
Abstract
Background
Antenatal care (ANC) is the care given to pregnant women to prevent poor feto-maternal outcomes during pregnancy. The World Health Organization recommends first ANC visit be started as early as possible within in 12 weeks of gestation. Although there is improvement in overall ANC coverage, a sizable proportion of pregnant women in Ethiopia delay the time to initiate their first ANC visit. Therefore, this study aimed to investigate factors associated with late ANC initiation among pregnant women attending public health centers in Addis Ababa, Ethiopia.
Methods
A facility-based cross-sectional study was conducted among 407 randomly selected pregnant women who attended ANC at selected public health centers in Addis Ababa from December 2020 to January 2021. Data were collected using pretested and structured questionnaires through a face-to-face interview and reviewing medical records. Binary and multivariable logistic regressions were fitted sequentially to identify predictors for late ANC initiation. Adjusted odds ratios with 95% CI were computed to measure the strength of associations and statistical significance was declared at a p-value < 0.05.
Result
This study showed that 47% of pregnant women started their first ANC visit late.The age of 30 years and above, being married, unplanned pregnancy, having a wrong perception about the timing of the first ANC visit, and not having ANC for previous pregnancy was significantly associated with late ANC initiation.
Conclusion
Nearly half of the women initiated their first ANC visit late. Tailored interventions aimed at promoting early ANC initiation should target married women, women with an unplanned pregnancy, women who perceived the wrong timing of their first ANC, and those who have no ANC for their previous pregnancy.
Similar content being viewed by others

Background
Antenatal care (ANC) is care given by trained health-care providers to pregnant women for the well-being of the mother and the fetus during pregnancy. The World Health Organization (WHO) recommends that ANC should be initiated within 12 weeks of gestation and considers “late initiation” when it is commenced after 12 weeks of gestation [1].
In 2017, nearly 295 000 mothers died from pregnancy and childbirth-related complications, which could be translated to 810 maternal deaths every day. The vast majority of these deaths (94%) occurred in low-income countries, of which Sub-Saharan Africa contributed to approximately 66% of deaths [2, 3]. Ethiopia is one of the Sub-Saharan African countries that contribute to this unacceptable high number of maternal deaths in the region with a maternal mortality ratio (MMR) of 412/per 100,000 live births [4].
Between 2000 and 2017, the maternal mortality rate was reduced only by 38% worldwide. Although reducing maternal deaths has remained a global priority, the progress towards the global target of reducing maternal mortality ratio (MMR) to 70 per 100,000 livebirths or less by 2030 is very slow, indicating the need for early risk identifications and management of pregnancy-related complications during ANC follow up [2, 3].
In 2016, the WHO approved a new ANC model with increased numbers of contacts from four visits to eight contacts, intending to reduce prenatal mortality and improve pregnancy outcomes. Recent evidence shows that eight or more ANC contacts can decrease perinatal deaths by 8 per 1000 births in comparison to four visits [5, 6].
In addition to the number of ANC contacts, the timing of its initiation is also an important factor for feto-maternal outcomes. Timely initiation of ANC visits serves as a gateway for risk identification and early diagnosis of pregnancy-related complications to improve pregnancy outcomes [7, 8]. For example, studies showed that regular antenatal care from a skilled provider reduces maternal mortality by 20% [9]. On the contrary, delaying ANC visits or lack of ANC follow-up is associated with adverse feto-maternal outcomes such as premature birth, low birth weight, stillbirth, and increased risk of maternal complications during pregnancy, childbirth, and the puerperium [9,10,11,12].
Evidence indicated that globally 43% of pregnant women initiate their first ANC visit timely, although there is a huge discrepancy between developed and developing regions [13]. For example, compared to the developed region, where 85% of pregnant women start their ANC follow-up in the first trimester, only 45% of pregnant women start the follow-up in the first trimester in developing regions, and this stands at 25% for Sub-Saharan Africa [14].
In Ethiopia, according to the Ethiopian Demography and Health Survey report (EDHS, 2016), 62% of the women had at least one ANC visit and only 20% of women had their first antenatal care visit during the first trimester [4].
The Ethiopian government, in its Health Sector Transformation Plan (2015/16–2019/20), set a goal to achieve 95% ANC utilization of at least 4 visits and adopted the WHO-focused ANC model in combination with the eight contacts to alleviate the problems related with late ANC initiation [15]. Yet, despite the efforts made by the government to achieve high coverage of ANC visits, the proportion of pregnant women starting their first ANC follow-up within the first trimester has remained low.
It has been reported that factors such as lack of education, distance from a health facility, low income, unplanned pregnancy, and previous obstetrics history are associated with the late initiation of ANC [16,17,18]. Furthermore, the coverage of ANC follow-up or its early initiation might be associated with some unmeasured factors. Investigating factors associated with late ANC initiation comprehensively in the such setting would be important for a program design and interventions. This study, therefore, aimed to investigate factors associated with late ANC initiation among pregnant women attending public health centers in Addis Ababa, Ethiopia.
Methods and materials
Study area and period
The study was conducted in Addis Ababa, the capital city of Ethiopia. There are eleven sub-cities in Addis Ababa, with over five million total population as of 2021. According to Federal Ministry of Health, there are 10 general Hospitals, two specialized hospitals, 36 private hospitals, 700 clinics and 35 non-governmental organizations and about 96 government health centers offering services to the dwellers of the city and the surrounding community [19]. This study was conducted from December 2020 to January 2021.
Study design and population
A facility-based cross-sectional study was conducted among pregnant women who came to attend their first ANC visit at selected public health centers during the study period. Pregnant women who came at below eight weeks of gestation and who were mentally ill were excluded from the study.
Sample size determination and sampling technique
The sample size was estimated using a single population proportion formula, with the assumption of proportion (P = 59.8%) [20], 95% Confidence interval, and 5% margin of error.
n = (1.96)2 × 0.598 (1−0.598)/ (0.05)2.
n = 3.8416 × 0.596 × 0.404/0.0025, n = 369.9 ~ 370.
Considering 10% non-response rate, the final sample size was 407.
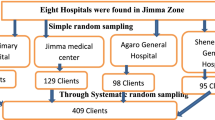
A simple random sampling technique was used to select eleven health centers, that is, one health center from each sub-city. For each selected health center, the average number of pregnant women was obtained from the ANC registration book. The total sample size was proportionally allocated to each health center based on the average number of pregnant women attending the ANC clinic. Then systematic random sampling was employed to select the study participants from each health center. During the study period, a total of 1016 pregnant women visited the selected health centers for ANC follow. The interval (Kth) for the systematic random sampling method was obtained dividing the number of pregnant women by the sample size which yielded three (1016/407 = 3). The first study participant was selected using lottery method and then every 3rd pregnant woman were enrolled to the study.
Data collection procedure and instrument
The data were collected through face-to-face interview using structured questionnaire adapted from existing literatures [16, 21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36]. The questionnaire contains questions on socio-demographic characteristics, obstetric factors, health service-related factors, and knowledge and attitude towards ANC (Additional file 1). Two days of training on the data collection tools and procedures was given for data collectors and supervisors. The questionnaire was pretested on 5% of the sample size, out of the selected health centers, and necessary adjustments were made before using it for the actual data collection. The validity of the questionnaire was assessed using face validity/content validity and the inter-rater reliability test was performed to check the reliability. The data were collected by five diploma holder nurses and supervised by two bachelor of science nurses who were working out of the selected study facilities. Gestational age was estimated by asking the women their last normal menstrual period (LNMP), and further medical records of the women were reviewed to obtain some information including obstetric history, gestational age estimation either from ultrasound reports or manual fundal height measurement if the women were unable to recall their LNMP.
Data processing and analysis
Data were checked for completeness and consistency. The cleaned data were coded and entered to Epi Info and analyzed using SPSS version 22. Descriptive statistics were computed to present the results of independent variables. The outcome variable was dichotomized as early versus late ANC initiation. A woman was considered to have early initiation of ANC if she commenced first ANC visit within the first trimester at or between eight and 12 weeks of pregnancy and considered to have a late ANC visit, otherwise [28].
A binary logistic regression models were used to assess the association between independent and outcome variables (late ANC initiation). The variables with P-value < 0.25 in a bivariate analysis were included in multivariable analysis to control for confounding effect. Hosmer and Lemeshow goodness‑of‑fit test was done to assess the fitness of the model during multivariable analysis. Adjusted odds ratios (AOR) with 95% CI were used to measure the strength of association between independent variables and outcome variable and level of significance was set at P value less than 0.05.
Results
Socio-demographic characteristics of the respondents
Out of 407 pregnant women, 401 included in this study, giving the response rate of 98.5%. The mean age of respondents was (28 ± 5 SD) years. Three hundred thirty-six (84%) of the respondents were married and 154 (38.4%) attended secondary school and above level.
A half of the respondents who delayed the timing of first ANC initiation were in the age group of 30 years and above (Table 1).
Obstetrics history of the respondents
Of the total respondents, 268 (66.8%) reported to have 1–2 parity. About one fifths of respondents reported to have experienced abortion and 20 (5%) reported to encounter child death (Table 2).
History of current pregnancy and timing of first ANC visit
Of 401 respondents, 188 (46.9%) started their first ANC late. One hundred sixty-one (40.2%) respondents confirmed their current pregnancy when menstruation period was late for two months and 119 (29.8%) confirmed their pregnancy by urine test offered by a health care provider. Among respondents, 339 (85%) reported that their current pregnancy was planned and 60 (15%) reported that the pregnancy was unplanned (Table 3).
Perception of the respondents on ANC services utilization
Three hundred fourteen (78.3%) of the respondents perceived that ANC is highly important to the health of mother and about 72% perceived that ANC is highly important for the fetus. Regarding the correct time of ANC booking, 242 (62.7%) of the women perceived that ANC should be initiated within or before 12 weeks of gestation and 144 (37.3%) perceived that ANC should begin after 12 weeks of gestation. Most of respondents, 249 (62%), had previous ANC follow up (Table 4).
Factors associated with late initiation of ANC
In a bivariate analysis, maternal age, marital status, educational status, occupation, transportation cost for ANC, pregnancy intention, perceived timing of ANC initiation, and previous history of ANC follow up were found to be associated with late initiation of ANC. However, in a multivariable logistic regression, maternal age, marital status, unplanned pregnancy, perceived timing of first ANC visit, and previous ANC follow up were found to be significantly associated with late initiation of ANC after adjusting for confounders.
The odds of late ANC initiation were 25% lower among women with the age of 30 and above compared to other age groups (AOR = 0.25, 95% CI 0.06, 0.83). The odds of late first ANC visit were 2.8 times higher among married women than single women (AOR = 2.81, 95% CI 1.29, 6.09).
Pregnant women with an unplanned pregnancy were 2.17 times more likely to start their ANC late compared to those women with planned pregnancies (AOR = 2.17, 95% CI 1.4, 4.67).
Pregnant women who perceived that the correct time of ANC booking was after 12 weeks of gestation were 8.58 times more likely to delay the ANC initiation compared to those who perceived that correct time of ANC booking was before 12 weeks of gestation (AOR = 8.58, 95% CI 5.75,14.80). Pregnant women who had no ANC for previous pregnancy were 5.45 times more likely to start their ANC lately compared to those who had ANC for previous pregnancy (AOR = 5.45, 95% CI 3.02, 9.83) (Table 5).
Discussion
Antenatal Care (ANC) is crucial for reducing maternal morbidity and mortality through early detection and treatment of pregnancy-related complications. The first ANC visit should be initiated as early as the pregnancy was confirmed or within 12 weeks of gestation. In our study, 46.9% of respondents booked their first ANC visit lately. This finding is consistent with other studies conducted in Addis Ababa (42.0%) [25], Jimma 48% [16], and Cameroon (44%) [29].
This study finding is higher compared to a study done in Debre Markos (33.4%) [23]. This variation could be due to the classification of the outcome. Because the study in Debre Markos classified mothers as late for booking ANC if they came after 16 weeks of gestation. In our study, however, late ANC has been considered if a pregnant woman started ANC follow-up after 12 weeks of gestation.
Yet, the prevalence of late ANC initiation in our study is lower than studies conducted in Tanzania (70.4%) [30], Zambia (72%) [31], and studies conducted in other parts of Ethiopia such as Ilu Ababor (71.2%) [27] and Tigray (85%) [24]. This improvement might be attributed to the current national emphasis given to the focused ANC, and the massive work done to improve maternal health outcomes in the country. Further, the sociocultural differences among the study populations might also contribute to the variation observed between our findings and the findings reported in previous studies.
In this study, pregnant women aged 30 years and above had lower odds of a late first ANC visit than other age groups. This might be because early pregnancy awareness is increased with maternal age. This finding is supported by the results of studies conducted in Ghana and other sub-Saharan African countries [32, 33].
This study revealed that the odds of a late first ANC visit were 2.8 times higher among married women as compared to those with a single marital status. The possible reason could be married women may feel more confident of their previous ANC experience, and familial or partner support, and may perceive that starting ANC follow-up lately may not impact their health and the health of their fetus. This is also supported by other study findings [16, 34, 35].
Pregnant women with an unplanned pregnancy were 2.17 times more likely to start their ANC late compared to those women with planned pregnancies. This might be because those women with an unplanned pregnancy may lack a support from their partners or families and become less motivated to seek ANC early compared to women with planned pregnancies. This finding is consistent with other previous studies reports [16, 18, 23, 36].
This study showed that the likelihoods of late ANC initiation were 8.58 times higher among women who perceived that the correct time of ANC initiation is after 12 weeks of gestation as compared to those who perceived that the correct time of ANC initiation is before 12 weeks of gestation. This finding is in line with the findings reported in studies conducted in Debre-Markos [23], Ilu Ababor [27], Addis Ababa [25], and southern Ethiopia [37].
This study indicated that previous ANC service is a strong predictor of late ANC initiation. The odds of late ANC booking were 5.45 times higher among women who had no ANC for previous pregnancy than those who had ANC for previous pregnancy. This might be related to the counseling and health education received on the importance of early initiation of ANC in the previous pregnancy. This finding is backed by the findings reported in studies conducted in different parts of Ethiopia [23, 27, 37].
Limitation of the study
This study considered only pregnant women attending ANC at the governmental health institutions. However, other pregnant women who visit private clinics, hospitals and NGOs which focus on maternity care were not included in this study. Furthermore, since the study was cross sectional, it was not possible to establish the temporal relationship of variables.
Conclusion
Almost half of the pregnant women booked their first ANC visit lately. Maternal age, marital status, pregnancy intention, perceived timing of ANC initiation and previous ANC service were identified predictors of late ANC initiation. All stakeholders should work more on awareness creation and addressing misperception, aiming to promote early ANC initiation among women who perceived wrong timing of first ANC, married women, women with unplanned pregnancy, and those who have no ANC for their previous pregnancy.
Data availability
All related data are presented fully within the paper. Additional data are available from the corresponding author on reasonable request.
Abbreviations
- ANC:
-
Antenatal care
- AOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- EDHS:
-
Ethiopian demographic and health survey
- ETB:
-
Ethiopian birr
- NGOs:
-
Non-governmental organizations
- WHO:
-
World health organization
References
World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience. World Health Organization; 2016.
World Health Organization. Maternal mortality: evidence brief. World Health Organization; 2019.
UNICEF, UNFPA. Trends in maternal mortality 2000 to 2017: estimates by WHO. World bank group and the United Nations population division; 2019.
Central Statistical Agency(CSA). ICF. Ethiopia demographic and health survey 2016: key indicators report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA. CSA and ICF. 2016.
World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience: summary: highlights and key messages from the World Health Organization’s 2016 global recommendations for routine antenatal care. World Health Organization; 2018.
World Health Organization. New guidelines on antenatal care for a positive pregnancy experience, 2016.
Alkema L, Chou D, Hogan D, Zhang S, Moller A-B, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN maternal mortality estimation inter-agency group. The lancet. 2016;387(10017):462–74.
Atuhaire R, Atuhaire LK, Wamala R, Nansubuga E. Interrelationships between early antenatal care, health facility delivery and early postnatal care among women in Uganda: a structural equation analysis. Global Health Action. 2020;13(1):1830463.
Woldeamanuel BT, Belachew TA. Timing of first antenatal care visits and number of items of antenatal care contents received and associated factors in Ethiopia: multilevel mixed effects analysis. Reproductive Health. 2021;18(1):1-6.7.
Beauclair R, Petro G, Myer L. The association between timing of initiation of antenatal care and stillbirths: a retrospective cohort study of pregnant women in Cape Town, South Africa. BMC Pregnancy Childbirth. 2014;14(1):1–10.
Pervin J, Rahman SM, Rahman M, Aktar S, Rahman A. Association between antenatal care visit and preterm birth: a cohort study in rural Bangladesh. BMJ Open. 2020;10(7):e036699.
Manjavidze T, Rylander C, Skjeldestad FE, Kazakhashvili N, Anda EE. The impact of antenatal care utilization on admissions to neonatal intensive care units and perinatal mortality in Georgia. PLoS ONE. 2020;15(12):e0242991.
Arsenault C, Jordan K, Lee D, Dinsa G, Manzi F, Marchant T, et al. Equity in antenatal care quality: an analysis of 91 national household surveys. The Lancet Global Health. 2018;6(11):e1186–95.
Moller A-B, Petzold M, Chou D, Say L. Early antenatal care visit: a systematic analysis of regional and global levels and trends of coverage from 1990 to 2013. The Lancet Global Health. 2017;5(10):e977–83.
Ethiopian Federal Minstry of Health. Health Sector Transformation Plan: 2015/16-2019/20. Federal Ministry of Health Addis Ababa, Ethiopia; 2015.
Tadele F, Getachew N, Fentie K, Amdisa D. Late initiation of antenatal care and associated factors among pregnant women in Jimma Zone Public Hospitals, Southwest Ethiopia, 2020. BMC Health Serv Res. 2022;22(1):1–8.
Paudel YR, Jha T, Mehata S. Timing of first antenatal care (ANC) and inequalities in early initiation of ANC in Nepal. Front Public Health. 2017;5:242.
Ebonwu J, Mumbauer A, Uys M, Wainberg ML, Medina-Marino A. Determinants of late antenatal care presentation in rural and peri-urban communities in South Africa: a cross-sectional study. PLoS ONE. 2018;13(3):e0191903.
Ethiopian Federal Ministry of Health. FMOH report,. 2020.
Tariku A, Melkamu Y, Kebede Z. Previous utilization of service does not improve timely booking in antenatal care: cross sectional study on timing of antenatal care booking at public health facilities in Addis Ababa. Ethiopian J Health Develop. 2010. https://doi.org/10.4314/ejhd.v24i3.68390.
Wolde HF, Tsegaye AT, Sisay MM. Late initiation of antenatal care and associated factors among pregnant women in Addis Zemen primary hospital, South Gondar, Ethiopia. Reproductive Health. 2019;16(1):1–8.
Alemu Y, Aragaw A. Early initiations of first antenatal care visit and associated factor among mothers who gave birth in the last six months preceding birth in Bahir Dar Zuria Woreda North West Ethiopia. Reproductive Health. 2018;15(1):1–8.
Ewunetie AA, Munea AM, Meselu BT, Simeneh MM, Meteku BT. DELAY on first antenatal care visit and its associated factors among pregnant women in public health facilities of Debre Markos town, North West Ethiopia. BMC Pregnancy Childbirth. 2018;18(1):1–8.
Grum T, Brhane E. Magnitude and factors associated with late antenatal care booking on first visit among pregnant women in public health centers in central zone of Tigray Region, Ethiopia: a cross sectional study. PLoS ONE. 2018;13(12):e0207922.
Gulema H, Berhane Y. Timing of first antenatal care visit and its associated factors among pregnant women attending public health facilities in Addis Ababa, Ethiopia. Ethiop J Health Sci. 2017;27(2):139–46.
Kolola T, Morka W, Abdissa B. Antenatal care booking within the first trimester of pregnancy and its associated factors among pregnant women residing in an urban area: a cross-sectional study in Debre Berhan town, Ethiopia. BMJ Open. 2020;10(6):e032960.
Tola W, Negash E, Sileshi T, Wakgari N. Late initiation of antenatal care and associated factors among pregnant women attending antenatal clinic of Ilu Ababor Zone, southwest Ethiopia: a cross-sectional study. PLoS ONE. 2021;16(1):e0246230.
World Health Organization. World health statistics 2016: monitoring health for the SDGs sustainable development goals. World Health Organization; 2016.
Tolefac PN, Halle-Ekane GE, Agbor VN, Sama CB, Ngwasiri C, Tebeu PM. Why do pregnant women present late for their first antenatal care consultation in Cameroon? Maternal health. Neonatol Perinatol. 2017;3(1):1–6.
Njiku F, Wella H, Sariah A, Protas J. Prevalence and factors associated with late antenatal care visit among pregnant women in Lushoto, Tanzania. Tanzania J Hlth Res [Internet]. 2017. Available from: https://www.ajol.info/index.php/thrb/article/view/135768.
Sinyange N, Sitali L, Jacobs C, Musonda P, Michelo C. Factors associated with late antenatal care booking: population based observations from the 2007 Zambia demographic and health survey. Pan Afr Med J. 2016;25:109. https://doi.org/10.11604/pamj.2016.25.109.6873.
Manyeh AK, Amu A, Williams J, Gyapong M. Factors associated with the timing of antenatal clinic attendance among first-time mothers in rural southern Ghana. BMC Pregnancy Childbirth. 2020;20(1):1–7.
Alem AZ, Yeshaw Y, Liyew AM, Tesema GA, Alamneh TS, Worku MG, et al. Timely initiation of antenatal care and its associated factors among pregnant women in sub-saharan Africa: a multicountry analysis of demographic and health surveys. PLoS ONE. 2022;17(1):e0262411.
Hailegebreal S, Gilano G, Seboka BT, Ahmed MH, Simegn AE. Spatial distribution and associated factors of antenatal care utilization in Ethiopia in 2019: spatial and multilevel analysis. 2021.
Belay A, Astatkie T, Abebaw S, Gebreamanule B, Enbeyle W. Prevalence and factors affecting the utilization of antenatal care in rural areas of Southwestern Ethiopia. BMC Pregnancy Childbirth. 2022;22(1):1–8.
Gebremeskel F, Dibaba Y, Admassu B. Timing of first antenatal care attendance and associated factors among pregnant women in Arba Minch Town and Arba Minch District, Gamo Gofa Zone, South Ethiopia. J Environ Public Health. 2015.
Kondale M, Tumebo T, Gultie T, Megersa T, Yirga H. Timing of first antenatal care visit and associated factors among pregnant women attending anatal clinics in Halaba Kulito governmental health institutions, 2015. J Women’s Health Care. 2016;5(308):2167–0420.
Acknowledgements
We acknowledge the study participants, data collectors, supervisors, health facility administrators, and staff for their willingness to give their time and information for this study.
Funding
This study was not funded.
Author information
Authors and Affiliations
Contributions
NG conceived the study, MA and SK involved in supervision, TM and AA was involved in report writing and drafted the manuscript, TAH & KTR revised the manuscript and involved in edition. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from the institutional review board of Adama Hospital Medical College with reference number AHMC-IRB/06/2020. Informed consent was obtained from study participants, parents in case of minor study participants and legally authorized representatives in case of illiterate participants. The study was conducted in accordance with regulations and guidelines for researches involving human beings.
Consent for publication
Not applicable.
Competing interests
The authors declare that there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Data collection tool/Questionaire.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Girma, N., Abdo, M., Kalu, S. et al. Late initiation of antenatal care among pregnant women in Addis Ababa city, Ethiopia: a facility based cross-sectional study. BMC Women's Health 23, 13 (2023). https://doi.org/10.1186/s12905-022-02148-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-022-02148-4