
Abstract
Background
This study evaluated the effect of ceramic primers containing 10-methacryloyloxydecyl phosphate (10-MDP) and γ-methacryloxypropyl trimethoxysilane (γ-MPTS) agents on the shear bond strength (SBS) of CAD/CAM ceramics with different chemical structures and resin cement.
Methods
A total of 640 CAD/CAM ceramic specimens were obtained from Vita Mark II (VM), IPS E.max CAD (EM), Vita Suprinity (VS) and Vita Enamic (VE). The specimens were divided into two groups: etched with hydrofluoric acid (HF) and unetched. Each group was treated with a different ceramic primer (Clearfil Ceramic Primer Plus, G-Multi Primer and Monobond S), except for an untreated group (n = 10). After ceramic primers and resin cement were applied to each ceramic surface, half of the specimens were thermally aged at 10,000 cycles, 5–55 ± 1 °C, with a dwell time of 30 s. The SBS was tested with a universal testing machine at a 0.5 mm/min crosshead speed. Data were analysed by using statistical software (SPSS 20). Normal data distribution was checked with the Shapiro‒Wilk test. Three-way ANOVA was used to analyse the difference between the numeric data of the HF etched and thermally aged groups. A post hoc Tukey test was applied in the paired comparison of significant difference. The statistical significance level was accepted as p < 0.05.
Results
The highest SBS values were obtained in the HF etched G-Multi primer applied nonaged EM group (28.3 ± 2.62 MPa), while the lowest values were obtained in the nonetched and thermally aged EM group that received no treatment (2.86 ± 0.04 Mpa). The SBS significantly increased in all specimens on which the ceramic primer was applied (p < 0.001). Thermal ageing had a significant negative effect on the SBS values in all groups (p < 0.001).
Conclusion
The positive combined effects of the 10-MDP and γ-MPTS agents resulted in a significant increase in the bonding strength of the resin cement to the CAD/CAM ceramics. In addition, the increase in the amount of inorganic filler provided a favourable effect on durable adhesion.
Similar content being viewed by others

Background
Dental ceramics have been used for many years in dentistry practice. Expectations such as better aesthetics, function and biocompatibility in permanent restorations have increased the demand for all-ceramic systems [1]. Today, all-ceramic restorations with high aesthetic and mechanical characteristics can be manufactured in a shorter time using computer-aided design and computer-aided manufacturing (CAD/CAM) technology without requiring operations such as dental impression, wax patterning and casting technology [2, 3].
Feldspathic ceramic blocks, which are the first blocks manufactured for use in CAD/CAM systems, have been extensively used. Inadequate mechanical characteristics despite high biological compatibility and aesthetics have caused the development of new blocks from different materials with different characteristics and usage areas [4, 5]. To reinforce glass ceramics, leucite was initially added to their composition without corrupting their translucence, and leucite-reinforced glass ceramic blocks were manufactured [6]. Lithium disilicate-reinforced glass ceramics were manufactured due to the mechanical inadequacy of leucite-reinforced glass ceramics. Since lithium disilicate-reinforced glass ceramics did not have adequate mechanical strength in the posterior region, a certain amount of zirconium was added, and the fracture resistance of the lithium disilicate-reinforced glass ceramics was increased [6, 7]. However, new generation hybrid ceramic blocks were manufactured by adding polymers to ceramic structures since there were problems regarding repair due to their fragile structures [8].
A durable adhesion between tooth and restoration often eliminates the problems that may occur in the postoperative period [9, 10]. Cementation procedures of ceramic restorations are high technical sensitivity-demanding applications that take time and critically affect long-term success. Acquisition of a successful adhesion requires very high sensitivity in terms of technique and material [10, 11]. Therefore, pretreatments are performed to increase the bonding strength of the resin cement to both the restoration surface and dental tissues [12]. Organofunctional ceramic primer bonding agents are used to provide chemical bonding and adhesion between inorganic substrates and organic polymers that have different characteristics. Ceramic primer applications constitute an important step in adhesive cementation and can potentially affect adhesive bonding and thus clinical success. Different factors affect the bonding characteristics of ceramic primers [13].
When the current literature was evaluated, it was reported that 10-MDP has a strong effect on increasing the bond strength due to its ability to bond to various substrates [14]. In addition, the aim was to increase the bond strength to ceramic materials by adding γ-MPTS to some universal adhesives. Some researchers claim that the bond strength of γ-MPTS to glass ceramics remains low due to the presence of water, low pH and early hydrolysis. Many studies have reported that 10-MDP and γ-MPTS together strongly increase the bonding strength. Sone studies have noted that the bond strength may be adversely affected in the long term due to the negative effects of residual solvents in the adhesive layer and 10-MDP from water after thermal cycling [14, 15].
The aim of this study was to evaluate the effect of ceramic primers with different chemical contents on the SBS of CAD/CAM ceramics with resin cement after thermal ageing. The null hypotheses were that the ceramic primers (1) and ceramic types (2) would not have a significant effect on the bonding performance of etched and nonetched CAD/CAM ceramics with resin cement after thermal ageing.
Methods
A general description of the materials with their manufacturers and compositions are listed in Table 1.
A total of 640 CAD/CAM ceramic specimens (12 × 14 × 2 mm) were obtained from Vita Mark II (VM), IPS E.max CAD (EM), Vita Suprinity (VS) and Vita Enamic (VE) CAD/CAM blocks using a sensitive cutting device (IsoMet Low-speed; Buehler, USA). Ceramic discs were placed in a self-curing acrylic resin (Integra; BG Dental, Ankara, Turkey) using cylinder-shaped moulds with a diameter of 25 mm and height of 15 mm with one surface facing upwards. The specimens were carefully polished with 600-800-1000-1200 grit silicon carbide abrasive papers (SiC) to create standardized surfaces. The specimen surfaces were thoroughly rinsed with distilled water in an ultrasonic bath to remove contaminants. CAD/CAM ceramic specimens were classified into four groups according to the ceramic type, and half of each ceramic group was etched with 5% HF for 60 s, and the other half was not etched. Then, ceramic groups were further divided into 4 subgroups for ceramic primer pretreatment before cementation (n = 10):
Group 1; Control group
Group 2; Clearfil Ceramic Primer Plus group
Group 3; G-Multi Primer group
Group 4; Monobond-S Ceramic Primer group
Group 1 had no treatment, and Groups 2–4 were treated with Clearfil Ceramic Primer Plus, G-Multi Primer and Monobond-S Ceramic Primer, respectively, according to the manufacturer’s instructions. After the application of the ceramic primers, Panavia V5 (Kuraray Noritake Dental, Japan) dual curing adhesive resin cement was applied to the ceramic surface using a transparent plastic mould with a hole (3 mm diameter and 2 mm height). The specimens were polymerized for 10 s using a high-intensity blue LED curing unit (1500 mW/cm2; Premium Plus, UK LTD). Then, all specimens were stored in 100% humidity for 24 h prior to the thermal cycling procedure. To simulate the oral environment before the shear test, 10,000 thermal cycles were applied at 5–55 ºC with a waiting period of 30 s on half of the specimens. The SBSs were tested with a universal test machine (Shimadzu, Japan) at a crosshead speed of 0.5 mm/min. The shear-bond force was recorded in newtons, and the bond strength was calculated in MPa. Fracture surfaces were examined with a stereomicroscope (Olympus SZ-4045 ESD, Japan) at x30 magnification, and failure types were noted as adhesive, cohesive, or mixed. Ceramic surfaces were also examined after HF etching and shear testing by using a scanning electron microscope (SEM; Evo LS10, Zeiss, Germany) at x1000 and x5000 magnifications.
Data were analysed using statistical software (Statistical Package for the Social Sciences [SPSS], version 20, SPSS Inc, Chicago, IL, USA). Normal data distribution was checked with the Shapiro‒Wilk test. Three-way ANOVA was used to analyse the difference between the numeric data of the HF etched and thermally aged groups. A post hoc Tukey test was applied in the paired comparison of significant difference. The statistical significance level was accepted as p < 0.05.
Results
The three-way ANOVA results are given in Tables 2 and 3.
The ceramic primers, different ceramic materials, HF etching and thermal ageing were the main parameters studied, and the interactions of these parameters affected the SBS (P < 0.001). The highest effective factors on bonding were the HF etching and the ceramic primer (η2 = 0.856; η2 = 0.851, respectively) and the lowest effective factor was the ceramic material (η2 = 0.448) according to the HF etching groups; 93.4% of the bond strength was explained by the ceramic primers and ceramic materials. The ceramic materials had the highest effective factor on bonding ceramic primer (η2 = 0.855) and the lowest effective factor (η2 = 0.505) according to the thermal ageing groups; 91.7% of the bond strength was explained by ceramic primers and ceramic materials.
Descriptive statistical values of the specimen groups and multiple comparisons are shown in Tables 4 and 5.
A statistically significant difference was found for the SBS. When the main effects of the ceramic primers were examined, the SBS was 5.49 in the nontreated group, 15.97 in the group treated with G-Multi primer, 11.32 in the group treated with Monobond S and 14.32 in the group treated with Clearfil Plus according to HF etching. When the main effects of the ceramic primers were examined, the SBS was 5.67 in the nontreated group, 17.18 in the group treated with G-Multi primer, 12.89 in the group treated with Monobond S and 15.95 in the group treated with Clearfil Plus according to thermal ageing.
The highest SBS values were obtained in the HF etched G-Multi primer applied nonaged EM group (28.3 ± 2.62), while the lowest values were obtained in the nonetched and thermally aged EM group that received no treatment (2.86 ± 0.04). The SBS significantly increased in all specimens on which HF etched and ceramic primer was applied (p < 0.001). Thermal ageing significantly decreased the SBS values in all groups (p < 0.001). Higher bonding values were observed on the G-Multi Primer and Clearfil Plus applied ceramic materials than those on the Monobond S and nontreated groups. The graph of the bonding values of the material groups and ceramic primers is shown in Figs. 1 and 2.

Graph of the shear bond strength values (MPa) for ceramics, primers and HF etching

Graph of the shear bond strength values (MPa) for ceramics, primers and thermal ageing
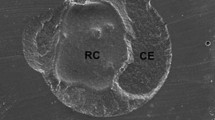
Ceramic surfaces are shown after HF etching in Fig. 3. Failure types are also shown in Fig. 4. Adhesive fractures were the most common failure type in the nontreated and thermally aged ceramics. The mixed and cohesive failure types were mainly obtained on G- Multi Primer applied surfaces, which contain 10-MDP and γ-MPTS.

SEM images of ceramic surface after HF etching (VM-A, EM-B, VS-C, VE-D)

SEM micrographs of failure types (Adhesive-A, Mixed-B, Cohesive-C)
Discussion
This study was conducted to evaluate the effect of surface pretreatment of CAD/CAM glass and hybrid ceramics with ceramic primers containing different chemical contents. According to the results, the lowest bonding values were obtained on the VE ceramics, while the highest values were obtained on EM ceramics. The lowest bond strength values were found in untreated groups, while the highest were found in the G-Multi Primer ceramic primer group. Therefore, the null hypotheses that ‘the ceramic primers (1) and ceramic types (2) would not have a significant effect on the bonding performance of etched and nonetched CAD/CAM ceramics to resin cement after thermal ageing’’ were disregarded.
The cement surface of CAD/CAM ceramic materials should be etched with 5% HF acid for a durable bond of resin cements to ceramics. Campos et al. [16] reported that a stronger bond strength between ceramics and resin cement formed after surface etching with HF acid. To dissolve the glassy matrix to increase the surface area and create better mechanical interlocking for the adhesives and resin cements, some studies recommend an increased etching time up to 60 s with HF [17,18,19]. It was observed that the bond strength of all ceramics etched with HF acid was significantly increased in this study.
Resin cements prevent the growth of cracks by penetrating the rough surfaces of ceramic base materials and microcracks and increase the fracture resistance of restorations [9]. Resin composite cements provide mechanical bonding by infiltrating the roughened ceramic surface and chemical bonding through ceramic primer application [20, 21]. Thus, acting together, the forces reaching the restoration are transferred in an effective and balanced way to the tooth tissue [22, 23]. Murillo-Gómez et al. [24] detected the lowest bond strength in the group that did not receive any bonding agent on the restoration surface in their study on dental ceramics. Chemical bonding with the least mechanical interlocking could be measured on ceramic surfaces that were not etched with HF and did not have any ceramic primer application; this could have potentially resulted in the lowest SBS values in unpretreated ceramics in our study. Apart from the control group, clinically acceptable bonding values were detected in all etched and pretreated ceramics.
Studies have shown that the bonding effect of bonding agents applied on restoration surfaces is related to the content of the material used. However, surface procedures and bonding agents certainly change the surface characteristics of the material and increase its bonding value. Different physical and chemical surface preparation operations are applied on ceramic surfaces. Studies have reported that suitable combinations of primers should be selected for the surface procedures applied on ceramics since ceramic primers have different chemical contents and bonding mechanisms [25]. Discussions in the literature question the effect of the ceramic primer bonding agent and the doctor’s application ability in the operations [24, 25].
Ceramic primer content applied in studies with the same composition as resin cement increases bonding. Koko et al. [26] investigated the bonding effect of PV5 resin cement to glass ceramic by adding different ratios of γ-MPTS to ceramic primers containing 1 wt% 10-MDP and observed that the addition of γ-MPTS up to 5% increased the bond strength. In another study, Dimitriadi et al. [27] noted that a silane primer (γ-MPTS containing) increased the hydrophobicity and bonding strength of the silane-containing bonding agent (10-MDP) with an etched ceramic surface. In this study, the highest bonding values were obtained for ceramics applied with G-Multi Primer and Clearfil Plus. This was most likely due to the presence of 10-MDP and γ-MPTS in the G-Multi primer and Clearfil Plus; our results support this deduction.
The acidic environment created by MDP increases its effectiveness by activating γ-MPTS. Thus, a stronger Si-O-Si connection is obtained by decreasing the contact angle on ceramic primer applied surfaces. In addition, MDP prevents the hydrolysis of γ-MPTS and provides a stronger bonding of more silane molecules to the glass phase. This mechanism is potentially the reason the bond strength is strongest in the G-Multi Primer applied group [26,27,28]. In our study, higher bonding values were measured in the EM and VS ceramic groups. This was potentially due to the stronger chemical interactions of the resin and lithium disilicate rather than their mechanical interlocking.
Various studies have shown that nonhomogeneous stresses develop at the bonding interface and extend into the substrate and the composite cement, thus leading to cohesive or mixed fractures. Clearly, the adhesive bond strength exceeds the intrinsic strength of the ceramics, leading to cohesive fractures [29, 30]. VS and EM as glass ceramics with reinforcing crystalline phases provide higher mechanical strength than VE and VM and thus demonstrate less cohesive/mixed fractures.
The lowest shear bonding values were found in the VE groups. The effect of acid etching on glass ceramics and hybrid ceramics is different due to their chemical structures. When hybrid ceramics are etched with acid, they cause dissolution in the inorganic matrix as well as the glass phase [31, 32]. Thus, it causes a decrease in bonding strength values. However, MDP and γ-MPTS have shown a positive effect on the bond strength of PV5 resin cement to hybrid VE ceramics [31]. Tokunaga et al. [33] applied MDP solution and a silane solution (containing γ-MPTS) to the ceramic surface and tested the bond strength of PV5 resin cement to VE ceramic. They reported that there was an increase in bond strength by applying MDP and an MDP-activated silane.
In our study, bond strength values decreased after thermal ageing in all groups. The decrease in bond strength was potentially due to hydrolysis of silicon-oxygen bonds at the ceramic-ceramic primer interface by water absorption. Some studies have shown that the water absorption increased with an increase in the ratio of TEGDMA and bis-GMA in the resin. It is possible that the presence of MDP and bis-GMA in the resin cements used in our study contributed to the acceleration of water absorption over time and affected the mechanical properties of resin cements after thermal ageing [34,35,36].
The tests applied in this study were not carried out in a real oral environment with constant temperature and pH changes. Since our study was conducted in a laboratory environment, it was not possible to fully reflect the clinical conditions. In our study, the main limitations are the application of shear force, the unmeasured restoration ligament strength under chewing forces, and the absence of a chewing simulator. Future research will be performed to study these limitations.
Conclusion
Ceramic primer agents containing 10-MDP and inorganic fillers increased the bonding strength. Increasing the amount of inorganic fillers inside ceramic materials could also improve the bond strength. In addition, 10-MDP prominently increased the effectiveness of γ-MPTS and created a stronger bond strength by improving silanization together. Micromechanical interlocking on ceramic surfaces etched with HF acid greatly contributed to increasing the adhesion quality. Thermal ageing caused negative effects on the bonding interface over time and decreased the bond quality over time.
Data Availability
The datasets used and/or analysed during the current study are available from corresponding author on reasonable request due to privacy reasons and large data size.
Abbreviations
- Bis-GMA:
-
Bisphenol A-glycidyl dimethacrylate
- TEGDMA:
-
Triethyleneglycol-dimethacrylate
- UDMA:
-
Urethane dimethacrylate
- γ-MPTS:
-
γ-methacryloxypropyl trimethoxysilane
- MDTP:
-
Methacryloyloxydecyl dihydrogen thiophosphate
- MDP:
-
Methacryloyloxydecyl dihydrogen phosphate
References
Moshaverinia A. Review of the modern dental ceramic restorative materials for esthetic dentistry in the minimally invasive age. Dent Clin. 2020;64(4):621–31.
Davidowitz G, Kotick PG. The Use of CAD/CAM in Dentistry. Dent Clin North Am. 2011;55:559–70.
Papadopoulos K, Pahinis K, Saltidou K, Dionysopoulos D, Tsitrou E. Evaluation of the surface characteristics of dental CAD/CAM materials after different surface treatments. Mater (Basel). 2020;13(4):981.
Coldea A, Swain MV, Thiel N. Mechanical properties of polymer-infiltrated-ceramic-network materials. Dent Mater 2013;29;419 – 26.
Elsaka SE. Bond strength of novel CAD/CAM restorative materials to self-adhesive resin cement: the effect of surface treatments. J Adhes Dent. 2014;16:531–40.
Gönüldaş F, Öztürk C, Atalay P, Öztaş D. Influence of different surface finishing techniques on machinable feldspathic and leucite-reinforced ceramics. Dent Mater J. 2019;38:317–22.
Fu L, Engqvist H, Xia W. Glass-ceramics in dentistry: a review. Mater (Basel). 2020;13(5):1049.
Demirel G, Baltacıoğlu IH. Influence of different universal adhesives on the repair performance of hybrid CAD-CAM materials. Restor Dent Endod. 2019;44(3):e23.
Blatz MB, Sadan A, Kern M. Resin-ceramic bonding: a review of the literature. J Prosthet Dent. 2003;89:268–74.
Venturini AB, Wandscher VF, Marchionatti AME, Evangelisti E, Ramos GF, Melo RM, Valandro LF. Effect of resin cement space on the fatigue behavior of bonded CAD/CAM leucite ceramic crowns. J Mech Behav Biomed Mater. 2020;110:103893.
Assunção Souza RO, da Silva NR, de Miranda LM, de Araújo GM, Duarte Moura DM, Medeiros Barbosa HA. Two-year follow-up of ceramic veneers and a full crown treated with self-etching ceramic primer: a case report. Oper Dent. 2020;45:352–8.
Lima RBW, Barreto SC, Hajhamid B, de Souza GM, de Goes MF. Effect of cleaning protocol on silica deposition and silica-mediated bonding to Y-TZP. Dent Mater. 2019;35:1603–13.
Dimitriadi M, Zafiropoulou M, Zinelis S, Silikas N, Eliades G. Silane reactivity and resin bond strength to lithium disilicate ceramic surfaces. Dent Mater. 2019;35:1082–94.
Att W, Dent M. Bonding durability between Zirconia and different types of tooth or Implant Abutments-A systematic review. Part II: outcomes of clinical studies. Int J Prosthodont. 2022;35:512–29.
Ye S, Lin JC, Kang LL, Li CL, Hou SS, Lee TL, Chuang SF. Investigations of silane-MDP interaction in universal adhesives: a ToF-SIMS analysis. Dent Mater. 2022;38(1):183–93.
Campos F, Almeida CS, Rippe MP, De Melo RM, Valandro LF, Bottino MA. Resin bonding to a hybrid ceramic: Effects of surface treatments and aging. Oper Dent. 2016;41:171–8.
Straface A, Rupp L, Gintaute A, Fischer J, Zitzmann NU, Rohr N. HF etching of CAD/CAM materials: influence of HF concentration and etching time on shear bond strength. Head & face med. 2019;15:1–10.
Veríssimo AH, Moura DMD, Tribst JPM, Araújo AMM, Leite FPP, Souza ROAE. Effect of hydrofluoric acid concentration and etching time on resin-bond strength to different glass ceramics. Braz Oral Res. 2019;33:e041.
Fonzar RF, Goracci C, Carrabba M, Louca C, Ferrari M, Vichi A. Influence of acid concentration and etching time on composite cement adhesion to lithium-silicate glass ceramics. J Adhes Dent. 2020;22(2):175–82.
Ho GW, Matinlinna JP. Insights on Ceramics as Dental materials. Part II. Chem Surf Treatments Silicon. 2011;3:117–23.
Salem RST, Ozkurt-Kayahan Z, Kazazoglu E. In vitro evaluation of shear bond strength of three primer/resin cement systems to monolithic zirconia. Int J Prosthodont. 2019;32(6):519–25.
Tian T, Tsoi JKH, Matinlinna JP, Burrow MF. Aspects of bonding between resin luting cements and glass ceramic materials. Dent Mater. 2014;30(7):e147–62.
Turgut S, Bagis B, Ayaz EA. Achieving the desired colour in discoloured teeth, using leucite-based cad-cam laminate Systems. J Dent. 2014;42:68–74.
Murillo-Gómez F, Rueggeberg FA, De Goes MF. Short- and long-term bond strength between resin cement and glass-ceramic using a silane-containing universal adhesive. Oper Dent. 2017;42:514–25.
Manso AP, Silva NRFA, Bonfante EA, Pegoraro TA, Dias RA, Carvalho RM. Cements and adhesives for all-ceramic restorations. Dent Clin North Am. 2011;55:311–32.
Koko M, Takagaki T, Abdou A, Inokoshi M, Ikeda M, Wada T, Uo M, Nikaido T, Tagami J. Effects of the ratio of silane to 10-methacryloyloxydecyl dihydrogenphosphate (MDP) in primer on bonding performance of silica-based and zirconia ceramics. J Mech Behav Biomed Mater 2020;112;104026.
Dimitriadi M, Petropoulou A, Vakou D, Zinelis S, Eliades G. In vitro evaluation of a silane containing self-adhesive resin luting agent. Dent Mater. 2023;39:181–91.
Koko M, Takagaki T, Abd El-Sattar NEA, Tagami J, Abdou A. MDP Salts: a New Bonding Strategy for Zirconia. J Dent Res. 2022;101(7):769–76.
Nguyen JF, Ruse D, Phan AC, Sadoun MJ. High-temperature-pressure polymerized resin-infiltrated ceramic networks. J Dent Res. 2014;93:62–7.
Özcan M, Vallittu PK. Effect of surface conditioning methods on the bond strength of luting cement to ceramics. Dent Mater. 2003;19:725–31.
Moura DMD, de Araújo AMM, de Souza KB, Veríssimo AH, Tribst JPM. de Assunção e Souza RO. Hydrofluoric acid concentration, time and use of phosphoric acid on the bond strength of feldspathic ceramics. Braz Oral Res 2020;34.
Ustun S, Ayaz EA. Effect of different cement systems and aging on the bond strength of chairside CAD-CAM ceramics. J Prost Dent. 2021;125(2):334–9.
Tokunaga E, Nagaoka N, Maruo Y, Yoshihara K, Nishigawa G, Minagi S. Phosphate group adsorption capacity of inorganic elements affects bond strength between CAD/CAM composite block and luting agent. Dent Mater J. 2021;40(2):288–96.
Lüthy H, Loeffel O, Hammerle CH. Effect of thermocycling on bond strength of luting cements to zirconia ceramic. Dent Mater. 2006;22(2):195–200.
Koko M, Takagaki T, Abdou A, Wada T, Nikaido T, Tagami J. Influence of 10-methacryloyloxydecyl dihydrogen phosphate (MDP) incorporated experimental cleaners on the bonding performance of saliva-contaminated zirconia ceramic. Clin Oral Invest. 2022;1785–95.
Massi Paschoalino V, Juste Paschoalino B, Özcan M, Luis Almeida de Carvalho R, de Carvalho RF, Al-Haj Husain N, Pessoa Pereira Leite F. Effect of different air-abrasion protocols on topography, surface wettability and adhesion of MDP monomer-based resin cement to zirconia. J Adhes Sci Technol. 2019;33(17):1948–58.
Acknowledgements
We acknowledge the Central Laboratory of Yuzuncu Yil University for cooperation in this study.
Funding
This study was not supported by any financial institution.
Author information
Authors and Affiliations
Contributions
All authors contributed equally to Conceptualization, Methodology, Formal analysis, Resources, Writing, Reviewing and Editing of the manuscript. Both authors read and approved the fnal manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics committee approval is not required for this in vitro study.
Conflict of Interest
The authors declare no conflict of interest.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Uğur, M., Kavut, İ., Tanrıkut, Ö.O. et al. Effect of ceramic primers with different chemical contents on the shear bond strength of CAD/CAM ceramics with resin cement after thermal ageing. BMC Oral Health 23, 210 (2023). https://doi.org/10.1186/s12903-023-02909-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-02909-z