
Abstract
Background
Children with life-threatening and life-limiting conditions can experience high levels of suffering due to multiple distressing symptoms that result in poor quality of life and increase risk of long-term distress in their family members. High quality symptom treatment is needed for all these children and their families, even more so at the end-of-life. In this paper, we provide evidence-based recommendations for symptom treatment in paediatric palliative patients to optimize care.
Methods
A multidisciplinary panel of 56 experts in paediatric palliative care and nine (bereaved) parents was established to develop recommendations on symptom treatment in paediatric palliative care including anxiety and depression, delirium, dyspnoea, haematological symptoms, coughing, skin complaints, nausea and vomiting, neurological symptoms, pain, death rattle, fatigue, paediatric palliative sedation and forgoing hydration and nutrition. Recommendations were based on evidence from a systematic literature search, additional literature sources (such as guidelines), clinical expertise, and patient and family values. We used the GRADE methodology for appraisal of evidence. Parents were included in the guideline panel to ensure the representation of patient and family values.
Results
We included a total of 18 studies that reported on the effects of specific (non) pharmacological interventions to treat symptoms in paediatric palliative care. A few of these interventions showed significant improvement in symptom relief. This evidence could only (partly) answer eight out of 27 clinical questions. We included 29 guidelines and two textbooks as additional literature to deal with lack of evidence. In total, we formulated 221 recommendations on symptom treatment in paediatric palliative care based on evidence, additional literature, clinical expertise, and patient and family values.
Conclusion
Even though available evidence on symptom-related paediatric palliative care interventions has increased, there still is a paucity of evidence in paediatric palliative care. We urge for international multidisciplinary multi-institutional collaboration to perform high-quality research and contribute to the optimization of symptom relief in palliative care for all children worldwide.
Similar content being viewed by others

Background
Worldwide, there are approximately 21 million children with conditions that can benefit from a palliative care approach [1]. Of these children, more than eight million need specialized paediatric palliative care [1, 2]. In the Netherlands, it is estimated that 7000 children, adolescents and young adults aged 0 to 20 years are living with life-threatening or life-limiting conditions and need palliative care [3]. Approximately, 23% of these children are diagnosed with oncological conditions and 77% have complex chronic conditions such as neonatal, neurological, or metabolic disorders [4, 5]. Annually, 1000 children die due to the consequences of these conditions [5]. All these children and their families require paediatric palliative care that focuses on improving quality of life and alleviating physical, psychological, social, and spiritual suffering [6].
As all children with life-threatening or life-limiting conditions can experience multiple distressing symptoms, high quality symptom treatment is an essential component of paediatric palliative care [2]. Previous international studies have reported high levels of suffering in children with cancer, complex chronic conditions, and advanced heart disease due to symptoms such as pain, dyspnoea, and fatigue [7,8,9,10]. Parents reported that these symptoms, which are often amenable to treatment, are insufficiently controlled [9, 10]. High levels of suffering due to symptoms decrease health-related quality of life in children and adolescents with life-threatening or life-limiting conditions [11, 12]. Poor quality of life affects not only the child but the whole family including parents and siblings [8, 13]. It also increases the risk of long-term distress in surviving family members [14]. Clearly, there is room for improvement in easing distress due to symptoms in these children. This is even more evident at the end of life, when suffering tends to worsen and attempts to control symptoms with traditional symptom-directed interventions are more likely to be unsuccessful [10, 15].
High quality symptom treatment should be ensured for all children with life-threatening or life-limiting conditions and their families. Clinical Practice Guidelines (CPGs) are powerful instruments that can facilitate consistent, efficient, and high-quality care by translating evidence into recommendations for clinical practice [16,17,18]. As a result, CPGs can contribute to the integration of high-quality palliative care into daily practice.
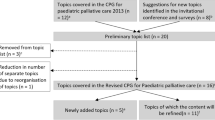
In 2013, the first Dutch CPG for Paediatric Palliative Care was published and provided the first recommendations on symptom treatment [19, 20]. Almost a decade after the development of the first Dutch CPG for paediatric palliative care, stakeholders expressed the need for an update and expansion of the CPG. Most importantly, health care providers and parents requested guidance on symptom treatment including treatment of refractory symptoms at the end-of life. Additionally, recommendations needed to be updated with evidence from new scientific literature. As a result, the first Dutch CPG for Paediatric Palliative care is revised and updated with recommendations on topics that were not covered in the first CPG [21].
The revised CPG provides recommendations on symptom treatment, advance care planning, shared decision-making, organisation of care, psychosocial care, and loss and bereavement care [21]. In this paper, we present the recommendations on symptom treatment and give an overview of the most recent evidence that was used to base recommendations upon. The recommendations on advance care planning, shared decision-making, and organisation of care; and psychosocial care and loss and bereavement care will be presented in two subsequent papers.
Methods
The full methodology of the Dutch CPG for paediatric palliative care has been published in a separate paper [22].
Scope
This guideline provides guidance on palliative care for all children aged 0 to 18 years with life- threatening or life-limiting conditions, their caregivers, and siblings (hereafter referred to as families) throughout the entire palliative trajectory (from palliative diagnosis till after end-of-life), with the ultimate goal to improve quality of palliative care and thereby quality of life of children and their families [6]. In this paper we provide recommendations for symptom treatment.
Multidisciplinary guideline development panel
The guideline development panel consisted of an expert panel of 56 professionals with expertise in paediatric palliative care and a panel of nine (bereaved) parents (Appendix A). Professionals from multiple disciplines such as psychologists, neurologists, paediatricians, nurse practitioners, dermatologists, anaesthesiologists, intensivists, physical and occupational therapists, and specialists in paediatric rehabilitation and intellectual disabilities were included in the guideline panel. Professionals were selected based on their experience with paediatric palliative care, of whom some had specific certified training in this field. Within the guideline development panel, a core group of 11 experts was established to ensure consistency throughout the guideline. The other 45 experts were appointed to working groups (WGs) that focused on symptom treatment (WG 1) and refractory symptom treatment (WG 2). WGs covered multiple topics for which sub-WGs were established. WG 1 consisted of 11 sub-WGs that focused on non-pharmacological and pharmacological interventions of anxiety and depression, delirium, dyspnoea, haematological symptoms, coughing, skin complaints, nausea and vomiting, neurological symptoms, pain, death rattle, and fatigue. WG 2 focused on paediatric palliative sedation and forgoing hydration and nutrition. All topics were selected based on priorities of health care providers and parents [22]. An overview of the working structure and guideline development process is shown in Appendix B and C.
Representation of patients and their families
Different methods were used to include perspectives of children and their families [22]. Two members of the core group were dedicated to ensure representation of child and family and their values during the entire guideline process. Additionally, a diverse panel consisting of nine (bereaved) parents of children with life-threatening or life-limiting conditions reviewed the first drafts of all guideline texts and recommendations and reviewed the complete concept guideline. We ensured that the panel represented a broad spectrum of experiences regarding paediatric palliative care by including parents of children with a variety of palliative conditions, age, and stage of disease (currently receiving palliative care or deceased).
Formulation of clinical questions
The two WGs formulated a total of 27 clinical questions (Appendix D). WG1 formulated 24 clinical questions on the effect non-pharmacological and pharmacological interventions for symptom treatment. WG 2 formulated three clinical questions that focused on the effect of paediatric palliative sedation and the effect of forgoing hydration and nutrition.
Search strategy and selection criteria
For the 27 clinical questions, we updated the literature search that was conducted for the former CPG (2013) [19] identifying randomized controlled trials (RCTs), controlled clinical trials (CCTs), or systematic reviews (SRs) of RCTs and CCTs on paediatric palliative care interventions (last update, January 24, 2020) (Appendix E). Studies were selected according to inclusion criteria related to study design (RCTs, CCTs, SRs of RCTs and CCTs), study population (children aged 0 to 18 with a life-threatening or life-limiting condition, according to the definition of the World Health Organization [6]) and study subject (paediatric palliative care interventions related to symptom treatment). Only studies published in English or Dutch language were included. Studies that described interventions on complementary or alternative medicine were excluded (Appendix F). We also searched for eligible studies in reference lists of included studies and identified SRs, guidelines, and textbooks. Moreover, we asked WG members to provide eligible studies.
Summary and appraisal of evidence
To answer the clinical questions, we summarized included studies in evidence tables. We categorized evidence by outcome measures in summary of findings tables. Then, we formulated conclusions of evidence for each outcome measure. The quality of the total body of evidence was graded using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) method [22]. Study selection, summary and appraisal of evidence and formulation of conclusions was performed by one independent reviewer [22]. All processes were checked by members of the core group. In case the systematic literature search would yield little to no evidence, we searched for textbooks on paediatric palliative care and existing evidence-based guidelines on general paediatrics, and paediatric and adult palliative care in several guideline databases (Appendix E). Textbooks and guidelines were included if they were deemed relevant for the topics addressed in the (sub) WGs (Appendix F). We used textbooks and recommendations from guidelines to refine considerations and recommendations for this guideline.
Translating evidence into recommendations
When translating the evidence into recommendations, several factors were taken into account: (1) the quality of the evidence (the higher the quality of evidence, the more likely it is to formulate a strong recommendation), (2) additional literature including textbooks and guidelines, (3) patient and family values and needs, (4) clinical expertise, (5) acceptability (legal and ethical considerations), (6) feasibility (sufficient time, knowledge, and manpower), and (7) benefits versus harms of the interventions. For each clinical question, WG members described the relevant considerations. Decisions regarding the final formulation of the recommendations were made through group consensus.
The strength of each recommendation was graded according to published evidence-based methods (appendix G) [23, 24]. Recommendations were categorised as strong to do (green), moderate to do (yellow) or strong not to do (red).
Results
Identification of evidence and additional literature
The systematic search for RCTs, CCTs and SRs of RCTs and CCTs on paediatric palliative care interventions yielded 5078 studies of which 168 were subjected to full-text screening. A total of 18 studies (three SRs of RCTs and 15 RCTs) on non-pharmacological and pharmacological interventions to treat symptoms were included (Appendix H). Furthermore, we included two textbooks, and 29 CPGs (six paediatric palliative care CPGs, 11 general paediatric CPGs and 12 adult palliative care CPGs) as additional literature to deal with lack of evidence (Appendix I).
Evidence
The evidence tables and summary of findings tables are presented in Appendix J and K and the conclusions of evidence are shown in Table 1.
Studies reported on the effects of the following specific interventions: non-invasive ventilation [25] and high intensity training [26] for dyspnoea; erythropoietin for anaemia (haematological symptoms) [27, 28]; naloxone for pruritus (skin complaints) [29]; self-hypnosis [30] and anti-emetics including ondansetron [31,32,33], metoclopramide [33], granisetron [34, 35], tropisetron [35], aprepipant [36], midazolam [37] and dexamethasone [37] for nausea and vomiting; botulinum toxin-A injections and occupational therapy [38, 39] for spasticity (neurological symptoms); and psychological interventions for parents including cognitive behavioural therapy, family therapy, problem-solving therapy and multi-systemic therapy [40] and adjuvant medication including intrathecal baclofen, botulinum toxin A injections, oral alendronate, oral risedronate and intravenous pamidronate [41] for pain.
A few interventions showed significant improvement in relief of symptoms or quality of life among children with life-threatening or life-limiting conditions. Non-invasive ventilation and high intensity training significantly improved exercise capacity in children with cystic fibrosis (very low quality evidence) [25, 26]. One study showed that treatment with naloxone significantly decreased incidence of pruritus in children who received opioids postoperatively (very low quality evidence). Regarding nausea and vomiting, self-hypnosis significantly decreased supplemental anti-emetic medication use and anticipatory nausea in children with cancer (very low quality evidence) [30]. In addition, most anti-emetic medication including ondansetron, granisetron, aprepipant, midazolam and dexamethasone significantly decreased the incidence of emetic episodes and/or nausea severity (very low to moderate quality evidence) [31,32,33,34,35,36,37]. Concerning interventions for neurological symptoms, botulinum toxin-A injections significantly decreased spasticity levels of upper limbs and significantly increased parent-reported efficacy in children with cerebral palsy (very low to low quality evidence) [38, 39]. Furthermore, cognitive behavioural therapy for parents significantly decreased child symptoms including pain in children with chronic illnesses (very low quality evidence) [40]. Additionally, oral alendronate decreased pain in children with osteogenesis imperfecta (low quality evidence) [41].
For other interventions no significant effects were found. This included treatment with erythropoietin to improve anaemia in children with cancer (low quality evidence) [27, 28]. Regarding pain in children with chronic illnesses, no significant effect was found for family therapy, problem-solving therapy, and multi-systemic therapy for parents which aimed to improve child symptoms (very low to low quality evidence) [40]. Also, botulinum toxin A injections, oral risedronate, and intravenous pamidronate did not significantly decrease pain (very low to low quality evidence) [41]. Furthermore, the effect of opioids on cancer-related pain remains unknown, as the systematic review did not identify any studies on this topic [42].
Additional literature
Because there was limited evidence on paediatric palliative care interventions, we identified additional literature. The relevant recommendations from 29 guidelines on paediatric palliative care, general paediatrics and adult paediatric palliative care [43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71] and the textbooks [72, 73] on paediatric palliative care were used to refine considerations and recommendations.
Translating evidence into recommendations
Recommendations were based upon the evidence, additional literature, clinical expertise, patient and family values, and other considerations such as costs and availability of medication. All members of the guideline development panel agreed that quality of life and values and needs of the child and family should be the main focus of every treatment-related decision. This was the starting point in the process of formulating recommendations.
Clinical experts, patient representatives and parents identified other key aspects that frequently influenced treatment-related recommendations. In addition to the treatment effects, the expected burden of treatment on the child was considered. Physical therapy techniques, for instance, can help to relief suffering due to coughing but are physically challenging and can only be considered if the child is willing and able to perform these techniques. Moreover, the adverse effects of potential interventions were considered. For example, starting antipsychotics to treat delirium carry a high risk of adverse effects [70]. Health care providers should be aware of these adverse effects of antipsychotics and monitor daily. If adverse effects occur, other medication should be considered. Finally, the child’s life-expectancy or prognosis is of importance. For example, vitamins and nutritional supplements should not be given to children with anaemia if life expectancy is short.
When formulating recommendations on paediatric palliative sedation and forgoing hydration and nutrition, clinical experts and parent representatives acknowledged the importance of thoughtful communication and careful preparation of all processes related to end-of-life care. Therefore, recommendations on refractory symptom treatment covered the entire process of paediatric palliative sedation and forgoing hydration and nutrition including communication, preparation, execution, and evaluation.
We formulated a total of 221 recommendations on (non-)pharmacological treatment of anxiety and depression, delirium, dyspnoea, haematological symptoms, coughing, skin complaints, neurological symptoms, pain, death rattle, fatigue, paediatric palliative sedation and forgoing hydration and nutrition. Based on the level of evidence and other factors such as patient and family values, clinical expertise, and benefits and harms of the intervention, we formulated 106 strong recommendations to do (green), 106 weak recommendations to consider (yellow) and six strong recommendations not to do (red). In three situations, there was insufficient evidence and lack of consensus among experts to determine whether the benefits of the specific intervention outweigh potential harms. As a result, it was not possible to formulate a recommendation. In Fig. 1 we provide an overview of the number of recommendations on symptom treatment per topic. All recommendations are shown in Tables 2 and 3.

Number and strength of recommendations on symptom treatment in paediatric palliative care
a It was not possible to formulate a recommendation due to insufficient evidence and lack of consensus among experts
Discussion
Optimal treatment to relieve symptoms in children with life-threatening or life-limiting conditions is intense and challenging. Although progress has been made in improving and integrating paediatric palliative care in the Netherlands [4], health care providers, parents and other stakeholders have urged for more guidance to relieve physical suffering and ease distress in these children and their families. We responded to this need by developing recommendations on symptom treatment, including anxiety and depression, delirium, dyspnoea, haematological symptoms, coughing, skin complaints, nausea and vomiting, neurological symptoms, pain, death rattle, fatigue, paediatric palliative sedation and forgoing hydration and nutrition, as part of the revised Dutch CPG for paediatric palliative care. With these recommendations we aim to optimize symptom treatment in paediatric palliative care in the Netherlands. Furthermore, these recommendations can be used in other countries to optimize symptom treatment on a global scale.
This study has multiple strengths. First of all, the selection of symptoms was based upon priorities of clinical experts and parents [22]. This approach allowed us to provide recommendations on the symptoms that were most relevant to children with life-threatening or life-limiting conditions and their families. Furthermore, in this way, we were able to provide recommendations for a diverse group of children without limiting to a specific diagnosis. It should be noted that the selection of symptoms does not cover the full range of symptoms that may occur in paediatric palliative care. Still, our selection of symptoms is most comprehensive in comparison to other international guidelines on paediatric palliative care [66]. Additionally, we introduce the first evidence-based recommendations on paediatric palliative sedation in Europe.
Second, our recommendations on symptom treatment are based on an evidence-based methodology, meaning that we systematically searched for RCTs, CCTs and SRs of RCTs and CCTs in scientific literature. We identified 18 studies reporting on effectivity of several non-pharmacological and pharmacological interventions to treat symptoms. We found that since the development of the first Dutch guideline in 2013, the number of studies on paediatric palliative care interventions has increased [19, 22]. However, after allocating the studies to the relevant clinical questions, we concluded that the evidence could only (partly) answer eight out of 27 clinical questions. Also, the total body of evidence was rated as low to very low quality, mainly due to imprecision of effects (as a result of small number of participants) and potential risk of bias. For the other 19 clinical questions on effects of symptom treatment, we did not find evidence. Therefore, we developed a strategy to deal with this lack of evidence and included additional literature: 29 guidelines on paediatric palliative care, general paediatrics, and adult palliative care, and two textbooks on paediatric palliative care.
Finally, our recommendations are carefully developed according to a transparent and comprehensive guideline methodology [22]. We closely collaborated with experts in paediatric palliative care from multiple disciplines and parents. The transparency and the interactive relationship between all stakeholders increased validity and trustworthiness of our guideline process and recommendations.
The recommendations within this guideline are based on national clinical expertise, patient perspectives, and international evidence. We believe that these targeted recommendations on symptom treatment will be largely applicable to other contexts and can give guidance for symptom treatment in other countries as well. However, country-specific factors such as availability of non- pharmacological and pharmacological interventions, infrastructure, financial resources, and cultural backgrounds, should always be carefully considered before applying any recommendations in other contexts.
Unfortunately, we identified multiple gaps in knowledge for non-pharmacological and pharmacological interventions to treat symptoms (Table 4). Even though evidence on paediatric palliative care has increased there is still paucity in evidence on non-pharmacological and pharmacological interventions to treat symptoms [19, 74]. However, it should be noted that these knowledge gaps are based on our search that focused on paediatric palliative care only. Extrapolating evidence from general paediatrics might fill some knowledge gaps for treatment of symptoms. On the other hand, it is acknowledged that paediatric palliative care requires expertise that is often lacking in general paediatrics [75]. Extrapolating study results from general paediatrics is not always appropriate, so caution is needed when applying this evidence.
It is clear that more research is required to relieve symptom-related suffering and to ease distress in children and family members. Future research should focus on international, multidisciplinary, and multi-institutional collaboration to reach higher numbers of participants, to broaden the scope of study questions and also improve study quality. In this way, we can strengthen the evidence base of our guideline and contribute to the optimization symptom treatment in paediatric palliative care. Additionally, attention should be given to facilitate implementation of knowledge and guidelines in paediatric palliative care for the purpose of achieving sufficient symptom relief in children with life-threatening and life-limiting conditions [75]. Furthermore, it should be noted that other factors such as access to financial resources and the organizational infrastructure of paediatric palliative care impact the quality of palliative care and differ among countries [2, 76]. These factors should be addressed to achieve optimal symptom treatment in paediatric palliative care on a global scale.
With these recommendations, we aim to limit symptom-related suffering and ease distress in children with life-threatening and life-limiting conditions and their families. Our methodology allowed us to provide evidence-based recommendations on a comprehensive selection of symptoms in close collaboration with experts in paediatric palliative care, and parents. Even though available evidence on symptom-related paediatric palliative care interventions has increased, there still is a paucity in evidence on non-pharmacological and pharmacological interventions to treat symptoms in paediatric palliative care. We urge for international multidisciplinary multi-institutional collaboration to perform high-quality research and to contribute to the optimization of symptom relief for all children with life-threatening or life-limiting conditions worldwide.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
- CPG:
-
Clinical Practice Guideline
- CCT:
-
Controlled Clinical Trial
- GRADE:
-
Grading Recommendation Assessment Development and Evaluation
- RCT:
-
Randomized Controlled Trial
- SR:
-
Systematic Review
- WG:
-
Working Group
- WG1:
-
Working group 1: Symptom treatment
- WG2:
-
Working group 2: Refractory symptom treatment
References
Connor SR, Downing J, Marston J. Estimating the global need for palliative care for children: a cross-sectional analysis. J Pain Symptom Manage. 2017;53(2):171–7.
Worldwide Hospice Palliative Care Alliance. Global Atlas of Palliative Care. London: Worldwide Hospice Palliative Care Alliance; 2020.
Kenniscentrum kinderpalliatieve zorg. Wat is kinderpalliatieve zorg? 2022. Updated 2022, December 1; cited 2023, October 29. Available from: https://kinderpalliatief.nl/over-kinderpalliatieve-zorg/wat-is-kinderpalliatieve-zorg/kinderpalliatieve-zorg.
Vallianatos S, Huizinga CSM, Schuiling-Otten MA, Schouten-van Meeteren AYN, Kremer LCM, Verhagen AAE. Development of the Dutch structure for integrated children’s palliative care. Children (Basel). 2021;8(9):741.
Centraal Bureau voor Statistiek. Overledenen; Doodsoorzaak (uitgebreide lijst), leeftijd, Geslacht: Statline; 2022. Updated 2022, December 20; cited 2023, February 22. Available from: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/7052_95/table?ts=1662990503553.
World Health Organization. Integrating palliative care and symptom relief into paediatrics: a WHO guide for health care planners, implementers and managers. Geneva: World Health Organization; 2018.
Balkin EM, Wolfe J, Ziniel SI, Lang P, Thiagarajan R, Dillis S, et al. Physician and parent perceptions of prognosis and end-of-life experience in children with advanced heart disease. J Palliat Med. 2015;18(4):318–23.
Marcus KL, Kao PC, Ma C, Wolfe J, DeCourcey DD. Symptoms and suffering at end of life for children with complex chronic conditions. J Pain Symptom Manage. 2022;63(1):88–97.
Wolfe J, Orellana L, Ullrich C, Cook EF, Kang TI, Rosenberg A, et al. Symptoms and distress in children with advanced cancer: prospective patient-reported outcomes from the PediQUEST study. J Clin Oncol. 2015;33(17):1928–35.
Wolfe J, Grier HE, Klar N, Levin SB, Ellenbogen JM, Salem-Schatz S, et al. Symptoms and suffering at the end of life in children with cancer. N Engl J Med. 2000;342(26):1997–9.
Rosenberg AR, Wolfe J, Wiener L, Lyon M, Feudtner C. Ethics, emotions, and the skills of talking about progressing disease with terminally ill adolescents: a review. JAMA Pediatr. 2016;170(12):1216–23.
Steineck A, Bradford MC, O’Daffer A, Fladeboe KM, O’Donnell MB, Scott S, et al. Quality of life in adolescents and young adults: the role of symptom burden. J Pain Symptom Manage. 2022;64(3):244–53.e2.
Tomlinson D, Hinds PS, Bartels U, Hendershot E, Sung L. Parent reports of quality of life for pediatric patients with cancer with no realistic chance of cure. J Clin Oncol. 2011;29(6):639–45.
Kreicbergs U, Valdimarsdottir U, Onelov E, Bjork O, Steineck G, Henter JI. Care-related distress: a nationwide study of parents who lost their child to cancer. J Clin Oncol. 2005;23(36):9162–71.
Wolfe J, Hammel JF, Edwards KE, Duncan J, Comeau M, Breyer J, et al. Easing of suffering in children with cancer at the end of life: is care changing? J Clin Oncol. 2008;26(10):1717–23.
Grimshaw JM, Russell IT. Effect of clinical guidelines on medical practice: a systematic review of rigorous evaluations. The Lancet. 1993;342(8883):1317–22.
Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, Vale L, et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol Assess. 2004;8(6):iii–iv, 1–72.
Lugtenberg M, Burgers JS, Westert GP. Effects of evidence-based clinical practice guidelines on quality of care: a systematic review. Qual Saf Health Care. 2009;18(5):385–92.
Knops RR, Kremer LC, Verhagen AA, Dutch Paediatric Palliative Care Guideline Group for S. Paediatric palliative care: recommendations for treatment of symptoms in the Netherlands. BMC Palliat Care. 2015;14:57.
Jagt-van Kampen CT, Kremer LC, Verhagen AA, Schouten-van Meeteren AY. Impact of a multifaceted education program on implementing a pediatric palliative care guideline: a pilot study. BMC Med Educ. 2015;15:194.
Nederlandse Vereniging voor Kindergeneeskunde. Richtlijn palliatieve zorg voor kinderen. 2022. Updated 2022, November 28; cited 2023, October 26. Available from: https://palliaweb.nl/richtlijnen-palliatieve-zorg/richtlijn/palliatieve-zorg-voor-kinderen.
van Teunenbroek KC, Kremer LCM, Verhagen AAE, Verheijden JMA, Rippen H, Borggreve BCM, et al. Palliative care for children: methodology for the development of a national clinical practice guideline. BMC Palliat Care. 2023;22(1):193.
Gibbons RJ, Smith S, Antman E. American College of Cardiology/American Heart Association clinical practice guidelines: Part I: where do they come from? Circulation. 2003;107(23):2979–86.
Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004;328(7454):1490.
Lima CA, Andrade Ade F, Campos SL, Brandao DC, Fregonezi G, Mourato IP, et al. Effects of noninvasive ventilation on treadmill 6-min walk distance and regional chest wall volumes in cystic fibrosis: randomized controlled trial. Respir Med. 2014;108(10):1460–8.
de Jong W, van Aalderen WM, Kraan J, Koeter GH, van der Schans CP. Inspiratory muscle training in patients with cystic fibrosis. Respir Med. 2001;95(1):31–6.
Büyükpamukçu M, Varan A, Kutluk T, Akyüz C. Is epoetin alfa a treatment option for chemotherapy-related anemia in children? Med Pediatr Oncol. 2002;39(4):455–8.
Razzouk BI, Hord JD, Hockenberry M, Hinds PS, Feusner J, Williams D, et al. Double-blind, placebo-controlled study of quality of life, hematologic end points, and safety of weekly epoetin alfa in children with cancer receiving myelosuppressive chemotherapy. J Clin Oncol. 2006;24(22):3583–9.
Maxwell LG, Kaufmann SC, Bitzer S, Jackson EVJ, McGready J, Kost-Byerly S, et al. The effects of a small-dose naloxone infusion on opioid-induced side effects and analgesia in children and adolescents treated with intravenous patient-controlled analgesia: a double-blind, prospective, randomized controlled study. Anesth Analg. 2005;100(4):953–8.
Jacknow DS, Tschann JM, Link MP, Boyce WT. Hypnosis in the prevention of chemotherapy-related nausea and vomiting in children: a prospective study. J Dev Behav Pediatr. 1994;15(4):258–64.
Parker RI, Prakash D, Mahan RA, Giugliano DM, Atlas MP. Randomized, double-blind, crossover, placebo-controlled trial of intravenous ondansetron for the prevention of intrathecal chemotherapy-induced vomiting in children. J Pediatr Hematol Oncol. 2001;23(9):578–81.
Brock P, Brichard B, Rechnitzer C, Langeveld N, Lanning M, Söderhäll S, et al. An increased loading dose of ondansetron: a north European, double-blind randomised study in children, comparing 5 mg/m2 with 10 mg/m2. Eur J Cancer. 1996;32(10):1744–8.
Köseoglu V, Kürekçi A, Sorici Ü, Atay A, Özcan O. Comparison of the efficacy and side-effects of ondansetron and metoclopramide-diphenhydramine administered to control nausea and vomiting in children treated with antineoplastic chemotherapy: a prospective randomized study. Eur J Pediatr. 1998;157(10):806–10.
Orchard PJ, Rogosheske J, Burns L, Rydholm N, Larson H, DeFor TE, et al. A prospective randomized trial of the anti-emetic efficacy of ondansetron and granisetron during bone marrow transplantation. Biol Blood Marrow Transplant. 1999;5(6):386–93.
Aksoylar S, Akman SA, Ozgenc F, Kansoy S. Comparison of tropisetron and granisetron in the control of nausea and vomiting in children receiving combined cancer chemotherapy. Pediatr Hematol Oncol. 2001;18(6):397–406.
Gore L, Chawla S, Petrilli A, Hemenway M, Schissel D, Chua V, et al. Aprepitant in adolescent patients for prevention of chemotherapy-induced nausea and vomiting: a randomized, double-blind, placebo-controlled study of efficacy and tolerability. Pediatr Blood Cancer. 2009;52(2):242–7.
Riad W, Altaf R, Abdulla A, Oudan H. Effect of midazolam, dexamethasone and their combination on the prevention of nausea and vomiting following strabismus repair in children. Eur J Anaesthesiol. 2007;24(8):697–701.
Olesch CA, Greaves S, Imms C, Reid SM, Graham HK. Repeat botulinum toxin-A injections in the upper limb of children with hemiplegia: a randomized controlled trial. Dev Med Child Neurol. 2010;52(1):79–86.
Copeland L, Edwards P, Thorley M, Donaghey S, Gascoigne-Pees L, Kentish M, et al. Botulinum toxin A for nonambulatory children with cerebral palsy: a double blind randomized controlled trial. J Pediatr. 2014;165(1):140–6 e4.
Eccleston C, Fisher E, Law E, Bartlett J, Palermo TM. Psychological interventions for parents of children and adolescents with chronic illness. Cochrane Database Syst Rev. 2015;4:CD009660.
Beecham E, Candy B, Howard R, McCulloch R, Laddie J, Rees H, et al. Pharmacological interventions for pain in children and adolescents with life-limiting conditions. Cochrane Database Syst Rev. 2015;3:CD010750.
Wiffen PJ, Cooper TE, Anderson AK, Gray AL, Gregoire MC, Ljungman G, et al. Opioids for cancer-related pain in children and adolescents. Cochrane Database Syst Rev. 2017;7:CD012564.
Bolier L, Speetjens P, Volker D, Sinnema H. JGZ-Richtlijn Angst. Utrecht: Trimbos-Instituut; 2016. Updated 2016; cited 2021, July 13. Available from: https://www.ncj.nl/richtlijnen/alle-richtlijnen/richtlijn/angst.
Oud M, van der Zanden R, Coronenberg I, Sinnema H. JGZ-richtlijn Depressie. Utrecht: Trimbos-instituut; 2016. Updated 2016; cited 2023, May 8. Available from: https://www.ncj.nl/richtlijnen/alle-richtlijnen/richtlijn/depressie.
National Institute for Health and Care Excellence. Care of dying adults in the last days of life. London: NICE; 2015. Updated 2015, December 16; cited 2023, May 8. Available from: www.nice.org.uk/guidance/ng31.
National Institute for Health Care and Excellence. Depression in Children and Young People: identification and mangement. London: NICE; 2019. Cited 2023, May 8. Available from: https://www.nice.org.uk/guidance/ng134.
Integraal Kankercentrum Nederland. Dyspneu in de palliatieve fase (3.0). 2015. Updated 2015, December 22; cited 2023, May 8. Available from: https://palliaweb.nl/richtlijnen-palliatieve-zorg/richtlijn/dyspneu.
Federatie Medisch Specialisten. Bloedtransfusiebeleid. 2019. Updated 2020, October 15; cited 2023, May 8. Available from: https://richtlijnendatabase.nl/richtlijn/bloedtransfusiebeleid/startpagina_-_bloedtransfusiebeleid.html.
Nederlandse vereniging voor kindergeneeskunde. Erytrocytentransfusies bij kinderen & neonaten met kanker. 2022. Updated 2022, June 29; cited 2023, May 8. Available from: https://richtlijnendatabase.nl/richtlijn/erytrocytentransfusies_bij_kinderen_neonaten_met_kanker/startpagina_-_erytrocytentransfusies.html.
Nederlandse Vereniging voor Kindergeneeskunde. Trombocytentransfusies bij kinderen met kanker. 2022. Updated 2022, June 29; cited 2023, May 8. Available from: https://richtlijnendatabase.nl/richtlijn/trombocytentransfusies_bij_kinderen_met_kanker/startpagina_-_trombocytentransfusies.html.
Integraal Kankercentrum Nederland. Hoesten (2.0). 2010. Updated 2010, June 18; cited 2023, May 8. Available from: https://palliaweb.nl/richtlijnen-palliatieve-zorg/richtlijn/hoesten.
Integraal Kankercentrum Nederland. Richtlijn Jeuk in de palliatieve fase. 2022. Updated 2022, February 21; cited 2023, May 8. Available from: https://palliaweb.nl/richtlijnen-palliatieve-zorg/richtlijn/jeuk.
Integraal Kankercentrum Nederland. Oncologische Ulcera. 2010. Updated 2010, August 11; cited 2023, May 8. Available from: https://palliaweb.nl/richtlijnen-palliatieve-zorg/richtlijn/oncologische-ulcera.
Nederlands Centrum Jeugdgezondheid. Huidafwijkingen, taakomschrijving en richtlijn voor de preventie, signalering, diagnostiek, begeleiding, behandeling en verwijzing. 2012. Updated 2012, May; cited 2023 May 8. Available from: https://assets.ncj.nl/docs/d3452a1b-34b2-4154-8106-9977ef5426f3.pdf.
Verpleegkundigen & Verzorgenden Nederland. Smetten (Intertrigo) preventie en behandeling. 2018. Updated 2018, September; cited 2023, May 8. Available from: https://www.venvn.nl/media/n0fppki5/richtlijn-smetten-september-2018.pdf.
Verpleegkundigen & Verzorgenden Nederland. Richtlijn Decubitus. 2021. Updated 2021, March 1; cited 2023, May 8. Available from: https://www.venvn.nl/media/adujx1ja/20210224-richtlijn-decubitus.pdf.
Dupuis LL, Robinson PD, Boodhan S, Holdsworth M, Portwine C, Gibson P, et al. Guideline for the prevention and treatment of anticipatory nausea and vomiting due to chemotherapy in pediatric cancer patients. Pediatr Blood Cancer. 2014;61(8):1506–12.
Integraal Kankercentrum Nederland. Misselijkheid en braken (4.0). 2014. Updated 2014, June 16; cited 2023, May 8. Available from: https://palliaweb.nl/richtlijnen-palliatieve-zorg/richtlijn/misselijkheid-en-braken.
Flank J, Robinson PD, Holdsworth M, Phillips R, Portwine C, Gibson P, et al. Guideline for the treatment of breakthrough and the prevention of refractory chemotherapy-induced nausea and vomiting in children with cancer. Pediatr Blood Cancer. 2016;63(7):1144–51.
National Institute for Health and Care Excellence. Spasticity in under 19s: Management. London: NICE; 2012. Updated 2016, November 29; cited 2023, May 8. Available from: www.nice.org.uk/guidance/cg145.
National Institute for Health and Care Excellence. Epilepsies: diagnosis and management. London: NICE; 2012. Updated 2021, May 12; cited 2023, May 8. Available from: www.nice.org.uk/guidance/cg137.
Nederlandse Vereniging van Revalidatieartsen. Cerebrale en/of spinale spasticiteit.: VRA; 2016. Updated 2016, January 1; cited 2023 May 8. Available from: https://richtlijnendatabase.nl/richtlijn/cerebrale_en_of_spinale_spasticiteit/cerebrale_en_of_spinale_spasticiteit_-_startpagina.html.
Nederlandse Vereniging voor Neurologie. Epilepsie. 2020. Cited 2023, May 8.
Joanna Briggs Institute. Effectiveness of non-pharmacological pain management in relieving chronic pain for children and adolescents. Best Pract. 2010;14(17):1–4.
Integraal Kankercentrum Nederland. Zorg in de stervensfase (1.0). 2010. Cited 2023, May 8. Available from: https://palliaweb.nl/richtlijnen-palliatieve-zorg/richtlijn/stervensfase.
National Institute for Health and Care Excellence. End of life care for infants, children and young people with life-limiting conditions: planning and management. London: NICE; 2016. Updated 2019, July 25; cited 2023, May 8. Available from: https://www.nice.org.uk/guidance/ng61.
Integraal Kankercentrum Nederland. Vermoeidheid bij kanker in de palliatieve fase (3.0). 2019. Updated 2019, May 9; cited 2023, May 8. Available from: https://palliaweb.nl/richtlijnen-palliatieve-zorg/richtlijn/vermoeidheid-bij-kanker.
Nederlandse Vereniging voor Kindergeneeskunde. Somatisch onvoldoende verklaarde lichamelijke klachten (SOLK) bij kinderen. 2019. Updated 2019, March 3; cited 2023, May 8. Available from: https://assets.nvk.nl/p/491522/files/SOLK.pdf.
Integraal Kankercentrum Nederland. Richtlijn palliatieve sedatie. 2022. Updated 2022, June 16. Available from: https://palliaweb.nl/richtlijnen-palliatieve-zorg/richtlijn/palliatieve-sedatie.
Nederlandse Vereniging voor Psychiatrie. Multidisciplinaire richtlijn pediatrisch delier (PD) en emergence delier (ED). 2021. Updated 2021, November 11; cited 2023, May 8. Available from: https://richtlijnendatabase.nl/richtlijn/pediatrisch_delier_pd_en_emergence_delier_ed/startpagina_-_pediatrisch_delier_pd_en_emergence_delier_ed.html.
Anderson A-K, Burke K, Bendle L, Koh M, McCulloch R, Breen M. Artificial nutrition and hydration for children and young people towards end of life: consensus guidelines across four specialist paediatric palliative care centres. BMJ Support Palliat Care. 2019;11:92–100.
Goldman A, Hain R, Liben S. Oxford Textbook of Palliative Care for Children. 2nd ed. Oxford: Oxford University Press; 2012.
Wolfe J, Hinds P, Sourkes B. Textbook of Interdisciplinary pediatric palliative care. United States of America: Saunders; 2011.
Fraser LK, Bluebond-Langner M, Ling J. Advances and challenges in European paediatric palliative care. Med Sci. 2020;8(2):20.
Nilsson S, Ohlen J, Hessman E, Brännström M. Paediatric palliative care: a systematic review. BMJ Support Palliat Care. 2020;10(2):157–63.
Arias-Casais N, Garralda E, Pons JJ, Marston J, Chambers L, Downing J, et al. Mapping pediatric palliative care development in the WHO-European Region: children living in low-to-middle-income countries are less likely to access it. J Pain Symptom Manage. 2020;60(4):746–53.
Acknowledgements
Collaborators of the working groups symptom treatment and refractory symptom treatment of the Dutch paediatric palliative care guideline (in alphabetic order)
First name | Middle initials | Surname |
Mattijs | W | Alsem |
Esther | M. M | van den Bergh |
Govert | Brinkhorst | |
Arno | Colenbrander | |
Linda | Corel | |
Jennifer | van Dijk | |
Laurent | Favié | |
Karin | Geleijns | |
Saskia | J | Gischler |
Lisette | ‘t Hart-Kerkhoffs | |
Hanneke | Heinen | |
Cindy | Joosen | |
Carla | C. M | Juffermans |
Hennie | Knoester | |
Barbara | de Koning | |
Tom | de Leeuw | |
Hilda | Mekelenkamp | |
Mariska | P | Nieuweboer |
Sebastianus | B.J | Oude Ophuis |
Suzanne | G. M. A | Pasmans |
Elise | M | van de Putte |
Emmy | Räkers | |
Irma | M | Rigter |
Christel | D | Rohrich |
Elisabeth | J | Ruijgrok |
Kim | van der Schoot | |
Ellen | Siegers-Bennink | |
Henriette | Sjouwke | |
Tanneke | Snijders-Groenendijk | |
Suzanne | van de Vathorst | |
Leo | van Vlimmeren | |
Anne | Weenink | |
Willemien | de Weerd | |
Ilse | H | Zaal-Schuller |
Funding
This study has received funding from The Netherlands Association for Health Research and Development (ZonMw). The funder of the study had no role in study design, data collection, data analysis, data interpretation, or in writing the manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
KvT, RM, EM, LK, EV, BB, JV, and HR conceived and designed the study. KvT, RM, and EM performed the search, data extractions, risk of bias assessment, and GRADE assessment. KvT, RM, EM, LK and EV interpreted the data. KvT, RM, IA, KB, CD, AG, MdG, KH, JL, MM, SM, JS, AS, JV, HR, BB, LK, EV, and EM contributed to the formulation of the recommendations. KvT, RM, EM, LK, and EV drafted the manuscript; and all authors critically revised the manuscript. All authors (KvT, RM, IA, KB, CD, AG, MdG, KH, JL, MM, SM, JS, AS, JV, HR, BB, LK, EV, and EM) and the collaborators approved the final version of this paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations. No institutional or other licensing committee’s approval is needed for guideline creation, as participants are not subjected to procedures and are not required to follow rules of behaviour. Therefore, in accordance to the Dutch law (Medical Research Involving Human Subjects Act (WMO), article 1b) ethics approval was deemed unnecessary: https://english.ccmo.nl/investigators/legal-framework-for-medical-scientific-research/your-research-is-it-subject-to-the-wmo-or-not.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix A.
Paediatric palliative care guideline panel. Appendix B. Working structure for guideline development. Appendix C. Guideline development process. Appendix D. Clinical questions. Appendix E. Search strategies. Appendix F. Inclusion criteria. Appendix G. Criteria for grading levels of evidence and strength of recommendations. Appendix H. Flowchart of the study selection process. Appendix I. Results of the systematic literature search: included studies; Appendix J. Evidence tables; Appendix K. Summary of findings tables, appraisal of evidence, and conclusions of evidence.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
van Teunenbroek, K.C., Mulder, R.L., Ahout, I.M.L. et al. A Dutch paediatric palliative care guideline: a systematic review and evidence-based recommendations for symptom treatment. BMC Palliat Care 23, 72 (2024). https://doi.org/10.1186/s12904-024-01367-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12904-024-01367-w