
Abstract
Background
Conventional glass ionomer cements (GICs) are currently the most widely used dental cements due to their chemical bonding into tooth structure, release of fluoride, and ease of manipulation and usage. One of their drawbacks is their low mechanical properties and high solubility. Carbon nanotubes (CNTs) could be utilized in dentistry due to their several potential applications. CNTs can be used as fillers to reinforce polymers or other materials. Additionally, silver (Ag) nanoparticles are highly effective at preventing dental biofilm and enhancing mechanical properties.
Objectives
The aim of the present in vitro study is to evaluate the compressive strength, surface microhardness, solubility, and antimicrobial effect of the conventional GIC reinforced with manual blending of 0.01 wt.% Ag doped CNT fillers.
Methods
The control group was prepared by mixing dental GIC powder with their liquid. The innovatively reinforced dental GIC group was prepared by incorporating 0.01 wt.% Ag doped CNT fillers into the GIC powder prior to liquid mixing. Chemical characterization was performed by XRF. While, physical characterization was done by measuring film thickness and initial setting time.
The compressive strength, surface microhardness, solubility, and antimicrobial effect against Streptococcus mutans bacteria using an agar diffusion test were measured. The data was statistically analyzed using independent sample t-tests to compare mean values of compressive strength, surface microhardness, solubility, and antimicrobial activity (p ≤ 0.05).
Results
The results revealed that innovative reinforced GIC with 0.01 wt.% Ag doped CNT fillers showed higher mean compressive strength, surface microhardness, and antimicrobial effect values than the conventional GIC control group; there was no significant difference between different groups in relation to the solubility test (P ≤ 0.05).
Conclusion
The innovatively reinforced GIC with 0.01 wt.% Ag doped CNT fillers had the opportunity to be used as an alternative to conventional GIC dental cements.
Similar content being viewed by others


Background
Polymers have widely dental applications [1,2,3,4]. Glass ionomer cement (GIC) is an aesthetic restorative material with a self-adhesive property [5, 6]. It is a mixture of fluoro-aluminosilicate glass powder and liquid polyacrylic acid in terms of chemistry [7]. It has been employed in a variety of dental applications, including minimally invasive and atraumatic direct restoratives, liner and bases, pit and fissure sealants, and endodontic sealers [8, 9]. Clinicians prefer to use GICs for long-term temporary restorations, the sandwich approach, luting agent, root caries, and permanent restorations in non-stress bearing areas, also cementation of orthodontic appliances and prosthodontic frameworks on the primary teeth [10,11,12]. Their properties are generally attractive for these applications and include high aesthetic properties, biocompatibility, fluoride-releasing and remineralization ability, chemical adhesion to the tooth surface, and matching the coefficient of thermal expansion of the natural tooth [13, 14]. Despite these benefits, their main disadvantage is low early mechanical properties in sites subjected to high stresses, and low wear resistance, in addition to their high solubility, which may affect their survival rates when used in load-bearing regions [13]. Film thickness and the initial setting time of the dental cements are two significant physical properties of an important aspect of restorative dentistry [15]. Several attempts were performed to improve the conventional GICs to stun their drawbacks, many studies aimed to enhance the mechanical characteristics of GICs. This was accomplished by adding nanofiller particles to GICs, such as bioactive glass, hydroxyapatite powders, metallic powders, nanoclay, and glass fibers [16,17,18,19].
Carbon nanotubes (CNTs) are cylindrical hollow structures consisting of a hexagonal network of carbon atoms at the nanoscale [20]. CNTs can be utilized as fillers to strengthen polymers or other materials, forming metal-based inorganic nanoparticles [21]. Multi-walled CNTs have emerged as superior fillers due to their larger surface area, high loading capacity, and potential to interact with biological membranes [22]. Consequently, their higher mechanical features and enhanced antimicrobial activity suggest that they would be utilized as promising fillers for dental applications [23]. They demonstrated adequate performance in reinforcement due to the load transfer on the interfacial bonding of the reinforced material and the CNTs [24].
Several metals, like silver, copper, gold, titanium, and zinc, have been employed as antimicrobial materials. Each of these metals has unique properties and a range of activities [25]. Silver (Ag) nanoparticles have long been utilized in dentistry due to their antibacterial activity. They are considered an efficient antibacterial filler, have great potential to inhibit biofilm, and also act as strengthening agents [20]. Functionalizing CNTs with other metallic nanoparticles such as gold, palladium, platinum, and silver may be able to produce nanofillers with predictable superior properties [26]. The doping of CNTs with Ag nanoparticles has potential applications as advanced nanocomposites with enhanced mechanical properties and antibacterial potential [22].
The aim of the present study was to evaluate the compressive strength, surface microhardness, solubility, and antimicrobial effect of dental GIC reinforced with Ag doped multi-walled CNT fillers against the untreated GIC (control). The null hypothesis was that the incorporation of 0.01 wt.% Ag doped CNT into conventional GIC would not affect the compressive strength, surface microhardness, solubility, or antimicrobial effect against Streptococcus mutans compared to the untreated control group.
Methods
The present experimental study was approved by the Medical Research Ethical Committee (MREC) of the National Research Centre (NRC), Cairo, Egypt (Reference number: 98072032023).
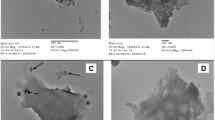
For this study, a commercially available conventional chemically cured GIC was provided in powder and liquid form: Fuji IX GP Extra (GC Corporation, Tokyo, Japan). Commercial multi-walled CNT doped with 12 wt.% Ag nanoparticle powder was also used (Nanografi Nano Technology, Jena, Germany). The specifications of the Ag-doped CNT were: an average particle length range of 15–25 nm, an average outside diameter less than 50 nm, an average inside diameter of 5 nm, and an average purity of more than 97 wt.%.
Preparation of the specimens
A total of 80 specimens were used. The specimens were divided into two main groups (n = 40/group) based on the type of powder used in the mixing process. The sample size was calculated using the G*Power (version 3.1.9.7) sample size calculator based on means and standard deviations [27]. The estimated sample size for each group was 10. The control group was prepared by mixing the conventional GIC powder with their liquid; the treated group was obtained by hand-mixing of 0.01 wt.% silver-doped CNT fillers with the conventional GIC powder using a mortar and pestle to obtain a homogenous powder. The prepared powder was then mixed with their liquid. The mixing of powder and liquid was done according to the manufacturer’s instructions. The mixed material from each group was placed in custom-made Teflon molds according to each test. A polyester strip was placed to prevent air trapping, and gentle compression was applied to the materials on both sides of the mold by a glass slide. Specimens were removed from the mold after the setting time specified by the manufacturer. The specimens were then examined visually for imperfections.
Characterization of prepared specimens
Chemical characterization of the control and treated specimens were performed using a non-destructive X-ray fluorescence (XRF) analysis (X-MET3000TXR, Oxford Instruments GmbH Co., Borsigstrasse, Germany) to verify their chemical composition [28].
Physical characterization of the control and treated specimens were assessed by measuring film thickness and setting time. The film thickness of the control and treated specimens was investigated according to the International Standard Organization (ISO) ISO standard 9917–2 instructions [29]. Using an electronic digital caliper (Digital Vernier Caliper, Mitutoyo, Japan), the thickness of two flat glass plates fastened in contact was measured four times to the nearest 0.1 m. This reading was recorded as reading A. The cement for each group (n = 10) was mixed according to the manufacturer’s instructions. After mixing, a consistent amount of each cement mixture was then distributed between the two glass plates. A load of 147 N was applied on the upper glass plate using a universal testing machine (Shimadzu Autograph AG–X Plus, Kyoto, Japan). The overall thickness of the plates with the specimen in between was recorded as reading B after seven minutes. The final combined film thickness for the specimen under test was determined as the difference between the thickness of the plates with and without the material between (B-A) [29].
Initial setting times was determined by the Gillmore needles (Humboldt MFG., Norridge, IL, USA) according to ADA specifications [30]. The initial setting time was calculated using a light needle with a tip diameter of 2.12 mm and a weight of 113.4 g. Every 30 s, the needle was positioned on the surface. Initial setting times were determined from the beginning of mixing until the needle did not leave a mark on the surface, respectively. Ten samples were measured for each group [31].
Testing of specimens
All the specimens were polished to remove any irregularities using 600-grit sandpaper. Specimens were protected with one layer of GIC varnish [32].
Compressive strength test
Ten cylinder-shaped specimens per group (12 mm in height and 6 mm in diameter) were prepared according to the standard specification for dental glass ionomer cements, ANSI/ADA Specification No. 66 (1989) [33]. The specimens were removed from the molds and stored in an incubator (CBM, S.r.l. Medical Equipment, 2431/V, Cremona, Italy) for 24 h in 95 ± 5% relative humidity at 37 °C. Specimens were loaded in compression at a crosshead speed of 1.0 mm/min in a universal testing machine (Shimadzu Autograph AG–X Plus, Kyoto, Japan) until fracture occurred [34].
Microhardness test
Ten disc-shaped specimens per group (5 mm in height and 2 mm in diameter) were prepared. The specimens were removed from the molds and incubated for 24 h in a highly humid environment at 37 °C. Surface microhardness for each specimen was determined using a digital Vickers hardness tester (NEXUS 400TM, INNOVATEST, model no. 4503, Maastricht, Netherlands). The indentations were made within 15 s of dwell time at a load of 100 g at 20 × magnificence. The mean surface microhardness value for each specimen was expressed in Vickers hardness numbers (VHN) [35].
Solubility test
Solubility was investigated using a Teflon mold measuring 7 mm in diameter and 2 mm in thickness [36], to obtain a disc-shaped specimen (n = 10). The specimens of each group were stored in a desiccator with silica gel (Merck KGaA, Darmstadt, Germany) for 2 h and then incubated in an incubator at 37 °C for 22 h. Specimens were weighed on a precision analytical balance instrument (Adam equipment 4 digits precision weighing balance, Adam Equipment Inc., Oxford, UK) with an accuracy of 0.001 g to obtain the initial mass (M1) values. Then, the specimens were immersed in a plastic flask containing 25 mL of distilled water, stored for 7 days, and incubated at 37 °C for 7 days. Then, each specimen was removed, dried gently with absorbent paper, and weighed again to get the mass values of the specimens after immersion (M2) [37]. The percentage of solubility was calculated using the equation [38]:
where M1 is the initial mass and M2 is the final mass of the specimens. The test was repeated three times [36].
Antibacterial activity test
Ten-disc specimens for each group measuring 2 mm in height and 4 mm in diameter were prepared. The specimens were stored in an incubator for 24 h at 37 °C. Then antibacterial activity of the specimens was evaluated against Streptococcus mutans bacteria. The antibacterial activity was investigated using agar diffusion method [39]. The Streptococcus mutans (EMCC 1815) bacterial strains were acquired. The samples were inoculated on Brain Heart Infusion (BHI) agar plates (HiMedia M211, HiMedia Laboratories Pvt. Limited, Mumbai, India) and then incubation at 37 °C for 3 days, the inhibition zone was observed. The total diameter of the inhibition zone in mm for each group was measured.
Statistical analysis
The statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) 16.0 statistical software (IBM-SPSS version 27.0, New York, NY, USA). Data was analyzed using independent sample t-tests to compare mean values of compressive strength, surface microhardness, solubility, and antimicrobial activity. The significance level was set at p ≤ 0.05.
Results
Chemical characterization results
The chemical composition of the control and treated specimens analyzed by XRF is represented in Table 1.
Physical characterization results
Film thickness
The results of the film thickness of the control and treated specimens are represented in Table 2. There was no significant difference (P = 0.07) in the film thickness values between untreated GIC (control) and treated GIC (24 µm and 24.4 µm respectively).
Setting time
The results of the initial setting time of the control and treated specimens are represented in Table 3. There was no significant difference (P = 0.5) in the initial setting time between untreated GIC (control) and treated GIC (97.7 and 98.7 s respectively).
Testing results
Compressive strength results
The results of the compressive strength are represented in Table 4. The compressive strength value of the treated GIC with the Ag-doped CNT group (172.7 MPa) was significantly higher than the untreated GIC (control) group (105 MPa), (P = 0.0001*).
Microhardness results
The results of the microhardness are represented in Table 5. The Vickers microhardness value of the treated GIC with the Ag-doped CNT group (92.5 VHN) was significantly higher than the untreated GIC (control) group (61.3 VHN), (P = 0.0001*).
Solubility results
The results of the solubility are represented in Table 6. There was no significant difference in solubility mean values among the control group (3.4%) and treated group (3.1%), (P = 0.1).
Antibacterial activity test
The results of the agar diffusion test against Streptococcus mutans are represented in Table 7. There was a significant difference in the antibacterial activity against Streptococcus mutans in both groups. The control group showed a significantly lower inhibition zone value around the discs (1 mm). While the treated group showed a significantly higher inhibition zone value around the peripheries of the treated discs (9 mm), (P = 0.0001*).
Discussion
Conventional GICs are extensively used in dentistry because of their distinctive qualities, such as chemical bonding to tooth structures, necessitating the least amount of dental preparation [40], chemical bonding with base metals, thermal compatibility with enamel, biocompatibility and low cytotoxicity, fluoride release ability, and provide chemical bonding to tooth structure, thus requiring a minimum tooth preparation [40]. However, one of the main issues with GIC is that it has a lower mechanical properties than recent resin composite materials [41]. The durability of GIC is affected by numerous factors, such as microhardness and solubility [36]. Solubility is one of the most crucial factors for evaluating the quality of materials used for liners, bases, luting agents, and restorations [36]. The solubility of restorative materials has a great influence on their stability, biocompatibility, and longevity [36].
As secondary caries is one of the most prevalent causes of dental restoration failure, it has also frequently been noted that the presence of biofilm on the surface of the restorative materials may facilitate the emergence of secondary caries lesions [42]. Secondary caries is mainly developed by the invasion of cariogenic bacteria, principally Streptococcus mutans [43]. Therefore, the antibacterial activity of restorative materials is of great value to avoid the possibility of secondary caries along the tooth-restoration interface [44]. The ideal’ dental cement and restoration should have several features, such as high surface and mechanical characteristics, adequate setting time, and a low film thickness (less than 25 µm) for the luting agent [45].
The development of nanotechnology has led to the development of new caries management strategies. In low concentrations, Ag nanoparticles have substantial antibacterial activity against Streptococcus mutans [46]. Ag nanoparticles may exhibit a synergistic antibacterial effect when combined with other antibacterial element [47].
The exceptional mechanical characteristics of CNT make it possible to be incorporated into dental materials for a pioneering functional application [48]. Ag-nanoparticles and CNTs could be functionalized together to create novel fillers that could be able to enhance the mechanical properties, surface microhardness, solubility, and antimicrobial activity of conventional GIC [24]. The functionalized CNT fillers were incorporated in a minimal concentration of 0.01 wt.% in an attempt to improve the mechanical properties without deterioration of the surface microhardness [49].
A compressive strength test simulates the load exerted on materials used in dental practice, the majority of mastication stresses are compressive in nature [50]. Compressive tests represent the critical value at which the material can withstand during the masticatory process [51]. The posterior teeth can withhold masticatory forces up to 125 MPa, while the primary dentition can only withstand compressive strength up to 100 MPa [52].
The current study has been carried out to evaluate the effect of incorporating 0.01 wt.% Ag-doped CNT fillers into commercially available conventional GIC on compressive strength, surface microhardness, solubility, and antimicrobial activity against Streptococcus mutans. The null hypothesis was rejected, where the incorporation of 0.01 wt.% Ag-doped CNT into conventional GIC significantly affected the compressive strength, surface microhardness and antimicrobial activity against Streptococcus mutans compared to the control group.
The result of the XRF confirmed that the chemical compounds of the Ag-doped CNTs were incorporated into glass ionomer material specimens. In accordance with ADA No. 8 [53], dental cement should have a film thickness no more than 25 µm for water-based luting cements and no more than 50 µm for resin-based cements. Minimal film thickness will lead to enhanced restoration retention and reduce marginal discrepancies [54]. Both treated and control groups provide a film thickness lower than 25 µm. Moreover, the results revealed no significant difference between groups, which may be attributed to the lower concentration of the added fillers in the treated groups. As regard the initial setting time, the results revealed no significant difference between groups, which may also be attributed to the lower concentration of the added fillers in the treated groups, which leads to a negligible effect.
The results of the present study showed that the addition of 0.01 wt.% Ag-doped CNT fillers into dental GIC significantly improved the compressive strength. This finding may be attributed to the expected reinforcing effect of Ag-doped CNT fillers [17]. Moreover, the incorporation of the minute amount of the strong CNT nanofillers may be responsible for inhibiting crack propagation by transferring the stress from the weaker matrix to the stronger nanoparticle fillers without deterioration of the interfacial bonding [55]. These results are in accordance with previous studies that showed a reinforcement ability for dental restorations after incorporation of CNT [56]. However, these results disagree with the study conducted by Spinola et al., which reported that the incorporation of 1 wt.% CNT fillers had a negative effect on the compressive strength of glass ionomers, which may be due to the non-homogeneous distribution of the nanoparticle fillers and the consequent formation of voids [57].
Moreover, The increase in surface microhardness in the treaed groups can be referred to the homogenous dispersion of hard Ag-doped CNT filler nanoparticles within the matrix [58]. Both the control and modified groups exhibited similar solubility percentages; this finding may be explained by the small amount of Ag-doped CNT nanoparticle fillers added, which was not enough to improve the dissolution of the matrix. Furthermore, the incorporation of Ag-doped CNT nanoparticle fillers improved the antibacterial effect of the treated groups. This finding may be due to the fact that Ag nanoparticles displayed powerful bactericidal activity against Streptococcus mutans by rupturing their outer cellular membrane [59, 60]. Additionally, multi-walled CNT exhibit potent antibacterial properties and have the ability to penetrate bacterial cell walls [61]. Moreover, other aspects could have a significant impact on the mechanical characteristics of GICS, such as the depth of cure [62, 63]. Therefore, future studies are needed, taking into careful account also these variables.
The present study's limitation is that the experimental conditions did not completely replicate clinical ones. However, all the specimens were subjected to the same testing conditions. Further studies are recommended to assess the effect of the incorporation of Ag-doped CNT to GIC in different concentrations in order to recognize the optimum concentrations required to improve the mechanical properties. Moreover, it is recommended to investigate the color changes associated with each concentration.
Conclusions
The innovatively reinforced GIC with 0.01 wt.% Ag doped CNT fillers had the opportunity to be used as an alternative to conventional GIC dental cements as it provides enhanced compressive strength, surface microhardness, and anti-bacterial activity against Streptococcus mutans compared to the conventional GIC.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are not publicly available due to institutional policy but are available from the corresponding author on reasonable request.
Abbreviations
- GICs:
-
Glass ionomer cements
- CNTs:
-
Carbon nanotubes
- Ag:
-
Silver
- wt.%:
-
weight percent
- MREC:
-
Medical Research Ethical Committee
- NRC:
-
National Research Centre
- XRF:
-
X-ray fluorescence
- VHN:
-
Vickers microhardness number
- EMCC:
-
The Egypt Microbial Culture Collection
- BHI:
-
Brain Heart Infusion
- MPa:
-
Megapascal
References
Rokaya D, Srimaneepong V, Sapkota J, Qin J, Siraleartmukul K, Siriwongrungson V. Polymeric materials and films in dentistry: An overview. J Adv Res. 2018;14:25–34.
Abdelraouf RM. Chemical analysis and microstructure examination of extended-pour alginate impression versus conventional one (characterization of dental extended-pour alginate). Int J Polym Mater Polym Biomater. 2018;67:612–8.
Abdelraouf RM, Bayoumi RE, Hamdy TM. Effect of powder/water ratio variation on viscosity, tear strength and detail reproduction of dental alginate impression material (In vitro and clinical study). Polymers (Basel). 2021;13:1–11.
Abdelraouf RM, Mohammed M, Abdelgawad F. Evaluation of shear-bond-strength of dental self-adhering flowable resin-composite versus total-etch one to enamel and dentin surfaces: An in-vitro study. Open Access Maced J Med Sci. 2019;7:2162–6.
Torres C, Ávila D, Gonçalves LL, Meirelles L, Mailart MC, Di Nicoló R, et al. Glass Ionomer Versus Self-adhesive Cement and the Clinical Performance of Zirconia Coping/Press-on Porcelain Crowns. Oper Dent. 2021. https://doi.org/10.2341/20-229-C.
Hamdy TM. Interfacial microscopic examination and chemical analysis of resin-dentin interface of self-adhering flowable resin composite. F1000Research. 2017;6:1688.
Kampanas NS, Antoniadou M. Glass ionomer cements for the restoration of non-carious cervical lesions in the geriatric patient. J Func Biomater. 2018;9:1–9.
Sidhu S, Nicholson J. A Review of Glass-Ionomer Cements for Clinical Dentistry. J Funct Biomater. 2016;7:16.
Khoroushi M, Keshani F. A review of glass-ionomers: From conventional glass-ionomer to bioactive glass-ionomer. Dent Res J (Isfahan). 2013;10:411–20.
Francisconi LF, Scaffa PMC, de Barros VR dos SP, Coutinho M, Francisconi PAS. Glass ionomer cements and their role in the restoration of non-carious cervical lesions. J Appl Oral Sci. 2009;17: 364–9.
Cacciafesta V, Sfondrini MF, Baluga L, Scribante A, Klersy C. Use of a self-etching primer in combination with a resin-modified glass ionomer: Effect of water and saliva contamination on shear bond strength. Am J Orthod Dentofac Orthop. 2003;124:420–6.
Walia T, Brigi C, Ziadkhani MM, Khayat AA, Tabibzadeh Z. Retention force of glass ionomer based luting cements with posterior primary zirconium crowns - A comparative in vitro study. J Clin Pediatr Dent. 2021;45:259–64.
Moghimi M, Jafarpour D, Ferooz R, Bagheri R. Protective effect of a nanofilled resin-based coating on wear resistance of glass ionomer cement restorative materials. BMC Oral Health. 2022;22:1–7.
Jassal M, Mittal S, Tewari S. Clinical effectiveness of a resin-modified glass ionomer cement and a mild one-step self-etch adhesive applied actively and passively in noncarious cervical lesions: An 18-month clinical trial. Oper Dent. 2018;43:581–92.
Park EY, Kang S. Current aspects and prospects of glass ionomer cements for clinical dentistry. Yeungnam Univ J Med. 2020;37:169–78.
Abdelnabi A, Hamza NK, El-Borady OM, Hamdy TM. Effect of different formulations and application methods of coral calcium on its remineralization ability on carious enamel. Open Access Maced J Med Sci. 2020;8:94–9.
Nicholson JW, Sidhu SK, Czarnecka B. Enhancing the mechanical properties of glass-ionomer dental cements: A review. Materials. 2020;13.
Hamdy TM, Mousa SMA, Sherief MA. Effect of incorporation of lanthanum and cerium-doped hydroxyapatite on acrylic bone cement produced from phosphogypsum waste. Egypt J Chem. 2020;63:1823–32.
Hamdy TM, El-Korashy SA. Novel bioactive zinc phosphate dental cement with low irritation and enhanced microhardness. e-Journal Surf Sci Nanotechnol. 2018;16:431–5.
Ghosh M, Shetty S. Effect of Addition of Graphene and Carbon Nanotubes on Flexural Strength of Polymethylmethacrylate- A Comparative In-Vitro Study. J Evol Med Dent Sci. 2020;9:1494–9.
Hamdy T. Polymerization shrinkage in contemporary resin-based dental composites: A Review Article. Egypt J Chem. 2021;64:3087–92.
Hoyos-Palacio LM, Cuesta Castro DP, Ortiz-Trujillo IC, Botero Palacio LE, Galeano Upegui BJ, Escobar Mora NJ, et al. Compounds of carbon nanotubes decorated with silver nanoparticles via in-situ by chemical vapor deposition (CVD). J Mater Res Technol. 2019;8:5893–8.
Alhotan A, Abdelraouf RM, El-Korashy SA, Labban N, Alotaibi H, Matinlinna JP, et al. Effect of Adding Silver-Doped Carbon Nanotube Fillers to Heat-Cured Acrylic Denture Base on Impact Strength, Microhardness, and Antimicrobial Activity: A Preliminary Study. Polymers (Basel). 2023;15:1–15.
Castro-Rojas MA, Vega-Cantu YI, Cordell GA, Rodriguez-Garcia A. Dental applications of carbon nanotubes. Molecules. 2021;26:1–14.
El-Rashidy AA, Abdelraouf RM, Habib NA. Effect of two artificial aging protocols on color and gloss of single-shade versus multi-shade resin composites. BMC Oral Health. 2022;22:1–12.
Liu F, Wang X di, Du S yu. Production of gold/silver doped carbon nanocomposites for effective photothermal therapy of colon cancer. Sci Rep. 2020;10:1–9.
Paiva L, Fidalgo TKS, da Costa LP, Maia LC, Balan L, Anselme K, et al. Antibacterial properties and compressive strength of new one-step preparation silver nanoparticles in glass ionomer cements (NanoAg-GIC). J Dent. 2018;69:102–9.
Wawrzyńczak A, Kłos J, Nowak I, Czarnecka B. Surface Studies on Glass Powders Used in Commercial Glass-Ionomer Dental Cements. Molecules. 2021;26:5279.
ISO 113581. International Organization for Standardization: ISO 9917-1:2007. Dentistry - Water-based cements - Part 1. Int Organ Stand. 2015;10406–1(20):3–6.
American Society for Testing and Materials. ASTMC266–03: Standard test method for time and setting ofhydraulic-cement paste by Gilmore needles. PhiladelphiaASTM. 2000;2010(C):1–4.
Chen S, Cai Y, Engqvist H, Xia W. Enhanced bioactivity of glass ionomer cement by incorporating calcium silicates. Biomatter. 2016;6:e1123842.
Imataki R, Shinonaga Y, Nishimura T, Abe Y, Arita K. Mechanical and functional properties of a novel apatite-ionomer cement for prevention and remineralization of dental caries. Materials (Basel). 2019;12.
ANSI/ADA specification no. 66* for dental glass ionomer cements. J Am Dent Assoc. 1989;119:205.
Chaudhary S, Sinha AA, Showkat I. Comparative evaluation of compressive strength of conventional glass ionomer cement and glass ionomer cement modified with nano-particles. ~ 574 ~ Int J Appl Dent Sci. 2020;6:574–6.
Bilić-Prcić M, Šalinović I, Gurgan S, Vural UK, Krmek SJ, Miletić I. Effects of incorporation of marine derived hydroxyapatite on the microhardness, surface roughness, and fluoride release of two glass-ionomer cements. Appl Sci. 2021;11:1–8.
Singer L, Bierbaum G, Kehl K, Bourauel C. Evaluation of the flexural strength, water sorption, and solubility of a glass ionomer dental cement modified using phytomedicine. Materials (Basel). 2020;13:1–14.
Pastila P, Lassila LVJ, Jokinen M, Vuorinen J, Vallittu PK, Mäntylä T. Effect of short-term water storage on the elastic properties of some dental restorative materials-A resonant ultrasound spectroscopy study. Dent Mater. 2007;23:878–84.
Gonulol N, Ozer S, Sen TE. Water sorption, solubility, and color stability of giomer restoratives. J Esthet Restor Dent. 2015;27:300–6.
Balouiri M, Sadiki M, Ibnsouda SK. Methods for in vitro evaluating antimicrobial activity: A review. J Pharmaceut Anal. 2016;6:71–9.
Malhotra S, Bhullar KK, Kaur S, Malhotra M, Kaur R, Handa A. Comparative evaluation of compressive strength and flexural strength of GC Gold Hybrid, GIC conventional and resin-modified glass-ionomer cement. J Pharm Bioallied Sci. 2022;14:S214–6.
Bonifácio CC, Kleverlaan CJ, Raggio DP, Werner A, De Carvalho RCR, Van Amerongen WE. Physical-mechanical properties of glass ionomer cements indicated for atraumatic restorative treatment. Aust Dent J. 2009;54:233–7.
Banas JA, Drake DR. Are the mutans streptococci still considered relevant to understanding the microbial etiology of dental caries? BMC Oral Health. 2018. https://doi.org/10.1186/s12903-018-0595-2.
Zaazou MH, Zaki DY, Abdelnabi A, Hamdy TM, Saleh RS, Hassan SN, et al. Comparative evaluation of caries prevalence among group of Egyptian adolescents using DMFS and ICDASII methods: a cross-sectional study. BMC Oral Health. 2023;23:1–9.
Elreash AA, Hamama H, Eldars W, Lingwei G, Zaen El-Din AM, Xiaoli X. Antimicrobial activity and pH measurement of calcium silicate cements versus new bioactive resin composite restorative material. BMC Oral Health. 2019. https://doi.org/10.1186/s12903-019-0933-z.
Choe Y-E, Kim Y-J, Jeon S-J, Ahn J-Y, Park J-H, Dashnyam K, et al. Investigating the mechanophysical and biological characteristics of therapeutic dental cement incorporating copper doped bioglass nanoparticles. Dent Mater. 2022;38:363–75.
Ammar N, El-Tekeya MM, Essa S, Essawy MM, Talaat DM. Antibacterial effect and impact on caries activity of nanosilver fluoride and silver diamine fluoride in dentin caries of primary teeth: a randomized controlled clinical trial. BMC Oral Health. 2022. https://doi.org/10.1186/s12903-022-02697-y.
Zeidan NK, Enany NM, Mohamed GG, Marzouk ES. The antibacterial effect of silver, zinc-oxide and combination of silver/ zinc oxide nanoparticles coating of orthodontic brackets (an in vitro study). BMC Oral Health. 2022. https://doi.org/10.1186/s12903-022-02263-6.
Mirza EH, Khan AA, Al-Khureif AA, Saadaldin SA, Mohamed BA, Fareedi F, et al. Characterization of osteogenic cells grown over modified grapheneoxide-biostable polymers. Biomed Mater. 2019;14:065004.
Dyachkova TP, Tarov DV, Burakova EA, Tugolukov EN, Blokhin AN, Galunin EV, et al. Polymer composites based on functionalized carbon nanotubes. IOP Conf Ser Mater Sci Eng. 2019;693:012011.
Wang L, D’Alpino PHP, Lopes LG, Pereira JC. Mechanical properties of dental restorative materials: relative contribution of laboratory tests. J Appl Oral Sci. 2003;11:162–7.
Ivanišević A, Rajić VB, Pilipović A, Par M, Ivanković H, Baraba A. Compressive strength of conventional glass ionomer cement modified with tio2 nano-powder and marine-derived hap micro-powder. Materials (Basel). 2021;14:4964.
Zaytsev D. Mechanical properties of human enamel under compression: On the feature of calculations. Mater Sci Eng C. 2016;62:518–23.
G Paffenbarger. American Dental Association Specification No. 8 for Dental Zinc Phosphate Cement. J Am Dent Assoc Dent Cosm. 1937;24:2019–23.
Khajuria RR, Singh R, Barua P, Hajira N, Gupta N, Thakkar RR. Comparison of film thickness of two commercial brands of glass ionomer cement and one dual-cured composite: An in vitro study. J Contemp Dent Pract. 2017. https://doi.org/10.5005/jp-journals-10024-2104.
AlMufareh NA, AlQhtani FA, AlKhureif A. Comparing the effects of carbon- and silver oxide-particles on the physical and mechanical properties of glass-ionomer cements: An in vitro study. Mater Express. 2021. https://doi.org/10.1166/mex.2021.1894.
Kechagioglou P, Andriotis E, Papagerakis P, Papagerakis S. Multiwalled carbon nanotubes for dental applications. Methods Molecul Biol. 2019;1922:121–8.
Spinola M, Dal Piva AMO, Barbosa PU, Torres CRG, Bresciani E. Mechanical Assessment of Glass Ionomer Cements Incorporated with Multi-Walled Carbon Nanotubes for Dental Applications. Oral. 2021;1:190–8.
Moshaverinia M, Navas A, Jahedmanesh N, Shah KC, Moshaverinia A, Ansari S. Comparative evaluation of the physical properties of a reinforced glass ionomer dental restorative material. J Prosthet Dent. 2019. https://doi.org/10.1016/j.prosdent.2019.03.012.
Meneses ML, Recalde M, Martin PL, Pardo AG. Antifungal activity of silver nanoparticles and clotrimazole against Candida spp. Brazilian J Pharm Sci. 2022;58:1–11.
AlJindan R, AlEraky DM. Silver Nanoparticles: A Promising Antifungal Agent against the Growth and Biofilm Formation of the Emergent Candida auris. J Fungi. 2022;8:744.
Laganà P, Visalli G, Facciolà A, Ciarello MP, Laganà A, Iannazzo D, et al. Is the antibacterial activity of multi-walled carbon nanotubes (Mwcnts) related to antibiotic resistance? an assessment in clinical isolates. Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph18179310.
Colombo M, Gallo S, Poggio C, Ricaldone V, Arciola CR, Scribante A. New resin-based bulk-fill composites: In vitro evaluation of micro-hardness and depth of cure as infection risk indexes. Materials (Basel). 2020;13:1308.
Pieniak D, Walczak A, Walczak M, Przystupa K, Niewczas AM. Hardness and wear resistance of dental biomedical nanomaterials in a humid environment with non-stationary temperatures. Materials (Basel). 2020;13:1255.
Acknowledgements
Not applicable.
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
T. H. contributed to the conception and design of the study, collection of data, interpretation of the analyzed data, checked the data and results, writing the manuscript, revised and reviewed the draft manuscript, read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study received ethical approval from the Medical Research Ethical Committee (MREC) of National Research Centre (NRC); Cairo, Egypt (Reference number: 98072032023). All methods were performed in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hamdy, T.M. Evaluation of compressive strength, surface microhardness, solubility and antimicrobial effect of glass ionomer dental cement reinforced with silver doped carbon nanotube fillers. BMC Oral Health 23, 777 (2023). https://doi.org/10.1186/s12903-023-03542-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03542-6