
Abstract
Background:
Poor health literacy is associated with lower utilization of preventable services. However, the relationship between health literacy and COVID-19 vaccine hesitancy remains controvertible.
Methods:
This study used data from 229,242 individuals who completed the Community Health Survey in Korea from August 16 to October 31 in 2021. To operationalize COVID-19 vaccine hesitancy, we measured vaccine refusal, which is defined as not having been vaccinated and not intending to get vaccinated against COVID-19. Health literacy is operationalized in two dimensions; the ability to understand spoken directions from health professionals and the ability to understand written information regarding health. Covariates include sex, age, educational level, marital status, employment status, basic living security pension status, and subjective health status. Two multivariable logistic regression models were run to determine factors associated with COVID-19 vaccine refusal. Model 1 included sociodemographic characteristics and subjective health status. Model 2 added two health literacy variables. Odds ratio (OR) and 95% confidence intervals (CI) were calculated.
Results:
Only 3.9% of the Korean adult population were estimated to refuse COVID-19 vaccine. The most commonly cited reasons for COVID-19 vaccine refusal were concerns about vaccine adverse events (47.6%), followed by the assessment of one’s own health status (29.5%). Individuals who found spoken directions very difficult to understand were more likely to refuse COVID-19 vaccine than those who found spoken directions very easy (OR = 1.55, 95% CI: 1.28–1.87, p < 0.001). People who did not pay attention to written information were more likely to refuse COVID-19 vaccine than those who reported it to be very easy to understand (OR = 1.28, 95% CI: 1.13–1.45, p < 0.001). People in all other categories of the literacy spectrum for either spoken or written information did not have an increased risk of COVID-19 vaccine refusal.
Conclusion:
Health literacy was significantly associated with COVID-19 vaccine refusal. Health literacy programs could be beneficial to reduce vaccine refusal, particularly for the people who find spoken directions from health professionals very difficult to understand and those who do not pay attention to written information.
Similar content being viewed by others


Introduction
According to a survey of a representative sample from 19 countries in June 2020, the proportion of respondents that expressed unwillingness to accept a COVID-19 vaccine ranged from 11.4 to 45.2%, raising concerns among public health experts [1]. Even before the COVID-19 pandemic hit the globe, the World Health Organization (WHO) recognized vaccine hesitancy as one of ten global health threats [2]. Vaccine hesitancy refers to the behaviors of individuals who refuse or delay the acceptance of vaccines that are available for vaccination services [3]. Some regarded vaccine hesitancy as an “ambiguous notion” that encompasses a set of behavior, beliefs, and attitudes towards vaccination [4]. This view mirrors the existence of discrepancies among experts in how to define vaccine hesitancy [5]. More recently, vaccine hesitancy was defined as “a state of indecisiveness regarding a vaccination decision, independently of behavior” [6]. The WHO summarized the reasons for vaccine hesitancy in general as the lack of confidence in vaccines or providers, complacency of not recognizing the need for a vaccine, and inconvenient access to vaccines [7]. A key reason for COVID-19 vaccine hesitancy was concerns about safety, in part because the vaccines were developed and produced at an accelerated speed to quickly respond to the pandemic [7, 8].
Vaccination experts concur that vaccine hesitancy is influenced by individuals’ characteristics such as knowledge, information, and health literacy [9, 10]. Health literacy is defined as “the degree to which individuals can obtain, process, understand, and communicate about health-related information needed to make informed health decisions [11].” Poor health literacy is associated with worse health outcomes and lower use of health services for chronic conditions, such as diabetes and asthma [12, 13]. Inadequate health literacy was also linked to lower use of preventive services, such as influenza and pneumococcal vaccinations [14, 15]. Likewise, willingness to accept COVID-19 vaccine is lower among adults with low health literacy scores and individuals who are less capable of detecting fake news about the vaccine, according to an online survey conducted in France [16]. In contrast, another survey among Italian adults shows that how well one understands information on vaccine is not associated with intention to get vaccinated against COVID-19 [17].
Unlike traditional vaccines, COVID-19 vaccines were developed and approved for use at an unprecedented pace since rapid mass vaccination was considered to be a global security issue [8]. This created many challenges in communicating accurate vaccine information to the general public [18]. While health literacy can play a major role in vaccination intentions, earlier studies were based on online survey data [16, 17, 19]. Therefore, there remains a gap in our understanding of the association between COVID-19 vaccine hesitancy and health literacy. The gap appears to be especially wide in the Korean context. To the best of our knowledge, no general link has been explored between health literacy and COVID-19 vaccine hesitancy in the Korean population. Some researchers only focused their attention on the ability to seek, search, understand, and evaluate health information online, which is referred to as eHealth literacy, as a predictor of intention to vaccinate against COVID-19 [20]. An online survey conducted in South Korea indicates that lower vaccine hesitancy is associated with the use of on- and off-line media to obtain information on the perceived benefits of vaccination [21], which does not represent health literacy per se. Given the paucity of evidence in the Korean context, this study aims to estimate the prevalence of COVID-19 vaccine hesitancy in the Korean adult population aged 19 years and older and to investigate the association between COVID-19 vaccine hesitancy and health literacy using data collected from a sample representative of the population in 2021 when COVID-19 vaccines were widely available.
Methods
Data
This study used data from the Community Health Survey (CHS) in Korea that was conducted by the Korea Disease Control and Prevention Agency from August 16 to October 31, 2021. The annual survey that began in 2008 collects data using in-person interviews. In 2021, a total of 229,242 individuals completed the survey [22]. The CHS uses a complex survey design in which administrative areas were cluster sampled using residential type as a stratification variable. A sample of households within each area were selected using systematic sampling. All members aged 19 and older of selected households were interviewed. All participants in the 2021 CHS were used for analysis.
Measures
For the purpose of this analysis, we examined COVID-19 vaccine refusal, which is an element of the much more comprehensive notion of COVID-19 vaccine hesitancy [4]. COVID-19 vaccine refusal is defined as not having been vaccinated and not intending to get vaccinated against COVID-19. The 2021 CHS included a set of new questions regarding COVID-19 vaccines, allowing for the exploration of the important subject of vaccine hesitancy. Participants were asked to indicate whether they have received a COVID-19 vaccine at the time of the survey. Those who have not been vaccinated were then asked to rate if they intend to get vaccinated against COVID-19 on a four-item scale (strongly agree, agree, disagree, strongly disagree). The respondents who answered ‘disagree’ or ‘strongly disagree’ on the scale were categorized as the vaccine refusal group. The vaccine acceptance group comprised those who have already been vaccinated and those who answered ‘strongly agree’ or ‘agree.’
Health literacy is operationalized in two dimensions; the ability to understand spoken directions from health professionals and the ability to understand written information regarding health. In the 2021 CHS, respondents were asked, “how difficult is it for you to understand spoken directions from health professionals like doctors and nurses?” and “how difficult is it for you to understand health information written on the newspaper, the web, etc.?” To the question regarding spoken directions, the respondents were to select one of the following items: very easy, easy, difficult, and very difficult. To the question regarding written information, the item of “do not pay attention to written information on health” was also provided for selection.
Covariates
Vaccine hesitancy is shown to be influenced by a number of sociodemographic factors, such as age [23], gender [24,25,26], educational level [23, 25, 26], marital status [26], income [7, 19, 26, 27], and employment status [7, 24, 27]. Worsening subjective health status also was associated with an increased risk of COVID-19 vaccine hesitancy [27]. Based on the literature review, we included sex, age, educational level, marital status, employment status, basic living security pension status, and subjective health status as covariates in statistical models. Age was grouped into 19–29, 30–39, 40–49, 50–59, 60–69, and ≥ 70 years. Educational level was divided into up to primary education, middle school, high school, and college or higher levels. Marital status was categorized into currently married, ever-married, and never-married. The ever-married category included the divorced and the widowed. Employment status was categorized into salaried, self-employed, and economically inactive. To account for financial situation, respondents were classified into those who received a basic living security pension (i.e., cash assistance for the needy) and those who did not. Subjective health status was measured in five categories (very healthy, healthy, neutral, unhealthy, very unhealthy).
Statistical analysis
The characteristics of study subjects were described in terms of the number of respondents in the sample, according to sociodemographic, health status, and health literacy variables. By adjusting the frequency with sample weights that were used in the sampling design of the CHS, we calculated the estimated percentage of the population. The χ2 (chi-square) test was used to test if COVID-19 vaccine refusal differed among the categories of each variable. Two multivariable logistic regression models were run to determine the association between health literacy and COVID-19 vaccine refusal. Model 1 included sociodemographic characteristics and subjective health status. Model 2 added two health literacy variables. Multivariable-adjusted odds ratio (OR) and 95% confidence intervals (CI) were calculated. We computed R2 of Nagelkerke, as recommended to be used as a measure of effect size for logistic regression models in the literature [28].
All statistical analyses were performed by using SAS version 9.4 (Cary, NC, USA). The Institutional Review Board of Kongju University approved the study protocol and waived the requirement for informed consent (reference No. KNU_IRB_2022-094).
Results
Only 3.9% of the study population were estimated to refuse COVID-19 vaccine (Table 1). The rest were either already vaccinated or intending to get vaccinated in the future. Spoken directions from health professionals were very easy and somewhat easy for 22.7% and 57.3%, respectively, to understand. Written information was very or somewhat easy for 71.3% to understand, whereas 12.0% did not pay attention to it. The most commonly cited reasons for COVID-19 vaccine refusal were concerns about vaccine adverse events (47.6%), followed by the assessment of one’s own health status (29.5%) (Table 2).
The prevalence of COVID-19 vaccine refusal differed by all of the sociodemographic, health status, and health literacy variables examined in this study except for sex (p < 0.001, Table 3). COVID-19 vaccine refusal was reported in 7.2% of people for whom spoken directions were very difficult and 3.5% of people for whom spoken directions were very easy. 4.5% of people who reported written information to be very difficult to understand and 4.1% of those who did not pay attention to written information were vaccine-hesitant.
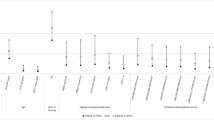
In model 1, people aged 40 years and older were less likely than those aged 19–29 years to refuse COVID-19 vaccine (Table 4, p < 0.001). The risk of COVID-19 vaccine refusal was smaller for the self-employed and the salaried than for economically inactive individuals (p < 0.001). Unhealthy and very unhealthy individuals were at greater risk of COVID-19 vaccine refusal than very healthy individuals (OR = 1.62, 95% CI: 1.42–1.83; OR = 3.35, 95% CI: 2.84–3.94, respectively, p < 0.001 in model 2). People who found spoken directions very difficult to understand were more likely to refuse COVID-19 vaccine than people who found spoken directions very easy (OR = 1.55, 95% CI: 1.28–1.87, p < 0.001 in model 2). People who did not pay attention to written information were more likely to refuse vaccine than people who reported it to be very easy to understand (OR = 1.28, 95% CI: 1.13–1.45, p < 0.001 in model 2). Model 2 shows an improved effect size compared to model 1, according to Nagelkerke’s R2.
Discussion
In a cross-national survey conducted in June 2020, 20.2% of participants in Korea expressed unwillingness to accept a COVID-19 vaccine if it is available [1]. The sentiment did not seem to improve with the passage of time; in another survey conducted between October to December of 2020, 39.8% of Korean adults were still hesitant or refused to be vaccinated [27]. Even in January 2021, COVID-19 vaccine hesitancy was reported to be considerably high according to online surveys in Korea [21] and China (53.3% and 35.5%, respectively) [29]. However, in the current analysis of data collected between August and October 2021, the prevalence of COVID-19 vaccine hesitancy is estimated to be low at 3.9% in the Korean adult population. This is on par with the prevalence of COVID-19 vaccine hesitancy (5.2%) among a convenience sample of US adults in February 2021 [30]. Such a swift change in vaccination intentions may have been due to the availability of COVID-19 vaccines, clinical trial data on safety and efficacy, and vaccination campaigns [19, 31]. Furthermore, a number of measures that the Korean government implemented may have played a role in increasing the vaccination coverage and intentions [32]. For example, mobile vaccination teams were in operation to remove physical barriers for the disabled. In addition, the government introduced various vaccination incentives, such as easing the requirements of social distancing and 2-weeks self-quarantine on return from travelling abroad for the fully vaccinated.
In the present study, COVID-19 vaccine-hesitant individuals cited concerns about vaccine safety as the most common reason for hesitancy, which was consistent with the previous findings [7, 27]. However, contrary to the earlier study [7], a lack of confidence in vaccine efficacy was rarely cited as the reason for hesitancy. This difference may have occurred in part because this present study used data collected in late 2021 when clinical trial data were available [31], and in another part because safety was a greater concern than a lack of efficacy as a reason for COVID-19 vaccine hesitancy [24].
An individual’s confidence in a vaccine is likely to be associated with ability to understand health information. The COVID-19 vaccine’s rapid pace of development may have led to a proliferation of misinformation, which could have posed a challenge to people with inadequate health literacy [26]. As it happens, concerns about COVID-19 vaccine safety were greater among people with lower health literacy, according to an email survey of US adults in January 2021 shortly after the emergency use authorizations of COVID-19 vaccines [19]. The risk of vaccine hesitancy is greater for people who found obtaining health information a frustrating task than for those who could easily navigate health information [30]. People who relied on social media for information and were susceptible to vaccine conspiracies appear to be hesitant to be vaccinated against COVID-19 [26].
This current study shows that poor health literacy is significantly associated with COVID-19 vaccine hesitancy. However, only the individuals who find spoken direction from health professionals very difficult to understand or those who do not pay attention to written health information have an increased risk of COVID-19 vaccine hesitancy compared to individuals who find health information, spoken and written, very easy to understand. People in all other categories of the literacy spectrum for either spoken or written information did not have an increased risk of vaccine hesitancy. These findings suggest that any incremental efforts to help people with poorest health literacy can improve vaccination intention for some vaccines. Likewise, efforts to increase the reach of written health information could have a material impact on mitigating vaccine hesitancy.
In addition to health literacy, sociodemographic variables, such as sex, age, and employment status, were significant predictors of COVID-19 vaccination hesitancy, which is consistent with the existing literature [23, 25, 27]. Health status was another significant predictor of COVID-19 vaccine hesitancy in the current study. People who rated themselves to be unhealthy were more likely to be COVID-19 vaccine-hesitant than those who perceived themselves to be very healthy. Moreover, assessment of one’s own health status was the second most commonly cited reason for vaccine hesitancy. However, evidence on the impact of health status on vaccine hesitancy is mixed in the literature. While US adults with five or more preexisting conditions were less COVID-19 vaccine-hesitant than people with none [26], German adults with chronic diseases were no less hesitant than those without one [25].
The association between health literacy and COVID-19 vaccine hesitancy shown in this study suggests a need for developing health literacy programs for the general public. A study in Germany showed that while communicating the benefits of COVID-19 vaccines was effective in significantly reducing vaccine hesitancy, its effect in areas with low health literacy was weaker [33]. This implies that increasing general health literacy through preemptive programs could improve the effect of any future urgent vaccination campaigns.
Aside from the general public, health professionals are also at risk of vaccine hesitancy [34]. Healthcare professionals were often the most trusted source of guidance regarding COVID-19 vaccines [35]. For that reason, health professionals’ own vaccine hesitancy could influence the general public’s vaccine hesitancy. There is evidence that some health professionals in the United States had COVID-19 vaccine hesitancy mainly due to safety concerns [36], and that health professionals’ own confidence in a particular vaccine influenced their recommendation to others [37]. Research reveals that a substantial proportion of primary care physicians in the Western hemisphere have inaccurate knowledge regarding vaccines [38]. Unsurprisingly, the literature points to the importance of educating health professionals as well as the general public using various communication tools, in order to reduce vaccine hesitancy [34].
To the best of our knowledge, this study is the first one to document the association between health literacy and COVID-19 vaccine hesitancy by using a large representative sample of the Korean population. This study indicates that only the individuals with lowest health literacy are at increased risk of vaccine hesitancy. These individuals find spoken directions from health professional very difficult to understand and they do not pay attention to written information. Any incremental efforts to help those individuals could reduce COVID-19 vaccine hesitancy. Despite the strengths, the findings should be interpreted with caution due to the following limitations. First, this study showed only association not causality due to the nature of a cross-sectional study design. Second, the measures of health literacy may not have fully captured the varied dimensions of a complex concept of health literacy, which has been measured by using a number of items [25]. Third, this study used self-reported data from the survey and therefore was subject to recall bias.
Conclusion
Health literacy is significantly associated with COVID-19 vaccine refusal. At most risk of COVID-19 vaccine refusal are people who have the most difficulty understanding directions from health professionals as well as those who do not pay attention to written health information. Any incremental efforts to help people understand spoken directions and pay attention to written health information will be beneficial to reduce COVID-19 vaccine hesitancy.
Availability of data and materials
The datasets generated and/or analysed during the current study are available in the Korea Disease Control and Prevention Agency repository (https://chs.kdca.go.kr/chs/rdr/rdrInfoDownMain.do).
References
Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2021;27:225–8. https://doi.org/10.1038/s41591-020-1124-9.
The World Health Organization. Ten threats to global health in 2019. [cited 26 Aug 2022]. Available: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019
MacDonald NE. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33:4161–4. https://doi.org/10.1016/j.vaccine.2015.04.036.
Peretti-Watel P, Larson HJ, Ward JK, Schulz WS, Verger P. Vaccine hesitancy: clarifying a theoretical framework for an ambiguous notion. PLoS Curr. 2015;7: ecurrents.outbreaks.6844c80ff9f5b273f34c91f71b7fc289. https://doi.org/10.1371/currents.outbreaks.6844c80ff9f5b273f34c91f71b7fc289.
Dubé È, Ward JK, Verger P, MacDonald NE. Vaccine hesitancy, acceptance, and anti-vaccination: Trends and future prospects for public health. Annu Rev Public Health. 2021;42:175–91. https://doi.org/10.1146/annurev-publhealth-090419-102240.
Larson HJ. Defining and measuring vaccine hesitancy. Nat Hum Behav. 2022;6:1609–10. https://doi.org/10.1038/s41562-022-01484-7.
Troiano G, Nardi A. Vaccine hesitancy in the era of COVID-19. Public Health. 2021;194:245–51. https://doi.org/10.1016/j.puhe.2021.02.025.
Kim JH, Hotez P, Batista C, Ergonul O, Figueroa JP, Gilbert S, et al. Operation Warp Speed: implications for global vaccine security. Lancet Glob Health. 2021;9:e1017–21. https://doi.org/10.1016/S2214-109X(21)00140-6.
Dubé E, Laberge C, Guay M, Bramadat P, Roy R, Bettinger JA. Vaccine hesitancy. Hum Vaccin Immunother. 2013;9:1763–73. https://doi.org/10.4161/hv.24657.
Biasio LR. Vaccine hesitancy and health literacy. Hum Vaccin Immunother. 2017;13:701–2. https://doi.org/10.1080/21645515.2016.1243633.
Berkman ND, Davis TC, McCormack L. Health literacy: what is it? J Health Commun. 2010;15:9–19. https://doi.org/10.1080/10810730.2010.499985.
Schillinger D, Grumbach K, Piette J, Wang F, Osmond D, Daher C, et al. Association of health literacy with diabetes outcomes. JAMA. 2002;288:475–82. https://doi.org/10.1001/jama.288.4.475.
Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97–107. https://doi.org/10.7326/0003-4819-155-2-201107190-00005.
Scott TL, Gazmararian JA, Williams MV, Baker DW. Health literacy and preventive health care use among Medicare enrollees in a managed care organization. Med Care. 2002;40:395–404.
Chen J-Z, Hsu H-C, Tung H-J, Pan L-Y. Effects of health literacy to self-efficacy and preventive care utilization among older adults. Geriatr Gerontol Int. 2013;13:70–6. https://doi.org/10.1111/j.1447-0594.2012.00862.x.
Montagni I, Ouazzani-Touhami K, Mebarki A, Texier N, Schück S, Tzourio C, et al. Acceptance of a Covid-19 vaccine is associated with ability to detect fake news and health literacy. Am J Public Health. 2021;43:695–702. https://doi.org/10.1093/pubmed/fdab028.
Biasio LR, Bonaccorsi G, Lorini C, Pecorelli S. Assessing COVID-19 vaccine literacy: a preliminary online survey. Hum Vaccin Immunother. 2021;17:1304–12. https://doi.org/10.1080/21645515.2020.1829315.
Ullah I, Khan KS, Tahir MJ, Ahmed A, Harapan H. Myths and conspiracy theories on vaccines and COVID-19: potential effect on global vaccine refusals. Vacunas. 2021;22:93–7. https://doi.org/10.1016/j.vacun.2021.01.001.
Kricorian K, Civen R, Equils O. COVID-19 vaccine hesitancy: misinformation and perceptions of vaccine safety. Hum Vaccin Immunother. 2022;18:1950504. https://doi.org/10.1080/21645515.2021.1950504.
Kim GY, Shin T, Son Y-J, Choi J. Psycho-behavioural factors influencing COVID-19 vaccine hesitancy among korean adults: the moderating role of age. J Adv Nurs. 2022;78:2904–15. https://doi.org/10.1111/jan.15273.
Lee M, You M. Direct and Indirect Associations of Media Use with COVID-19 vaccine hesitancy in South Korea: cross-sectional web-based survey. J Med Internet Res. 2022;24:e32329. https://doi.org/10.2196/32329.
Korea Disease Control and Prevention Agency. Community Health Survey 2021 User Guide. Osong, Korea. ; 2021. Available: http://chs.kdca.go.kr
Ogilvie GS, Gordon S, Smith LW, Albert A, Racey CS, Booth A, et al. Intention to receive a COVID-19 vaccine: results from a population-based survey in Canada. BMC Public Health. 2021;21:1017. https://doi.org/10.1186/s12889-021-11098-9.
Dror AA, Eisenbach N, Taiber S, Morozov NG, Mizrachi M, Zigron A, et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. 2020;35:775–9. https://doi.org/10.1007/s10654-020-00671-y.
Umakanthan S, Lawrence S. Predictors of COVID-19 vaccine hesitancy in Germany: a cross-sectional, population-based study. Postgrad Med J. 2022. https://doi.org/10.1136/postgradmedj-2021-141365. [cited 27 Aug 2022].
Ruiz JB, Bell RA. Predictors of intention to vaccinate against COVID-19: results of a nationwide survey. Vaccine. 2021;39:1080–6. https://doi.org/10.1016/j.vaccine.2021.01.010.
Hwang SE, Kim W-H, Heo J. Socio-demographic, psychological, and experiential predictors of COVID-19 vaccine hesitancy in South Korea, October-December 2020. Hum Vaccines Immunother. 2022;18:1–8. https://doi.org/10.1080/21645515.2021.1983389.
Gómez-Benito J, Hidalgo MD, Padilla J-L. Efficacy of Effect size measures in logistic regression. Methodol. 2009;5:18–25. https://doi.org/10.1027/1614-2241.5.1.18.
Wang C, Han B, Zhao T, Liu H, Liu B, Chen L, et al. Vaccination willingness, vaccine hesitancy, and estimated coverage at the first round of COVID-19 vaccination in China: a national cross-sectional study. Vaccine. 2021;39:2833–42. https://doi.org/10.1016/j.vaccine.2021.04.020.
Weerakoon SM, Henson-Garcia M, Valerio-Shewmaker MA, Messiah SE, Knell G. Contributions of trustworthiness, health literacy, and self-efficacy in communicating with COVID-19 vaccine–hesitant audiences: web-based survey study. JMIR Form Res. 2022;6:e38076. https://doi.org/10.2196/38076.
Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. NEJM. 2020;383:2603–15. https://doi.org/10.1056/NEJMoa2034577.
Kwon SL, Oh J. COVID-19 vaccination program in South Korea: a long journey toward a new normal. Health Policy Technol. 2022;11:100601. https://doi.org/10.1016/j.hlpt.2022.100601.
Steinert JI, Sternberg H, Prince H, Fasolo B, Galizzi MM, Büthe T, et al. COVID-19 vaccine hesitancy in eight european countries: prevalence, determinants, and heterogeneity. Sci Adv. 2022;8:eabm9825. https://doi.org/10.1126/sciadv.abm9825.
Jarrett C, Wilson R, O’Leary M, Eckersberger E, Larson HJ. Strategies for addressing vaccine hesitancy – A systematic review. Vaccine. 2015;33:4180–90. https://doi.org/10.1016/j.vaccine.2015.04.040.
Solís Arce JS, Warren SS, Meriggi NF, Scacco A, McMurry N, Voors M, et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat Med. 2021;27:1385–94. https://doi.org/10.1038/s41591-021-01454-y.
Gu M, Taylor B, Pollack HA, Schneider JA, Zaller N. A pilot study on COVID-19 vaccine hesitancy among healthcare workers in the US. PLoS ONE. 2022;17:e0269320. https://doi.org/10.1371/journal.pone.0269320.
Paterson P, Meurice F, Stanberry LR, Glismann S, Rosenthal SL, Larson HJ. Vaccine hesitancy and healthcare providers. Vaccine. 2016;34:6700–6. https://doi.org/10.1016/j.vaccine.2016.10.042.
Collange F, Verger P, Launay O, Pulcini C. Knowledge, attitudes, beliefs and behaviors of general practitioners/family physicians toward their own vaccination: a systematic review. Hum Vaccin Immunother. 2016;12:1282–92. https://doi.org/10.1080/21645515.2015.1138024.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Inmyung Song wrote the main manuscript text and Soo Hyun Lee reviewed the manuscript. IS and SL conceptualized the study. IS analyzed the data and drafted the manuscript. All authors revised the manuscript for important intellectual content, and all authors read and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was received from The Kongju National University Institutional Review Board (reference No. KNU_IRB_2022-094). The IRB waived the requirement for informed consent. All methods performed as a part of this study were in accordance with the Kongju National University Institutional Review Board guidelines.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open AccessThis article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Song, I., Lee, S.H. COVID-19 vaccine refusal associated with health literacy: findings from a population-based survey in Korea. BMC Public Health 23, 255 (2023). https://doi.org/10.1186/s12889-023-15182-0
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15182-0