast number of community residents. Only when the community doctor is familiar with the recognition, treatment, and referral of stroke, can more patients with stroke benefit.
Stroke is one of the diseases that cause human disability and death, and AIS accounts for 80% of all strokes [1]. Numerous studies have shown that improving modifiable risk factors for stroke, including hypertension, diabetes, hyperlipidemia, and smoking, can reduce the incidence of the disease [15,16,17,18]. Compared with before intensive education, the proportion of community doctors who knew how to properly manage the risk factors for stroke, such as hypertension, diabetes, and atrial fibrillation, was also significantly higher (P<0.001).
The National Stroke Registry of China reported that 17.7% of 11,560 patients with ischemic stroke or TIA experienced a recurrence within 1 year [19]. Rapid identification and treatment of TIA are important to prevent recurrence of cerebral infarction. Through intensive education, the proportion of doctors who could correctly manage TIA increased significantly (P<0.001).
The main method of AIS management is intravenous thrombolysis, and the earlier the time, the greater the benefit of patients [8]. After intensive education, the proportion of doctors who knew the most effective treatment was thrombolytic therapy and knew the time window of thrombolytic therapy increased significantly (P<0.001). Our results showed that the stroke management ability of community doctors increased after intensive education. After the education, 68.1% of community doctors in the Jinjiang District of Chengdu knew the guidelines for the prevention and treatment of cerebrovascular diseases, and 81.5% thought they had stroke management ability. Hence, this intensive education is helpful for the prevention, recognition, treatment, referral, and rehabilitation of patients with stroke.
The shortcomings of this study are as follows: (1) the scope of the survey is limited to the Jinjiang District of Chengdu, the sample size was small, and the results do not reflect the overall situation of Chengdu; (2) compared with open-ended questions, the closed questions used in this survey may have resulted in a higher response rate in the evaluation of the ability to master stroke-related knowledge; and (3) not all knowledge of stroke management was assessed in the test questionnaires.
Conclusions
In summary, the capacity of community doctors in the Jinjiang district of Chengdu is far from meeting the requirements of stroke prevention and treatment before intensive education. Intensive stroke education of community doctors proved to be beneficial in improving their theoretical knowledge and clinical management of stroke. This can help in improving the diagnosis and treatment capacity of community health centers, thereby achieving the goals of reducing the incidence and mortality of stroke. Therefore, intensive education is worth promoting.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AIS:
-
Acute ischemic stroke
- MR-CLEAN:
-
Multicenter randomized clinical trial of endovascular treatment for acute ischemic stroke in the Netherlands
- TIA:
-
Transient ischemic attack
References
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2095–128.
Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, et al. Prevalence, incidence, and mortality of stroke in China: results from a Nationwide population-based survey of 480 687 adults. Circulation. 2017;135:759–71.
Yang J, Zhang J, Ou S, Wang N, Wang J. Knowledge of community general practitioners and nurses on pre-hospital stroke prevention and treatment in Chongqing, China. PLOS ONE. 2015;10:e0138476.
Chen C, Qiao X, Kang H, Ding L, Bai L, Wang J. Community physicians' knowledge of secondary prevention after ischemic stroke: a questionnaire survey in Shanxi Province, China. BMC Med Educ. 2015;15:197.
Sim CY, Wan Zaidi WAW, Shah SA, Wan Yahya WNN, Tan HJ. Knowledge of acute stroke management among healthcare professionals: development and validation of acute stroke management questionnaire (ASMaQ). J Stroke Cerebrovasc Dis. 2021;30(1):105421.
Chinese Medical Association. Chinese national guidelines for prevention of ischemic stroke and transient ischemic attack. Chin J Neurol. 2010;43(2):1–8.
Chinese Academy of Neurology. Guidelines for the diagnosis and treatment of acute ischemic stroke in China in 2014. Chin J Neurol. 2015;4:246–57.
Meretoja A, Keshtkaran M, Tatlisumak T, Donnan GA, Churilov L. Endovascular therapy for ischemic stroke: save a minute-save a week. Neurology. 2017;88:2123–7.
Chinese Society of Gerontology, emergency medicine group. Consensus of Chinese experts on emergency treatment for acute ischemic stroke in 2018. Chin J Stroke. 2018;13:956–67.
Chinese Society of Neurology. Cerebrovascular disease Group of Chinese Society of neurology. Chinese primary cerebrovascular disease prevention guidelines 2015. Chin J Neurol. 2015;48:629–43.
Stroke screening and prevention engineering Committee of National Health and Family Planning Commission. Technical specifications for stroke screening and prevention. Chin J Neurol. 2014;47:199–202.
Meng XJ, Hou S, Fei XP, Kang ZW, Gao SL, Xu RZ, et al. Knowledge and ability of treatment of stroke among physicians in rural area of Liaoning Province. Chin Gen Pract. 2010;13:399–400.
Shuang-Xia DU, Chun-Ying LI. Community doctors should play an important role in the treatment of stroke. Med Philos(Clinical Decision Making Forum Edition) 2011.
Furie KL, Kasner SE, Adams RJ, Albers GW, Bush RL, Fagan SC, et al. Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42(1):227–76.
The multiple risk factor intervention trial research group. Mortality rates after 10.5 years for participants in the multiple risk factor intervention trial. Findings related to a priori hypotheses of the trial. The multiple risk factor intervention trial research group. JAMA. 1990;263:1795–801 PMID: 2179590.
Fortmann SP, Flora JA, Winkleby MA, Schooler C, Taylor CB, Farquhar JW. Community intervention trials: reflections on the Stanford Five-City project experience. Am J Epidemiol. 1995;142:576–86 PMID: 7653465.
Rothwell PM, Coull AJ, Giles MF, Howard SC, Silver LE, Bull LM, et al. Oxford Vaseular study. Change in stroke incidence, mortality, case-fatality, severity, and risk factors in Oxfordslhire, UK from l98l to 2004 (Oxford Vascular Study). Lancet. 2004;363:l925–33.
Cheng XM, Du XL, Wu SP, Wang WZ, Li SC, Jiang GX, et al. The interventional experiment of stroke risk factors in seven cities in the nation—incidence change. Chin J Prev Control Chronic Dis. 1992;2:43–6.
Wang Y, Xu J, Zhao X, Wang D, Wang C, Liu L, et al. Association of hypertension with stroke recurrence depends on ischemic stroke subtype. Stroke. 2013;44(5):1232–7.
Acknowledgements
We thank all community residents in the Jinjiang district of Chengdu city.
Funding
This work was funded by the Health and Family Planning Commission of Chengdu, China (2015009). The funding body was not involved in database management (collection, analysis, and interpretation of data), designing of the study, or writing of the manuscript and has no access to patient information. The study protocol underwent a peer-review process by the funding body.
Author information
Authors and Affiliations
Contributions
XMZ and YH were responsible for the study conception and design, data collection, first draft of the paper, and final manuscript. JW was responsible for the conception and design of the study and data analysis and interpretation. LYH was responsible for data collection. Xue-Min Zhong and Yao Huang contributed equally to this paper. All authors read and approved the final manuscript for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this study was obtained from the Medical and Health Research Ethics Committee of the Second People’s Hospital of Chengdu, China. Written informed consent was obtained from all the participants. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhong, Xm., Huang, Y., He, L. et al. Effect of intensive education on stroke prevention and management ability of community doctors: a cross-sectional study. BMC Med Educ 22, 53 (2022). https://doi.org/10.1186/s12909-022-03125-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-022-03125-z