
Abstract
Background
Obesity is the most important driver of non-alcoholic fatty liver disease (NAFLD); nevertheless, the relationship of weight-adjusted waist index (WWI), a new obesity index, with NAFLD is unclear.
Methods
This retrospective study used data from the NAGALA project from 1994 to 2016. WWI values were calculated using waist circumference (WC) and weight measurements of the participants. Three stepwise adjusted logistic regression models were developed to assess the relationship of WWI with NAFLD in the whole population and in both sexes. Additionally, we also conducted a series of exploratory analysis to test the potential impact of body mass index (BMI), age, smoking status and exercise habits on the association of WWI with NAFLD. Receiver operating characteristic (ROC) curves were used to estimate cut-off points for identifying NAFLD in the entire population and in both sexes.
Results
The current study included a population of 11,805 individuals who participated in health screenings, including 6,451 men and 5,354 women. After adjusting for all non-collinear variables in the multivariable logistic regression model, we found a significant positive correlation of WWI with NAFLD. For each unit increase in WWI, the risk of NAFLD increased by 72% in the entire population, by 84% in men, and by 63% in women. Furthermore, subgroup analyses revealed no significant discrepancies in the correlation of WWI with NAFLD across individuals with varying ages, exercise habits, and smoking status (all P-interaction > 0.05), except for different BMI groups (P-interaction < 0.05). Specifically, compared to the overweight/obese group, the relationship of WWI with NAFLD was significantly stronger in the non-obese group, especially in non-obese men. Finally, based on the results of ROC analysis, we determined that the WWI cut-off point used to identify NAFLD was 9.7675 in men and 9.9987 in women.
Conclusions
This study is the first to establish a positive correlation between WWI and NAFLD. Moreover, assessing the influence of WWI on NAFLD in individuals without obesity may yield more valuable insights compared to those who are overweight or obese.
Similar content being viewed by others


Background
NAFLD, the prevailing chronic liver disease globally, encompasses a range of liver conditions varying from uncomplicated steatosis to fibrosis [1,2,3]. As the metabolic syndrome manifestation in the liver, NAFLD is not only linked to the progression of liver cirrhosis and hepatocellular carcinoma but is also closely linked to the occurrence of cardiovascular diseases, chronic kidney disease, diabetes and malignancies [1, 4,5,6,7,8]. Alarming trends emerge as lifestyle shifts and obesity rates soar, causing a drastic surge in NAFLD prevalence. Relevant data showed an escalation from 25.3% (1990–2006) to 38.2% (2016–2019), impacting roughly one-third of the world's population [2]. This presents a significant challenge to healthcare systems [3, 9]. Therefore, NAFLD risk screening in the general population is very necessary.
As we all know, obesity is an important risk factor for NAFLD [3, 10, 11], and especially the existence of central obesity is closely related to the occurrence of NAFLD [1, 12]. Previously, various obesity-related indices have been widely used to identify or predict NAFLD. Many obesity indices, including the commonly used waist circumference (WC) and BMI, have been shown to be independently associated with NAFLD [13, 14]. However, it is important to note that BMI cannot differentiate fat distribution [15], and there are limitations in using BMI due to the influence of the "obesity paradox" [16,17,18,19]. Additionally, WC, although highly correlated with BMI, may not be suitable as a substitute for BMI [20].
WWI is a recently proposed new anthropometric index, which exhibits a weaker correlation with BMI and reduces the risk of the "obesity paradox" associated with BMI [21]. Furthermore, high WWI not only reflects both low muscle mass and high-fat mass in the body simultaneously [22], but also can be used to evaluate the subcutaneous and visceral fat area [23]. Previous studies have found strong associations of WWI with cardiovascular diseases, type 2 diabetes, hyperuricemia, and adult urinary protein excretion [21, 24,25,26,27,28,29]. However, the research on NAFLD and WWI is limited, with only one study published in May 2023 reporting an independent association between hepatic steatosis and WWI in a population of Americans [30]. Therefore, this study aimed to further explore the association of WWI with NAFLD using data from the NAGALA project.
Methods
Data source and study design
The data for current research was obtained from the NAGALA project. In summary, the NAGALA research project began in 1994 and recruited and collected data from the general population participating in the Human Dockyard Examination Program at the Murakami Memorial Hospital in Japan. The project's objective was to identify and evaluate long-term health conditions and associated risk elements. The study design has been described in more detail in other publications [31]. Additionally, the research data from the study has been made publicly available on the DRYAD public database by Okamura and colleagues [32]. In accordance with the Dryad Terms of Service, the data can be used for secondary analysis with new research hypotheses. It is important to note that the implementation of the NAGALA project was authorized by the Murakami Memorial Hospital Ethics Committee, and informed consent for data usage was obtained from each participant [31]. The current study is a post-hoc analysis based on the data from the NAGALA project, and the research protocol and design were authorized by Jiangxi Provincial People's Hospital Ethics Committee (IRB 2021–066).
This study’s purpose was to assess the relationship of NAFLD with WWI using the NAGALA dataset. With the new research hypothesis, we conducted a cross-sectional design and included 20,944 individuals who underwent medical examinations between 1994 and 2016. Among these individuals, we further excluded participants with a diagnosis of diabetes or liver disease (excepted fatty liver) at baseline, as well as those with FPG > 6.1 mmol/L, using medications, having the habit of drinking, and covariable data missing, resulting in a final analysis cohort of 11,805 participants (Fig. 1).

Flow chart for inclusion and exclusion of study participants
Data collection and measurements
Experienced healthcare professionals measured and recorded various anthropometric measurements of the participants, including WC, height, weight, and arterial blood pressure. BMI was calculated on the basis of weight and height. WWI was calculated as \(\frac{{\text{WC}}({\text{cm}})}{\sqrt{Weight(kg)}}\) [21].
Information on age, drinking status, sex, smoking status, and exercise habits was collected through a questionnaire. The classification of smoking status included individuals who were not smokers, those who used to be smokers, and individuals who were currently smokers. Exercise habits were determined based on engaging in any type of physical activity at least once per week.
After fasting for 8 h, venous blood samples were collected from the antecubital vein of the subjects and stored in siliconized glass tubes containing sodium fluoride. These samples were then centrifuged immediately and stored at -80 degrees Celsius until analysis. Blood tests were carried out using a modular analysis system (Hitachi High-Technologies Corp., Ltd., Tokyo, Japan), which involved measuring biochemical parameters such as high-density lipoprotein cholesterol (HDL-C), aspartate aminotransferase (AST), fasting plasma glucose (FPG), gamma-glutamyl transferase (GGT), total cholesterol (TC), alanine aminotransferase (ALT), and triglycerides (TG). According to the manufacturer's data, the coefficients of variation of the above biochemical parameters are 1.7%, 1.9%, 2.3%, 2.5%, 2.1%, 2%, 2.3% and 1.2%, respectively. Additionally, glycated hemoglobin A1c (HbA1c) was measured using high-performance liquid chromatography.
Evaluate NAFLD
The professional ultrasound technician examined the participants' abdomen by color ultrasound. To avoid selection bias, gastroenterologists did not have access to participants' clinical information when making the diagnosis. They evaluated several key items, including liver brightness, liver-kidney echo contrast, deep attenuation and vascular blurring based on abdominal ultrasonography, and made a diagnosis of NAFLD [33].
Statistical analysis
First, subjects were divided into 2 groups according to gender, and the distribution type of continuous variables was assessed using QQ plots. Categorical variables were shown in the baseline table as frequency (percentage), and continuous variables were shown as median (interquartile distance) or mean (standard deviation); Chi-square test, Mann–Whitney U test, and t-test were used for between-group comparisons.
Second, we used multivariate linear regression to assess the collinearity between WWI and covariates (Supplementary Table 1) [34], and then performed multivariate logistic regression models with stepwise adjustment of non-collinear variables to determine the relationship of NAFLD with WWI. The results were presented as ORs with 95% confidence intervals (CIs). Model 1 firstly made preliminary adjustments for sex, BMI and age. Model 2 further adjusted for participants' lifestyle habits (drinking status, smoking status, exercise habits). Model 3 included adjustments for all non-collinear variables. Subsequently, based on Model 3, we conducted four sensitivity analyses: Sensitivity-1 excluded participants with exercise habits at baseline, Sensitivity-2 excluded participants over 60 years old at baseline, Sensitivity-3 excluded participants with systolic/diastolic blood pressure ≥ 140/90 mmHg at baseline, and Sensitivity-4 only participants with baseline BMI less than 25 kg/m2 were included. Sensitivity-5 excluded patients with hypertriglyceridemia at baseline. After determining the association between WWI and NAFLD, we further used restricted cubic spline (RCS) to fit and visualize the association between WWI and NAFLD. It is noteworthy that, considering the significant differences between sexes in terms of body composition, shape, and energy metabolism [35], the aforementioned correlational analyses were conducted separately within the entire population and within each gender.
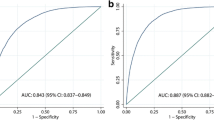
Third, we performed exploratory stratified logistic regression analysis to test the relationship of WWI with NAFLD in different ages, BMI, smoking status, and exercise habits subgroups and examined differences among subgroups using likelihood ratio tests. In addition, we also used the ROC curve to analyze the recognition value of WWI to NAFLD in the whole population, men and women, and calculated the corresponding area under the curve, cut-off point, sensitivity and specificity. Furthermore, we applied ROC curves to analyze the discriminative value of WWI for NAFLD in the entire cohort, as well as in males and females separately. This included calculating the area under the curve (AUC), cut-off points, sensitivity, and specificity for each respective group.
In this research, all data analyses were conducted using R software (version 3.4.3) and Empower Stats (version 2.0), and the significance standard was set to P < 0.05 (two-sided).
Results
Baseline information
Eleven thousand eight hundred five participants were eventually included in the current study, including 6,451 men and 5,354 women. Table 1 shows the baseline characteristics of the study population grouped by gender. It can be seen that at baseline, male participants had significantly higher levels of weight, height, BMI, WC, ALT, AST, GGT, TC, TG, FPG, SBP, DBP and lower levels of WWI and HDL-C than those of the female population. In addition, male participants had significantly more smoking habits and a significantly higher prevalence of NAFLD (30.31% vs 7.21%).
Association of WWI with NAFLD and sensitivity analysis
Significant positive correlations of NAFLD with WWI were observed in multivariate logistic regression models in all the whole population and men or women (Models 1–3) (Table 2). Although the associations weakened to some extent with stepwise adjustment of covariates, the positive correlation between WWI and NAFLD remained unchanged. After adjusting for all non-collinear variables, for every additional unit of WWI, the risk of NAFLD increased by 72% in the whole population, 84% in men and 63% in women.
Furthermore, based on Model 3, we carried out five sensitivity analyses. The sensitivity analysis results were consistent with the main results, indicating a significant positive correlation between WWI and NAFLD, with increasing NAFLD risk as WWI increased (Table 3). These findings further confirmed the relatively stable positive correlation of WWI with NAFLD.
Subgroup analysis
After confirming the relationship of WWI with NAFLD, we further explored the differences in this association among different subgroups; notably, stratified analysis was separately carried out in the whole population and in men and women. According to the common clinical cut-off points, we stratified BMI and age, while the stratification methods mentioned earlier were used for smoking status and exercise habits. The new analysis results (Table 4) found no significant differences in the relationship of WWI with NAFLD among different subgroups based on age, habits of exercise, and smoking status, except for different BMI groups (P-interaction < 0.05). Specifically, compared to the overweight/obese group (BMI ≥ 25 kg/m2), the correlation of NAFLD with WWI was higher in the non-obese group (BMI < 25 kg/m2).
Nonlinear association between WWI and NAFLD
Using RCS, we further modeled the dose–response relationship of WWI with NAFLD in the whole population and in both sexes. As shown in Fig. 2, after adjusting for all non-collinear variables, we observed that the positive trend between WWI and NAFLD risk remained unchanged. Individuals with higher levels of WWI had a stronger correlation with NAFLD compared to those with lower WWI levels. Furthermore, the RCS analysis indicated a non-linear relationship of NAFLD with WWI (All P for non-linearity: < 0.05). It can be observed that in the analysis of the whole population and for both sexes, the increasing trend of the correlation between WWI and NAFLD gradually slowed down when WWI was around 10.

Restricted cubic spline analysis of WWI for the estimation of the risk of NAFLD; A all population; B women; C men. Restricted cubic spline model adjusted for sex, age, height, BMI, drinking status, smoking status, exercise habits, ALT, AST, GGT, HDL-C, TC, TG, FPG, HbA1c and DBP. Note: Sex itself is not adjusted in the analysis based on gender stratification. NAFLD: non-alcoholic fatty liver disease; WWI: weight-adjusted waist index
ROC analysis
Table 5 presents the ROC analysis results of WWI for the identification of NAFLD. The findings revealed that the AUCs of WWI for detecting NAFLD in the entire population, males, and females were 0.6868, 0.7184, and 0.7631, respectively, with corresponding cut-off values of 9.7300, 9.7675, and 9.9987. Compared to the other groups, WWI demonstrated higher accuracy in identifying NAFLD in females, and also had a higher cut-off value.
Discussion
This observational study involving 11,805 subjects revealed a positive correlation of WWI with NAFLD. This association was consistent across different age groups, exercise habits and smoking status, except for different BMI groups. Notably, the relationship of WWI with NAFLD was stronger in the non-obese population compared to the overweight/obese population.
As far as we know, this is the first study investigating the relationship of WWI with NAFLD. Previous studies have shown that obesity as defined by the traditional obesity index BMI is closely related to the occurrence of NAFLD, and there is a significant dose-dependent relationship [13]. In recent years, with the in-depth study of obesity and NAFLD, people pay more attention to the role of central obesity in the occurrence and development of NAFLD, and people's concept has gradually changed to that central obesity is the key factor leading to the development of NAFLD [1, 12, 14, 35]. In the current study, we revealed an independent correlation between WWI, an index assessing central obesity, and NAFLD. For each unit increase in WWI, the risk of NAFLD increased by 72% in the entire population, by 84% in men, and by 63% in women.
WWI has attracted considerable attention as a novel obesity index since its introduction in 2018. Initially proposed by Park et al., WWI was developed to address the "obesity paradox" observed in cardiovascular disease associated with BMI, while accounting for the high correlation between WC and BMI. They standardized WC by body weight and demonstrated a linear correlation between WWI and cardiovascular-related diseases and mortality rates [21]. Subsequent studies have shown the efficacy of WWI in risk assessment for cardiovascular diseases [24,25,26] and its potential value in metabolic-related diseases, kidney diseases, and other areas [27,28,29]. Recently, Shen et al. investigated the association of WWI with liver fat deposition in Americans, further expanding the applications of WWI. They quantified liver fat deposition and fibrosis using vibration-controlled transient elastography and found a significant positive correlation of WWI with liver fat deposition. Moreover, by fitting the smooth curve, they also found a U-shaped nonlinear correlation of WWI with liver fibrosis, and on both sides of WWI equal to 10.92, the WWI-related liver fibrosis risk showed an opposite trend [30]. Building upon Shen et al.'s study, our research further evaluated the association of WWI with NAFLD, yielding significant positive associations. These findings provided further support for Shen et al.'s results [30], suggesting that WWI was a useful index for evaluating liver fat deposition. However, it is noteworthy that our study also identified a nonlinear relationship between WWI and NAFLD; whether in the entire population, men or women, there was a gradual attenuation of the positive association when WWI approached 10, which contrasted with Shen et al.'s findings.
The underlying mechanisms linking WWI and NAFLD remain unclear. Several possible explanations included: (i) WWI reflects central obesity, which actively contributes to adipocyte dysfunction, insulin resistance, and chronic inflammation, all of which further promote the development of NAFLD [10, 36]. (ii) WWI is positively correlated with the visceral fat area, and visceral fat, due to its unique anatomical location, releases metabolites that more easily reach the liver, thus affecting hepatic fat metabolism [37]. (iii) WWI reflects muscle mass reduction. Similar to the mechanisms of obesity, infiltration of adipose tissue into skeletal muscle is associated with insulin resistance and chronic inflammation, both of which contribute to NAFLD development [38, 39].
It is important to note that, in the current analysis subgroup of the research, whether in the whole population or in the men and women, the correlation between WWI and NAFLD was found to be particularly stronger in non-obese individuals. In fact, "lean-type" NAFLD has garnered increasing attention from scholars in recent years [40]. According to the report, about 40% of people with NAFLD worldwide are classified as non-obese, and nearly one in five of them are thin [41]. Researchers have conducted several studies in non-obese populations to explore the potential mechanisms underlying the susceptibility to NAFLD. These mechanisms may include: (i) genetic predisposition is considered the primary cause of "lean-type" NAFLD. The PNPLA3 gene has been identified as a genetic determinant of NAFLD, and lean individuals are more susceptible to the effects of PNPLA3 gene polymorphisms, increasing their likelihood of carrying risk alleles compared to overweight and obese individuals [42,43,44]. (ii) Diet is an important factor in NAFLD. Studies have found that lean individuals tend to consume more fructose and cholesterol, which will promote the occurrence of NAFLD [43, 44]. (iii) Other factors such as metabolic syndrome, disrupted gut microbiota, and decreased skeletal muscle mass and function have also been implicated in the formation of non-obese NAFLD [42,43,44]. It is noteworthy that non-obese NAFLD patients are not at low risk for overall mortality, cardiovascular-related mortality, or liver-related mortality [41, 45]. Therefore, while focusing on the obese population, attention should also be paid to the occurrence of NAFLD in non-obese individuals.
Strengths and limitations
Strengths
(i) For the first time, we found a correlation between a new obesity indicator, WWI, and NAFLD, and these findings can provide new insights into the risk management of NAFLD. (ii) WWI is easy to calculate and suitable for practical applications. Moreover, the NAGALA project's samples were drawn from a general health check-up population, and it had a sufficient sample size, making it applicable for promotion among ordinary people. (iii) This study employed rigorous statistical methods to adjust for non-collinear variables and performed four sensitivity analyses, indicating the reliability of the research findings.
Limitations
(i) The NAGALA study was conducted in a Japanese population, and further investigation is needed to determine its applicability in other regions or populations. (ii) This study was cross-sectional in nature and cannot establish a causal association of WWI with NAFLD. (iii) The diagnosis of NAFLD in this study was based on abdominal ultrasonography, which may underestimate liver fat content in some patients [46]. (iv) Although we included and controlled for known covariates, there still may be unmeasured confounding variables that could interfere with the conclusions of this study.
Conclusions
The current study demonstrated a positive and nonlinear association of WWI with NAFLD, with a more pronounced effect of WWI on NAFLD risk in non-obese individuals compared to overweight or obese individuals. These findings provided valuable new reference information for the risk assessment of NAFLD and added new evidence to its prevention.
Availability of data and materials
The data used in this study have been uploaded to the "Dryad" database by Professor Okamura et al. (https://doi.org/10.5061/dryad.8q0p192).
Abbreviations
- NAFLD:
-
Non-alcoholic fatty liver disease
- WWI:
-
Weight-adjusted waist index
- ROC:
-
Receiver operating characteristic
- TC:
-
Total cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- TG:
-
Triglyceride
- WC:
-
Waist circumference
- BMI:
-
Body mass index
- GGT:
-
γ-Glutamyl transferase
- AST:
-
Aspartate aminotransferase
- HbA1c:
-
Glycosylated hemoglobin A1c
- FPG:
-
Fasting glucose
- ALT:
-
Alanine aminotransferase
- OR:
-
Odds ratio
- CI:
-
Confidence intervals
- RCS:
-
Restricted cubic spline
References
Cotter TG, Rinella M. Nonalcoholic Fatty Liver Disease 2020: The State of the Disease. Gastroenterology. 2020;158:1851–64. https://doi.org/10.1053/j.gastro.2020.01.052.
Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77:1335–47. https://doi.org/10.1097/HEP.0000000000000004.
Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15:11–20. https://doi.org/10.1038/nrgastro.2017.109.
Kotronen A, Yki-Järvinen H. Fatty liver: a novel component of the metabolic syndrome. Arterioscler Thromb Vasc Biol. 2008;28:27–38. https://doi.org/10.1161/ATVBAHA.107.147538.
Tanase DM, Gosav EM, Costea CF, Ciocoiu M, Lacatusu CM, Maranduca MA, et al. The Intricate Relationship between Type 2 Diabetes Mellitus (T2DM), Insulin Resistance (IR), and Nonalcoholic Fatty Liver Disease (NAFLD). J Diabetes Res. 2020;2020:3920196. https://doi.org/10.1155/2020/3920196.
Targher G, Byrne CD, Tilg H. NAFLD and increased risk of cardiovascular disease: clinical associations, pathophysiological mechanisms and pharmacological implications. Gut. 2020;69:1691–705. https://doi.org/10.1136/gutjnl-2020-320622.
Lonardo A, Mantovani A, Targher G, Baffy G. Nonalcoholic Fatty Liver Disease and Chronic Kidney Disease: Epidemiology, Pathogenesis, and Clinical and Research Implications. Int J Mol Sci. 2022;23:13320. https://doi.org/10.3390/ijms232113320.
Wang Z, Zhao X, Chen S, Wang Y, Cao L, Liao W, et al. Associations Between Nonalcoholic Fatty Liver Disease and Cancers in a Large Cohort in China. Clin Gastroenterol Hepatol. 2021;19:788–796.e4. https://doi.org/10.1016/j.cgh.2020.05.009.
Perumpail BJ, Khan MA, Yoo ER, Cholankeril G, Kim D, Ahmed A. Clinical epidemiology and disease burden of nonalcoholic fatty liver disease. World J Gastroenterol. 2017;23:8263–76. https://doi.org/10.3748/wjg.v23.i47.8263.
Polyzos SA, Kountouras J, Mantzoros CS. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism. 2019;92:82–97. https://doi.org/10.1016/j.metabol.2018.11.014.
Quek J, Chan KE, Wong ZY, Tan C, Tan B, Lim WH, et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023;8:20–30. https://doi.org/10.1016/S2468-1253(22)00317-X.
Kim D, Touros A, Kim WR. Nonalcoholic Fatty Liver Disease and Metabolic Syndrome. Clin Liver Dis. 2018;22:133–40. https://doi.org/10.1016/j.cld.2017.08.010.
Li L, Liu DW, Yan HY, Wang ZY, Zhao SH, Wang B. Obesity is an independent risk factor for non-alcoholic fatty liver disease: evidence from a meta-analysis of 21 cohort studies. Obes Rev. 2016;17:510–9. https://doi.org/10.1111/obr.12407.
Pang Q, Zhang JY, Song SD, Qu K, Xu XS, Liu SS, et al. Central obesity and nonalcoholic fatty liver disease risk after adjusting for body mass index. World J Gastroenterol. 2015;21:1650–62. https://doi.org/10.3748/wjg.v21.i5.1650.
Romero-Corral A, Somers VK, Sierra-Johnson J, Thomas RJ, Collazo-Clavell ML, Korinek J, et al. Accuracy of body mass index in diagnosing obesity in the adult general population. Int J Obes (Lond). 2008;32:959–66. https://doi.org/10.1038/ijo.2008.11.
Horwich TB, Fonarow GC, Clark AL. Obesity and the Obesity Paradox in Heart Failure. Prog Cardiovasc Dis. 2018;61:151–6. https://doi.org/10.1016/j.pcad.2018.05.005.
Gravina G, Ferrari F, Nebbiai G. The obesity paradox and diabetes. Eat Weight Disord. 2021;26:1057–68. https://doi.org/10.1007/s40519-020-01015-1.
Fassio A, Idolazzi L, Rossini M, Gatti D, Adami G, Giollo A, et al. The obesity paradox and osteoporosis. Eat Weight Disord. 2018;23(3):293–302. https://doi.org/10.1007/s40519-018-0505-2.
Curcic IB, Berkovic MC, Kuna L, Roguljic H, Smolic R, Varzic SC, et al. Obesity Paradox in Chronic Liver Diseases: Product of Bias or a Real Thing? J Clin Transl Hepatol. 2019;7:275–9. https://doi.org/10.14218/JCTH.2019.00029.
Mahmoud I, Al-Wandi AS, Gharaibeh SS, Mohamed SA. Concordances and correlations between anthropometric indices of obesity: a systematic review. Public Health. 2021;198:301–6. https://doi.org/10.1016/j.puhe.2021.07.042.
Park Y, Kim NH, Kwon TY, Kim SG. A novel adiposity index as an integrated predictor of cardiometabolic disease morbidity and mortality. Sci Rep. 2018;8:16753. https://doi.org/10.1038/s41598-018-35073-4.
Kim NH, Park Y, Kim NH, Kim SG. Weight-adjusted waist index reflects fat and muscle mass in the opposite direction in older adults. Age Ageing. 2021;50:780–6. https://doi.org/10.1093/ageing/afaa208.
Kim JY, Choi J, Vella CA, Criqui MH, Allison MA, Kim NH. Associations between Weight-Adjusted Waist Index and Abdominal Fat and Muscle Mass: Multi-Ethnic Study of Atherosclerosis. Diabetes Metab J. 2022;46:747–55. https://doi.org/10.4093/dmj.2021.0294.
Ding C, Shi Y, Li J, Li M, Hu L, Rao J, et al. Association of weight-adjusted-waist index with all-cause and cardiovascular mortality in China: A prospective cohort study. Nutr Metab Cardiovasc Dis. 2022;32(5):1210–7. https://doi.org/10.1016/j.numecd.2022.01.033.
Zhang D, Shi W, Ding Z, Park J, Wu S, Zhang J. Association between weight-adjusted-waist index and heart failure: Results from National Health and Nutrition Examination Survey 1999–2018. Front Cardiovasc Med. 2022;9:1069146. https://doi.org/10.3389/fcvm.2022.1069146.
Zhao P, Shi W, Shi Y, Xiong Y, Ding C, Song X, et al. Positive association between weight-adjusted-waist index and hyperuricemia in patients with hypertension: The China H-type hypertension registry study. Front Endocrinol (Lausanne). 2022;13:1007557. https://doi.org/10.3389/fendo.2022.1007557.
Yu S, Wang B, Guo X, Li G, Yang H, Sun Y. Weight-Adjusted-Waist Index Predicts Newly Diagnosed Diabetes in Chinese Rural Adults. J Clin Med. 2023;12:1620. https://doi.org/10.3390/jcm12041620.
Li Q, Qie R, Qin P, Zhang D, Guo C, Zhou Q, et al. Association of weight-adjusted-waist index with incident hypertension: The Rural Chinese Cohort Study. Nutr Metab Cardiovasc Dis. 2020;30:1732–41. https://doi.org/10.1016/j.numecd.2020.05.033.
Qin Z, Chang K, Yang Q, Yu Q, Liao R, Su B. The association between weight-adjusted-waist index and increased urinary albumin excretion in adults: A population-based study. Front Nutr. 2022;9:941926. https://doi.org/10.3389/fnut.2022.941926.
Shen Y, Wu Y, Fu M, Zhu K, Wang J. Association between weight-adjusted-waist index with hepatic steatosis and liver fibrosis: a nationally representative cross-sectional study from NHANES 2017 to 2020. Front Endocrinol (Lausanne). 2023;14:1159055. https://doi.org/10.3389/fendo.2023.1159055.
Okamura T, Hashimoto Y, Hamaguchi M, Obora A, Kojima T, Fukui M. Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: a population-based longitudinal study. Int J Obes (Lond). 2019;43:139–48. https://doi.org/10.1038/s41366-018-0076-3.
Okamura T, et al. Data from: Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: a population-based longitudinal study. Dryad, Dataset. 2019. https://doi.org/10.5061/dryad.8q0p192.
Hamaguchi M, Kojima T, Itoh Y, Harano Y, Fujii K, Nakajima T, et al. The severity of ultrasonographic findings in nonalcoholic fatty liver disease reflects the metabolic syndrome and visceral fat accumulation. Am J Gastroenterol. 2007;102:2708–15. https://doi.org/10.1111/j.1572-0241.2007.01526.x.
Kim JH. Multicollinearity and misleading statistical results. Korean J Anesthesiol. 2019;72:558–69. https://doi.org/10.4097/kja.19087.
Ballestri S, Nascimbeni F, Baldelli E, Marrazzo A, Romagnoli D, Lonardo A. NAFLD as a Sexual Dimorphic Disease: Role of Gender and Reproductive Status in the Development and Progression of Nonalcoholic Fatty Liver Disease and Inherent Cardiovascular Risk. Adv Ther. 2017;34(6):1291–326. https://doi.org/10.1007/s12325-017-0556-1.
Fujii H, Kawada N, Japan Study Group Of NafldJsg-Nafld. The Role of Insulin Resistance and Diabetes in Nonalcoholic Fatty Liver Disease. Int J Mol Sci. 2020;21:3863. https://doi.org/10.3390/ijms21113863.
Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update. Physiol Rev. 2013;93:359–404. https://doi.org/10.1152/physrev.00033.2011.
Kim JA, Choi KM. Sarcopenia and fatty liver disease. Hepatol Int. 2019;13(6):674–87. https://doi.org/10.1007/s12072-019-09996-7.
De Fré CH, De Fré MA, Kwanten WJ, Op de Beeck BJ, Beeck BJ, Van Gaal LF, Francque SM. Sarcopenia in patients with non-alcoholic fatty liver disease: is it a clinically significant entity? Obes Rev. 2019;20:353–63. https://doi.org/10.1111/obr.12776.
Seto WK, Yuen MF. Nonalcoholic fatty liver disease in Asia: emerging perspectives. J Gastroenterol. 2017;52:164–74. https://doi.org/10.1007/s00535-016-1264-3.
Ye Q, Zou B, Yeo YH, Li J, Huang DQ, Wu Y, et al. Global prevalence, incidence, and outcomes of non-obese or lean non-alcoholic fatty liver disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2020;5(8):739–52. https://doi.org/10.1016/S2468-1253(20)30077-7.
Chan WK. Comparison between obese and non-obese nonalcoholic fatty liver disease. Clin Mol Hepatol. 2023;29:S58–67. https://doi.org/10.3350/cmh.2022.0350.
Patel AH, Peddu D, Amin S, Elsaid MI, Minacapelli CD, Chandler TM, et al. Nonalcoholic Fatty Liver Disease in Lean/Nonobese and Obese Individuals: A Comprehensive Review on Prevalence, Pathogenesis, Clinical Outcomes, and Treatment. J Clin Transl Hepatol. 2023;11:502–15. https://doi.org/10.14218/JCTH.2022.00204.
Kim D, Kim WR. Nonobese Fatty Liver Disease. Clin Gastroenterol Hepatol. 2017;15:474–85. https://doi.org/10.1016/j.cgh.2016.08.028.
Xu R, Pan J, Zhou W, Ji G, Dang Y. Recent advances in lean NAFLD. Biomed Pharmacother. 2022;153:113331. https://doi.org/10.1016/j.biopha.2022.113331.
Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2018;67:328–57. https://doi.org/10.1002/hep.29367.
Acknowledgements
Thanks to Professor Okamura and his team for contributing available research data.
Funding
This study was supported by the Natural Science Foundation of Jiangxi Province [No. 20232BAB216004 to YZ].
Author information
Authors and Affiliations
Contributions
GT-S, YZ, CH-Y, MB-K and SM-H conceived the research, drafted the manuscript, and did the statistical analysis. XH and CW are responsible for curation and validation of study data. YZ revised the manuscript and designed the study. All authors read and approved the final manuscript. YZ and GT-S are the guarantors and, as such, had full access to the data and take responsibility for its integrity and accuracy.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The NAGALA project was authorized by the Murakami Memorial Hospital Ethics Committee, and informed consent for data usage was obtained from each participant. The current study is a post-hoc analysis based on the data from the NAGALA project, and the research protocol and design were authorized by Jiangxi Provincial People's Hospital Ethics Committee (IRB 2021–066). We confirm that all methods were carried out in accordance with relevant guidelines and regulation under the ‘Ethics approval and consent to participate’ in the declaration section of the manuscript.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Collinearity diagnostics steps.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yu, C., He, S., Kuang, M. et al. Association between weight-adjusted waist index and non-alcoholic fatty liver disease: a population-based study. BMC Endocr Disord 24, 22 (2024). https://doi.org/10.1186/s12902-024-01554-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-024-01554-z