
Abstract
Background
Pregnancy; It is an important process that directly affects the mother and the fetus, where women benefit more from health services and the need for health-related decision-making and information increases. It is very important to determine and improve the health literacy level of these women. The study determined the relationship between vaccine hesitancy and health literacy in pregnant women.
Methods
It is a cross-sectional type of research. The research was carried out in a state hospital. The online form was sent to 230 pregnant women. Ethics committee, institution and scale permissions were obtained for the study. The data of the study were collected online by using the questionnaire prepared by scanning the literature, the Anti-Vaccination Scale and the Health Literacy Scale. Statistical analyzes of the data were performed using the SPSS version 25 program.
Results
The Vaccine Hesitancy Scale score of the pregnant women was 55.53 ± 10.15, whereas their Health Literacy Scale score was 98.57 ± 21.48. Health literacy was associated with the sociodemographic and obstetric characteristics of the pregnant women. Educational status, economic status, place of residence, and family structure were associated with vaccine hesitancy.
Conclusions
It was determined that there was a negative correlation between the anti-vaccination scale scores of the pregnant women and the health literacy scale scores. As a result, it was determined that the anti-vaccination level of the pregnant women was moderate and the health literacy level was sufficient. It can be recommended to provide appropriate trainings and counseling to target groups, which will increase the health literacy level of pregnant women.
Similar content being viewed by others

Introduction
Health literacy is the capacity that determines people’s ability to access, comprehend and use accurate information that supports their appropriate health status and is sustainable throughout their lives [1]. Pregnancy is an important process directly affecting the mother and fetus, and during this process, women benefit more from health services, and their need for health-related decision making and information increases. This is an important opportunity to determine and improve the health literacy level of women [2].
Considering various studies in the world, in a cross-sectional study conducted in Germany (2017), it was determined that 54.3% of individuals had limited health literacy [3]. It was reported that 29% of people in the Netherlands had low health literacy, with the lowest health literacy rates being Bulgaria (37%) and Spain (42%) [4]. In a study conducted in China, it was determined that 81% of individuals had a low level of health literacy [5].
It has been found that 69.4% of individuals in Turkey have insufficient and problematic health literacy levels [6]. In the other study, it was determined that 55.4% of them had insufficient health literacy level, 22.2% of them had adequate and excellent level of health literacy [7].
Vaccination is the simplest, safest and most effective way to prevent infectious diseases. They build up resistance against certain infections by using the body’s natural defenses. Vaccines save about 2–3 million lives each year [8]. Although vaccine hesitancy has accelerated in the world since 1990, the concept of vaccine hesitancy came to the fore with the vaccination studies of Edward Jenner in England in 1796. Vaccination began to be widespread in the 1800s [9]. According to WHO, “vaccine hesitation” means delaying in accepting the administration of some vaccines or not allowing the administration of some vaccines even though vaccine availability is possible. “vaccine opposition” is the situation in which individuals do not voluntarily receive all vaccines [10].
Although great advances were made in vaccination in the past century, vaccine-preventable diseases are re-emerging due to vaccine hesitancy and remain a major threat to society [11]. Poor health literacy has been associated with less adoption of protective behaviors such as immunizations [12]. It is thought that individuals with a high level of health literacy will be able to get information about vaccination from the right sources and have an important place in the fight against vaccine opposition, which has become a major threat to the society [13].
Women’s health behaviors are decisive in raising and improving the health standards of the society. Pregnancy is a critical period when women use basic health services more frequently and become more open to learning [14]. Maternal health literacy level affects the ability of pregnant women to make the best decisions for themselves and their babies [15]. It was determined that health literacy training given to pregnant women increased their compliance with pregnancy, general self-efficacy and health literacy level [16].
It is important to determine the anti-vaccination opposition in pregnant women and the concept of health literacy, which increases its importance day by day. Community health nurses, midwives and social workers are key in this regard. Studies examining the relationship between anti-vaccination and health literacy in pregnant women are limited. Its aim is to examine the relationship between anti-vaccination and health literacy in pregnant women.
Methods
Participants and procedures
The population of this cross-sectional study consisted of pregnant women who applied to a city hospital in western Turkey. In the study, the calculation (d-value) method developed by Cohen was used to calculate the effect size in order to examine the relationship between vaccine hesitancy and health literacy in pregnant women. In the light of academic studies, whose d value, which is the effect size index, was reported, the “G.Power-3.1.9.2” program was used in the sample calculation (d = 0.25, 1-α=%95, 1-β=%95), and the number of participants was calculated as 197 pregnant women [13, 17]. The sample consisted of 230 pregnant women who agreed to participate in the study. The data were collected by applying an online form to 230 pregnant women who agreed to participate in the study. The online form was collected by delivering it to the pregnant women through the pregnancy school group. The pregnant women who did not have a Turkish comprehension problem were included in the sampling inclusion criteria. The study will take place between April 2021 and February 2022. The vaccine names included in the study are flu vaccine, tetanus-diphtheria-pertussis vaccine during pregnancy, hepatitis B vaccine during pregnancy and rabies vaccine. The study was conducted in a hospital due to easier access to pregnant women.
Measures
The data were collected by the researchers using a questionnaire, the “Vaccine Hesitancy Scale”; and the “Health Literacy Scale” were used.
Data collection form
The survey, which consists of 2 parts, includes 25 questions in total. In the first part, there are 18 questions including “socio-demographic characteristics” (age, gender, educational status, family type, number of pregnancies, etc.), while in the second part, there are 7 questions in which the data about “vaccine and health literacy” (vaccination status, where they got information such as getting vaccinated with a doctor’s recommendation, etc.) were collected. The questions were formed in line with the literature [13, 18, 19]. In the questionnaire, participants’ gestational week, 1st, 2nd week. and 3rd trimester.
Vaccine hesitancy scale
The Vaccine Hesitancy Scale (VHS) was developed by Kılınçarslan et al. [20] to measure the level of vaccine hesitation. This scale is a 5-point Likert scale. The total score can vary between 21 and 105. A higher score on the scale means that participants have higher hesitations about vaccination [20]. (Appendix-1). The Cronbach Alpha (a) internal consistency value of this study was determined as 0.87.
Health literacy scale
It was developed as 47 items by Sørensen et al. [21] to measure the health literacy levels of individuals, and simplified as 25 items by Toçi et al. [22]. The Turkish validity and reliability analyzes of the Health Literacy Scale (HLS) were performed by Aras and Temel-Bayık [23]. The scale, which consists of 25 items and four subscales, is answered in a 5-point likert structure. All items of the scale have a positive structure, and there is no reverse item. The higher the score, the higher the level of health literacy [23]. (Appendix-2). The Cronbach Alpha (a) coefficient of this study was found to be 0.97.
Statistical analysis
Analyzes were calculated with SPSS version 25 program. Kolmogorov-Smirnov test was used to test the normality of scores obtained from a continuous variable. In addition to descriptive statistical methods while evaluating the study data, Independent Sample t-Test and One-Way ANOVA (Variance) Analysis were used to test the quantitative difference between groups. Qualitative variables in the research are frequency (n, %); continuous variables were presented as mean and standard deviation. Multiple comparisons were calculated with Scheffe test in groups where the difference in the ANOVA test results was significant. The level of relationship between two continuous variables was evaluated with the Pearson correlation test. The results were calculated at the 95% confidence interval, and the significance was calculated at the p < 0.05 level.
Results
230 pregnant women were included in the study. The mean age of the pregnant women was 28.20 ± 6.08; 63.5% were under the age of 30; and 97% were married. According to their education level, 24.8% of the pregnant women were primary school graduates, 33.9% were secondary school graduates, and 41.3% were higher education graduates. According to their economic status, it was determined that 35.2% of the pregnant women’s income did not cover their expenses, that 47.4% of the pregnant women’s income was equal to their expenses, and that 17.4% of the pregnant women’s income was more than their expenses. 23.5% of the pregnant women were actively working in a job,; 93% were living in a district or province; 83.5% had a social security; 84.8% had a nuclear family structure; and 7% had a diagnosed chronic disease. It was determined from the available data that 7% of them used a drug regularly, that 25.2% used cigarettes, and that 7.4% used alcohol. (Table 1).
When the total and sub-dimension scores of the pregnant women on the HLS were examined, it was determined that the total score was 98.57 ± 21.48. When the total score of the pregnant women on the VHS was examined, it was determined that the total score was 55.53 ± 10.15.
It was determined that the HLS scores differed statistically significantly according to marital status, education level, place of residence, and economic status. It was determined that the level of health literacy increased in the married participants, those with a high education level, those living in cities, and those with a high economic status (p < 0.05). It was determined that the health literacy levels of the pregnant women, who had 3 or more pregnancies and had 3 or more births, were higher. (p = 0.003; p = 0.001).
It was determined that the VHS scores of the pregnant women differed statistically significantly according to education level, place of residence, economic level, and family structure, and that the anti-vaccination rate of the pregnant women living in the city was lower (p < 0.05).
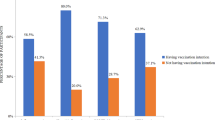
It was determined that 77% of the pregnant women had their vaccinations completely according to the pregnancy calendar, that 20.9% had the flu vaccine in the last 1 year, and that 56.1% received information about vaccines from health staff. 58.7% stated that the information they obtained about vaccines was positive, while 44.8% stated that the information obtained from the written and visual media about vaccines never changed their opinion about the vaccine. 73% of the pregnant women stated that they could get the tetanus vaccine upon the recommendation of a doctor, whereas 65.2% stated that they could get the hepatitis-B vaccine. It was determined from the available data that 10% of the pregnant women thought that it was inconvenient to have the rabies vaccination in case of suspected animal bites during pregnancy. (Table 2).
It was determined that the mean VHS scores of the pregnant women who were regularly vaccinated according to the immunization schedule were statistically significantly lower (t = 5.334; p < 0.001).
It was determined that the VHS scores of the pregnant women differed statistically significantly according to the source of information about vaccines (F = 9,661; p < 0.001). In the subgroup analyzes, it was found out that this difference was caused by the pregnant women whose vaccine information source was scientific publications on vaccines. From this finding, it was determined that the anti-vaccination resistance of the pregnant women who had information about the vaccine from scientific publications was lower.
It was found that the mean VHS score of the pregnant women, who thought that the information they obtained about vaccines was positive, was statistically significantly lower (t = 4.919; p < 0.001). It was found that the mean HLS scores of the pregnant women, who changed their minds about vaccines as a result of the information they obtained from television, radio or the internet, were found to be statistically significantly higher (t = 4.834; p < 0.001). It was found that the mean VHS score of the pregnant women, who stated that they could get the tetanus-diphtheria-pertussis vaccine during pregnancy upon the recommendation of a doctor, was statistically significantly lower (t = 4.847; p < 0.001). It was determined that the mean HLS scores of the pregnant women, who stated that they could get the hepatitis-B vaccine during pregnancy upon the recommendation of a doctor, were statistically significantly lower (t = 3.570; p < 0.001). (Table 3)
A statistically significant and negative correlation was found between the VHS scores of the pregnant women and their HLS total and sub-dimension scores (p < 0.001). From this finding, it was determined that as the health literacy level of the pregnant women decreased, the anti-vaccination attitude increased.
A statistically significant and positive correlation was found between the HLS total score and the HLS sub-dimension scores (p < 0.001). From this finding, it was determined that as the HLS sub-dimension scores increased, the total scale score also increased (Table 4).
Discussion
It was determined that the general vaccine hesitancy score averages of the individuals participating in our study were 55.53 ± 10.15. Pregnant women are a high-risk group for the effects of Covid-19 infection [24, 25]. In a study investigating the factors affecting Covid-19 vaccination in pregnant women, it was reported that only 51.5% of pregnant women accepted to be vaccinated, and that the determined rate was lower than the general population vaccination rate [25].
In the study, it was determined that one of the factors affecting vaccine hesitancy was the level of education. It was determined that the anti-vaccination rate was higher in the primary school graduates. In the study conducted by Çınar et al. [26] the tetanus immunization status of pregnant women, their frequency, their approach to the tetanus vaccine and the factors affecting it were determined, and it was reported that high school or higher education increased vaccination. Polat et al. [25] showed that as the level of education increased, the rate of vaccination also increased. In the study conducted by Afolabi et al. [27], it was concluded that pregnant women with a lower education level were more likely to hesitate in taking the hepatitis B vaccine. It is thought that as the education level of pregnant women increases, access to the right information from the right source increases. The study supports the literature.
In the study, it was determined that the vaccine opposition of the pregnant women who thought that their knowledge about vaccines was positive was lower. In the study of Dağdeviren et al. [28] when the reasons for vaccine opposition in pregnant women were questioned, 46% reported that they did not know that they should be vaccinated, 12.5% thought that the vaccine was not protective, and 2.3% reported that they had concerns about the content of the vaccine. In a study, it was reported that fear was the leading reason for pregnant women not to have the tetanus vaccine [26]. In the study conducted on pregnant women, it was reported that the information conveyed about the safety and importance of vaccination increased the intake of tetanus, diphtheria and pertussis (Tdap) vaccines in pregnant women [29]. In a study conducted in China, it was determined that individuals who received negative information about the Covid-19 vaccine and had doubts about the source of information were more likely to experience vaccine hesitancy [30]. According to a study conducted in Kelantan, participants had concerns such as doubts about the safety of the Covid- 19 vaccine (51.6%), doubts about its effectiveness (50.7%) and fear of adverse effects (61.1%) [31]. The fact that pregnant women have sufficient and positive knowledge about vaccines affects the level of anti-vaccination.
In a study, it was concluded that the second most common reason for individuals to experience vaccine hesitancy was the information they heard from the media and the internet. 25% of individuals participating in that study stated that they heard that the vaccine was harmful from the media and the internet [32]. In a study, it was seen that individuals who used medical websites as a source of information had a more positive attitude towards vaccines than individuals who used social media [33]. In this study, it was found that the pregnant women who changed their minds about vaccines as a result of the information they received from television, radio or the internet had higher anti-vaccination. The available literature supports the findings of this study. Non-scientific data disseminated through the media and social media play an important role in vaccine rejection and opposition.
In another study, it was determined that individuals who received information about vaccines from healthcare professionals were more likely to consider having their children vaccinated [34]. It was concluded that the main reason for women to receive seasonal influenza and pertussis vaccines during pregnancy in Ireland was the recommendation of a doctor [35]. In another study conducted in Italy, the main barriers to vaccination for influenza and pertussis vaccines were determined as not receiving vaccination advice from any healthcare provider (81%) and safety concerns (18%) [36]. Considering the results of the studies, it is thought that vaccination can be increased with the advice of a health professional or doctor.
In society, especially in pandemics, governments should cooperate on increasing vaccination programs [37]. Health education and consultancy services are important to increase immunization knowledge [38]. A study conducted in adults reported that HLS had a positive effect on immunization [39]. In another study, it was found that pregnant women with high HLS levels had lower teratogenic risk perceptions regarding the flu vaccine [2]. The findings of our study support the literature, but it seems that more study results are needed.
In the study in which the immunization knowledge proficiency levels, attitudes and behaviors, and health literacy levels of adults were evaluated, it was determined that there was a positive relationship between the level of health literacy and the level of immunization knowledge and attitudes towards immunization services [13]. In a study conducted in Spain, it was concluded that women with high health literacy levels were more likely to refuse immunization [40]. In another study, it was concluded that as the health literacy level increased, the vaccine hesitancy decreased [41]. Another study states that increasing education against vaccine refusal and incorporating motivational interviewing skills are the first steps towards increasing mothers’ vaccine acceptance [42]. In another study, there was a relationship between internet decision-making and COVID-19 vaccine hesitancy in pregnant women. Health professionals, information specialists and librarians emphasize that they should direct people to reliable sources about vaccines [43]. In this study, a statistically significant and negative correlation was found between the VHS scores of the pregnant women and their HLS total and sub-dimension scores. The results of this study support the literature, but it is known as the first study to examine vaccine hesitancy and health literacy in pregnant women. It seems that more academic studies are needed.
No difference was found between pregnant women’s opposition to vaccination according to pregnancy characteristics (gestational week, number of pregnancies, number of live births and miscarriage). In a study, it was reported that the vaccination rates of nulliparous pregnant women were higher [44]. In another study, it was determined that multiparous people had higher rates of not accepting the vaccine [25]. In a study investigating flu vaccine uptake among pregnant women in Singapore, no difference in vaccine uptake was found according to trimester [45].
Conclusion
The Vaccine Hesitancy Scale score of the pregnant women was 55.53 ± 10.15, while their Health Literacy Scale score was 98.57 ± 21.48. It was determined that the health literacy level of the pregnant women was sufficient and that the level of vaccine hesitancy was moderate.
It was determined that the HLS total and sub-dimension scores differed statistically significantly according to marital status, education level, place of residence, economic status, and number of pregnancies (p < 0.05). It was determined that the level of health literacy increased among those with a high level of education, those living in cities, and those with a high economic status. It was determined that the health literacy levels of the pregnant women who had 3 or more pregnancies and had 3 or more births were lower.
It was determined that the VHS scores of the pregnant women showed statistically significant differences according to education level, place of residence, economic level, and family structure. It was found that the mean VHS scores of the pregnant women who graduated from primary school, those with low economic status, and those with extended family structure were statistically significantly higher. It was determined that the anti-vaccination rate of the pregnant women living in cities was lower, and that there was a negative correlation between the Vaccine Hesitancy Scale scores of the pregnant women and their health literacy scale scores.
In light of the findings, this study is the first known research in the literature examining health literacy and vaccine hesitancy in pregnant women. It was determined that there was a negative relationship between pregnant women’s anti-vaccine scale scores and health literacy scale scores. As a result, it was determined that the pregnant women’s opposition to vaccination was at a moderate level and their health literacy level was sufficient. Training programs about the importance of immunization given to pregnant women by community health nurses will raise awareness in pregnant women. Community health nurses should provide appropriate training and consultancy to the target group, which will increase the health literacy level of pregnant women. Successful educational interventions on vaccine hesitancy and health literacy contribute to pregnant women on how and from which sources they can access accurate information. Community health nurses, midwives and social workers should fight against vaccination in cooperation. Interventional studies on vaccine hesitancy and health literacy in pregnant women are recommended.
Limitations
This study is the first known research in the literature examining health literacy and vaccine hesitancy in pregnant women. However, the study has some limitations. The first of these is the collection of the data based on the self-reports of the pregnant women. In addition, since the results of the research are related to the sample in which the research was conducted, they cannot be generalized.
Data availability
The data that support the findings of this study are available from Seda Cangöl Sögüt but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are how ever available from the authors upon reasonable request and with permission of Seda Cangöl Sögüt.
References
World Health Organization. Improving health literacy. 2022. https://www.who.int/activities/improving-health-literacy. [Date of access 9.11.2022].
Sahin E, Yesilcinar I, Geris R, Pasalak SI, Seven M. The impact of pregnant women’s health literacy on their health-promoting lifestyle and teratogenic risk perception. Health Care Women Int. 2021;42(4–6):598–610. https://doi.org/10.1080/07399332.2020.1797036
Schaeffer D, Berens EM, Vogt D. Health literacy in the German population. Dtsch Arztebl Int. 2017;114(4):53–60. https://doi.org/10.3238/arztebl.2017.0053
Sørensen K, Pelikan JM, Röthlin F, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. 2015;25(6):1053–8. https://doi.org/10.1093/eurpub/ckv043
Yang Q, Yu S, Wang C, et al. Health literacy and its socio-demographic risk factors in Hebei: a cross-sectional survey. Med (Baltim). 2021;100(21):e25975. https://doi.org/10.1097/MD.0000000000025975
Abacıgil F, Beşer E, Baran Deniz E, Erata M, Harlak H, Karakaya K, Evci Kiraz ED. Turkish health literacy scales reliability and validity study, Pınar Okyay, Filiz Abacıgil (Ed) Repub Turk Ministry Health 2016. https://ekutuphane.saglik.gov.tr/Yayin/530
Bakan AB, Yıldız M. A study on determining the health literacy levels of individuals aged 21–64. Health Soc. 2019;29(3):33–40.
World Health Organization. Immunization coverage. 2022. Retrieved: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage [Date of access 9.11.2022].
Jacobson RM, St Sauver JL, Finney Rutten LJ. Vaccine Hesitancy. Mayo Clin Proc. 2015;90(11):1562–1568. https://doi.org/10.1016/j.mayocp.2015.09.006
MacDonald NE, SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4. https://doi.org/10.1016/j.vaccine.2015.04.036
Puri N, Coomes EA, Haghbayan H, Gunaratne K. Social media and vaccine hesitancy: new updates for the era of COVID-19 and globalized infectious diseases. Hum Vaccin Immunother. 2020;16(11):2586–93. https://doi.org/10.1080/21645515.2020.1780846
Castro-Sánchez E, Vila-Candel R, Soriano-Vidal FJ, Navarro-Illana E, Díez-Domingo J. Influence of health literacy on acceptance of influenza and pertussis vaccinations: a cross-sectional study among Spanish pregnant women. BMJ Open. 2018;8(7):e022132. https://doi.org/10.1136/bmjopen-2018-022132
Çam C, Unsal A, Arslantas D, Kilinc A, Ozturk Emiral G. Evaluation of ımmunization knowledge sufficiency levels, attitudes and behaviors and health literacy levels of adults. Osmangazi J Med. 2021;43(1):7–19. https://doi.org/10.20515/otd.696984
Gokoglu AG. The effect of women’s health literacy level on health behaviors and child health. Baskent Univ Fac Health Sci J. 2021;6(2):132–48. http://busbid.baskent.edu.tr/index.php/busbid/article/view/296/173
Yee LM, Silver R, Haas DM, Parry S, Mercer BM, Wing DA, Grobman WA. Association of Health Literacy among Nulliparous Individuals and maternal and neonatal outcomes. JAMA Netw Open. 2021;4(9):e2122576. https://doi.org/10.1001/jamanetworkopen.2021.22576
Aslantekin Özçoban F, Ergün S, Erkal Aksoy Y. Effects of health literacy education on adaptation to pregnancy, self-efficacy, fear of childbirth and health literacy in Turkish pregnant women: a randomized, controlled trial. Health Soc Care Community. 2022;30(2):e537–49. https://doi.org/10.1111/hsc.13690
Guclu OA, Demirci H, Ocakoglu G, Guclu Y, Uzaslan E, Karadag M. Relationship of pneumococcal and influenza vaccination frequency with health literacy in the rural population in Turkey. Vaccine. 2019;37(44):6617–23. https://doi.org/10.1016/j.vaccine.2019.09.049
Akca E, Gokyildiz Surucu S, Akbas M. Health perception, health literacy and related factors in pregnant women. J Inonu Univ Health Serv Vocat School. 2020;8(3):630–42. https://doi.org/10.33715/inonusaglik.735467
Turkay M, Ay EG, Aktekin MR. Anti-vaccine status in a selected groups in Antalya. Mediterranean J Med. 2017;(3)2:107–12. https://dergipark.org.tr/en/download/article-file/2156991
Kilincarslan MG, Sarıgul B, Toraman C, Sahin EM. Development of the valid and reliable scale of vaccine hesitancy Turkish language. Konuralp Med J. 2020;12(3):420–9. https://doi.org/10.18521/ktd.693711
Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, Brand H. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80. https://doi.org/10.1186/1471-2458-12-80
Toçi E, Burazeri G, Sorensen K, Jerliu N, Ramadani N, Roshi E, Brand H. Health literacy and socioeconomic characteristics among older people in transitional Kosovo. Br J Med Med Res. 2013;3(4):1646–58.
Biyik Temel A, Aras Z. Evaluation of validity and reliability of the Turkish version of health literacy scale. Florence Nightingale J Nurs. 2017;25(2):85–94. https://doi.org/10.17672/fnhd.94626
Mitchell SL, Schulkin J, Power ML. Vaccine hesitancy in pregnant women: a narrative review. Vaccine. 2023;41(29):42204227. https://doi.org/10.1016/j.vaccine.2023.05.047
Polat G, Saglam ZA, Polat I, Yucel B. Patient factors affecting covıd-19 vaccination in pregnancy: a survey study. Med J Istanbul Kanuni Sultan Suleyman. 2022;14(2):170–5. https://doi.org/10.14744/iksstd.2022.31644
Cınar G, Akdemir-Kalkan I, Yilmaz-Karadag F, Hocaoglu M, Deniz S, Isık ME, Kaplan-Atalay E. Evaluation of the knowledge, attitudes and behaviors of pregnant women on tetanus vaccination. Klimik J. 2022;35(2). https://doi.org/10.36519/kd.2022.4229
Afolabi IB, Aremu AB, Maidoki LA, Atulomah NO. Predictors of Hepatitis B virus infection vaccine hesitancy among pregnant women attending Antenatal Care at Lubaga Hospital, Kampala, Uganda. Int J Womens Health. 2022;14:1093–104. https://doi.org/10.2147/IJWH.S378000
Dağdeviren G, Örgül G, Yücel A, Şahin D. Tetanus vaccine during pregnancy: data of a tertiary hospital in Turkey. Turk J Med Sci. 2020;50(8):1903–8. https://doi.org/10.3906/sag-2001-77
Dempsey AF, Brewer SE, Sevick C, Pyrzanowski J, Mazzoni S, O’Leary ST. Tdap vaccine attitudes and utilization among pregnant women from a high-risk population. Hum Vaccin Immunother. 2016;12(4):872–8. https://doi.org/10.1080/21645515.2015.1094594
Huang Y, Su X, Xiao W, Wang H, Si M, Wang W, Qiao Y. COVID-19 vaccine hesitancy among different population groups in China: a national multicenter online survey. BMC Infect Dis. 2022;22(1):153. https://doi.org/10.1186/s12879-022-07111-0
Sham F, Shahed ANM, Baharudin NS, Majid N, Yajid S. Covid-19 Vaccination Acceptance and its Associated factors among community in Kelantan. Malaysian J Nurs (MJN). 2023;15(Supplimentary 1):125–38. https://doi.org/10.31674/mjn.2023.v15isupp1.013
Özceylan G, Toprak D, Esen ES. Vaccine rejection and hesitation in Turkey. Hum Vaccin Immunother. 2020;16(5):1034–9. https://doi.org/10.1080/21645515.2020.1717182
Mansur F, Biyik E. Effect of digital media used as social marketing tool, on ındividual attitudes toward Covid-19 vaccine. Anadolu Univ J Social Sci. 2022;22(1):257–78. https://doi.org/10.18037/ausbd.1095162
Çıklar S, Güner PD, Knowledge. Behavior and attitude of mother’s about childhood immunization and reasons and reeasons of vaccination rejection and hesitancy: a study of mixed methodology. Ankara Med J. 2020;20(1):180–95. https://doi.org/10.5505/amj.2020.80148
Quattrocchi A, Mereckiene J, Fitzgerald M, Cotter S. Determinants of influenza and pertussis vaccine uptake in pregnant women in Ireland: a cross-sectional survey in 2017/18 influenza season. Vaccine. 2019;37(43):6390–6. https://doi.org/10.1016/j.vaccine.2019.09.008
Vilca LM, Cesari E, Tura AM, Di Stefano A, Vidiri A, Cavaliere AF, Cetin I. Barriers and facilitators regarding influenza and pertussis maternal vaccination uptake: a multi-center survey of pregnant women in Italy. Eur J Obstet Gynecol Reprod Biol. 2020;247:10–5. https://doi.org/10.1016/j.ejogrb.2020.02.007
Theresia SIM, Reñosa MDC, Accelerating. COVID-19 vaccination amid natural disasters in Indonesia. Malaysian J Nurs (MJN). 2023;14(3):201–8. https://doi.org/10.31674/mjn.2023.v14i03.024
Moschese V, De Angelis L, Capogna MV, Graziani S, Baglivo F, Pietropolli A, Rizzo C. Vaccine hesitancy and knowledge regarding maternal immunization among reproductive age women in central Italy: a cross sectional study. Front Global Women’s Health, 4. https://doi.org/10.3389/fgwh.2023.1237064
Castro-Sánchez E, Chang PWS, Vila-Candel R, Escobedo AA, Holmes AH. Health literacy and infectious diseases: why does it matter? Int J Infect Dis. 2016;43:103–10. https://doi.org/10.1016/j.ijid.2015.12.019
Castro-Sánchez E, Vila-Candel R, Soriano-Vidal FJ, Navarro-Illana E, Díez-Domingo J. Influence of Health Literacy on Acceptance of Influenza and Pertussis vaccinations: a cross-sectional study among Spanish pregnant women. BMJ Open. 2018;8(7):e022132.
Ertas H, Gode A. Investigation of relationship between health literacy with anti-vaccine: a study on college students. J Acad Value Stud. 2021;1:1–14. https://doi.org/10.29228/javs.49907
Moriarty KL, Oyenuga RO, Olafuyi O, Schwartz DA. Causes and effects of COVID-19 vaccine hesitancy among pregnant women and its Association with adverse maternal, placental, and perinatal outcomes. Yale J Biol Med. 2024;97(1):73–84. https://doi.org/10.59249/LPOQ5146
Uludağ E, Serçekuş P, Yıldırım Gökşen DF, Alataş SE, Özkan S. Is decision-making based on the internet during pregnancy a predictive factor for vaccine hesitancy in pregnant women during the pandemic? Women Health. 2024;64(1):5–13. https://doi.org/10.1080/03630242.2023.2277879
Bartolo S, Deliege E, Mancel O, Dufour P, Vanderstichele S, Roumilhac M, Faure K. Determinants of influenza vaccination uptake in pregnancy: a large single-centre cohort study. BMC Pregnancy Childbirth. 2019;19(1):1–9. https://doi.org/10.1186/s12884-019-2628-5
Offeddu V, Tam CC, Yong TT, Tan LK, Thoon KC, Lee N, Yung CF. Coverage and determinants of Influenza vaccine among pregnant women: a cross-sectional study. BMC Public Health. 2019;19(1):1–12. https://doi.org/10.1186/s12889-019-7172-8
Acknowledgements
The authors are grateful to all participants who agreed to participate voluntarily in this study.
Funding
This study received no funding.
Author information
Authors and Affiliations
Contributions
KÇ, SCS—conception, design, drafting the article. KÇ, SCS—data collection. KÇ, SCS—conception, design, data analysis and interpretation, drafting the article. KÇ, SCS—conception, design, interpretation of data, critical revision of the draft. KÇ, SCS—design, data analysis and interpretation, drafting the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Approval was obtained from the Institute Clinical Research Ethics Committee of the School of Graduate Studies of Çanakkale Onsekiz Mart University, Turkey (Number: E-95564340-050.02.04-2100034245, Decision No: 15/112, Decision Date: 19.02.2021). Institutional permission (Number: E-12641312-044) was obtained from the institution where the research was conducted. Necessary permissions were obtained from the authors of the scales to be used in the study. Informed consent was obtained from the pregnant women at the beginning of the google form in electronic form before participating in the study. The participants were not paid in return for their participation, but they were allowed to get the executive summary about the results if they wanted. The study was conducted in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
* This article is a master’s thesis completed at the Graduate Education Institute of Çanakkale Onsekiz Mart University, Turkey.
* The study was presented as a presentation in the Third International/Fourth National Congress of Public Health Nursing.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Çetin, K., Sögüt, S.C. The relationship between vaccine hesitancy and health literacy in pregnant women: a cross-sectional study *. BMC Women's Health 24, 361 (2024). https://doi.org/10.1186/s12905-024-03148-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-024-03148-2