
Abstract
Background
Dietary indices and scores are valuable predictive markers against chronic diseases. Several previous studies have revealed the beneficial effects of diabetes risk reduction score (DRRS) against diabetes and cancer incidence. However, its association with metabolic abnormalities among obese individuals have not been revealed before. In the current study, we aimed to investigate the association between DRRS and metabolic risk factors among obese individuals.
Methods
In the current cross-sectional study, 342 obese individuals [Body mass index (BMI) ≥ 30 kg/m2] aged 20–50 years were included. Dietary intake was assessed by a validated semi-quantitative food frequency questionnaire (FFQ) of 168 food items and DRRS was calculated. Metabolic syndrome (MetS) was defined based on the guidelines of the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III). Enzymatic methods were used to assess serum lipids, glucose, and insulin concentrations. Blood pressure was measured by a sphygmomanometer and body composition with bioelectrical impedance analysis (BIA).
Results
Those with a higher adherence to DRRS had a significantly higher intake of energy, fiber, and lower protein compared with those in the lower quartiles. Moreover, lower intakes of trans fats, meat, sugar sweetened beverages (SSB), and glycemic index (GI) with higher intakes of fruits, cereal fiber, polyunsaturated fatty acids/ saturated fatty acids (PUFA/ SFA) ratio, coffee, and nuts were observed in the highest versus lowest DRRS categories. Lower systolic blood pressure, diastolic blood pressure, triglyceride and, higher high-density lipoprotein values were observed in higher DRRS categories. Logistic regression analysis showed that hypertension was significantly associated with adherence to DRRS among obese individuals, the odds ratio (OR) was 0.686 (95% confidence interval [CI], 0.26–0.84) after adjustment for potential confounders. But the risk of other components of MetS was not significantly associated with higher quartiles of adherence to DRRS. Also, a non-significantly lower prevalence of MetS was observed in the higher quartile of DRRS.
Conclusions
According to the results of the current study, higher DRRS was associated with lower blood pressure, modified serum lipids, and lower Mets prevalence. Further studies in different populations are warranted for better generalization of the obtained findings.
Similar content being viewed by others


Introduction
Obesity is one of the most important health concerns in the world and is associated with numerous co-morbidities; obesity is associated with reduced quality of life [1,2,3], increased risk of mental illness and psychological problems [4,5,6,7], alongside with increased weight self-stigma and body image dissatisfaction and distortion [8,9,10]. Also, obese individuals are at greater risk of non-communicable metabolic diseases like type 2 diabetes [11, 12], metabolic syndrome (MetS) [13, 14], cardiovascular disorders [15,16,17], kidney problems [18, 19], and most types of cancers [20,21,22]. Lifestyle modification including changes in dietary behaviors and physical activity schedule is one of the most important preventive and therapeutic approaches against obesity [23,24,25]; in recent years numerous dietary interventions for obesity treatment have been developed and multiple dietary indices for obesity prevention and prediction of obesity-related disorders have been proposed including dietary quality indices [26, 27], dietary inflammatory index [28], dietary diversity score [29, 30], and dietary antioxidant capacity [31], or special dietary regimens (e.g. Mediterranean dietary pattern [32], or MIND diet [33], etc.
These dietary indices are focusing on a particular aspect of diet; for example, dietary antioxidant capacity focuses on the antioxidant potential of diet or dietary diversity score, mostly considers the diversity of food items that one consumes. However, dietary scores that are focusing on the disease-diet associations are most important and useful, because they are taking a direct potential of one’s diet in increasing the risk of a special disease into account; the diabetes risk reduction score (DRRS) is a newly developed index, first introduced by Rhee JJ et al. [34], as a combined score of several dietary components that are recently been found to be associated with risk of type 2 diabetes, these food components include red and processed meats, nuts, coffee and sugar-sweetened beverages (SSBs), glycemic index (GI), cereal fiber, polyunsaturated fatty acid to the saturated fatty acid ratio (P:S), and trans fats. Based on the DRRS components, this diet is generally high in phenolic compounds, antioxidant vitamins and minerals, and antioxidant nutrients, also DRRS contains a lot of unsaturated fatty acids, which may have anti-inflammatory, antioxidant, and anti-atherogenic properties, So adopting a diet with diabetes risk reduction features may lower the risk of developing cardio-metabolic risk factors including insulin resistance [35]. Regarding the DRRS's anti-inflammatory components, the improvement in insulin and leptin sensitivity and decreased inflammation state favor the effects of alpha-melanocyte stimulating hormone (α-MSH) on controlling appetite, increasing satiety, and increasing energy expenditure [36]. Additionally, agouti-related peptide (AgRP) is an endogenous antagonist of α-MSH, and the secretory activity of AgRP neurons is controlled by inflammatory signals [37,38,39]. A limited number of studies have been performed regarding the DRRS and disease association; such as risk of type 2 diabetes [34], breast cancer, pancreatic cancer, and hepatocellular carcinoma [40,41,42,43]. In addition, in a study of Iran, a negative association between higher adherence to DRRS and components of metabolic syndrome has been revealed [35]; again, the same authors identified same results in patients with chronic kidney diseases (CKD) [44]. As mentioned above, there are limited number of studies showing the beneficial effects of higher adherence to DRRS and incident metabolic disorders; and further studies should be performed to identify its possible beneficial effects in different disease statuses. Moreover, obesity is a chronic situation that leads to numerous co-morbidities and it is essential to study the preventive role of diet. By evaluation of the relationship between DRRS and cardio-metabolic risk factors, it can be stated that whether adherence to DRRS with sufficient intake of healthy dietary factors in reduced intake of diabetes-triggering food items can be associated with reduced occurrence of cardiovascular disease risk factors and the consequent prevention of chronic diseases? In the current cross-sectional study, we evaluated the associations between higher adherence to DRRS and cardiovascular risk factors including serum lipids, glycemic markers, and indicators of insulin resistance and inflammatory response among obese individuals.
Methods and materials
Participants
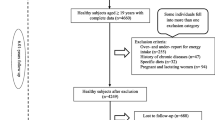
The participants of the current cross-sectional study were those who participated in two previous projects, including 342 obese individuals (57.9% males and 41.5% females) [45,46,47]. Study subjects were invited by public announcements from both Tabriz and Tehran cities and were aged between 20 to 50 years old with a body mass index (BMI) of more than 30 kg/m2. The exclusion criteria included: being pregnant, lactating, menopause, having recent bariatric surgery, or any cardiovascular disorders, cancers, hepatic and renal diseases, diabetes mellitus, and taking any weight-affecting medications. Full-informed approved written consent was taken from all of the participants and the study proposal was approved by the Ethics Committee of Tabriz University of Medical Sciences, Tabriz, Iran (registration code: IR.TBZMED.REC.1398.460 and IR. TBZMED.REC.1396.768).
General characteristics and anthropometric assessments
Socio-demographic information including sex, age, smoking status, education attainment, marital status, occupation, medical histories, and family size were obtained via a questionnaire; then, socioeconomic status (SES) score was calculated [47]. SES was determined using the information about educational status, occupational position, home ownership, and family size. Education was considered as a categorical variable in the current study, while individuals were asked to mention their highest degree of educational attainment. This variable was graded on a 5-point scale ranging from 0 to 5. (Illiterate: 0, less than diploma: 1, diploma and associate degree: 2, bachelors: 3, masters: 4 and higher: 5). The occupational class of female subjects were divided into five categories (housewife, employee, student, self-employed and others). Male individuals' occupational status was classified as follows: 1 unemployed, 2 workers, 2 farmers and ranchers, 3 others, 4 employees, and 5 self-employed. As a result, participants were classified as 3, 4, or 6 in terms of family size. Furthermore, if they were a renter or a landlord, they were assigned a score of 1 or 2. Following, each participant was assigned a score between zero and 15 for their overall SES score, and individuals were divided into three categories based on SES tertiles: low, middle, and high. Participants' physical activity levels were assessed using a shortened version of the International Physical Activity Questionnaire (IPAQ) [48]. Body composition measurements were done by the bioelectrical impedance analysis (BIA) method (Tanita, BC-418 MA, Tokyo, Japan). Height and weight were measured using a wall-mounted stadiometer and a Seca scale (Seca co., Hamburg, Germany) to the nearest 0.5 cm and 0.1 kg respectively. Waist circumference (WC) was measured at the midpoint between the lower costal margin and the iliac crest using a tape measure to the nearest 0.1 cm while hip circumference (HC) was measured over the widest part of the buttocks and was recorded to the nearest 0.1 cm. BMI and waist-to-hip ratio (WHR) were calculated. Blood pressure was measured with a standard mercury sphygmo-manometer twice in the same arm after at least 15 min of rest and then the mean of the two measurements was used for analysis. MetS was defined according to the National Cholesterol Education- Adult Treatment Panel (NCEP-ATP)- III criteria [49].
Dietary assessments
Dietary information was collected using a validated semi-quantitative food frequency questionnaire (FFQ), adapted for the Iranian population [50]. The FFQ was a list of frequently consumed food items with specified serving sizes in Iran. The participants were asked to state whether they consumed each food item daily, weekly, monthly, or yearly, as well as how often and how much using the general standard portion sizes, cooking yields, and edible food portions provided in the Iranian household manual [51]. Each food item's reported frequency was converted to a daily intake. Using common measurements, portion amounts of consumed items were converted to grams. For instance, one slice of Taftoon bread, a typical Iranian bread, measuring 10 by 10 cm, equals 15 g.
The DRRS was calculated from nine dietary factors; diabetes- protective food items were assigned in ascending order and the diabetes-triggering factors were assigned in descending order to compose the final DRRS. Diabetes-protective food items included coffee (either caffeinated or decaffeinated), cereal fiber, nuts, whole fruits, and polyunsaturated to saturated fat ratio while the diabetes-triggering factors included GI, trans fats, SSBs/fruit juices, and meats (red and processed). As previously suggested by Kang JH et al. [40], total fruits were added as a diabetes-protective factor and combined fruit juices with SSBs as one adverse factor. For each of the nine dietary factors, we assigned for each participants a quintile value ranging from 1 (consistent with the highest type 2 diabetes risk) to 5 (consistent with the lowest type 2 diabetes risk). From the sum of these quintile values, the final DRRS is obtained. The final DRRS ranged from 9 to 45 while the higher scores denote higher adherence to the diabetes risk reduction diet.
Biochemical assessment
10 ml venous blood samples were obtained from each individual and blood samples were centrifuged at 4500 rpm for 10 min to separate sera and plasma samples. Serum total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and fasting blood sugar (FBS) were evaluated using commercial kits (Pars Azmoon, Tehran, Iran). Furthermore, the low-density lipoprotein cholesterol (LDL-C) level was estimated by the Friedewald equation [26]. Enzyme-linked immunosorbent assay kits were used to measure serum insulin concentrations (Bioassay Technology Laboratory, Shanghai Korean Biotech, Shanghai City, China). Homeostatic model assessment for insulin resistance (HOMA-IR) was calculated as follows: fasting insulin (μ IU/ml) × fasting glucose (mmol/l) /22.5. Plasma agouti-related peptide (Ag-RP) and α-melanocyte-stimulating hormone (α-MSH) were assessed using enzyme-linked immunosorbent assay kits (Bioassay Technology Laboratory, China).
Statistical analyses
Statistical analysis of the data was performed using Statistical Package for Social Sciences (version 21.0; SPSS Inc, Chicago IL) at a statistical significance level of < 0.05. Data are presented as frequency (%) for categorical variables and median ± interquartile range (IQR) for continuous variables. The differences in discrete and continuous variables across different quartiles of dietary DRRS were compared using the chi-square test and one-way ANOVA respectively. Analysis of covariance (ANCOVA) was used for the comparison of biochemical variables after adjustment for confounders (age, sex, BMI, physical activity, and energy intake). Also adjustment for mentioned potential confounders was performed for comparison of dietary intakes of study participants by dietary DRRS quartiles. Chi-square was used to test the trends of MetS’ prevalence and linear regression analysis was used for trend analysis of biochemical parameters across different DRRS quartiles. Logistic regression analysis was performed to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) of the risk of MetS components across dietary DRRS quartiles after adjustment for BMI and total energy intake.
Results
The current cross-sectional study was conducted among 342 obese individuals (median BMI of 33.9 kg/m2) which includes 58% male and 42% female (median age of 38 years old). The results are presented in Tables 1, 2, 3 and 4. Table 1 shows the general characteristics of study participants according to DRRS categories. Women and those with higher BMIs were more likely to be at higher categories of DRRS. Other characteristics were not significantly different between different DRRS quartiles (P > 0.05). Tables 2 and 3 present the comparison of dietary energy, macronutrients and, DRRS components across different DRRS quartiles. Those with higher adherence to DRRS had a significantly higher intake of energy, and fiber compared with those at the lower quartiles. Moreover, lower intakes of trans fats, meat, SSB, and GI with higher intakes of fruits, cereal fiber, PUFA/ SFA ratio, coffee, and nuts were observed in the highest versus lowest DRRS categories (P < 0.001); however, after adjustment for the confounding effects of age, gender, BMI, physical activity and energy intake the significant difference of coffee, PUFA/ SFA ratio, trans fat and nuts across DRRS quartiles was lost. Higher adherence to DRRS was associated with lower systolic blood pressure (SBP) (P-adjusted = 0.01, with a remarkable reducing linear trend, 0.022), diastolic blood pressure (DBP) (P-crude = 0.012, P-trend = 0.126), TG (P-adjusted = 0.002, P-trend = 0.089) and higher HDL values (P-adjusted = 0.001, P-trend = 0.074). However, for DBP, this significant difference was disappeared after adjustment for potential confounders (P-adjusted = 0.253). No significant difference for other variables was observed. Table 5 presents odds ratios (ORs) and 95% confidence intervals (CIs) of the components of MetS risk across different quartiles of dietary DRRS after adjustment for BMI and energy intake. Subjects with higher adherence to DRRS had reduced risk of hypertension compared with those with the lower adherence (OR 0.688, 95% CI 0.26–0.84, p < 0.05). There was no significant association between other MetS components across DRRS quartiles. As illustrated in Fig. 1, lower prevalence of MetS was observed in the third and fourth quartiles of DRRS; although, this difference was not statistically significant (p = 0.245).

The prevalence of metabolic syndrome in different quartiles of DRRS. Mets, metabolic syndrome; DRRS, diabetes risk reduction score; Chi-square test used for test the prevalence of metabolic syndrome trend in quartiles of DRRS (P = 0.245). p-value adjusted for age, sex, BMI, physical activity, and total daily energy intake
Discussion
In the current study, we investigated the association between DRRS and metabolic risk factors among 342 obese individuals. According to our results, higher adherence to DRRS was associated with more favorable cardiovascular risk factors including lower blood pressure, lower TG, and higher HDL concentrations. Although, the highest DRRS quartile was associated with the lowest prevalence of Mets among obese individuals, this difference were not statistically significant after adjustment for confounders. To our knowledge, it is the first study that investigated the adherence to DRRS among obese individuals and revealed its beneficial effects toward cardio-metabolic risk factors. Although, for weight loss, different strategies have been developed and numerous interventions are available [52], but, most of obese individuals are unable to control their weight and therefore, their population is increasing worldwide [53,54,55]. As previously mentioned, there are a limited number of studies that evaluated adherence to DRRS and almost all of them confirmed its protective role against chronic diseases like diabetes [34], metabolic syndrome [35], and cancers [40, 41]. The ingredients of DRRS are comparable with other dietary indices; for example, higher adherence to a dietary approach to stop hypertension diet (DASH) that is full of whole grains, nuts, fruits and vegetables and, legumes was associated with lower serum lipids [56,57,58], lower odds of metabolic syndrome [59, 60], and more favorable cardiovascular health [61, 62] in numerous studies; a similar situation was observed for a Mediterranean dietary pattern that includes whole grains, monounsaturated fat, plant proteins, seafood, fruits, and vegetables and is associated with reduced cardiovascular risk factors [63, 64] and metabolic syndrome incidence in different populations [65, 66]. The beneficial effects of DRRS are attributed to its dietary ingredients; dietary fiber favors each MetS component separately by improving blood pressure, reducing cholesterol, improving glucose metabolism, and regulate body weight [67]. Additionally, dietary fiber reduces inflammation and oxidative stress, both of which have been associated with MetS development [68,69,70,71]. Similarly, the positive lipid-lowering effects of fruits are possibly because of their fiber, polyphenol, or phytosterol content, increased fecal bile acids and neutral steroids excretion, and increased fecal cholesterol and fatty acid excretion [72, 73]. Moreover, they exert antioxidant actions by protection against lipid peroxidation and reduced inflammatory response, and protection of vascular endothelial function [74,75,76]. In the study of Kempf K et al. [77], habitual coffee consumption for one month significantly reduced serum concentrations of interleukins, and increased adiponectin concentrations; also serum concentrations of total cholesterol, HDL cholesterol, and apolipoprotein A-I increased in response to regular coffee consumption among healthy subjects. Although the health effects of coffee on serum lipids and glucose tolerance depend on the type of coffee and the health status of participants; for example, in comparison to decaffeinated coffee, caffeine, ground caffeinated coffee, and instant caffeinated coffee increased lipolysis; furthermore, when compared to a placebo, acute caffeine ingestion increased glucose tolerance, whereas regular decaffeinated coffee decreased glucose tolerance [78, 79]. A meta-analysis of the intervention trials which were performed in Western countries revealed that those with hyperlipidemia were more sensitive to the cholesterol-raising effect of coffee [80]. Reduced consumption of red meat, trans fats and, SSBs are also helpful in healthy effects of DRRS. Numerous previous studies revealed the direct association between red meat consumption and blood pressure [81], twenty-year blood pressure change [82] and, incident hypertension [83]. High trans fatty acid consumption is associated with increased serum lipids and reduced consumption of trans fatty acid modifies serum lipids [84,85,86]. The arcuate nucleus (ARC) of the hypothalamus is one area of the brain that is a potential target for the effects of inflammatory cytokines. According to our results, the reduction in AgRP levels among DRRS quartiles was marginally significant after adjusting for confounders. Neurons in the ARC that express the neuropeptide AgRP are important areas contributing to orexigenic drive [37]. Leptin and insulin resistance develop in AgRP neurons as well as in peripheral tissues as a result of activation of the c-Jun N-terminal Kinase (JNK)-1 pathway, which also causes AgRP neurons to be activated more frequently. Therefore, JNK1 activation in AgRP neurons may cause leptin resistance, which could then lead to the development of systemic insulin resistance in obese individuals [87]. In addition, models of both acute and chronic inflammation show elevated expression of AgRP mRNA[88]. Therefore, it is expected that by increasing adherence to the DRRS and improving insulin resistance and reduced inflammation, a decrease in AgRP levels be observed; interestingly, after adjustment for the confounders, serum AgRP concentrations reduced in higher quartiles of DRRS in a marginally significant threshold (p = 0.065). After analysis, the most influential confounding factor in ANCOVA for the AgRP was sex, that could be explained by the regulation of AgRP expression by estrogen [89, 90]. DRRS, summarizes all of these food components altogether and identifies their synergistic or inhibitory effects same as what we encounter in our daily usual diet. So, it is a unique indicator of healthy dietary intake and the its effects are more realistic compared with other food scores with a very limited number of food ingredients. The current study has also some limitations; first of all, the cross-sectional design of the study limits the casual inference. Second, there was no long-term follow-up of study participants and due to dynamic change of both diet (e.g. DRRS) and cardio-metabolic risk factors over the years, longitudinal assessment of these factors will help to explain the causality. Third, the FFQ that was used in the current study was not originally developed for DRRS evaluation and the collected data may stem for recall bias, however, we used a valid and reliable FFQ that is adapted for the target population and we performed this study in a relatively large number of participants.
In conclusion, in the current cross-sectional study, DRRS was associated with favorable blood pressure and serum lipids in obese individuals. Moreover, the lowest prevalence of MetS was observed in the highest DRRS categories. Due to the limited number of studies investigating the health benefits of DRRS, further studies are warranted to identify its health effects in different populations and different disease statuses.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to some restrictions that applied by the ethical committee but are available from the corresponding author on reasonable request.
References
Minhas M, Murphy CM, Balodis IM, Samokhvalov AV, MacKillop J. Food addiction in a large community sample of Canadian adults: prevalence and relationship with obesity, body composition, quality of life and impulsivity. Addiction. 2021;116(10):2870-9.
De Zwaan M, Petersen I, Kaerber M, Burgmer R, Nolting B, Legenbauer T, et al. Obesity and quality of life: a controlled study of normal-weight and obese individuals. Psychosomatics. 2009;50(5):474–82.
Milan Z, Titta K, Razvan Constantin D, Nikola A, Bojan B, Dan Iulian A, et al. Leisure-Time Physical Activity and All-Cause Mortality: A Systematic Review. Revista de Psicología del Deporte (Journal of Sport Psychology). 2022;31(1):1–16.
Holt RI, Peveler RC. Obesity, serious mental illness and antipsychotic drugs. Diabetes Obes Metab. 2009;11(7):665–79.
Luppino FS, de Wit LM, Bouvy PF, Stijnen T, Cuijpers P, Penninx BW, et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry. 2010;67(3):220–9.
Schroeder K, Kubik MY, Sirard JR, Lee J, Fulkerson JA. Sleep is inversely associated with sedentary time among youth with obesity. Am J Health Behav. 2020;44(6):756–64.
Lutz M, Vargas C, Stojanova J, Arancibia M. Diet and depressive disorders. Archives of Clinical Psychiatry (São Paulo). 2021;48:117–22.
Latner JD, Wilson RE. Obesity and body image in adulthood. 2011.
Sarwer DB, Thompson JK. Obesity and body image disturbance. 2002.
Farhangi MA, Emam-Alizadeh M, Hamedi F, Jahangiry L. Weight self-stigma and its association with quality of life and psychological distress among overweight and obese women. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity. 2017;22(3):451–6.
Singh AK, Chaube B, Zhang X, Sun J, Citrin KM, Canfrán-Duque A, et al. Hepatocyte-specific suppression of ANGPTL4 improves obesity-associated diabetes and mitigates atherosclerosis in mice. J Clin Invest. 2021;131(17):e140989.
Dowaidar M. Discoveries in gene-environment interactions that influence CVD, lipid traits, obesity, diabetes, and hypertension appear to be able to influence gene therapy. 2021.
Wong JC, O’Neill S, Beck BR, Forwood MR, Khoo SK. Comparison of obesity and metabolic syndrome prevalence using fat mass index, body mass index and percentage body fat. PLoS One. 2021;16(1):e0245436.
Payab M, Tayanloo-Beik A, Falahzadeh K, Mousavi M, Salehi S, Djalalinia S, et al. Metabolomics prospect of obesity and metabolic syndrome; a systematic review. Journal of Diabetes & Metabolic Disorders. 2021:1–29.
Silveira EA, Kliemann N, Noll M, Sarrafzadegan N, de Oliveira C. Visceral obesity and incident cancer and cardiovascular disease: An integrative review of the epidemiological evidence. Obes Rev. 2021;22(1): e13088.
Norrman E, Petzold M, Gissler M, Spangmose AL, Opdahl S, Henningsen A-K, et al. Cardiovascular disease, obesity, and type 2 diabetes in children born after assisted reproductive technology: A population-based cohort study. PLoS Med. 2021;18(9): e1003723.
Rosengren A. Obesity and cardiovascular health: the size of the problem. Eur Heart J. 2021;42(34):3404.
Kjaergaard AD, Teumer A, Witte DR, Stanzick K-J, Winkler TW, Burgess S, et al. Obesity and Kidney Function: A Two-Sample Mendelian Randomization Study. Clin Chem. 2021;68:461.
Erstad BL, Nix DE. Assessment of kidney function in patients with extreme obesity: a narrative review. Ann Pharmacother. 2021;55(1):80–8.
Lega IC, Lipscombe LL. Diabetes, obesity, and cancer—pathophysiology and clinical implications. Endocr Rev. 2020;41(1):33–52.
Donohoe F, Wilkinson M, Baxter E, Brennan DJ. Mitogen-activated protein kinase (MAPK) and obesity-related cancer. Int J Mol Sci. 2020;21(4):1241.
Teper Y, Eibl G. Pancreatic Macrophages: Critical Players in Obesity-Promoted Pancreatic Cancer. Cancers. 2020;12(7):1946.
Hawkes C. Uneven dietary development: linking the policies and processes of globalization with the nutrition transition, obesity and diet-related chronic diseases. Glob Health. 2006;2(1):1–18.
Musaiger AO, Al-Khalifa F, Al-Mannai M. Obesity, unhealthy dietary habits and sedentary behaviors among university students in Sudan: growing risks for chronic diseases in a poor country. Environ Health Prev Med. 2016;21(4):224–30.
Aghajani R, Nemati N, Hojjati Zidashti Z, Bagherpour T. Effect of aerobic program in the morning and afternoon on obestatin and the body composition of overweight and obese women. Journal of Chemical Health Risks. 2020;10(2):117–25.
Kadam Ii, Neupane S, Wei J, Fullington LA, Li T, An R, et al. A Systematic Review of Diet Quality Index and Obesity among Chinese Adults. Nutrients. 2021;13(10):3555.
Kourlaba G, Panagiotakos DB. Dietary quality indices and human health: a review. Maturitas. 2009;62(1):1–8.
Varkaneh HK, Fatahi S, Tajik S, Rahmani J, Zarezadeh M, Shab-Bidar S. Dietary inflammatory index in relation to obesity and body mass index: A meta-analysis. Nutr Food Sci. 2018;48:702.
Salehi-Abargouei A, Akbari F, Bellissimo N, Azadbakht L. Dietary diversity score and obesity: a systematic review and meta-analysis of observational studies. Eur J Clin Nutr. 2016;70(1):1–9.
Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Yadav B, Hills AP. High dietary diversity is associated with obesity in Sri Lankan adults: an evaluation of three dietary scores. BMC Public Health. 2013;13(1):1–8.
Beşağıl P, Çalapkorur S, Şahin H. Determination of the relationship between total antioxidant capacity and dietary antioxidant intake in obese patients. Niger J Clin Pract. 2020;23(4):481.
Buckland G, Bach A, Serra-Majem L. Obesity and the Mediterranean diet: a systematic review of observational and intervention studies. Obes Rev. 2008;9(6):582–93.
Aminianfar A, Keshteli AH, Esmaillzadeh A, Adibi P. Association between adherence to MIND diet and general and abdominal obesity: a cross-sectional study. Nutr J. 2020;19(1):1–9.
Rhee JJ, Mattei J, Hughes MD, Hu FB, Willett WC. Dietary diabetes risk reduction score, race and ethnicity, and risk of type 2 diabetes in women. Diabetes Care. 2015;38(4):596–603.
Mirmiran P, Farhadnejad H, Teymoori F, Asghari G, Parastouei K, Azizi F. The association of dietary diabetes risk reduction score and its components with risk of metabolic syndrome incident in Tehranian adults. BMC Endocr Disord. 2021;21(1):1–9.
Farias G, Netto BDM, Boritza KC, Bettini SC, Dâmaso AR, de Freitas ACT. Mechanisms of sustained long-term weight loss after RYGB: α-MSH is a key factor. Neuropeptides. 2018;69:60–5.
Scarlett JM, Zhu X, Enriori PJ, Bowe DD, Batra AK, Levasseur PR, et al. Regulation of agouti-related protein messenger ribonucleic acid transcription and peptide secretion by acute and chronic inflammation. Endocrinology. 2008;149(10):4837–45.
Arliny Y, Yunus F, Burhan E, Andarini S, Jusman SWA, Yunir E, et al. Diagnostic Predictors of Active Tuberculosis Infection in Diabetic Patients with Latent Tuberculosis: A Review on Cathelicidin and 1, 25‑dihydroxyvitamin D. infection (LTBI). 2021;1:2.
Ghanbari E, Asgari P, Seraj-Khorrami N. Effectiveness of Transcranial Direct Current Stimulation on Cravings in Overweight Individuals. International Journal of Body, Mind and Culture. 2022;9(2):140-8.
Kang JH, Peng C, Rhee JJ, Farvid MS, Willett WC, Hu FB, et al. Prospective study of a diabetes risk reduction diet and the risk of breast cancer. Am J Clin Nutr. 2020;112(6):1492–503.
Turati F, Bravi F, Rossi M, Serraino D, Mattioli V, Augustin L, et al. Diabetes risk reduction diet and the risk of breast cancer. European journal of cancer prevention: the official journal of the European Cancer Prevention Organisation (ECP). 2021;1;31(4):339-45.
Luo X, Sui J, Yang W, Sun Q, Ma Y, Simon TG, et al. Type 2 diabetes prevention diet and hepatocellular carcinoma risk in US men and women. Am J Gastroenterol. 2019;114(12):1870.
Huang Y, Liu F, Chen A-M, Yang P-F, Peng Y, Gong J-P, et al. Type 2 diabetes prevention diet and the risk of pancreatic cancer: A large prospective multicenter study. Clin Nutr. 2021;40(11):5595–604.
Asghari G, Mirmiran P, Ramezan M, Farhadnejad H, Tahmasebinejad Z, Azizi F. Association Between Dietary Diabetes Risk Reduction Score and Chronic Kidney Disease in Adults: Tehran Lipid and Glucose Study. 2020.
Abbasalizad Farhangi M, Vajdi M, Nikniaz L, Nikniaz Z. The interaction between dietary inflammatory index and 6 P21 rs2010963 gene variants in metabolic syndrome. Eating and weight disorders : EWD. 2020;25(4):1049–60.
Abbasalizad Farhangi M, Vajdi M, Nikniaz L, Nikniaz Z. Interaction between Vascular Endothelial Growth Factor-A (rs2010963) Gene Polymorphisms and Dietary Diversity Score on Cardiovascular Risk Factors in Patients with Metabolic Syndrome. Lifestyle genomics. 2020;13(1):1–10.
Khodarahmi M, Asghari-Jafarabadi M, Abbasalizad FM. A structural equation modeling approach for the association of a healthy eating index with metabolic syndrome and cardio-metabolic risk factors among obese individuals. PLoS ONE. 2019;14(7): e0219193.
Washburn RA. Assessment of physical activity in older adults. Res Q Exerc Sport. 2000;71(sup2):79–87.
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation. 2005;112:2735–52.
Mirmiran P, Esfahani FH, Mehrabi Y, Hedayati M, Azizi F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 2010;13(5):654–62.
Ghaffarpour M, Houshiar-Rad A, Kianfar H. The manual for household measures, cooking yields factors and edible portion of foods. Tehran: Nashre Olume Keshavarzy. 1999;7(213):42–58.
Jakicic JM, Clark K, Coleman E, Donnelly JE, Foreyt J, Melanson E, et al. Appropriate intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc. 2001;33:2145.
Ruhm CJ, editor Current and future prevalence of obesity and severe obesity in the United States. Forum for Health Economics & Policy; 2007: De Gruyter.
Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15(5):288–98.
Tang D, Bu T, Feng Q, Liu Y, Dong X. Differences in overweight and obesity between the North and South of China. Am J Health Behav. 2020;44(6):780–93.
Chiu S, Bergeron N, Williams PT, Bray GA, Sutherland B, Krauss RM. Comparison of the DASH (Dietary Approaches to Stop Hypertension) diet and a higher-fat DASH diet on blood pressure and lipids and lipoproteins: a randomized controlled trial–3. Am J Clin Nutr. 2016;103(2):341–7.
Zhang N, Xiao X, Xu J, Zeng Q, Li J, Xie Y, et al. Dietary Approaches to Stop Hypertension (DASH) diet, Mediterranean diet and blood lipid profiles in less-developed ethnic minority regions. Bri J Nutr. 2022;128(6):1137-46.
Jasim O, Mahmood M, Ad’hiah A. Significance of Lipid Profile Parameters in Predicting Pre-Diabetes. Archives of Razi Institute. 2022;77(1):267–74.
Saneei P, Fallahi E, Barak F, Ghasemifard N, Keshteli AH, Yazdannik AR, et al. Adherence to the DASH diet and prevalence of the metabolic syndrome among Iranian women. Eur J Nutr. 2015;54(3):421–8.
Ghorabi S, Salari-Moghaddam A, Daneshzad E, Sadeghi O, Azadbakht L, Djafarian K. Association between the DASH diet and metabolic syndrome components in Iranian adults. Diabetes Metab Syndr. 2019;13(3):1699–704.
Liese AD, Bortsov A, Günther AL, Dabelea D, Reynolds K, Standiford DA, et al. Association of DASH diet with cardiovascular risk factors in youth with diabetes mellitus: the SEARCH for Diabetes in Youth study. Circulation. 2011;123(13):1410–7.
Siervo M, Lara J, Chowdhury S, Ashor A, Oggioni C, Mathers JC. Effects of the Dietary Approach to Stop Hypertension (DASH) diet on cardiovascular risk factors: a systematic review and meta-analysis. Br J Nutr. 2015;113(1):1–15.
Giugliano D, Esposito K. Mediterranean diet and cardiovascular health. Ann N Y Acad Sci. 2005;1056(1):253–60.
Ros E, Martínez-González MA, Estruch R, Salas-Salvadó J, Fitó M, Martínez JA, et al. Mediterranean diet and cardiovascular health: Teachings of the PREDIMED study. Adv Nutr. 2014;5(3):330S-S336.
Babio N, Bulló M, Salas-Salvadó J. Mediterranean diet and metabolic syndrome: the evidence. Public Health Nutr. 2009;12(9A):1607–17.
Kastorini C-M, Milionis HJ, Esposito K, Giugliano D, Goudevenos JA, Panagiotakos DB. The effect of Mediterranean diet on metabolic syndrome and its components: a meta-analysis of 50 studies and 534,906 individuals. J Am Coll Cardiol. 2011;57(11):1299–313.
Satija A, Hu FB. Cardiovascular benefits of dietary fiber. Curr Atheroscler Rep. 2012;14(6):505–14.
C Fernandez-Garcia J, Cardona F, J Tinahones F. Inflammation, oxidative stress and metabolic syndrome: dietary modulation. Current Vascular Pharmacology. 2013;11(6):906–19.
Ghanim H, Batra M, Abuaysheh S, Green K, Makdissi A, Kuhadiya ND, et al. Antiinflammatory and ROS suppressive effects of the addition of fiber to a high-fat high-calorie meal. J Clin Endocrinol Metab. 2017;102(3):858–69.
Wei B, Liu Y, Lin X, Fang Y, Cui J, Wan J. Dietary fiber intake and risk of metabolic syndrome: A meta-analysis of observational studies. Clin Nutr. 2018;37(6):1935–42.
Paul R, Mukkadan J. Modulation of blood glucose, oxidative stress, and anxiety level by controlled vestibular stimulation in prediabetes. Journal of Natural Science, Biology and Medicine. 2020;11(2):111-.
Jenkins DJ, Popovich DG, Kendall CW, Vidgen E, Tariq N, Ransom TP, et al. Effect of a diet high in vegetables, fruit, and nuts on serum lipids. Metabolism. 1997;46(5):530–7.
Lampe JW. Health effects of vegetables and fruit: assessing mechanisms of action in human experimental studies. Am J Clin Nutr. 1999;70(3):475s-s490.
Zhao C-N, Meng X, Li Y, Li S, Liu Q, Tang G-Y, et al. Fruits for prevention and treatment of cardiovascular diseases. Nutrients. 2017;9(6):598.
Goswami B, Sarkar S, Bhattacharjee B, Sengupta S. Serum levels of nitric oxide and its correlation with endothelial nitric oxide synthase gene expression among type 2 diabetic patients with or without hypertension: a comparative study in a tertiary care hospital of North East India. J Nat Sci Biol Med. 2021;12(2):207.
Storz MA. The role of vegan diets in lipotoxicity-induced beta-cell dysfunction in type-2-diabetes. J Popul Ther Clin Pharmacol. 2020;27(SP2):e22–38.
Corrêa TA, Rogero MM, Mioto BM, Tarasoutchi D, Tuda VL, César LA, et al. filtered coffee increases cholesterol and inflammation biomarkers independent of roasting degree: A clinical trial. Nutrition. 2013;29(7–8):977–81.
Ramli NNS, Alkhaldy AA, Mhd Jalil AM. Effects of caffeinated and decaffeinated coffee consumption on metabolic syndrome parameters: a systematic review and meta-analysis of data from randomised controlled trials. Medicina. 2021;57(9):957.
PAVLOS S, NIKIFOROU C. Medicinal Plants Against Obesity: A Met-Analysis of Literature. Journal of Complementary Medicine Research. 2022;12(4):244-.
Cai L, Ma D, Zhang Y, Liu Z, Wang P. The effect of coffee consumption on serum lipids: a meta-analysis of randomized controlled trials. Eur J Clin Nutr. 2012;66(8):872–7.
Masala G, Bendinelli B, Versari D, Saieva C, Ceroti M, Santagiuliana F. Anthropometric and dietary determinants of blood pressure in over 7000 Mediterranean women: the European Prospective Investigation into Cancer and Nutrition-Florence cohort. J Hypertens. 2008;26:2112–20.
Wang Z, Huang Q, Wang L, Jiang H, Wang Y, Wang H, et al. Moderate intake of lean red meat was associated with lower risk of elevated blood pressure in Chinese Women: Results from the China Health and Nutrition Survey, 1991–2015. Nutrients. 2020;12(5):1369.
Lajous M, Bijon A, Fagherazzi G, Rossignol E, Boutron-Ruault MC, Clavel-Chapelon F. Processed and unprocessed red meat consumption and hypertension in women. Am J Clin Nutr. 2014;100:948–52.
Aro A, Jauhiainen M, Partanen R, Salminen I, Mutanen M. Stearic acid, trans fatty acids, and dairy fat: effects on serum and lipoprotein lipids, apolipoproteins, lipoprotein(a), and lipid transfer proteins in healthy subjects. Am J Clin Nutr. 1997;65(5):1419–26.
Ascherio A. Trans fatty acids and blood lipids. Atheroscler Suppl. 2006;7(2):25–7.
Bendsen NT, Chabanova E, Thomsen HS, Larsen TM, Newman JW, Stender S, et al. Effect of trans fatty acid intake on abdominal and liver fat deposition and blood lipids: a randomized trial in overweight postmenopausal women. Nutrition & Diabetes. 2011;1(1):e4-e.
Baldini G, Phelan KD. The melanocortin pathway and control of appetite-progress and therapeutic implications. J Endocrinol. 2019;241(1):R1–33.
Gasmi A, Noor S, Piscopo S, Menzel A. Lifestyle Genetics-Based Reports in the Treatment of Obesity. Arch Razi Inst. 2021;76(4):707.
Titolo D, Cai F, Belsham DD. Coordinate regulation of neuropeptide Y and agouti-related peptide gene expression by estrogen depends on the ratio of estrogen receptor (ER) α to ERβ in clonal hypothalamic neurons. Mol Endocrinol. 2006;20(9):2080–92.
Guerra ZC, Moore JR, Londoño T, Castro Y. Associations of acculturation and gender with obesity and physical activity among Latinos. Am J Health Behav. 2022;46(3):324–36.
Acknowledgements
We thank all of the study participants. We also are thankful from Research Undersecretary of Tabriz University of Medical Sciences for their financial support (Grant number: 71049).
Funding
Present study has been financially supported by a grant from Tabriz University of Medical Sciences. (registration code: IR.TBZMED.REC.1398.460 and IR. TBZMED.REC.1396.768). The funders had no role in hypothesis generation, recruiting and designing the study. Their role was only financial supporting.
Author information
Authors and Affiliations
Contributions
All authors approved the final version of the article. MAF and GS designed the project and supervised it. MAF also contributed in statistical analysis, NN and SK were involved in manuscript writing and NN revised it. SJ and FJ were involved in hypothesis generation and data collection. GS, SJ and SK were also involved in data collection. EF was involved in English edition and AMA was involved in data analysis and also revision of the paper.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study protocol has been approved by the ethics committee of the Tabriz University of Medical Sciences (registration code: IR.TBZMED.REC.1398.460 and IR. TBZMED.REC.1396.768). Written informed consent was obtained from all of the participants before participation in the study. All methods in the current research were performed in accordance with the declaration of Helsinki’s guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Siri, G., Nikrad, N., Keshavari, S. et al. A high Diabetes Risk Reduction Score (DRRS) is associated with a better cardio-metabolic profile among obese individuals. BMC Endocr Disord 23, 31 (2023). https://doi.org/10.1186/s12902-023-01279-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-023-01279-5