
Abstract
Background
The proportion of women in medicine is approaching that of men, but female physicians are still in the minority as regards positions of power. Female physicians are struggling to reach the highest positions in academic medicine. One reason for the disparities between the genders in academic medicine is the fact that female physicians, in comparison to their male colleagues, have a lower rate of scientific publishing, which is an important factor affecting promotion in academic medicine. Clinical physicians work in a stressful environment, and the extent to which they can control their work conditions varies. The aim of this paper was to examine potential impeding and supportive work factors affecting the frequency with which clinical physicians publish scientific papers on academic medicine.
Methods
Cross-sectional multivariate analysis was performed among 198 female and 305 male Swedish MD/PhD graduates. The main outcome variable was the number of published scientific articles.
Results
Male physicians published significantly more articles than female physicians p <. 001. In respective multivariate models for female and male physicians, age and academic positions were significantly related to a higher number of published articles, as was collaborating with a former PhD advisor for both female physicians (OR = 2.97; 95% CI 1.22–7.20) and male physicians (OR = 2.10; 95% CI 1.08–4.10). Control at work was significantly associated with a higher number of published articles for male physicians only (OR = 1.50; 95% CI 1.08–2.09). Exhaustion had a significant negative impact on number of published articles among female physicians (OR = 0.29; 95% CI 0.12–0.70) whilst the publishing rate among male physicians was not affected by exhaustion.
Conclusions
Women physicians represent an expanding sector of the physician work force; it is essential that they are represented in future fields of research, and in academic publications. This is necessary from a gender perspective, and to ensure that physicians are among the research staff in biomedical research in the future.
Similar content being viewed by others


Background
During the last few decades, the number of female physicians in European countries has increased considerably and we are now approaching an even distribution between female and male physicians [1]. In Europe and North America, since the 1970s, women have entered academic fields of medicine in increasing numbers [2]. Nevertheless, female physicians are still struggling to reach the highest positions in academic medicine [3,4]. Women represent a persistently low proportion of faculty in senior and leadership roles in the field [5-8]. Female physicians face barriers to academic career progression [9] and are under-represented, compared to their male counterparts, at senior levels. For example, in the UK, one in five medical schools do not have a female professor [10], only two out of the 33 heads of medical schools are women, and at a professorial level only 11% of clinical academics are women [11]. Previous research in the field of academic medicine shows that the disparities between the genders in academic medicine are due to the fact that male physicians have a higher publishing rate than their female colleagues [12] i.e. female physicians lack this important qualification for promotion in academic medicine. One reason might be that women obtain fewer grants [13,14] and are often found to be financially disadvantaged when variations in the distribution of work time and productivity are considered [15,16]. Women are also underrepresented on the editorial boards of major medical journals [17]. In the UK, the number of female first authors in prestigious journals has increased but not as female senior authors, and we do not know if these authors have been clinical physicians [18]. The gender publication gap also exists among younger academic hospital physicians who might be expected to emphasize work-life balance and display less gender publication bias [19]. Furthermore, female physicians are less likely than male physicians to have a mentor, and this lack of mentoring could negatively affect women’s careers [20-24]. It has been reported that women with mentors produce more published work, spend more time on research activity, and have higher overall career satisfaction than those without mentors [24]. The most common obstacles identified by women faculty members in achieving career advancement goals have been shown to be clinical workload, insufficient financial support for research, and insufficient institutional support [20,25-27].
Throughout the world women leave their academic careers in far greater numbers than their male colleagues [4,28-30]. One reason may be that women suffer discrimination due to gender. For example, it has been shown that peer reviewers for research grants cannot judge scientific merit without considering gender [28-31]. The peer reviewers overestimate male achievements and/or underestimate female performance, as shown throughout multiple-regression analyses of the relationship between defined parameters of scientific productivity and competence scores, and in a meta-analysis of the peer-review process.
There is a known hierarchy within medical academic research, and this structure precludes female physicians from moving upward in the field of academic medicine [32]. The hierarchical structure in academia takes advantage of female physicians’ lack of confidence in terms of proficiency and academic achievement. Furthermore, recruitment processes are experienced as excluding women [32].
When women seek senior positions or research grants and their former advisors are co-authors on later scientific papers the women might be judged as being dependent on the former supervisor, while men might be seen as new partners [3]. To establish an academic career, younger researchers need to show their independence, and it is difficult to get your own research grants if you have been assessed as dependent [28]. However, we lack research about whether collaboration with a former advisor has any impact on future publications.
In the US, the under-representation of female physicians in higher ranks of academic medicine has been found to be partly related to work time and high stress [20]. Competing demands of research, teaching and clinical work are difficult to cope with for all clinical academics [33]. One of the most common obstacles identified by women faculty members in achieving career advancement goals is clinical workload. In a Polish longitudinal study, low levels of stress and burnout experienced by the physician were prerequisites for success in a medical career [34]. Hence, it is important to consider the influence of exhaustion on the number of publications. Job demands have been found to be the most important antecedents of exhaustion [35-37].
In societies that value gender equality, it is unacceptable for medical research to lag behind in this respect. Although research is supposed to be objective, in reality it is influenced by the researcher [38], which is why it is relevant that the female population is represented by female medical researchers.
Aim of the study
Discovering which factors interfere with the biomedical research of female physicians is a necessary step for increasing the number of active female physician scientists and for ensuring that physicians are among the research staff of the future. Previous studies have highlighted gender differences in academic medical publications. This is, to our knowledge, the first study that statistically analyses work-related factors related to this publication gap where the number of publications is the outcome variable. We wish to examine gender differences among clinical physicians working at a university hospital and who also have a PhD. Having control over the amount of work assigned, setting one’s own work hours, and continuing to collaborate on research with a former PhD advisor are hypothesized to be associated with a higher rate of publication. In contrast, exhaustion is hypothesized to be associated with a lower incidence of academic publication.
Methods
Settings
The HOUPE study is a longitudinal research program concerning work-related health, organizational culture, career paths and working conditions in university hospitals in several European countries. In Sweden, the study was carried out in 2005 at large governmental university hospitals in the central part of the country. A letter was sent to each eligible physician. The letter contained a personal password and log-on information to access the web-based questionnaire. Four reminders to participate were sent by email. In addition, a paper version of the questionnaire was sent in order to provide an alternative for those who were reluctant to respond electronically. The study was reviewed and approved by the Regional Ethics Board (Stockholm) on 8 December 2004, number 04-913/2. Further details about the HOUPE study are presented in work by Fridner et al. cited in the references [39-41].
Participants
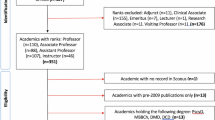
Eligible physicians (permanently employed and actively working) received written information about the survey, together with endorsements by the director of the University Hospital, the chairperson of the local medical association, and the project manager. The response rate was 59.8%, and the response rate for female physicians was slightly higher than for male physicians (65% and 53.7% respectively). The present paper includes the 503 physicians who stated that they had a PhD, 198 (51.4%) of the female physicians, and 305 (66.9%) of the male physicians.
Dependent variable
The outcome variable, number of published articles, was assessed by using the Physician Career Path Questionnaire (PCPQ) [3]. In the present study, a dichotomization was made between < =16 and >16 articles. We chose this cut-off point since having more than 16 published articles demonstrates a continuous record of publishing following a PhD degree, and entitles a person to apply for associate professorship in Sweden [42].
Independent variables
The independent factor of Are you still doing research with your former thesis advisor? (with answers divided into “Yes” or “No”), and academic position were both assessed by using PSPQ [3].
Age groups were divided into three categories: “younger than 40 years of age”, “40-54 years of age” and “55 years of age or older”. Factors regarding civil status (in a relationship, married/living with a partner or single, divorced/separated), number of children, number of children under the age of 18 years living in the household, and number of children before gaining PhD degree were also included in the analysis.
Exhaustion was measured according to a five-item scale (α = 0.80, e.g. “After my work, I usually feel worn out and weary”) based on the “Mini Oldenburg Burnout Inventory” (MOLBI) [36]. This dimension was measured by four answer options: “totally agree”, “agree”, “disagree” and “totally disagree”.
We assessed items from the Nordic Questionnaire for Psychological and Social Factors at Work (QPS-Nordic) [43] concerning control over the amount of work assigned and setting one’s own work hours, each measured using a scale with a 5-point range from “never or very seldom” (1) to “very often”(5), with α = 0.83.
Statistical analysis
The socio-demographics and other characteristics of the physicians with a PhD were assessed by numerical count and percentages, as well as by means and standard deviation. Chi square tests for discrete variables and independent-sample t-tests for scales were used to compare female and male physicians who had a PhD degree. First, bivariate logistic regression was performed with each of the potential independent variables to find the significant and near significant unadjusted odds ratios (ORs) with respect to the outcome. We performed multiple logistic regressions (MLOGR) to identify parsimonious sets of non-colinear independent variables that explained the largest amount of variance for the outcome variable. This analysis was conducted separately for the female and male physicians. Statistical analysis was performed using SPSS software (SPSS version 21, SPSS Inc., Chicago, Illinois).
Results
The characteristics of physicians with a PhD are reported with frequency distributions in Table 1.
Male physicians had published significantly more scientific articles, χ2 (2) = 30.113 (p = 0.001). There were no significant differences in age, χ2 (2) = 4.160 (p >0.05, ns). Significantly more men compared to women were in a relationship χ2 (1) = 9.630 (p = 0.002). A χ2-test also showed a significant relationship between gender and number of children χ2 (2) = 8.730 (p = 0.013), in that male physicians had more children than their female colleagues, and the same was true for the number of children under 18 years currently in the household χ2 (2) = 8.691 (p = 0.013). The number of physicians who already had children before taking a PhD was also examined in the study, and the result showed a significant difference χ2 (2) = 6.797 (p = 0.033). More women compared to men had their children before taking a PhD. Male physicians held academic positions to a significantly higher degree than female physicians χ2 (3) = 10.017 (p = 0.018).
There were no significant differences as regards collaboration with a former thesis advisor, χ2 (2) = 4.948 (p = 0.05, ns).
In the study, sex differences relating to control over one’s work were analysed by comparing, for each gender, the self-estimated level of control over the amount of work assigned, work pace, the possibilities for breaks, and the extent to which it was possible to set one’s own work hours. The results are presented in Table 1. Male physicians reported greater freedom to control their work in terms of work-time flexibility and work pace, t (483) = 5.138 (p = 0.001). Furthermore, a comparison of the level of exhaustion in women and men was made, which found a significant difference between female and male physicians, t (480) = −4.748 (p = 0.001), in that female physicians experienced greater exhaustion.
On bivariate logistic regression, for both genders, the non-adjusted risk estimates for various factors suggested a significant relationship between the quantity of scientific work published and age, academic position, collaboration with a former PhD thesis advisor, control over work pace, and number of children living in the household under 18 years old (Table 2). Exhaustion had a significant association with the number of scientific publications for female physicians only.
In Table 3 an adjusted Odds Ratio (OR) and Confidence Intervals (CI) from the multiple logistic regression models are presented, which compare research publications among female and male physicians with a PhD. Age and academic position were significantly related to a higher rate of published articles for both female and male physicians (OR = 3.22; 95% CI 1.36-7.61 and OR = 2.30; 95% CI 1.31-4.04) and (OR = 3.09; CI 1.87-5.12 and OR = 2.54; CI 1.92-3.36) respectively. Female and male physicians collaborating with former PhD advisors published more articles than those not collaborating with former advisors: female physicians (OR = 2.97; 95% CI 1.22–7.20) and male physicians (OR = 2.10; 95% CI 1.08–4.10). Control at work was significantly associated with a higher number of published articles for male physicians (OR = 1.50; 95% CI 1.08–2.09) but not for females. Exhaustion had a significant negative association with the number of published articles among female physicians (OR = 0.29; 95% CI 0.12–0.70), whilst the publishing rate among male physicians was not significantly affected by exhaustion.
Discussion
This study investigated factors that impede or support scientific publication among female and male physicians with a PhD working at a university hospital. Our findings show that male physicians published significantly more scientific articles compared to female physicians. Having control over one’s work, still collaborating with former thesis advisors, and not experiencing exhaustion were all associated with a higher number of published articles.
To our knowledge, this is the first report to compare work conditions and academic production among female and male physicians with a PhD (in Sweden the granting of a PhD in academic medicine requires the candidate to have a minimum of six peer-reviewed published articles) working in the same university hospital. The advantages of quite a high response rate and a large sample size strengthen the power of this study. Women publish less, and one reason might be an uneven distribution of research funds between women and men, in that women are given less funding than their male colleagues. In reviewing applications to the Swedish Council for Working Life and Social Research (FAS), the analysis showed that female applicants were less likely than men to get research grants. In turn, men’s applications received higher ratings than women’s in peer reviews [44]. However, women were less likely to apply for funding than men and they request smaller amounts of money [45].
There have been suggestions that female researchers’ careers are delayed due to childbearing after being awarded the PhD, when one is supposed to start one’s career. The biological clock clashes with the tenure clock. However, in our population, 80.7% of the female physicians had children before receiving their PhD degree; i.e. they had already simultaneously engaged in both work as physicians and the writing of articles for their thesis. Previous research by Fridner [3] confirms this by showing that in fact the male physicians were more likely to become parents after taking a PhD than their female colleagues. We always control for age, civil status and amount of children when we use binary logistic regression. Most of the literature on women, academic productivity and children are from the 90s. In Sweden fathers, especially well educated, are on parental-leave and stay at home from work when their children are sick. Therefore, we did not find it necessary to include child-care in the hypothesis, and our results show that children did not turn out to be a significant factor for non-publication.
It was hypothesized that collaboration with former PhD advisors would be associated with the publication of a greater number of articles. Through such collaboration, physicians had access to a role model. A high quality relationship with one’s advisor may also alleviate the influence of job demands on job strain [37]. We found that both female and male physicians published more when they had continued to collaborate with a former thesis advisor, compared to those who did not. This result is appealing, considering that previous research indicates that male advisors tend to favour male PhD students with the resources and tools they need for advancement in their academic careers. Women have more often reported that their mentor has taken credit for their work [29].
The results in this study showed that physicians with more control over work time and work pace had a higher publishing rate. It was shown that men, to a greater extent than women, experienced this control. Such control gave them an opportunity to plan their time when conducting clinical research and writing scientific articles. This can be related to earlier research indicating that the work environment influences one’s creativity and innovation [46]. Hence, it can be presumed that positive work conditions promote achievements in research. Since the male physicians in the present study felt more satisfied regarding control at work, it is possible that this is linked to the higher publishing rate among men. For female physicians, no such relation between publication and control over their work was found. Furthermore, it can be assumed that the feeling of control also diminishes the risk of exhaustion, at least for male physicians. This is the first time that a study in this field has shown that lack of control over work time and work pace may have a negative impact on publishing rate for physicians in academic medicine. This result is in line with earlier research which found the work environment to be strenuous, especially for women, due to hierarchical structures in academic medicine [32]. Previous research has revealed that there is a will in academic medicine to move towards non-hierarchical structures. Therefore, organizations with a flatter structure could promote more innovative and creative work environments [45]. Other research recommends an institutional approach that acknowledges the impact of hidden gender-linked biases in academic medicine that marginalize women and negatively affect their well-being [47].
It is known that women physicians experience greater exhaustion than men [48-51], and this is confirmed in our study. To our knowledge, no earlier research has found that exhaustion may prevent women from publishing scientific articles. In the present study it was hypothesized that exhaustion could negatively affect a person’s publishing rate. It seemed unexpectedly the direction could be that low publication rate would increase the risk of exhaustion. The study found that female physicians suffered from exhaustion to a greater extent than their male colleagues. In addition, exhaustion was a risk factor for women’s lower publishing rate. Previous research has shown that both interpersonal and social factors predict exhaustion among physicians [52]. It is important for hospital organizations to prevent these kinds of problems. Today, young women represent a larger proportion of the total number of medical students than previously, and thus more women are likely to become future researchers in biomedical medicine. Clinical research tends to become deficient when female physicians are not included in networks of academic medicine. Moreover, they do not achieve the same publishing rate as male physicians and they are not promoted to high positions [53,54]. As female physicians are more exposed to exhaustion, this factor may also have a negative impact on future clinical research.
Limitations
Our data is cross-sectional, and thus excludes conclusions about the directionality of the associations we have found. The results are from one hospital, but this academic hospital demands a PhD from physicians in order to qualify for a major position. In the future, this might be the case for all university hospitals, which will increase competition within academic medicine. Due to the anonymity of the data, a multilevel analysis, in which departments and units could be separated, has not been possible.
Conclusions
Considering that women physicians are an increasing proportion of the physician work force it is essential that they are also represented in the future field of research and academic publications. Control over work, and issues of work-related health such as exhaustion, need to be acknowledged within academia in order to achieve this aim.
References
Johannesson KA, Hagen TP. Variations in labour supply between female and male hospital physicians: result from a modern welfare state. Health Policy. 2011;107:74–82.
Buddeberg-Fischer B, Leemann R, Klaghofer R. Sociodemographic and career aspects in female and male faculty members of Swiss medical schools. Swiss Med Wkly. 2003;133:318–22.
Fridner A. Career paths and career patterns among physicians with a PhD. PhD thesis. Uppsala University, Department of Psychology; 2004.
Kilminster S, Downes J, Gough B, Murdoch-Eaton D, Roberts T. Women in medicine – is there a problem? A literature review of the changing gender composition, structures and occupational cultures in medicine. Med Educ. 2007;41:39–49.
Nonnemaker L. Women physicians in academic medicine: new insights from cohort studies. N Engl J Med. 2000;342:399–405.
Yedidia MJ, Bickel J. Why aren’t there more women leaders in academic medicine? The views of clinical department chairs. Acad Med. 2001;76:453–65.
Darcy A, Reed MD, Enders F, Lindor R, McClees M, Lindor KD. Gender differences in academic productivity and leadership appointments of physicians throughout academic careers. Acad Med. 2011;86:1.
Wagner AK, McEllington J, Chan L, Wagner III EP, Segal N, Gerber LH. How gender impacts career development and leadership in rehabilitation medicine: a report from the AAPM &R Research Committee. Arch Phys Med Rehabil. 2007;88:560–8.
Medical Academic Staff Committee. Health policy and economic research unit. Women in academic medicine: challenges and issues. London: British Medical Association; 2004.
Sandhu B, Margerison C, Holdcroft A. Women in the UK medical academic workforce. Med Educ. 2007;41:909–14.
London Medical Schools Council. Women in clinical academia. Attracting and developing the medical and dental workforce of the future. 2007.
Kaufman RR, Chevan J. The gender gap in peer-reviewed publications by physical therapy faculty members: a productivity puzzle. Phys Ther. 2011;91:122–31.
Jagsi R, Guancial E, Worobey C, Henault L, Chang Y, Starr R, et al. The “gender gap” in authorship of academic medical literature: a 35-year perspective. N Engl J Med. 2006;355:281–7.
Valian V. Why so slow: the advancement of women. Cambridge MA: MIT Press; 1999.
Ash AS, Carr PL, Goldstein R, Friedman RH. Compensation and advancement of women in academic medicine. Is there equity? Ann Intern Med. 2004;141:205–12.
Wright AL, Schwindt LA, Bassford TL, Reyna VF, Shisslak CM, St Germain PA, et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one U.S. College of medicine. Acad Med. 2003;78:500–8.
Amrein K, Langmann A, Fahrleitner-Pammer A, Pieber TR, Zollner-Schwetz I. Women underrepresented on editorial boards of 60 major medical journals. Gend Med. 2011;8:378–88.
Sidhu R, Rajashekhar P, Lavin VL, Parry J, Attwood J, Holdcroft A, et al. The gender imbalance in academic medicine: a study of female authorship in the United Kingdom. J R Soc Med. 2009;102:337–42.
Tevik Løvseth L, Cüneyt Güzey I, Fridner A, Minucci D, Linaker OM. Age and gender differences in authorship among university hospital physicians in Sweden, Norway and Italy (The HOUPE Study). Br J Med Med Res. 2014;27:4582–90.
Blood EA, Ulrich NJ, Hirshfeld-Becker DR, Seely EW, Connelly MT, Warfield CA, et al. Academic women faculty: are they finding the mentoring they need? J Womens Health. 2012;21(11):1201–8.
Pololi L, Knight S. Mentoring faculty in academic medicine. A new paradigm? J Gen Intern Med. 2005;20:866–70.
Mayer AP, Files JA, Ko MG, Blair JE. Academic advancements of women in medicine: do socialized gender differences have a role in mentoring? Mayo Clin Proc. 2008;83:204–7.
Reid MB, Misky GJ, Harrisson RA, Sharpe B, Auerbach A, Glasheen JJ. Mentorship, productivity, and promotion among academic hospitalists. J Gen Intern Med. 2011;27:23–7.
Stamm M, Buddeberg-Fischer B. The impact of mentoring during postgraduate training on doctors’ career success. Med Educ. 2011;45:488–96.
Levinson W, Kaufman K, Clark B, Tolle SW. Mentors and role models of women in academic medicine. West J Med. 1991;154:423–6.
Carr PL, Pololi L, Knight S, Conrad P. Collaboration in academic medicine: reflections on gender and advancement. Acad Med. 2009;84:1447–53.
Sambunjak D, Straus SE, Marusic A. Mentoring in academic medicine. A systematic review. JAMA. 2006;296:1103–15.
Waisbren SE, Bowles H, Hasan T, Emans SJ, Goldberg C, Gould S, et al. Gender differences in research grants applications and funding outcomes for medical school faculty. J Womens Health. 2008;17:207–14.
Wennerås C, Wold A. Nepotism and sexism in peer-review. Nature. 1997;387:341–3.
Bickel J. The work that remains at the intersection of gender and career development. Arch Phys Med Rehabil. 2007;88:683–6.
Hamel MB, Ingelfinger JR, Phimister E, Solomon CG. Women in academic medicine. Progress and challenges. N Engl J Med. 2006;355:310–2.
Bornmann L, Mutz R, Daniel HD. Gender differences in grant peer review: a meta-analysis. J Informetrics. 2007;1:226–38.
Conrad P, Carr P, Knight S, Renfrew MR, Dunn MB, Pololi L, et al. Hierarchy as a barrier to advancement for women in academic medicine. J Womens Health. 2010;19:799–805.
Dacre J, Shepherd S. Women and medicine. Clin Med. 2010;10:544–7.
Tartas M, Walkiewicz M, Majkowicz M, Budzinski W. Psychological factors determining success in a medical career. A 10-year longitudinal study. Med Teach. 2011;33:163–72.
Demerouti E, Bakker AB, Vardakou I, Kantas A. The convergent validity of two burnout instruments: a multitrait-multimethod analysis. Eur J Psychol Assess. 2003;19:12–23.
Bakker AB, Demerouti E. The Job demands-resources model: state of the art. J Managerial Psychol. 2007;22:309–28.
Rosenthal R. Covert communication in classrooms, clinics, courtrooms and cubicles. Am Psychol. 2002;57:839–49.
Fridner A, Belkic K, Marini M, Minucci D, Pavan L, Schenk-Gustafsson K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (The HOUPE Study): Cross-Sectional Associations With Work Stressors. Gend Med. 2009;6:314–28.
Fridner A, Belkić K, Minucci D, Marini M, Putoto G, Simonato P, et al. Work environment and recent suicidal thoughts among male university hospital physicians in Europe (HOUPE) study. Gend Med. 2011;8:269–79.
Fridner A, Belkić K, Marini M, Gustafsson Sendén M, Schenk-Gustafsson K. Why don’t academic physicians seek needed professional help for psychological distress? Swiss Med Wkly. 2012;142:1–8.
Karolinska Institutet. Docent Committee, Dnr 2517/2006-660. Stockholm: Karolinska Institutet; 2006.
Lindström K. User’s guide for the QPS – Nordic. General nordic questionnaire for psychological and social factors at work. Copenhagen, Denmark: Nordic Council of Ministers; 2000.
Norström T. Men are more likely than women to receive research funding from FAS. [article in Swedish]. Lakartidningen. 2012;109:1962–3.
European Commission EUR 23721 EN. The gender challenge in research funding. Assessing the European national scenes. 2009.
Landman S, Dandalou V. Complex manifestations of gender disparity in academic medicine. Open Womens Health J. 2009;3:5–10.
Pololi LH, Civian JT, Brennan RT, Dottolo AL, Krupat E. Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2012;28:201–7.
Canvinet C, Östergren P-O, Lindeberg S, Choi B, Karasek R, Moghadassi M, et al. Conflict between the work and family domains and exhaustion among vocationally active men and women. Soc Sci Med. 2010;70:1237–45.
Evengård B, Jacks A, Pedersen NL, Sullivan PF. The epidemiology of chronic fatigue in the Swedish Twin Registry. Psychol Med. 2005;35:1317–26.
Schuitemaker GE, Dinant MD, van der Pol GA, Appels A. Assessment of vital exhaustion and identification of subjects at increased risk of myocardial infarction in general practice. Psychosomatics. 2004;45:414–8.
Sjögren E, Kristenson M. Can gender differences in psychosocial factors be explained by socioeconomic status? Scand J Public Health. 2006;34:59–68.
Kowalski C, Ommen O, Driller E, Ernstmann N, Wirtz M, Köhler T, et al. Burnout in nurses – the relationship between social capital in hospitals and emotional exhaustion. J Clin Nurs. 2010;19:1654–63.
Carnes M, Morrissey C, Geller SE. Women’s health and women’s leadership in academic medicine: hitting the same glass ceiling? J Women Health. 2008;17:1453–62.
Lee RT, Seo B, Hladkyj S, Lowell BL, Schwartsmann L. Correlates of physicians’ burnout across regions and specialties: a meta-analysis. Hum Resour Health. 2013;11:48.
Acknowledgements
The authors are grateful to the physicians who participated in this study. The authors are also grateful to Mari Eneroth for her review of the article and for her helpful suggestions.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AF designed the study, prepared the data-set, and performed the statistical analysis, GÅ and AN drafted the manuscript, MSG helped to draft the manuscript, KSG and LTL participated in the design and coordination of the study. All the authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Fridner, A., Norell, A., Åkesson, G. et al. Possible reasons why female physicians publish fewer scientific articles than male physicians – a cross-sectional study. BMC Med Educ 15, 67 (2015). https://doi.org/10.1186/s12909-015-0347-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-015-0347-9