
Abstract
Background
Obesity is associated with an increased breast cancer risk in postmenopausal women and may contribute to worse outcomes. Black women experience higher obesity and breast cancer mortality rates than non-Black women. We examined associations between race, obesity, and clinical tumor stage with breast cancer prognosis.
Methods
We conducted a prospective cohort study in 1,110 breast cancer patients, using univariable and multivariable Cox regression analyses to evaluate the effects of obesity, race/ethnicity, and clinical tumor stage on progression-free and overall survival (PFS and OS).
Results
22% of participants were Black, 64% were Hispanic White, and 14% were non-Hispanic White or another race. 39% of participants were obese (body mass index [BMI] ≥ 30 kg/m2). In univariable analyses, tumor stage III-IV was associated with worse PFS and OS compared to tumor stage 0-II (hazard ratio [HR] = 4.68, 95% confidence interval [CI] = 3.52–6.22 for PFS and HR = 5.92, 95% CI = 4.00-8.77 for OS). Multivariable analysis revealed an association between Black race and worse PFS in obese (HR = 2.19, 95% CI = 1.06–4.51) and non-obese (HR = 2.11, 95% CI = 1.05–4.21) women with tumors staged 0-II. Obesity alone was not associated with worse PFS or OS.
Conclusions
Results suggest a complex interrelationship between obesity and race in breast cancer prognosis. The association between the Black race and worse PFS in tumor stages 0-II underscores the importance of early intervention in this group. Future studies are warranted to evaluate whether alternative measures of body composition and biomarkers are better prognostic indicators than BMI among Black breast cancer survivors.
Similar content being viewed by others
Background
The increasing prevalence of obesity in the United States presents a public health challenge. About 42.4% of American adults are obese and non-Hispanic Black adults are disproportionately affected [1]. Obesity is a risk factor associated with multiple health consequences, including diabetes, hypertension, dyslipidemia, stroke, and all-cause mortality [2]. Importantly, accumulating evidence suggests that obesity is linked to breast cancer incidence, recurrence, and worse clinical outcomes [3,4,5,6].
Women who are obese are more likely to present at a later stage of the disease, with larger tumors and more positive lymph nodes at the time of diagnosis [4, 7, 8]. Additionally, obesity is associated with more treatment complications and reduced efficacy of chemotherapy and hormone therapy, contributing to higher rates of locoregional recurrence compared to non-obese women [5]. Obesity is linked to an increased risk of developing a second primary cancer, particularly of the contralateral breast, endometrium, and colon [3, 4, 9], and a greater risk of distant metastases at ten-year follow-up [7]. Finally, obesity is associated with worse overall and disease-free survival [3, 5, 8, 10, 11].
Multiple mechanisms underly the association between obesity and breast cancer outcomes. First, aromatase activity in adipose tissue raises circulating estrogen levels. Estrogen has a proliferative effect on breast tissue, contributing to incidence and recurrence [5]. Second, adipose tissue is highly metabolically active [3, 5]. Production of proinflammatory cytokines tumor necrosis factor alpha (TNF-alpha) and interleukin six (IL-6) in adipose may contribute to breast cancer pathogenesis [5]. The adipokine leptin, which increases in proportion to body mass index (BMI) is also thought to be implicated in cancer progression and metastasis [3, 12]. High levels of leptin have been shown to promote tumor cell migration and invasion, induce epithelial-to-mesenchymal transition, stimulate angiogenesis, and promote breast cancer stem cell survival [3].
The prevalence of obesity varies by race and breast cancer prognosis [13]. Although the risk of developing breast cancer is similar in Black and White women, Black women are more likely to die from breast cancer [13]. Racial disparities in prognosis may be driven by multiple biological and non-biological factors [13]. Low socioeconomic status and other social factors experienced by Black women may limit access to healthcare and cause delays in screening, detection, and treatment [13,14,15]. The higher prevalence of comorbid conditions, including obesity, diabetes, hypertension, and cardiovascular and respiratory disease, among Black women is also hypothesized to contribute to worse clinical outcomes [5, 13, 14]. In addition, the incidence of triple-negative breast cancer (TNBC), an aggressive and treatment-resistant subtype, is also higher among Black women [14]. Biological factors underlying racial differences in outcomes include differences in the tumor microenvironment, gene expression, tumor suppressors, and genetic susceptibility loci [13, 16]. Multiple studies have identified differences in the expression of cancer-associated genes in Black women compared to White women [17,18,19]. Because gene expression can be altered by environmental and/or lifestyle factors, epigenetic influences may mediate the link between non-biological factors such as race or obesity, and the biological factors associated with worse breast cancer prognosis.
Accumulating evidence suggests that the relationship between obesity, race, and clinical tumor stage in breast cancer prognosis is complex [16, 20,21,22,23,24,25,26]. This study aims to evaluate the characteristics associated with progression-free and overall survival in a racially and ethnically diverse cohort of breast cancer patients [22]. We assess the interrelationship among BMI, race, and clinical tumor stage in breast cancer prognosis to improve patient counseling and guide the development of targeted interventions for high-risk groups.
Methods
Study population
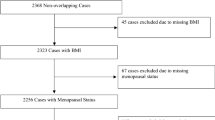
We evaluated 1,115 post-surgical breast cancer patients scheduled to receive adjuvant radiation therapy (RT) at the Sylvester Comprehensive Cancer Center (SCCC) and Jackson Memorial Hospital (JMH) in Miami, Florida, between 2008 and 2014. Participants were recruited for a case-control study and/or a study assessing RT-induced skin toxicity to the intact breast. Each patient completed a self-administered questionnaire with [1] demographic information [2], self-reported race and ethnicity [3], self-reported height and weight, and [4] assessment of breast cancer risk factors (including family history, presence of comorbidities, and smoking status). Clinical and pathological tumor characteristics were obtained from pathology reports and medical records. Informed consent was obtained from all participants at the time of enrollment. This study was approved by the Institutional Review Board at the University of Miami and Jackson Memorial Hospital.
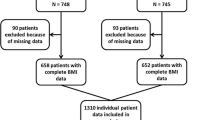
Inclusion criteria included female patients aged 18 or older who were diagnosed with breast carcinoma stages 0-IV (American Joint Committee on Cancer), were scheduled to receive treatments at SCCC or JMH between 2008 and 2014 and were able and willing to provide informed consent. Exclusion criteria included patients who were aged less than 18, received prior radiation to the currently treated breast or chest wall, were undergoing concurrent chemotherapy, or were unable to provide written consent. We had a final sample size of 1,110 following the exclusion of participants who were lost to follow-up or had missing information.
Assessment of patient and clinical variables
We evaluated race (non-Black or Black), obesity status (obese or non-obese), age at diagnosis (< 60 years or ≥ 60 years), and smoking status (never, former, or current) as patient covariates. Former smoking was defined as having smoked 100 or more lifetime cigarettes and current smoking was defined as active smoking. Clinical variables, including estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), and triple-negative (TN) status, as well as clinical tumor stage (0-II or III-IV), were determined using medical records. The clinical tumor stage was based on the American Joint Committee on Cancer staging scheme [27]. Body mass index (BMI) was calculated using the National Institute of Health (NIH) conversion formula using self-reported height and weight at the time of enrollment. In the current study, BMI < 30 was considered non-obese and BMI ≥ 30 was considered obese.
Assessment of progression-free survival and overall survival
Participants were followed for up to 13 years through a review of the medical records, with the evaluation completed as of July 31, 2021. Progression-free survival (PFS) was defined as the time elapsed from diagnosis to the earliest date of disease progression (second primary, recurrence, metastasis, or death). Overall survival (OS) was defined as the time elapsed from diagnosis to death. Event-free patients were censored at the date of the last follow-up.
Statistical analysis
Descriptive statistics (Number, percent) are presented for patient and clinical characteristics stratified by obesity status. The bivariate association of obesity status and patient and clinical characteristics was assessed by a Chi-square test for categorical variables. PFS was defined as the time from diagnosis to recurrence, metastasis, secondary breast cancer, death, or last follow-up, whichever occurred first. OS was defined as the time from diagnosis to death or last follow-up. Event-free patients were censored at the date of the last follow-up. Selected covariates associated with obesity or with PFS or OS were included in the multivariable Cox regression model based on univariable analysis and literature review. PFS and OS were estimated by the Kaplan-Meier method and the associations with race and obesity were assessed by a log-rank test. Univariable Cox proportional hazard analysis was used for potential covariables on time-to-event outcomes of PFS and OS. Multivariable Cox proportional hazard analysis was used to assess the association between pretreatment obesity and race category with PFS and OS adjusted for selected covariables. The non-Black obese group was selected as the reference group in multivariable analyses, as Kaplan Meier survival analyses revealed this group to have lower or equal PFS and OS compared to other groups (Fig. 1). Results were reported as hazard ratios (HR) with 95% confidence intervals (95% CI). Statistical significance was set at a threshold of P < 0.05. The heterogeneity of obesity effect by race and by tumor stage was assessed in multivariable analyses stratified by clinical tumor stage (0-II and III-IV). Data analysis was conducted using SAS (version 9.4, Cary, NC).

Progression-free survival and overall survival by race and obesity. Kaplan-Meier curves demonstrating PFS and OS by race and obesity, stratified by clinical tumor stage. A PFS in all participants B PFS in clinical tumor stage 0-II C PFS in clinical tumor stage III-IV D OS in all participants E OS in clinical tumor stage 0-II F OS in clinical tumor stage III-IV. PFS, progression-free survival; OS, overall survival; B, Black race; NB, Non-Black race. Obese was defined as BMI ≥ 30 and non-obese was defined as BMI < 30 (kg/m2). P-values were determined using a log-rank test; a p-value < 0.05 was considered statistically significant
Results
Patient and clinical characteristics
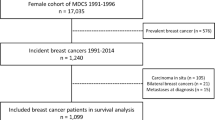
The study population included 1,110 breast cancer patients, 918 (82.7%) of whom were progression-free by the last follow-up and 192 (17.3%) of whom experienced disease progression (including 105 deaths, seven second-primary cancers, 48 breast cancer recurrences, and 123 metastases). 75 women (6.8%) experienced two or more outcomes. The mean age at diagnosis was 54.7 years (range: 24.5–85.0). 30.5% of participants were ≥ 60 years old at diagnosis and 69.5% were < 60 years old. Most of our sample self-identified as Hispanic White (64.1%), 21.7% of participants identified as Black, and 14.1% identified as Non-Hispanic White or another race/ethnicity. Non-Hispanic White and Other categories were combined due to their similar progression-free and overall survival. 76.4% of participants had stage 0-II disease upon enrollment and 23.6% of participants had stage III-IV disease.
38.7% of participants were obese, defined as BMI ≥ 30 kg/m2. A significantly higher proportion of obese participants were ≥ 60 years old at diagnosis (43.2% vs. 36.8% <60 years old; p = 0.044), Black (52.3% vs. 35.0% non-Black; p < 0.001), never smokers (40.4% vs. 39.6% for former smokers vs. 23.7% for current smokers) and had ≥ 2 comorbid conditions (52.4% vs. 44.2% for one comorbidity vs. 26.8% for no comorbidities; p < 0.001). Additional patient and tumor characteristics are summarized in Table 1.
Univariable Cox regression analysis of progression-free survival
Univariable analysis in Table 2 reveals a significantly worse PFS for Black (HR: 1.63, 95% CI: 1.20–2.22) compared to non-Black race and for Hispanic White (HR: 2.36, 95% CI: 1.30–4.27) or Black (HR: 3.44, 95% CI: 1.85–6.40) race/ethnicity, compared to non-Hispanic White/Other. There was a significantly worse PFS for clinical tumor stages III-IV (HR: 4.68, 95% CI: 3.52–6.22) compared to clinical tumor stages 0-II, and worse PFS for tumors that were ER-negative (HR: 1.83, 95% CI: 1.36–2.45), PR-negative (HR: 1.83, 95% CI: 1.38–2.43), HER2-positive (HR: 1.46, 95% CI: 1.04–2.07), or triple-negative (HR: 1.88, 95% CI: 1.35–2.63).
Univariable Cox regression analysis of overall survival
Univariable analysis in Table 3 shows a significantly worse OS for Black (HR: 1.63, 95% CI: 1.07–2.47) compared to non-Black race, for Hispanic White (HR: 2.49, 95% CI: 1.08–5.74) or Black (HR: 3.61, 95% CI 1.51–8.64) race/ethnicity compared to non-Hispanic White/Other, and for former smokers (HR: 1.72, 95% CI: 1.17–2.53) compared to never smokers. Current smoking was associated with worse OS, but this was not statistically significant (HR: 1.86, 95% CI: 1.00-3.47). There was a significantly worse OS for clinical tumor stages III-IV (HR: 5.92, 95% CI: 4.00-8.77) compared to tumor stages 0-II, and worse OS for tumors that were ER-negative (HR: 2.04, 95% CI: 1.38–3.02), PR-negative (HR: 2.33, 95% CI: 1.59–3.43), or triple-negative (HR: 2.38, 95% CI: 1.55–3.66).
Multivariable Cox regression analysis of progression-free survival and overall survival by clinical tumor stage
For combined race and obesity at clinical tumor stages 0-II (Table 4A), being Black and obese or Black and non-obese was associated with worse PFS (HR: 2.11, 95% CI: 1.05–4.21 for Black-obese and HR: 2.19, 95% CI: 1.06–4.51 for Black-non-obese). Former smoking was associated with worse OS (HR: 2.82, 95% CI: 1.47–5.41). Current smoking was also associated with worse OS (HR: 2.61, 95% CI: 0.95–7.12), though this was not statistically significant. At clinical tumor stages III-IV (Table 4B), only TNBC was significantly associated with worse PFS (HR: 1.63, 95% CI: 1.04–2.55) and OS (HR: 2.70, 95% CI: 1.58–4.61).
Discussion
This study uses a large racially and ethnically diverse population to evaluate patient and clinical characteristics associated with worse PFS and OS in early (clinical tumor stages 0-II) and advanced (clinical tumor stages III-IV) breast cancer. Race and obesity status were combined in multivariable models to evaluate their joint effects. In the early breast cancer group, obese and non-obese Black women had significantly higher hazards of progression compared to non-Black, obese women. Our results emphasize the importance of race as a prognostic indicator in breast cancer that, when combined with obesity status, may contribute to worse outcomes. We know from prior studies that Black women are more likely to have worse breast cancer prognosis despite a similar risk of developing breast cancer compared to their White counterparts [13]. Reasons for this disparity include racial differences in the tumor microenvironment, gene expression, socioeconomic status, and access to healthcare.
We found a significant association between combined race and obesity with worse PFS in early, but not advanced breast cancer (Table 4A and 4B). Differences in gene expression by race and obesity status may underlie disparities in outcomes; such differences may also vary by tumor stage and subtype. For example, Do et al. observed differential hypomethylation of obesity-associated genes in Black women, which was associated with greater all-cause mortality compared to White women [20]. Xing et al. identified increased expression of SOS1, a gene that is activated by a compound secreted from adipocytes, implicated in anti-apoptotic pathways, and has been linked to breast cancer progression and metastasis, in Black women compared to White women, as well as altered expression of its epigenetic regulatory elements [16]. SOS1 is activated by a compound secreted from adipocytes. Finally, resistin is another gene that may mediate this link, as it is associated with obesity, insulin resistance, and breast cancer risk, and is expressed higher in the tumors of Black women than in White women [21, 24]. Like our findings, Vallega et al. observed increased resistin expression in Black women for tumors that were early-stage and receptor-negative [21]. They did not observe any difference in resistin expression in Stage III tumors in interracial comparisons [21]. Importantly, our observation of worse PFS in stage 0-II disease but not at later stages highlights the importance of early intervention strategies in Black women with breast cancer, due to the higher hazard of progression of early-stage disease compared to non-Black women. Future studies are needed to uncover which molecular pathways are differentially activated by race and obesity and why, paving the way for novel therapeutics and policy interventions.
Although previous studies suggest that obesity is independently associated with breast cancer incidence, recurrence, and worse clinical outcomes, we did not identify an association of obesity status with PFS or OS that was independent of race [3,4,5,6]. It is possible that race is a more substantial driver of outcomes than obesity in this cohort, or that the interaction between race and obesity is a stronger driver of outcomes than obesity alone. Previous works highlight the interaction between race and obesity at the molecular level; epigenetic modulation of multiple tumorigenic molecular pathways in adipocytes has been linked to differences in all-cause mortality, progression, and metastasis in Black women compared to White women [16, 18,19,20,21, 28].
The lack of association of obesity status with PFS or OS may be attributed to the limitations of BMI as a measure of obesity. Emerging evidence suggests that BMI is an oversimplified metric, as it does not distinguish between muscle and adipose, nor does it describe patterns of adipose distribution [29,30,31]. Adipose tissue is nonuniform, and while there is some evidence to suggest that subcutaneous fat provides nutritional reserve in advanced cancer, visceral adipose is pro-inflammatory, with a poor cardiometabolic risk profile that promotes tumor growth [29]. In addition, high muscle mass may be linked to better cancer outcomes, whereas low muscle mass has been associated with recurrence, surgical complications, treatment toxicity, and worse OS [29]. Because BMI does not account for muscle mass, those with higher muscle mass may be misclassified as obese despite a potentially lower risk of progression. Finally, in a study of Black breast cancer survivors, higher waist-to-hip ratio and central adiposity were associated with worse breast cancer-specific and overall survival, whereas BMI was not associated with worse outcomes [30]. The findings in our study may reflect the limitations of BMI as a measure of obesity and future studies are needed to evaluate whether central obesity or higher adiposity are more sensitive prognostic indicators for predicting PFS or OS in Black breast cancer survivors.
Kaplan Meier survival analyses revealed that non-Black obese women had the lowest hazard of progression among all participants in the tumor stage 0-II group (Fig. 1). Non-Black obese and non-Black non-obese women performed similarly in terms of OS. Accordingly, the non-Black obese group was selected as the reference group in multivariable analyses. Emerging literature describes an ‘obesity paradox’ in which obesity is associated with worse outcomes in early cancer, but is protective at later stages by providing a nutritional reserve to protect against cachexia [23, 26, 32]. The findings in Fig. 1 may reflect a slightly protective effect of obesity. However, we observe this finding in the early-stage group only and not at later stages, which is inconsistent with descriptions of the obesity paradox. Any protective effects of obesity in the advanced group may be obscured by the small sample size attributed to (a) the smaller proportion of participants with advanced-stage cancer and (b) the smaller proportion of participants with advanced-stage cancer who remain obese despite the associated wasting. Future studies with larger samples are necessary to better characterize the conditions under which obesity may benefit cancer patients.
The stratified multivariable analyses demonstrate an association of TNBC with worse PFS and OS in the advanced breast cancer group. The association with worse outcomes in this cohort is best explained by the aggressiveness of TNBC. TNBC lacks hormone receptor expression and is thus not susceptible to hormonal therapies, leading to worse outcomes [33, 34]. Additionally, TNBC grows faster than other subtypes and is more likely to be diagnosed at a later stage, as evidenced by the higher proportion of patients with TNBC (22.3%) in the advanced breast cancer group compared to the early breast cancer group (13.7%).
Multivariable Cox models revealed a 2.82-fold increased hazard of death in former smokers compared to never smokers in the early-stage breast cancer group (95% CI, 1.47–5.41) (Table 4A). These findings are consistent with the known association of smoking with widespread organ damage, all-cause mortality, and cancer-specific mortality [35]. There was a similar 2.61-fold increased hazard of death associated with current smoking, though this finding was not statistically significant (Table 4A). The lack of significant association of current smoking with PFS or OS in either group or of former smoking with PFS or OS in the advanced-stage group is likely due to the small sample size.
This study has several strengths. First, a prospective study design is appropriate to assess the patient and clinical characteristics associated with PFS and OS. In addition, we utilize a large racially and ethnically diverse cohort that we followed for up to 13 years, enabling us to evaluate inter-group differences in outcomes. Moreover, previous studies suggest that genetic and epigenetic factors may also play a role in breast cancer prognosis [22]. For this cohort, we have both outcome and genome-wide association studies (GWAS) data available, which enables us to conduct future research using genetic prediction models to examine the factors that contribute to breast cancer prognosis.
This study has several limitations. First, the lack of association between race, obesity, and worse PFS or OS in advanced breast cancer could be attributed to the small sample size in the advanced breast cancer group. Future studies with larger sample sizes are necessary to elucidate potential differences. Second, our use of BMI as a measure of obesity may not accurately reflect differences in adiposity. Our decision to use BMI was based on its extensive use in previous studies and the patient data that was available from the study enrollment survey. Third, our patient population includes a large proportion of Hispanic White individuals, reflecting the racial and ethnic composition of the local population; results may therefore not be generalizable to all populations. In addition, our study findings are limited by the small sample size of Black individuals, as demonstrated by the wide confidence intervals. Finally, our study protocol did not evaluate socioeconomic status or a proxy such as insurance status. It is possible that potential residual confounding of unmeasured variables may contribute to the outcomes observed.
Conclusions
Our findings suggest a complex relationship between obesity and race in breast cancer prognosis. The significant association of combined Black race and obesity status with worse PFS in early-stage breast cancer highlights the importance of targeted early intervention strategies among Black women with breast cancer. An interaction of race and obesity at the molecular level may contribute to the observed differences in PFS; future studies are needed to characterize how environmental and lifestyle factors may alter the expression of cancer-associated genes. Finally, the lack of association between obesity status and PFS or OS in this study may suggest that alternate measures of body composition better illustrate the role of obesity in breast cancer outcomes. Future studies need evaluate whether central obesity and adiposity are more sensitive prognostic indicators.
Data availability
Availability of data and materials: The data sets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- BMI:
-
body mass index
- CI:
-
confidence interval
- ER:
-
estrogen receptor
- HR:
-
hazard ratio
- HER2:
-
human epidermal growth factor receptor 2
- OS:
-
overall survival
- PR:
-
progesterone receptor
- PFS:
-
progression-free survival
- TNBC:
-
triple-negative breast cancer
References
Hales CMCM, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. In: Statistics NCfH, editor. NCHS Data Brief, no 360. Hyattsville, MD2020.
NHLBI. Guidelines (2013) for managing overweight and obesity in adults. Preface to the Expert Panel Report (comprehensive version which includes systematic evidence review, evidence statements, and recommendations). Obes (Silver Spring). 2014;22(Suppl 2):S40.
Barone I, Giordano C, Bonofiglio D, Andò S, Catalano S. The weight of obesity in breast cancer progression and metastasis: clinical and molecular perspectives. Sem Cancer Biol. 2020;60:274–84.
Ecker BL, Lee JY, Sterner CJ, Solomon AC, Pant DK, Shen F, et al. Impact of obesity on breast cancer recurrence and minimal residual disease. Breast Cancer Res. 2019;21(1):41.
Lee K, Kruper L, Dieli-Conwright CM, Mortimer JE. The impact of obesity on breast Cancer diagnosis and treatment. Curr Oncol Rep. 2019;21(5):41.
Warren LE, Ligibel JA, Chen YH, Truong L, Catalano PJ, Bellon JR. Body Mass Index and Locoregional recurrence in women with early-stage breast Cancer. Ann Surg Oncol. 2016;23(12):3870–9.
Ewertz M, Jensen M-B, Gunnarsdóttir KÁ, Højris I, Jakobsen EH, Nielsen D, et al. Effect of obesity on Prognosis after early-stage breast Cancer. J Clin Oncol. 2010;29(1):25–31.
Majed B, Moreau T, Senouci K, Salmon RJ, Fourquet A, Asselain B. Is obesity an independent prognosis factor in woman breast cancer? Breast Cancer Res Treat. 2008;111(2):329–42.
Druesne-Pecollo N, Touvier M, Barrandon E, Chan DS, Norat T, Zelek L, et al. Excess body weight and second primary cancer risk after breast cancer: a systematic review and meta-analysis of prospective studies. Breast Cancer Res Treat. 2012;135(3):647–54.
Chan DSM, Vieira AR, Aune D, Bandera EV, Greenwood DC, McTiernan A, et al. Body mass index and survival in women with breast cancer—systematic literature review and meta-analysis of 82 follow-up studies. Ann Oncol. 2014;25(10):1901–14.
Dawood S, Broglio K, Gonzalez-Angulo AM, Kau SW, Islam R, Hortobagyi GN, et al. Prognostic value of body mass index in locally advanced breast cancer. Clin Cancer Res. 2008;14(6):1718–25.
Ando S, Gelsomino L, Panza S, Giordano C, Bonofiglio D, Barone I et al. Obesity, leptin and breast Cancer: epidemiological evidence and proposed mechanisms. Cancers (Basel). 2019;11(1).
Yedjou CG, Tchounwou PB, Payton M, Miele L, Fonseca DD, Lowe L et al. Assessing the racial and ethnic disparities in breast Cancer mortality in the United States. Int J Environ Res Public Health. 2017;14(5).
Dietze EC, Chavez TA, Seewaldt VL. Obesity and triple-negative breast Cancer: disparities, controversies, and Biology. Am J Pathol. 2018;188(2):280–90.
Foy KC, Fisher JL, Lustberg MB, Gray DM, DeGraffinreid CR, Paskett ED. Disparities in breast cancer tumor characteristics, treatment, time to treatment, and survival probability among African American and white women. NPJ Breast Cancer. 2018;4:7.
Xing F, Zhao D, Wu SY, Tyagi A, Wu K, Sharma S, et al. Epigenetic and posttranscriptional modulation of SOS1 can promote breast Cancer metastasis through obesity-activated c-Met Signaling in African-American Women. Cancer Res. 2021;81(11):3008–21.
Huang T, Huang X, Nie Y, Shi X, Shu C. A combined effect of expression levels of obesity-related genes and clinical factors on Cancer Survival Rate. Biomed Res Int. 2020;2020:8838676.
Zhang F, Liu S. Mechanistic insights of adipocyte metabolism in regulating breast cancer progression. Pharmacol Res. 2020;155:104741.
Ilozumba MN, Yao S, Llanos AAM, Omilian AR, Zhang W, Datta S, et al. mTOR pathway gene expression in association with race and clinicopathological characteristics in Black and White breast cancer patients. Discov Oncol. 2022;13(1):34.
Do WL, Conneely K, Gabram-Mendola S, Krishnamurti U, D’Angelo O, Miller-Kleinhenz J, et al. Obesity-associated methylation in breast tumors: a possible link to disparate outcomes? Breast Cancer Res Treat. 2020;181(1):135–44.
Vallega KA, Liu N, Myers JS, Yu K, Sang QX. Elevated Resistin Gene expression in African American estrogen and progesterone receptor negative breast Cancer. PLoS ONE. 2016;11(6):e0157741.
Puyana C, Schindler E, Lee E, Hu JJ. Genetic predisposition to obesity and inflammation in a tri-racial/ethnic breast cancer population. J Translational Genet Genomics. 2022;6(2):223–39.
Modi ND, Tan JQE, Rowland A, Koczwara B, Abuhelwa AY, Kichenadasse G, et al. The obesity paradox in early and advanced HER2 positive breast cancer: pooled analysis of clinical trial data. npj Breast Cancer. 2021;7(1):30.
Stewart PA, Luks J, Roycik MD, Sang QX, Zhang J. Differentially expressed transcripts and dysregulated signaling pathways and networks in African American breast cancer. PLoS ONE. 2013;8(12):e82460.
McQuade JL, Daniel CR, Hess KR, Mak C, Wang DY, Rai RR, et al. Association of body-mass index and outcomes in patients with metastatic melanoma treated with targeted therapy, immunotherapy, or chemotherapy: a retrospective, multicohort analysis. Lancet Oncol. 2018;19(3):310–22.
Lennon H, Sperrin M, Badrick E, Renehan AG. The obesity Paradox in Cancer: a review. Curr Oncol Rep. 2016;18(9):56.
Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The Eighth Edition AJCC Cancer staging Manual: continuing to build a bridge from a population-based to a more personalized approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–9.
McCullough LE, Chen J, Cho YH, Khankari NK, Bradshaw PT, White AJ, et al. DNA methylation modifies the association between obesity and survival after breast cancer diagnosis. Breast Cancer Res Treat. 2016;156(1):183–94.
Caan BJ, Cespedes Feliciano EM, Kroenke CH. The importance of body composition in explaining the overweight Paradox in Cancer-counterpoint. Cancer Res. 2018;78(8):1906–12.
Bandera EV, Qin B, Lin Y, Zeinomar N, Xu B, Chanumolu D, et al. Association of Body Mass Index, Central Obesity, and body composition with mortality among black breast Cancer survivors. JAMA Oncol. 2021;7(8):1–10.
Buss J. Limitations of body mass index to assess body fat. Workplace Health Saf. 2014;62(6):264.
Alarfi H, Salamoon M, Kadri M, Alammar M, Haykal MA, Alseoudi A, et al. The impact of baseline body mass index on clinical outcomes in metastatic breast cancer: a prospective study. BMC Res Notes. 2017;10(1):550.
Yin L, Duan J-J, Bian X-W, Yu S-c. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res. 2020;22(1):61.
Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast Cancer. N Engl J Med. 2010;363(20):1938–48.
Services USDoHaH. The Health consequences of Smoking—50 years of progress: a report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014.
Acknowledgements
The authors would like to thank the participants and the clinical staff in the department of Radiation Oncology at the University of Miami Sylvester Comprehensive Cancer Center and Jackson Memorial Hospital.
Funding
This study was supported by a grant funded by the National Institutes of Health (R01CA135288, R03CA195643, and R21CA234880 to Hu JJ).
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript. EAS, WZ, and JJH made substantial contributions to the conception, design, and drafting of the work. EAS, WZ, JJH, and IMR have made substantial contributions to the analysis and interpretation of the data. CT, FCM, GRY, and LGA have made substantial contributions to patient enrollment and data collection.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board at the University of Miami and Jackson Memorial Hospital. Informed consent was obtained from all participants upon enrollment.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schindler, E.A., Takita, C., Collado-Mesa, F. et al. The interrelationship between obesity and race in breast cancer prognosis: a prospective cohort study. BMC Women's Health 24, 312 (2024). https://doi.org/10.1186/s12905-024-03020-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-024-03020-3