
Abstract
Purpose
Examine the association between obesity and clinical outcomes in early breast cancer and assess if patient, tumor, and treatment characteristics modify such associations in Malmö Diet and Cancer Study patients (MDCS).
Methods
The MDCS enrolled 17,035 Swedish women from 1991 to 1996. At enrollment, participants' body mass index (BMI), waist circumference and body fat percentage measures were collected. We identified all female MDCS participants with invasive breast cancer from 1991 to 2014. Follow-up began at breast cancer diagnosis and ended at breast cancer recurrence (BCR), death, emigration, or June 8, 2020. The World Health Organization guidelines were used to classify BMI, waist circumference, and body fat percentage into three categories of healthy weight, overweight, and obesity. We fit Cox regression models to compute adjusted hazard ratios (HRs) with 95% confidence intervals (CI) of BCR according to body composition. To evaluate effect measure modification, we stratified Cox models by patient, tumor, and treatment characteristics.
Results
In total, 263 BCRs were diagnosed over 12,816 person-years among 1099 breast cancer patients with a median follow-up of 11.1 years. Obesity according to BMI (HR = 1.44 [95%CI 1.00–2.07]), waist circumference (HR = 1.31 [95%CI 0.98–1.77]), and body fat percentage (HR = 1.41 [95%CI 1.02–1.98]) was associated with increased risk of BCR compared with healthy weight. Obesity was stronger associated with BCR in patients with low socioeconomic position (HR = 2.55 [95%CI 1.08–6.02]), larger tumors > 20 mm (HR = 2.68 [95%CI 1.42–5.06]), estrogen-receptor-negative breast cancer (HR = 3.13 [95%CI 1.09–8.97]), and with adjuvant chemotherapy treatment (HR = 2.06 [95%CI 1.08–4.31]).
Conclusion
Higher pre-diagnostic BMI, waist circumference, and body fat percentage was associated with increased risk of BCR. The association between obesity and BCR appears dependent on patient, tumor, and treatment characteristics.
Similar content being viewed by others

Introduction
Since the 1980s, advances in breast cancer detection and treatment have resulted in an increasing number of patients surviving breast cancer [1, 2]. Concurrently there has been an increase in obesity prevalence [3] with globally 110,000 breast cancer cases attributable to excess body weight in 2012 [4]. This has motivated researchers to investigate preventive public health interventions [5] and initiate trials with weight-loss interventions [6] to reduce the risk and improve the outcome of breast cancer. Yet, limited research has been carried out to identify characteristics of breast cancer patients that have negative health effects of their obesity. Obesity may be associated with poor breast cancer prognosis due to insufficient treatment [7]. For example, chemotherapy is dosed based on body surface area and the drug dosage determination guidelines include a praxis called dose-capping, meaning that a reduced, sub-optimal, chemotherapy dose may be prescribed to patients with obesity to minimize toxicities [7, 8]. Patients with greater body size can also be affected by underdosing due to underestimated body surface area [9]. Further, treatment with aromatase inhibitors may be less effective in breast cancer patients with obesity due to their inherently higher levels of aromatase [10, 11]. Obesity may also be associated with poor breast cancer prognosis due to metabolic changes. In individuals with obesity, white adipocytes are likely to become hypertrophic and hyperplastic, resulting in physiologic changes such as elevated FFAs and triglycerides, increased blood glucose, and insulin resistance. Further, obesity-associated adipose tissue produces more pro-inflammatory cytokines, such as tumor necrosis factor alpha, interleukin-6, interleukin-1, and adipokines. Through these mechanisms the presence of excess adipocytes and the obesity-induced change in adipose tissue may promote the early stages of metastasis [12,13,14]. To identify breast cancer patients with obesity at higher risk of disease recurrence and death, it is important to investigate whether patient, tumor and treatment characteristics can predict patient sub-populations in need of improved surveillance and/or treatment.
Body mass index (BMI) is still the standard tool for measuring and defining obesity [15]. Yet, BMI is controversial and its specificity questioned. Several other anthropometric measures have been suggested as more precise in determining obesity [15] and may be relevant to use systematically when assessing breast cancer patients for treatment.
The purpose of this study was to examine the association between pre-diagnostic anthropometric measures and breast cancer outcomes in the Malmö Diet and Cancer Study (MDCS). Further, the study aimed to assess patient, tumor and treatment characteristics associated with prognosis in breast cancer patients with obesity.
Patients and methods
We conducted a prospective cohort study nested in the MDCS cohort.
Data sources
The MDCS is a prospective cohort study that enrolled 17,035 women in Malmö, Sweden from 1991 to 1996. The primary objective of the MDCS was to investigate associations between dietary patterns and cancer risk. The MDCS enrolled 42.6% of the eligible population born between 1923 and 1950 [16]. The MDCS is updated annually with information on incident cancer cases and vital status through record linkage to the Swedish Cancer Registry, the Southern Swedish Regional Tumor Registry, and the Swedish Cause of Death Registry. All Swedish residents have a unique civil registration number in the National Population Register, allowing for 100% accurate data linking.
Study population
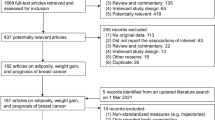
Between 1991 and 2014, 1240 female MDCS participants were diagnosed with invasive breast cancer (Fig. 1). Participants with a breast cancer diagnosis before enrollment in MDCS were excluded as prevalent cases. We also excluded participants with carcinoma in situ, bilateral breast cancer or de novo metastatic disease. The final study population in the survival analyses included 1099 female breast cancer patients.

Flowchart of the study population. *MDCS = Malmö Diet and Cancer Study
Anthropometric measures
Trained research nurses collected anthropometric measures including, height, weight, waist circumference, and body fat percentage upon enrollment in the MDCS [16, 17]. Hence, the anthropometric data used in this study was collected at study baseline prior to the diagnosis of breast cancer. We used the World Health Organization’s definition of BMI in kg/m2, waist circumference in centimeters and body fat percentage to group the patients according to body composition [18]. Patients with a BMI of 18.5–24.9 kg/m2, a waist circumference below 81 cm, or a body fat percentage of 24% or lower were considered to have healthy weight. Patients with a BMI of 25.0–29.9 kg/m2, a waist circumference between 81 and 85 cm, or a body fat percentage exceeding 24% but below 32%, were considered to have overweight. Patients with a BMI of more than 30.0 kg/m2, a waist circumference of more than 85 cm, or a body fat percentage of 32% or more were considered to have obesity [18]. In the multivariable models, these variables were included as categorical variables with healthy weight as the reference group.
A body shape index (ABSI) has been suggested to predict mortality risk more precisely than alternative anthropometric measures. Therefore, we calculated ABSI according to the suggested formula by Krakauer and Krakauer [19]:
In multivariable analyses, ABSI was divided into cohort-specific tertiles and the first tertile was used as the reference group.
BMI was used to determine body composition for descriptive purposes of patient characteristics in Table 1 and sensitivity analyses.
Socioeconomic position
Consistent with the Swedish socioeconomic classification [20], we categorized socioeconomic position (SEP) for descriptive purposes as low if patients had unskilled manual labor with < 2 years of post-high school education, low-middle if skilled manual labor with > 2 years of post-high school education, high-middle if assistant non-manual labor with < 3 years of post-high school education, and high if non-manual labor with ≥ 3 years of post-high school education. In multivariable models, SEP was dichotomized into low SEP vs high SEP. The low SEP group included patients categorized as low or low-middle and the high SEP group included patients categorized as high-middle and high.
Definitions of analytic variables
Age was described as the median age at breast cancer diagnosis. In the multivariable models, age was included as a continuous variable defined at the time of breast cancer diagnosis.
We defined three categories of tumor size in millimeters (mm): less than 10 mm, 10–20 mm, and more than 20 mm. Tumor size was modeled as a categorical variable [21]. In sensitivity analyses, tumor size was modeled as a dichotomous variable (≤ 20 mm/ > 20 mm). The histological grade of breast cancer was assessed and described according to the Nottingham Histological Grade [22] and categorized as grade I, grade II, and grade III; this was modeled as a categorical variable. Menopausal status at diagnosis (premenopausal/postmenopausal), estrogen-receptor (ER) status (positive/negative), lymph node status (positive [present metastatic lymph nodes]/negative [no metastatic lymph nodes]), surgery (breast cancer conserving surgery/mastectomy), along with the intended adjuvant treatment with radiation (yes/no), chemotherapy (yes/no), and endocrine therapy (yes/no) were all treated as dichotomous variables.
Outcome
The primary endpoint was breast cancer recurrence (BCR), defined as the time from breast cancer diagnosis until the earliest occurrence of invasive loco-regional recurrence or distant metastases. Trained medical doctors retrieved data on recurrence from medical charts of all patients diagnosed with breast cancer in the MDCS. The secondary endpoint was mortality, defined as the time from breast cancer diagnosis until death from any cause. Data on mortality was retrieved from the Swedish Cause of Death Registry.
Follow-up and statistical analysis
Follow-up for BCR and mortality began at breast cancer diagnosis and continued until the first event of BCR, death, emigration or end of follow-up on June 8, 2020. Patients with these events were censored.
We used Cox regression models to compute crude and adjusted hazard ratios (HRs) with 95% confidence intervals (95%CI) for BCR and mortality. Only patients with complete data on all regressed variables were included in the analyses. The adjusted model included the following co-variables: age at diagnosis (continuous), node status (dichotomous), ER status (dichotomous), histological grade (categorical), tumor size (categorical), type of surgery (dichotomous), adjuvant radiotherapy (dichotomous), adjuvant chemotherapy (dichotomous), and adjuvant endocrine therapy (dichotomous). Complete case data were available for 941 patients, which were included in the adjusted models.
We performed a series of pre-planned sensitivity analyses using Cox regression models adjusted for the previously stated covariates excluding the stratification variable of interest to investigate the association between obesity and breast cancer prognosis. The reference group used for the stratified analyses was within strata, i.e., we compared healthy weight versus obesity among patients with low SEP. First, we examined differences in patient characteristics among healthy weight and breast cancer patients with obesity according to BMI in terms of BCR. Second, we investigated the prognostic value of tumor characteristics according to BMI in relation to BCR. Third, to examine any possible differences in treatment patterns according to BMI, we conducted analyses of BCR and BMI stratified by treatment with adjuvant chemotherapy, radiotherapy, endocrine therapy, and type of primary surgery. Finally, to assess whether the exposure of obesity combined with certain patient, tumor and treatment characteristics was greater than the individual effects alone, we conducted pre-planned interaction tests between obesity and the stratified factors that displayed a negative effect on the outcome. We used logistic regression models adjusted for the previously stated co-variates, dichotomous exposure to obesity, and the variable of interest, we estimated the relative excess risk due to interaction [23].
Results
Among 1099 eligible patients, 263 BCRs were diagnosed over 12,816 person-years with a median follow-up of 11.1 years (interquartile range [IQR] was 6.6–16.2). The median time from collection of anthropometric measures until breast cancer diagnosis was 10.8 years (IQR 6.0–15.4). The cohort consisted of 556 patients with healthy weight, 384 patients with overweight and 159 patients with obesity. In the cohort, median BMI was 24.9 kg/m2 (IQR 22.8–27.7), median waist circumference was 77 cm (IQR 71–84), and the median body fat percentage was 31% (IQR 28–34). The median age at breast cancer diagnosis was 66.3 years (IQR 61.2–72.8). Patients with obesity were generally older than patients with healthy weight (Table 1).
Patients with overweight or obesity according to BMI were more often diagnosed with a higher histological grade, had larger tumors and positive nodal status at diagnosis compared with patients with healthy weight (Table 1). Invasive lobular breast cancer was more common among patients with healthy weight. Endocrine therapy, radiotherapy, and mastectomy were less frequently assigned to patients with overweight than to patients with healthy weight or obesity. However, chemotherapy was more frequently assigned to patients with overweight or obesity than to patients with healthy weight. Patients with obesity had lower SEP than patients with healthy weight, while patients with healthy weight were more likely to smoke than patients with overweight or obesity.
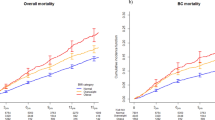
In multivariable analyses, having obesity according to BMI was associated with an increased rate of BCR (HRadj = 1.56 [95%CI 1.00–2.46) and mortality (HRadj = 1.51 [95%CI 1.05–2.18) in comparison to having healthy weight (Table 2). Having obesity according to waist circumference was also associated with a higher risk of BCR (HRadj = 1.46 [95%CI 1.00–2.13]) and mortality (HRadj = 1.45 [95%CI 1.07–1.96]). Patients with obesity according to body fat percentage were at higher risk of BCR (HRadj = 1.41 [95%CI 1.02–1.98]), whereas the precision of the mortality estimate was lower (HRadj = 1.30 [95%CI 0.74–2.27]). Having a high ABSI was not associated with increased risk of BCR (Tertile 3, HRadj = 0.97 [95%CI 0.68–1.39]), but increased risk of mortality (Tertile 3, HRadj = 1.24 [95%CI 0.91–1.71]) (Supplemental Table S1).
In Fig. 2, the association between body composition (BMI) and BCR is depicted according to patient characteristics. Having obesity was associated with BCR in postmenopausal women (HRadj = 1.49 [95%CI 0.98–2.40]). Patients with obesity had an increased risk of BCR if they had low SEP (HRadj = 2.55 [95%CI 1.08–6.02]) or if they were non-smokers (HRadj = 1.66 [95%CI 1.01–2.73]). No association between having obesity and BCR was observed among patients with high SEP (HRadj = 1.47 [95%CI 0.58–3.75]) or smokers (HRadj = 1.12 [95%CI 0.43–2.92]).

The relationship between patient characteristics and recurrence rates in breast cancer patients with healthy weight vs obesity defined by BMI. Forest plot shows adjusted HR (95% CI) of breast cancer recurrence for patients with obesity (BMI ≥ 30.0) compared with patients with healthy weight (BMI 18.5–24.9), according to stratified patient characteristics. *BCR = breast cancer recurrence. **The stratified analyses were adjusted for the following co-variables excluding the stratified variable of interest: age, histological grade, tumor size, nodal status, estrogen-receptor status, surgery, planned adjuvant radio-, chemo-, and endocrine therapy. ***The relative excess risk due to interaction with 95% CI for socioeconomic position was 0.94 (0.11–1.76) indicating a super-additive interaction effect, suggesting that the response to multimodal exposure are greater than the sum of the independent responses to low socioeconomic position or obesity alone
Figure 3 illustrates the relationship between body composition (BMI) and BCR based on tumor characteristics. Certain tumor characteristics were linked to the rate of recurrence, with histological grade III being associated with an increased risk of BCR in breast cancer patients with obesity (HRadj = 2.08 [95%CI 0.99–4.39]). No association between obesity and BCR was observed for patients with histological grade I (HRadj = 1.89 [95%CI 0.49–7.31]) or histological grade II (HRadj = 1.61 [95%CI 0.81–3.19]). In comparison to patients with healthy weight, patients with obesity who had tumors larger than 20 mm at breast cancer diagnosis were at increased risk of BCR (HRadj = 2.68 [95%CI 1.42–5.06]). However, patients with obesity and tumors of 20 mm or less were not at increased risk of BCR (HRadj = 0.91 [95%CI 0.45–1.85]). Patients with obesity who were diagnosed with ductal breast cancer had increased risk of BCR (HRadj = 1.53 [95%CI 1.00–2.34]), while no association was observed among patients diagnosed with lobular breast cancer (HRadj = 0.72 [95%CI 0.31–1.68]). Patients with obesity and ER-negative disease had an increased risk of BCR (HRadj = 3.13 [95%CI 1.09–8.97]) compared with patients with healthy weight. Similarly, patients with obesity and ER-positive disease had increased risk of BCR compared with patients with healthy weight (HRadj = 1.38 [95%CI 0.98–2.02]).

The relationship between tumor characteristics and recurrence rates in breast cancer patients with healthy weight vs with obesity defined by BMI. Forest plot shows adjusted HR (95% CI) of breast cancer recurrence for patients with obesity (BMI ≥ 30.0) compared with patients with healthy weight (BMI 18.5–24.9), according to stratified tumor characteristics. *BCR = breast cancer recurrence; ER = estrogen receptor. ** The stratified analyses were adjusted for the following co-variables excluding the stratified variable of interest: age, histological grade, tumor size, nodal status, estrogen-receptor status, surgery, planned adjuvant radio-, chemo-, and endocrine therapy. *** The relative excess risk due to interaction (RERI) with 95% CI for tumor size > 20 mm was 1.78 (− 0.16–3.72)”. The relative excess risk due to interaction with 95% CI for ER-negative disease was 0.79 (− 0.84–2.46). In this case, the RERI value is 1.78 and 0.79, which are greater than zero, indicating the presence of positive interaction between the risk factors (tumor size > 20 mm or ER-negative disease and obesity) on the outcome. However, the 95% CI for RERI includes zero. This suggests some uncertainty, and the possibility that there is actually no interaction between the two risk factors cannot be ruled out. A larger sample size may be needed
Breast cancer patients with obesity who were assigned to adjuvant chemotherapy had a higher risk of BCR compared with breast cancer patients with a healthy weight (HRadj = 2.06 [95%CI 1.08–4.31]). Patients not assigned to chemotherapy were not at a higher risk of BCR (HRadj = 1.31 [95%CI 0.79–2.17]) (Fig. 4).

The relationship between treatment characteristics and recurrence rates in breast cancer patients with healthy weight vs obesity defined by BMI. Forest plot shows adjusted HR (95% CI) of breast cancer recurrence for patients with obesity (BMI ≥ 30.0) compared with patients with healthy weight (BMI 18.5–24.9), according to stratified treatment characteristics. *BCR = breast cancer recurrence. ** The stratified analyses were adjusted for the following co-variables excluding the stratified variable of interest: age, histological grade, tumor size, nodal status, estrogen-receptor status, surgery, planned adjuvant radio-, chemo-, and endocrine therapy. ***The relative excess risk due to interaction with 95% CI for chemotherapy in patients with obesity was 1.21 (0.95–3.37) indicating a super-additive interaction effect, suggesting that the response to these exposures combined is greater than the sum of the independent responses to chemotherapy and obesity alone
Discussion
This study showed an association between obesity and inferior breast cancer outcomes. We identified several characteristics that indicate a worse prognosis among patients with obesity. Low SEP was associated with a poor breast cancer prognosis among breast cancer patients with obesity compared with patients with healthy weight. Tumor characteristics, such as histological grade III, a tumor larger than 20 mm, ductal histology, or ER-negative tumors were associated with poorer prognosis in breast cancer patients with obesity compared with patients with healthy weight. Finally, patients with obesity who were assigned to treatment with chemotherapy had a poorer prognosis compared with patients with healthy weight who were assigned chemotherapy.
BMI has been criticized as a tool for determining obesity since it does not differentiate between fat tissue and other body tissues, such as muscle tissue [24, 25]. Given ethnic and geographical variation in the relationship between fat tissue and other body tissues globally [26], it has been suggested that anthropometric measures other than BMI should be used to better predict obesity and its impact on disease [15, 27, 28]. Waist circumference more specifically indicate central obesity compared with BMI [29] and central obesity has been suggested a better predictor of inferior breast cancer outcome than peripheral obesity [30]. Body fat percentage is another anthropometric measure that has been suggested to have disease prognostic value [31]. However, in comparison to BMI and waist circumference, which can be collected using a standard weight and measurement, evaluating body fat percentage is more complex and requires a bioelectrical impedance analyzer. Few studies have investigated the relationship between body fat percentage and breast cancer outcomes [32]. ABSI has recently been suggested to better predict obesity-related mortality than BMI [33], but few studies have investigated its relationship to breast cancer prognosis. Our findings confirm previously reported mortality predictions [33]. Nevertheless, when adjusting for breast cancer prognostic factors or predicting BCR, ABSI added no value. In this study, all anthropometric measures served as prognostic tools for breast cancer outcome; as the measures were comparably associated with breast cancer outcome. However, no comparative statistical tests were used to assess the prognostic difference of the anthropometric measures.
Previous investigations studying the impact of low SEP on breast cancer outcome suggested that low SEP was associated with higher mortality [34], but not BCR indicating potential under-detection of BCR among patients with low SEP [35]. In this study, the association between obesity and poor prognosis was predominantly present among breast cancer patients with low SEP regardless of whether studying recurrence or mortality, while no association between obesity and poor prognosis was evident among patients with high SEP. Reasons underlying these findings are not clear, but may be partly explained by differences in access to healthcare and adherence to treatment and follow-up [36]. Low SEP is associated with a poorer diet, physical inactivity [37, 38], and higher comorbidity, which may contribute to a worse prognosis [39]. Yet, other explanations as to why obesity might be a mediator for social inequality in breast cancer outcomes may exist.
The observation that non-smoking patients with obesity have a poorer prognosis than smoking patients with obesity is likely to be due to misclassification and residual confounding in the association and indicates presence of the obesity paradox when stratifying analyses for smoking status [40].
The observed association between having obesity and increased risk of BCR in breast cancer patients with ER-positive disease agrees with previous research [41] and was recently highlighted by the International Association for Research on Cancer [42]. While previous research has established that obesity is associated with poorer outcomes in ER-positive breast cancer, our study suggests that this association may be even stronger in estrogen-independent breast cancer, and add novel insights to the relationship between breast cancer subtypes, obesity, and clinical outcomes. Recent research supports our findings and suggests that obesity is also a prognostic factor in hormone-independent breast cancer [43, 44].
The observed increased risk of BCR and mortality among women with obesity assigned chemotherapy treatment reflects previous studies [45, 46]. Despite existing literature supporting the safety of weight-based doses of chemotherapy regardless of weight-status [8] dose-capping in patients with obesity can occur [47, 48]. No data on chemotherapy dosing was available in this study. Therefore, we were unable to determine if patients with obesity received the optimal dose of chemotherapy. Dose-capping might thereby have contributed to our findings [7]. It is important to highlight this potentially suboptimal treatment with chemotherapy and to call on future studies to ensure optimal healthcare regardless of body composition [49].
We observed no difference in the risk of BCR in patients with obesity who were treated with endocrine therapy versus those who were not. We were unable to stratify by the type of endocrine therapy. As a result, those treated with tamoxifen may conceal any possible association between poor prognosis and obesity in breast cancer patients treated with aromatase inhibitors.
Our study has limitations. The patients’ anthropometric measures were obtained upon cohort-enrollment, not at breast cancer diagnosis. As anthropometric measures like BMI can fluctuate over time, our study results may be prone to misclassification bias [50]. Conclusions on intervention strategies for breast cancer survivors cannot be developed based on findings of this study as data on anthropometric measures were collected prior to breast cancer diagnosis. Intervention strategies to improve breast cancer prognosis are generally assigned to the time of diagnosis or during the post-diagnostic adjuvant treatment plan [51]. Similarly, information on SEP was retrieved upon enrollment in the MDCS, and may be misclassified. However, this is unlikely as participants in the MDCS were at least 40 years old at inclusion, and the yearly rate of workplace change for Swedish women over 40 is 5% [52]. Some studies have linked dietary [53] and physical activity [54] habits to the prognosis of breast cancer. We do not account for these possible confounders in our models, which should be considered when interpreting the results of this study. Further, our study is limited by small sample size and the findings; therefore, need to be validated in larger cohorts. Finally, the adjustment for co-variates in multivariable models attenuated the associations between some anthropometric measures and outcomes; therefore, our study might be prone to residual confounding.
With an ongoing obesity epidemic worldwide, having overweight or obesity will become more common than having healthy weight [55], it is therefore pertinent to identify populations of breast cancer patients with overweight or obesity who have a poor prognosis. Such information could be used to optimize treatment for all breast cancer patients, regardless of body composition. This study has highlighted several patient populations with obesity who may have a higher treatment demand than others when diagnosed with breast cancer. Yet, the associations observed in this study needs to be confirmed in larger cohorts with more up-to-date data.
Conclusion
Obesity defined by high pre-diagnostic levels of BMI, waist circumference and body fat percentage were associated with an increased risk of recurrence and mortality among breast cancer patients. In this study, breast cancer patients with obesity and low SEP, a large breast tumor, breast cancer of high histological grade, ER-negative breast cancer, and/or patients intended to be treated with chemotherapy were at higher risk of BCR and mortality compared to similar patients with healthy weight. The identification of these vulnerable patient groups among breast cancer patients with obesity may help guide researchers to patient populations in need of improved screening and/or treatment interventions.
Availability of data and materials
The data that support the findings of this study are available to appropriate academic parties upon reasonable request to the Malmö Preventative Project/Malmö Diet and Cancer Study/ Malmö Offspring Study steering committee (please see https://www.malmo-kohorter.lu.se/malmo-cohorts).
Abbreviations
- BCR:
-
Breast cancer recurrence
- BMI:
-
Body mass index
- ABSI:
-
A Body Shape Index
- SEP:
-
Socioeconomic position
- MDCS:
-
Malmö Diet and Cancer Study
- ER:
-
Estrogen receptor
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- IQR:
-
Interquartile range
References
Hortobagyi GN. Breast cancer: 45 years of research and progress. J Clin Oncol. 2020;38(21):2454–62.
Giaquinto AN, Sung H, Miller KD, Kramer JL, Newman LA, Minihan A, et al. Breast cancer statistics, 2022. CA Cancer J Clin. [Cited 2022 Oct 23];n/a(n/a). Available from: https://onlinelibrary.wiley.com/doi/abs/10.3322/caac.21754.
Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. The Lancet. 2017;390(10113):2627–42.
Lyon: International Agency for Research on Cancer. Cancer attributable to obesity [online database]. [Cited 2022 Jun 21]. Available from: http://gco.iarc.fr/obesity/home.
Liu L, Segura A, Hagemann AR. Obesity education strategies for cancer prevention in women’s health. Curr Obstet Gynecol Rep. 2015;4(4):249–58.
Goodwin PJ, Segal RJ, Vallis M, Ligibel JA, Pond GR, Robidoux A, et al. The LISA randomized trial of a weight loss intervention in postmenopausal breast cancer. Npj Breast Cancer. 2020;6(1):1–7.
Slawinski CGV, Barriuso J, Guo H, Renehan AG. Obesity and cancer treatment outcomes: interpreting the complex evidence. Clin Oncol. 2020;32(9):591–608.
Silvestris N, Argentiero A, Natalicchio A, D’Oronzo S, Beretta GD, Acquati S, et al. Antineoplastic dosing in overweight and obese cancer patients: an Associazione Italiana Oncologia Medica (AIOM)/Associazione Medici Diabetologi (AMD)/Società Italiana Endocrinologia (SIE)/Società Italiana Farmacologia (SIF) multidisciplinary consensus position paper. ESMO Open. 2021;6(3): 100153.
Redlarski G, Palkowski A, Krawczuk M. Body surface area formulae: an alarming ambiguity. Sci Rep. 2016;6:27966–27966.
Winer EP, Hudis C, Burstein HJ, Wolff AC, Pritchard KI, Ingle JN, et al. American Society of Clinical Oncology Technology Assessment on the Use of Aromatase Inhibitors As Adjuvant Therapy for Postmenopausal Women With Hormone Receptor-Positive Breast Cancer: Status Report 2004. J Clin Oncol. 2005;23(3):619–29.
Pfeiler G, Königsberg R, Hadji P, Fitzal F, Maroske M, Dressel-Ban G, et al. Impact of body mass index on estradiol depletion by aromatase inhibitors in postmenopausal women with early breast cancer. Br J Cancer. 2013;109(6):1522–7.
Lengyel E, Makowski L, DiGiovanni J, Kolonin MG. Cancer as a matter of fat: The crosstalk between adipose tissue and tumors. Trends Cancer. 2018;4(5):374–84.
Rosendahl AH, Bergqvist M, Lettiero B, Kimbung S, Borgquist S. Adipocytes and Obesity-Related Conditions Jointly Promote Breast Cancer Cell Growth and Motility: Associations With CAP1 for Prognosis. Front Endocrinol. 2018;9. Cited 2023 Apr 27. Available from: https://www.frontiersin.org/articles/10.3389/fendo.2018.00689.
Bergqvist M, Elebro K, Borgquist S, Rosendahl AH. Adipocytes Under Obese-Like Conditions Change Cell Cycle Distribution and Phosphorylation Profiles of Breast Cancer Cells: The Adipokine Receptor CAP1 Matters. Front Oncol. 2021;11. Cited 2023 Apr 27. Available from: https://www.frontiersin.org/articles/10.3389/fonc.2021.628653.
Sommer I, Teufer B, Szelag M, Nussbaumer-Streit B, Titscher V, Klerings I, et al. The performance of anthropometric tools to determine obesity: a systematic review and meta-analysis. Sci Rep. 2020;10(1):12699.
Manjer J, Carlsson S, Elmståhl S, Gullberg B, Janzon L, Lindström M, et al. The Malmö Diet and Cancer Study: representativity, cancer incidence and mortality in participants and non-participants. Eur J Cancer Prev Off J Eur Cancer Prev Organ ECP. 2001;10(6):489–99.
Berglund G, Elmståhl S, Janzon L, Larsson SA. Design and feasibility. J Intern Med. 1993;233(1):45–51.
Report of a WHO expert committee. Physical status : the use of and interpretation of anthropometry. 1995 Feb. Cited 2022 Oct 13. Report No.: 854. Available from: https://www.who.int/publications-detail-redirect/9241208546.
Krakauer NY, Krakauer JC. A new body shape index predicts mortality hazard independently of body mass index. PLoS One. 2012;7(7):20.
Statistics Sweden. MIS 1982:4. Socio-economic classification. MIS 1982:4 Socio-economic classification. 2007 Sep 18; Cited 2022 Aug 24. Available from: https://www.scb.se/en/finding-statistics/statistics-by-subject-area/other/other/other-publications-non-statistical/pong/publications/mis-19824.-socio-economic-classification/.
Cong L, Liu Q, Zhang R, Cui M, Zhang X, Gao X, et al. Tumor size classification of the 8th edition of TNM staging system is superior to that of the 7th edition in predicting the survival outcome of pancreatic cancer patients after radical resection and adjuvant chemotherapy. Sci Rep. 2018;8:10383.
Bloom HJG, Richardson WW. Histological grading and prognosis in breast cancer. Br J Cancer. 1957;11(3):359–77.
VanderWeele TJ, Knol MJ. A Tutorial on Interaction. Epidemiol Methods. 2014;3(1):33–72.
Cornier MA, Després JP, Davis N, Grossniklaus DA, Klein S, Lamarche B, et al. Assessing Adiposity. Circulation. 2011;124(18):1996–2019.
Garvey WT, Mechanick JI. Proposal for a scientifically correct and medically actionable disease classification system (ICD) for Obesity. Obesity. 2020;28(3):484–92.
Rush EC, Goedecke JH, Jennings C, Micklesfield L, Dugas L, Lambert EV, et al. BMI, fat and muscle differences in urban women of five ethnicities from two countries. Int J Obes. 2007;31(8):1232–9.
van Dijk SB, Takken T, Prinsen EC, Wittink H. Different anthropometric adiposity measures and their association with cardiovascular disease risk factors: a meta-analysis. Neth Heart J. 2012;20(5):208.
Bandera EV, Fay SH, Giovannucci E, Leitzmann MF, Marklew R, McTiernan A, et al. The use and interpretation of anthropometric measures in cancer epidemiology: a perspective from the world cancer research fund international continuous update project. Int J Cancer. 2016;139(11):2391–7.
Chan DSM, Vieira R, Abar L, Aune D, Balducci K, Cariolou M, et al. Postdiagnosis body fatness, weight change and breast cancer prognosis: Global Cancer Update Program (CUP global) systematic literature review and meta-analysis. Int J Cancer;n/a(n/a). Cited 2022 Nov 14. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/ijc.34322.
Bandera EV, Qin B, Lin Y, et al. Association of Body Mass Index, Central Obesity, and Body Composition With Mortality Among Black Breast Cancer Survivors. JAMA Oncol. 2021;7(8):1186–95. https://doi.org/10.1001/jamaoncol.2021.1499.
Bergqvist M, Elebro K, Sandsveden M, Borgquist S, Rosendahl AH. Effects of tumor-specific CAP1 expression and body constitution on clinical outcomes in patients with early breast cancer. Breast Cancer Res BCR. 2020;22:67.
Liu LN, Lin YC, Miaskowski C, Chen SC, Chen ML. Association between changes in body fat and disease progression after breast cancer surgery is moderated by menopausal status. BMC Cancer. 2017;17(1):863.
Christakoudi S, Tsilidis KK, Muller DC, Freisling H, Weiderpass E, Overvad K, et al. A Body Shape Index (ABSI) achieves better mortality risk stratification than alternative indices of abdominal obesity: results from a large European cohort. Sci Rep. 2020;10(1):14541.
Vaccarella S, Georges D, Bray F, Ginsburg O, Charvat H, Martikainen P, et al. Socioeconomic inequalities in cancer mortality between and within countries in Europe: a population-based study. Lancet Reg Health - Eur. 2022;28: 100551.
Hjorth CF, Damkier P, Ejlertsen B, Lash T, Sørensen HT, Cronin-Fenton D. Socioeconomic position and prognosis in premenopausal breast cancer: a population-based cohort study in Denmark. BMC Med. 2021;19(1):235.
Orsini M, Trétarre B, Daurès JP, Bessaoud F. Individual socioeconomic status and breast cancer diagnostic stages: a French case–control study. Eur J Public Health. 2016;26(3):445–50.
Alkerwi A, Vernier C, Sauvageot N, Crichton GE, Elias MF. Demographic and socioeconomic disparity in nutrition: application of a novel Correlated Component Regression approach. BMJ Open. 2015;5(5): e006814.
Armstrong S, Wong CA, Perrin E, Page S, Sibley L, Skinner A. Association of physical activity with income, race/ethnicity, and sex among adolescents and young adults in the United States: findings from the National Health and Nutrition Examination Survey, 2007–2016. JAMA Pediatr. 2018;172(8):732–40.
Chlebowski RT, Aragaki AK, Anderson GL, Thomson CA, Manson JE, Simon MS, et al. Low-fat dietary pattern and breast cancer mortality in the women’s health initiative randomized controlled trial. J Clin Oncol. 2017;35(25):2919–26.
Banack HR, Stokes A. The ‘obesity paradox’ may not be a paradox at all. Int J Obes. 2017;41(8):1162–3.
Chan DSM, Vieira AR, Aune D, Bandera EV, Greenwood DC, McTiernan A, et al. Body mass index and survival in women with breast cancer-systematic literature review and meta-analysis of 82 follow-up studies. Ann Oncol Off J Eur Soc Med Oncol. 2014;25(10):1901–14.
Lauby-Secretan B, Scoccianti C, Loomis D, Grosse Y, Bianchini F, Straif K. Body Fatness and Cancer — Viewpoint of the IARC Working Group. https://doi.org/10.1056/NEJMsr1606602. Massachusetts Medical Society; 2016. Cited 2022 Feb 3. Available from: https://www.nejm.org/doi/10.1056/NEJMsr1606602.
Harborg S, Zachariae R, Olsen J, Johannsen M, Cronin-Fenton D, Bøggild H, et al. Overweight and prognosis in triple-negative breast cancer patients: a systematic review and meta-analysis. NPJ Breast Cancer. 2021;7(1):1–9.
Lohmann AE, Soldera SV, Pimentel I, Ribnikar D, Ennis M, Amir E, et al. Association of obesity with breast cancer outcome in relation to cancer subtypes: a meta-analysis. JNCI J Natl Cancer Inst. 2021 ;(djab023). Cited 2021 Apr 28. Available from: https://doi.org/10.1093/jnci/djab023.
Ewertz M, Jensen MB, Gunnarsdóttir KÁ, Højris I, Jakobsen EH, Nielsen D, et al. Effect of obesity on prognosis after early-stage breast cancer. J Clin Oncol Off J Am Soc Clin Oncol. 2011;29(1):25–31.
de Azambuja E, McCaskill-Stevens W, Francis P, Quinaux E, Crown JPA, Vicente M, et al. The effect of body mass index on overall and disease-free survival in node-positive breast cancer patients treated with docetaxel and doxorubicin-containing adjuvant chemotherapy: the experience of the BIG 02–98 trial. Breast Cancer Res Treat. 2010;119(1):145–53.
Griggs JJ, Sorbero MES, Lyman GH. Undertreatment of obese women receiving breast cancer chemotherapy. Arch Intern Med. 2005;165(11):1267–73.
Griggs JJ, Culakova E, Sorbero MES, van Ryn M, Poniewierski MS, Wolff DA, et al. Effect of patient socioeconomic status and body mass index on the quality of breast cancer adjuvant chemotherapy. J Clin Oncol. 2007;25(3):277–84.
Bouleftour W, Mery B, Chanal E, Rowinski E, Viard A, Forges F, et al. Obesity and chemotherapy administration: between empiric and mathematic method review. Acta Oncol. 2019;58(6):880–7.
BMI and Lifetime Changes in BMI and Cancer Mortality Risk - PMC. Cited 2023 Apr 27. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4399977/.
Iyengar NM. Inclusion of exercise in cancer treatment planning: when is the right time? JACC CardioOncol. 2022;4(4):504–6.
Fredrik W. Andersson Jan Andersson Andreas Poldahl. Sannolikheten att byta jobb - Den kommunala jobb balansens betydelse. Sannolikheten att byta jobb. Cited 2022 Aug 26. Available from: https://www.scb.se/contentassets/b1ae4493ffd1404987a4d32cbf213ae5/sannolikheten-att-bytajobb.pdf.
Wang T, Farvid MS, Kang JH, Holmes MD, Rosner BA, Tamimi RM, et al. Diabetes risk reduction diet and survival after breast cancer diagnosis. Cancer Res. 2021;81(15):4155–62.
Fortner RT, Brantley KD, Tworoger SS, Tamimi RM, Rosner B, Farvid MS, et al. Physical activity and breast cancer survival: results from the Nurses’ Health Studies. JNCI Cancer Spectr. 2023;7(1):pkac085.
Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity | NEJM. Cited 2022 Sep 1. Available from: https://www.nejm.org/doi/full/10.1056/NEJMsa1909301.
Acknowledgements
We acknowledge the support from Lund University Infrastructure grant “Malmö Population-based 1 cohorts” (STYR 2019/2046). We acknowledge the assistance from Statistics Sweden (Statistiska Centralbyrån, SCB) for retrieving the death and/or emigration dates. We acknowledge the Obesity and Cancer Research network Denmark for initiating this collaboration (www.obecare.dk).
Role of the funder
The funders did not play a role in the design of the study; the collection, analysis and interpretation of the data; the writing of the manuscript; and the decision to submit the manuscript for publication.
Prior presentations
Presented in part at the Nordic Obesity Meeting, 17-19 November 2022, Copenhagen, Denmark and the San Antonio Breast Cancer Symposium, 6-10 December 2022, San Antonio, Texas, USA.
Code availability
The code developed during this study is available upon reasonable request. Analyses were performed using Stata®, version 17 (StataCorp, College Station, TX, USA).
Funding
This work was supported by Aarhus University (to SH); Danish Cancer Research Foundation (DKF-2021–81-738 to SH); Danish Cancer Society (R349-A19981 to SH and R328-A19070 to DCF); Danish Comprehensive Cancer Center (project no. 7 and 14 to SB); Governmental Funding of Clinical Research within the National Health Service–ALF (to AHR); Swedish Cancer Society (to SB); Swedish Breast Cancer Association (to AHR); Dir A Påhlsson Foundation (to AHR); and Mrs. Berta Kamprad Foundation (to AHR and MK).
Author information
Authors and Affiliations
Contributions
Study concept and design (SH, AHR, SB), statistical analyses (SH), provision of study material (SB, MF, AHR), collection and assembly of data (SH, MF), interpretation of data (SH, MF, DCF, MK, SD, AHR, SB), manuscript preparation (SH, SB), manuscript editing (SH), and manuscript review (MF, DCF, MK, SD, AHR, SB). All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical permission was obtained from the Ethical Committee at Lund University (D652/2005 and complement 501/2006 and 23/2007). Informed consent was obtained from all participants. The study was performed in accordance with relevant guidelines and regulations.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary Table S1. A body shape index in relation to breast cancer recurrence and mortality.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Harborg, S., Feldt, M., Cronin-Fenton, D. et al. Obesity and breast cancer prognosis: pre-diagnostic anthropometric measures in relation to patient, tumor, and treatment characteristics. Cancer Metab 11, 8 (2023). https://doi.org/10.1186/s40170-023-00308-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40170-023-00308-0