
Abstract
Background
South-Asian immigrants to Western countries have a high prevalence of type 2 diabetes mellitus (T2DM) and increased adipose tissue insulin resistance (AT-IR), as compared to their Western counterparts. Fetuin-A is a hepatokine known to influence AT-IR.
Aim
Can plasma fetuin-A concentrations explain an ethnic difference in adipose tissue insulin resistance?
Methods
We performed a two-step euglycemic-hyperinsulinaemic clamp and measured plasma concentrations of fetuin-A and non-esterified fatty acids (NEFA), in 18 Pakistani and 21 Norwegians with T2DM (age 29–45y) in Norway. AT-IR was calculated as NEFA-suppression during the clamp. The adipokines/cytokines leptin, adiponectin, visfatin, PTX3, IL-1β, INF-γ, and IL-4 were measured in fasting plasma. Liver fat was estimated by CT-scans.
Results
Despite a lower BMI, Pakistani patients displayed higher AT-IR than Norwegians. NEFA-suppression during clamp was lower in Pakistani than Norwegians (mean=-20.6%, 95%CI=[-40.8, -0.01] and p = 0.046). Plasma fetuin-A concentration was higher in Pakistani than Norwegians (43.4 ng/mL[12.7,74.0], p = 0.007) and correlated negatively to %NEFA-suppression during clamp (rho=-0.39, p = 0.039). Plasma fetuin-A concentration explained 22% of the ethnic difference in NEFA-suppression during the clamp. Pakistani patients exhibited higher plasma leptin and lower PTX3 levels than Norwegian, and plasma visfatin correlated positively to plasma fetuin-A levels in the Pakistani patients. We observed no correlation between plasma fetuin-A and liver fat, but fetuin-A correlated negatively with plasma IL-1β, INF-γ, and IL-4 concentrations. Plasma IL-4 concentration was lower in Pakistani than in Norwegian patients.
Conclusion
Fetuin-A may contribute to explain the discrepancy in T2DM prevalence between Pakistani and Norwegians patients by influencing AT-IR.
Similar content being viewed by others
Introduction
South Asian immigrants living in Western countries have a high prevalence of type 2 diabetes mellitus (T2DM) [1,2,3,4,5,6]. Norway has a growing population of Pakistani immigrants, especially in the capital Oslo, with a high prevalence of T2DM manifesting at a younger age than in ethnic Norwegians [7]. The pathophysiology of T2DM in this population may differ from the common form of T2DM in the Western population, and a deeper understanding may help to develop more efficient prevention and treatment strategies, and also give new insight into the general pathogenesis of T2DM [8]. For example, our previous findings indicated a more pronounced influence of insulin resistance on lipid metabolism in Pakistani compared to Norwegian patients with T2DM [9].
Expanded and inflamed adipose tissue is a major contributor to insulin resistance in other tissues, such as the liver [10, 11], by increased lipolysis and altered adipokine secretion [12]. However, a reverse relationship may also exist, where the liver induces adipose tissue resistance through altered secretion of hepatokines [13, 14]. This cross-relationship is known as the “adipose tissue-liver axis” of insulin resistance [13].
Recently, several studies have focused on the hepatokine fetuin-A and its potential role in regulating adipose tissue insulin resistance [15,16,17,18,19,20]. In vitro studies have shown that fetuin-A may serve as an adaptor protein for saturated fatty acid (SFA) and explain SFA-induced activation of Toll-like receptor 4 (TLR4) signaling and inhibition of the insulin receptor tyrosine kinase in adipocytes [19,20,21]. Furthermore, rodents lacking fetuin-A may be protected from diet-induced insulin resistance [22]. In humans, high levels fetuin-A and nonesterified fatty acids (NEFA) may together predict insulin resistance in adipose tissue [15, 20]. Moreover, fetuin-A has been shown to impair insulin receptor tyrosine kinase activity [21]. Notably, fetuin-A mediated adipose tissue insulin resistance may promote inflammatory cytokine production [19]. Obese human participants with T2DM have increased levels of fetuin-A [19] that correlate with increased levels of several pro-inflammatory cytokines [23]. Furthermore, fetuin-A may inhibit adiponectin production in adipocytes, contributing to insulin resistance [24]. However, it remains unknown if ethnic differences in adipose tissue insulin resistance [9] can be explained by altered secretion of fetuin-A.
We hypothesized that (i) fetuin-A would be associated with adipose tissue insulin resistance in T2DM, and (ii) could mediate ethnic differences in T2DM prevalence between young Pakistani and Norwegians. We have measured plasma concentration of fetuin-A and adipose tissue insulin resistance, calculated as NEFA-suppression during a two-step euglycemic hyperinsulinemic clamp, in young Pakistani and Norwegian men and women with T2DM from the DIPI study [25].
Materials and methods
DIPI is a cross-sectional study comparing young first generation Pakistani immigrants with T2DM living in Oslo, Norway to ethnic Norwegian patients aged ≤ 45 years [9, 26]. Exclusion criteria were: ethnicities other than Norwegian or Pakistani, positive antibodies to glutamic acid decarboxylase (GAD) or islet antigen 2 (IA2) auto-antibodies, age > 45 years, persons unwilling or unable to give informed consent.
Participants
Details regarding the study participants had been described previously [9, 26]. Briefly, T2DM patients of either Pakistani (n = 18) or Norwegian (n = 21) origin (51% women) between age 29 to 45 years were recruited from the diabetes outpatient clinics at Lovisenberg Deaconess Hospital and Aker University Hospital in Oslo. We searched patient registries and identified 195 patients that were randomly invited to participate in the study. All participants were treated according to current national and international guidelines for T2DM with education about healthy lifestyle and pharmacological antidiabetic treatment as appropriate. None were treated with GLP-1 receptor agonists or SGLT2-inhibitors. Participant characteristics were similar to a subgroup of 80 with available data out of the 155 non-included patients in terms of HbA1cand anthropometrics.
Anthropometrical measurements
Height and weight were measured with light clothing without shoes. Waist and hip circumferences were assessed with a tape at the midpoint between the lowest rib margin and the iliac crest, and at the level of the major trochanter, respectively. A Tanita Body Composition Analyzer BC-418 (Tokyo, Japan) was used to estimate percentage total body fat, body fat mass in kilograms and fat free mass in kilograms from a subset of Norwegians (n = 17) and Pakistani (n = 14) patients. A CT Somatom (Erlangen, Germany) scan was performed on patients in a supine position with their arms above the head. Liver fat content was estimated from attenuation in Hounsfield Units (HU). All subjects were fasting and voided urine before measurement.
Insulin resistance
All patients stopped taking oral antidiabetic drugs for two days, and insulin for at least 12 h before the examination [9, 26]. They also refrained from strenuous physical exercise and alcohol intake during these two days, and they fasted from midnight before the examination. We performed a euglycemic hyperinsulinemic clamp [27] with two steps; first administering a primed, continuous insulin dose of 40 mU/m2/min for a minimum of 100 min, until at least 30 min of stable euglycemia was obtained, and then immediately a 400 mU/m2/min insulin infusion, also for a minimum of 100 min, with at least 30 min of stable euglycemia at the end. Body surface area was calculated using the Mosteller equation [28]. Insulin sensitivity was measured as the glucose infusion rate during low and high insulin infusion rates in µmol/m2/min and denoted GIR40 and GIR400, respectively.
EDTA plasma was collected for non-esterified fatty acid (NEFA) measurements before and 30 min into the two steps euglycemic clamp. EDTA plasma was immediately frozen at -70° C after collection. Adipose tissue insulin resistance was defined as percent NEFA-suppression from before to 30 min into the clamp [9].
Biomarker analysis
Fasting plasma glucose was measured by the glucose oxidase method on a Glucose Analyzer II (Beckman Instruments, CA 92,821, USA). Serum insulin was analyzed using the radioimmunoassay (RIA) kit, formerly from Linco Research Inc. (St. Charles, MO, USA), presently available from Millipore Corp. (Billerica, MA, USA). HbA1c was measured by high-performance liquid chromatography on a Variant analyzer (Bio-Rad, Richmond, CA, USA). Fasting serum total cholesterol, HDL cholesterol, and triglycerides were measured using a routine enzymatic method (Roche Diagnostics, Mannheim, Germany). Serum LDL cholesterol was calculated using the Friedewald equation [29]. NEFA were analyzed using a NEFA C enzymatic color test kit, (Wako Chemicals GmbH, Neuss, Germany), modified to run on a Technicon RA1000 (Technicon Instruments Corp., Tarrytown, NY). Plasma levels of adiponectin and leptin were analyzed using RIA kits from Millipore Corp. (Billerica, MA, USA). Measurements of plasma levels of fetuin-A were performed using Human fetuin-A ELISA (BioVendor Laboratory Medicine, Inc. (Modrice, Czech Republic). Pentraxin 3 (PTX3) was measured using ELISA from R&D systems (Minneapolis, MN, USA). IL-1β, INF-γ and IL-4 were assessed using BioPlex Human Cytokine panel, Bio-Rad Laboratories Inc (Hercules, CA, USA). The intra-assay variability for fetuin-A was on average 3.75% between duplicates. Only one assay was used so there is no inter-assay variability issue.
Power calculations
Post-hoc power analyses indicated that we achieved 91.5% power to detect ethnical difference in plasma fetuin-A levels, and 71.1% power to detect ethnical difference in NEFA suppression during the clamp.
Statistical analyses
Group comparisons are presented as box-and-whisker plots and statistical significance was calculated using Wilcoxon signed-rank tests. Bivariate and partial (correction for BMI) correlations were tested using Spearman’s ranked tests and presented as scatter plots. Mediation analyses were performed using Baron and Kenny’s mediation steps [30]. Briefly, the null model was a linear model for adipose insulin resistance (the outcome) as a function of ethnicity. Next, a model was constructed substituting the outcome with the mediator of interest (plasma fetuin-A concentration). Finally, a full model was constructed similar to the null model, but also included the mediator of interest as a covariate. The potential interpretations of the full model are as follows [30]: (1) if the effect of ethnicity on adipose tissue insulin resistance is reduced and becomes insignificant, the mediator (fetuin-A) may fully explain ethnic differences in adipose tissue insulin resistance; (2) if the effect of ethnicity on adipose tissue insulin resistance is reduced, but remains significant, the mediator (fetuin-A) may only partially explain ethnic differences in adipose tissue insulin resistance, and; (3) if the effect of ethnicity on adipose tissue insulin resistance remains similar despite the presence of the potential mediator, then fetuin-A does not explain ethnic differences in adipose tissue insulin resistance. We considered a P ≤ 0.05 as statistically significant. R 3.1.1 was used for all calculations.
Results
Group differences at baseline
The groups were similar in terms of age, sex, and fasting plasma glucose, as described previously [9]. Norwegian patients exhibited higher BMI, body weight, total body fat mass, and lean body mass, and had a shorter duration of diabetes as compared to Pakistani (Table 1).
Ethnic differences in adipose tissue insulin resistance and plasma fetuin-A concentrations
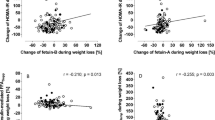
NEFA-suppression during the clamp was lower in Pakistani than Norwegians (-41.2%, p = 0.045) (Fig. 1A). Plasma fetuin-A concentration was higher in Pakistani then Norwegians (9.2%, p = 0.008) (Fig. 1B). These differences were present both with and without adjustment for BMI. Plasma fetuin-A concentrations correlated negatively to %NEFA-suppression (Fig. 1C) during clamp (rho=-0.39, p = 0.039) across all participants. Within-group correlations were in the same directions but did not reach statistical significance for plasma fetuin-A concentrations vs. %NEFA-suppression (Norwegians: rho=-0.27, p = 0.371 and Pakistani: rho=-0.19 p = 0.491). Plasma fetuin-A concentration mediated 22% of the ethnic difference in NEFA-suppression during the clamp (Fig. 1D). Similar results were obtained with or without BMI correction (data not shown). In comparison, we observed no correlations between plasma fetuin-A concentrations and markers of skeletal muscle insulin resistance during clamping (GIR40 and GIR400, data not shown).

Ethnic differences in plasma fetuin-A levels and adipose tissue insulin resistance. A Insulin-induced suppression of lipolysis during the 2-step euglycemic hyperinsulinemic clamp, and B plasma fetuin-A concentrations in Norwegian (NOR) and South-Asian (SA) persons. C Correlations between plasma fetuin-A concentration and insulin-induced suppression of lipolysis during the 2-step euglycemic hyperinsulinemic clamp. The thick lines represents the correlation across all persons, and the stapled lines represent within-group correlations. D Mediation analyses on effects of plasma fetuin-A concentration on adipose tissue insulin resistance. *p < 0.05, **p < 0.01. AT-IR; Adipose tissue insulin resistance. NEFA; non-esterified fatty
Sensitivity analyses
Because the ethnic groups differed in terms of T2DM-duration, HbA1c levels and T2DM treatments (Table 1), we constructed multiple regression models adjusting for these factors (Table 2). T2DM duration tended to correlate with NEFA-suppression (p = 0.091) whereas HbA1c levels or treatment regime showed no associations with NEFA-suppression (Table 2). The relationship between ethnicity and NEFA-suppression was not moderated by any of these factors (Table 2). T2DM duration, HbA1c levels or treatment regime were not associated with plasma fetuin-A levels and did not moderate the relationship between ethnicity and plasma fetuin-A levels (Table 2).
Differences due to sex
We observed no sex differences in NEFA-suppression or plasma fetuin-A concentrations (data not shown).
Ethnic differences in markers of adiposity and adipose tissue inflammation
After adjustment for BMI, Pakistani patients displayed 21.0% higher plasma leptin (p = 0.029) (Fig. 2A) and 46.8% lower PTX3 (p = 0.0006) (Fig. 2D) levels compared to Norwegian. We observed no group difference in plasma visfatin levels (Fig. 2C), and a non-significant tendency to lower adiponectin levels (23.4%, p = 0.088) in Pakistani than Norwegian patients (Fig. 2B).

Ethnic differences in markers of adipose tissue inflammation. A-D Group comparisons. E-F Correlation scatter plots. *p < 0.05 and **p < 0.01. NOR; Norwegian. SA; South-Asian (Pakistani)
We observed no ethnic differences in the Spearman correlation between plasma fetuin-A and markers of adipose tissue inflammation (Fig. 2E-H), except for plasma visfatin levels, which correlated to plasma fetuin-A in Pakistani (rho = 0.58, p = 0.028), but not in Norwegian patients (Fig. 2G).
Ethnic differences in markers of liver fat
After adjusting for BMI, Pakistani exhibited higher waist-hip-ratio (5.4%, p = 0.025), similar liver fat content, and higher plasma aspartate aminotransferase (ASAT) (37.8%, p = 0.025) and alanine transaminase (ALAT) (18.0%, p = 0.090) levels than Norwegians (Fig. 3A-D). Plasma fetuin-A levels correlated positively to the waist-hip-ratio (rho = 0.56, p = 0.031), and the plasma ASAT (rho = 0.67, p < 0.001) and ALAT (rho = 0.74, p < 0.001) levels, in Pakistani patients only (Fig. 3E-H). We observed no significant correlations between plasma fetuin-A levels and liver fat content assessed by CT in any of the ethnic groups.

Ethnic differences in markers of liver fat content. A Group comparison of the waist-hip-ratio (WHR), B estimated liver fat content, and plasma levels of C ASAT and D ALAT. E Correlation between plasma fetuin-A levels and the waist-hip-ratio (WHR), F liver fat, G plasma ASAT and H ALAT levels. The grey stapled lines and the rho-values represent correlations in Pakistani patients. *p < 0.05, and ***p < 0.001. HUE = Hounsfield units. NOR; Norwegian. SA; South-Asian (Pakistani)
Associations between plasma fetuin-A, and IL-1β, INF-γ, and IL-4 levels
We observed negative correlations between the plasma concentrations of fetuin-A and IL-1β (Fig. 4A), INF-γ (Fig. 4B), and IL-4 (Fig. 4C), across the ethnic groups. Within-group correlations were in the same directions, but did not reach statistical significance for plasma fetuin-A concentrations vs. IL-1β (Norwegians: rho=-0.36, p = 0.231 and Pakistani: rho=-0.42 p = 0.114), plasma fetuin-A concentrations vs. INF-γ (Norwegian: rho=-0.27, p = 0.215 and Pakistani: rho=-0.02, p = 0.943), nor for plasma fetuin-A concentrations vs. IL-4 (Norwegian: rho = 0.20, p = 0.505 and Pakistani: rho = 0.31, p = 0.263).

Plasma fetuin-A and IL-1β, INF-γ, and IL-4 levels. A Correlation scatter plots between plasma levels of fetuin-A and IL-1β, B INF-γ and C IL-4. D Group comparisons of plasma levels of IL-1β, E INF-γ and F IL-4. *p < 0.05. NOR; Norwegian. SA; South-Asian (Pakistani)
After adjusting for BMI, Pakistani patients exhibited a non-significant tendency to lower plasma concentrations of IL-1β (-40.2%, p = 0.078) and INF-γ (-87.4%, p = 0.067), and lower IL-4 (-53.1%, p = 0.014) than Norwegian (Fig. 4D-F).
Discussion
We observed that differences in adipose tissue insulin resistance between Pakistani and Norwegian patients with T2DM could be explained partly by differences in plasma fetuin-A concentrations. We also observed signs of more adipose tissue inflammation in Pakistani vs. Norwegian patients, and the inflammatory markers were associated with higher plasma levels of fetuin-A. The elevated plasma concentration of fetuin-A in Pakistani vs. Norwegian patients might relate to lower plasma levels of IL-1β, INF-γ, and IL-4 seen in the Pakistani patients.
Adipose tissue lipolysis is normally suppressed by insulin. Reduced suppression of lipolysis in response to insulin is thus an indicator of adipose tissue insulin resistance. Adipose tissue insulin resistance may contribute to lipid-induced insulin resistance in other tissues due to higher NEFA availability for the liver and can be a major pathogenic factor in T2DM [13, 16, 17]. However, an opposite relationship has been proposed where the liver may induce or worsen lipid-induced adipose tissue insulin resistance through increased secretion of fetuin-A that may bind saturated fatty acids and activate TLR4-signaling in adipose tissue, forming a vicious cycle to increase insulin resistance [13, 31].
We observed that young Pakistani patients with T2DM displayed reduced suppression of lipolysis in response to hyperinsulinemia during the clamp, suggesting that they have increased adipose tissue insulin resistance as compared to their Norwegian counterparts, in accordance with previous observations [9]. Furthermore, we show that these Pakistani patients with T2DM also display elevated plasma fetuin-A levels and that this difference in plasma fetuin-A levels might explain some of the observed difference in adipose tissue insulin resistance. In contrast, we observed no correlation between fetuin-A and measures of skeletal muscle insulin resistance. Thus, the effect of fetuin-A seems specific for insulin resistance in adipose tissue, as we have also indicated in a previous study [20].
Furthermore, despite differences in T2DM duration, HbA1c levels and T2DM treatment regimens between the two groups, adjusting for these factors in multiple regression analyses did not alter the associations between ethnicity, NEFA-suppression and plasma fetuin-A levels. We also note that body fat distribution is among the most important determinants of cardiometabolic risk and strongly impacts on insulin resistance of different organs [32]. However, we did not detect any difference in body fat percent of waist-hip ratio between the groups. Furthermore, low gluteofemoral fat mass strongly affect insulin resistance, independently of total fat mass [32], but we did not detect any group differences in thigh fat mass. We note that data obtained by body impedance analyses and CT-scans are not optimal to estimate body composition, and are greatly outperformed by magnetic resonance imaging (MRI) [33]. Thus, our data may give false negative results. We also note that differences in socioeconomic status may influence our results [34]. Unfortunately, we do not have data on the patients socioeconomic background.
We observed signs of more adipose tissue inflammation in Pakistani than Norwegian patients, as reflected in higher plasma concentrations of leptin [35], and lower plasma adiponectin and the anti-inflammatory PTX3 cytokine [36]. Moreover, increased plasma levels of the proinflammatory cytokine visfatin [37] were associated with higher plasma levels of fetuin-A in Pakistani patients, as also reported by others [38]. These observations are in line with in vitro studies showing that fetuin-A may increase proinflammatory cytokine production by activation of the TLR4 pathway in adipocytes [19]. Moreover, incubation with fetuin-A may inhibit the production of anti-inflammatory cytokines, such as adiponectin, and promote proinflammatory cytokines, such as IL-1β, TNF-α and IL-6 in human adipocytes and mice [24]. In vivo human studies have reported that enhanced levels of fetuin-A correlate with increased levels of several pro-inflammatory cytokines [19, 23]. Hence, we speculate that the increased adipose tissue insulin resistance in Pakistani than Norwegians might be explained by fetuin-A-induced inhibition of adipocyte insulin signaling by activation of inflammatory pathways [20, 21].
We also explored potential links to why plasma fetuin-A levels may be higher in Pakistani than Norwegian patients with T2DM. Pakistani patients had a higher waist-to-hip ratio than Norwegians, which correlated to increased plasma fetuin-A levels. However, we did not detect any ethnic differences in estimated liver fat content using CT-scans, nor any correlations between plasma fetuin-A levels and estimated liver fat content. These results are somewhat surprising because we expected a difference in liver fat content between the groups studied [39]. However, while CT-based diagnosis of hepatic steatosis is considered quite accurate, it is outperformed by dual gradient echo MRI (DGE-MRI) and 1 H-MRS in the diagnosis of non-alcoholic fatty liver disease (NAFLD) [33]. Our CT-derived estimation of liver fat content may explain why we did not observe a group difference, nor an association between liver fat content and fetuin-A levels in the present study. We observed higher plasma ASAT and ALAT concentrations in Pakistani patients, which correlated to increased plasma levels of fetuin-A.
Some researchers have suggested a cytokine-dependent down-regulation of fetuin-A expression in response to high plasma levels of IL-1β, INF-γ, and IL-4 [40]. Thus, we measured IL-1β, INF-γ, and IL-4 levels in plasma in our participants. We observed that plasma fetuin-A concentration was negatively correlated to plasma IL-1β, INF-γ, and IL-4 levels, consistent with previous reports [23, 40, 41]. We also observed lower plasma IL-4 levels, and tendencies to lower plasma IL-1β and INF-γ levels in Pakistani than Norwegian T2DM patients. Hence, we speculate that lower plasma levels of especially IL-4 may partly explain the difference in plasma fetuin-A levels between Pakistani and Norwegian T2DM patients. However, the exact mechanisms behind the links between fetuin-A and the pro/anti-inflammatory cytokines remain unknown.
The main weakness of this study is our limited sample size. Our results should be regarded as suggestive. Another weakness of this study is that we have no data on NEFA composition and dietary fat intake. Fetuin-A binds several types of NEFAs with different affinities, the strongest affinity is for saturated fatty acids like palmitic acid [15, 19]. Thus, differences in plasma NEFAs composition might influence the ability of fetuin-A to induce adipose tissue TLR4-signaling. Another weakness is that we do not have liver biopsies and we are unable to assess mRNA expression of fetuin-A directly. Furthermore, our study has a cross-sectional design and cannot imply causality. Future studies should be performed on a higher number of participants, monitor dietary intake, and perform more comprehensive lipidomics and cytokine profiling in blood and adipose tissue.
Taken together, we suggest a role for fetuin-A in the pathogenesis of T2DM by influencing adipose tissue inflammation and insulin resistance. Future studies should asses if elevated plasma fetuin-A levels may explain the high prevalence and early manifestation of T2DM in subjects with South Asian ethnicity living in Western countries.
Availability of data and materials
Data are available from the corresponding author on reasonable request.
Abbreviations
- ASAT:
-
Aspartate aminotransferase
- ALAT:
-
alanine transaminase
- anti-GAD:
-
anti-glutamic acid decarboxylate
- anti-IA2:
-
anti-protein tyrosine phosphatase
- BMI:
-
body-mass index
- ELISA:
-
enzyme-linked immunosorbent assay
- GIR40:
-
glucose infusion rate at the low insulin infusion clamp step
- GIR400:
-
glucose infusion rate at the high insulin infusion clamp step
- IL-1β:
-
interleukin-1 beta
- INF-γ:
-
interferon-gamma
- IL-4:
-
interleukin-4
- NEFA:
-
non-esterified fatty acids
- T2DM:
-
type 2 diabetes mellitus
References
Mather HM, Keen H. The Southall Diabetes Survey: prevalence of known diabetes in Asians and Europeans. Br Med J (Clin Res Ed). 1985;291(6502):1081–4.
McKeigue PM, Shah B, Marmot MG. Relation of central obesity and insulin resistance with high diabetes prevalence and cardiovascular risk in South Asians. Lancet (London, England). 1991;337(8738):382–6.
Kanaya AM, Wassel CL, Mathur D, Stewart A, Herrington D, Budoff MJ, et al. Prevalence and correlates of diabetes in South asian indians in the United States: findings from the metabolic syndrome and atherosclerosis in South asians living in america study and the multi-ethnic study of atherosclerosis. Metab Syndr Relat Disord. 2010;8(2):157–64.
Garduño-Diaz SD, Khokhar S. Prevalence, risk factors and complications associated with type 2 diabetes in migrant South Asians. Diabetes/metabolism research and reviews. 2012;28(1):6–24.
Agyemang C, van der Linden EL, Bennet L. Type 2 diabetes burden among migrants in Europe: unravelling the causal pathways. Diabetologia. 2021;64(12):2665–75.
Jenum AK, Diep LM, Holmboe-Ottesen G, Holme IMK, Kumar BN, Birkeland KI. Diabetes susceptibility in ethnic minority groups from Turkey, Vietnam, Sri Lanka and Pakistan compared with Norwegians - the association with adiposity is strongest for ethnic minority women. BMC Public Health. 2012;12(1):150.
Tran AT, Diep LM, Cooper JG, Claudi T, Straand J, Birkeland K, et al. Quality of care for patients with type 2 diabetes in general practice according to patients’ ethnic background: a cross-sectional study from Oslo, Norway. BMC Health Serv Res. 2010;10:145.
Sattar N, Gill JM. Type 2 diabetes in migrant south Asians: mechanisms, mitigation, and management. The lancet Diabetes & endocrinology. 2015;3(12):1004–16.
Wium C, Aasheim ET, Ueland T, Michelsen AE, Thorsby PM, Larsen IF, et al. Differences in insulin sensitivity, lipid metabolism and inflammation between young adult Pakistani and Norwegian patients with type 2 diabetes: a cross sectional study. BMC Endocr Disord. 2013;13:49.
Turer AT, Scherer PE. Adiponectin: mechanistic insights and clinical implications. Diabetologia. 2012;55(9):2319–26.
Ouchi N, Parker JL, Lugus JJ, Walsh K. Adipokines in inflammation and metabolic disease. Nature reviews Immunology. 2011;11(2):85–97.
Lee S, Norheim F, Langleite TM, Gulseth HL, Birkeland KI, Drevon CA. Effects of long-term exercise on plasma adipokine levels and inflammation-related gene expression in subcutaneous adipose tissue in sedentary dysglycaemic, overweight men and sedentary normoglycaemic men of healthy weight. Diabetologia. 2019;62(6):1048–64.
Roden M, Shulman GI. The integrative biology of type 2 diabetes. Nature. 2019;576(7785):51–60.
Wu C, Borné Y, Gao R, López Rodriguez M, Roell WC, Wilson JM, et al. Elevated circulating follistatin associates with an increased risk of type 2 diabetes. Nat Commun. 2021;12(1):6486.
Stefan N, Haring HU. Circulating fetuin-A and free fatty acids interact to predict insulin resistance in humans. Nature medicine. 2013;19(4):394–5.
Gerst F, Wagner R, Kaiser G, Panse M, Heni M, Machann J, et al. Metabolic crosstalk between fatty pancreas and fatty liver: effects on local inflammation and insulin secretion. Diabetologia. 2017;60(11):2240–51.
Peter A, Kovarova M, Staiger H, Machann J, Schick F, Königsrainer A, et al. The hepatokines fetuin-A and fetuin-B are upregulated in the state of hepatic steatosis and may differently impact on glucose homeostasis in humans. Am J Physiol Endocrinol Metab. 2018;314(3):E266-e73.
Stefan N, Haring HU. The role of hepatokines in metabolism. Nat Rev Endocrinol. 2013;9(3):144–52.
Pal D, Dasgupta S, Kundu R, Maitra S, Das G, Mukhopadhyay S, et al. Fetuin-A acts as an endogenous ligand of TLR4 to promote lipid-induced insulin resistance. Nature medicine. 2012;18(8):1279–85.
Lee S, Norheim F, Gulseth HL, Langleite TM, Kolnes KJ, Tangen DS, et al. Interaction between plasma fetuin-A and free fatty acids predicts changes in insulin sensitivity in response to long-term exercise. Physiological reports. 2017;5(5).
Auberger P, Falquerho L, Contreres JO, Pages G, Le Cam G, Rossi B, et al. Characterization of a natural inhibitor of the insulin receptor tyrosine kinase: cDNA cloning, purification, and anti-mitogenic activity. Cell. 1989;58(4):631–40.
Mathews ST, Singh GP, Ranalletta M, Cintron VJ, Qiang X, Goustin AS, et al. Improved insulin sensitivity and resistance to weight gain in mice null for the Ahsg gene. Diabetes. 2002;51(8):2450–8.
Sindhu S, Akhter N, Shenouda S, Wilson A, Ahmad R. Plasma fetuin-A/α2-HS-glycoprotein correlates negatively with inflammatory cytokines, chemokines and activation biomarkers in individuals with type-2 diabetes. BMC Immunology. 2016;17(1):33.
Hennige AM, Staiger H, Wicke C, Machicao F, Fritsche A, Häring HU, et al. Fetuin-A induces cytokine expression and suppresses adiponectin production. PloS one. 2008;3(3):e1765.
Wium C, Gulseth HL, Eriksen EF, Birkeland KI. Characteristics of glucose metabolism in Nordic and South Asian subjects with type 2 diabetes. PloS one. 2013;8(12):e83983.
Wium C, Eggesbø HB, Ueland T, Michelsen AE, Torjesen PA, Aukrust P, et al. Adipose tissue distribution in relation to insulin sensitivity and inflammation in Pakistani and Norwegian subjects with type 2 diabetes. Scand J Clin Lab Invest. 2014;74(8):700–7.
DeFronzo RA, Tobin JD, Andres R. Glucose clamp technique: a method for quantifying insulin secretion and resistance. The American journal of physiology. 1979;237(3):E214-23.
Mosteller RD. Simplified calculation of body-surface area. The New England journal of medicine. 1987;317(17):1098.
Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clinical chemistry. 1972;18(6):499–502.
Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82.
Hartwig S, Raschke S, Knebel B, Scheler M, Irmler M, Passlack W, et al. Secretome profiling of primary human skeletal muscle cells. Biochimica et biophysica acta. 2014;1844(5):1011–7.
Stefan N. Causes, consequences, and treatment of metabolically unhealthy fat distribution. The lancet Diabetes & endocrinology. 2020;8(7):616–27.
Lee SS, Park SH, Kim HJ, Kim SY, Kim MY, Kim DY, et al. Non-invasive assessment of hepatic steatosis: prospective comparison of the accuracy of imaging examinations. J Hepatol. 2010;52(4):579–85.
Jenum AK, Sletner L, Voldner N, Vangen S, Mørkrid K, Andersen LF, et al. The STORK Groruddalen research programme: A population-based cohort study of gestational diabetes, physical activity, and obesity in pregnancy in a multiethnic population. Rationale, methods, study population, and participation rates. Scand J Public Health. 2010;38(5 Suppl):60–70.
Pérez-Pérez A, Sánchez-Jiménez F, Vilariño-García T, Sánchez-Margalet V. Role of Leptin in Inflammation and Vice Versa. Int J Mol Sci. 2020;21(16):5887.
Guo H, Qiu X, Deis J, Lin T-Y, Chen X. Pentraxin 3 deficiency exacerbates lipopolysaccharide-induced inflammation in adipose tissue. International Journal of Obesity. 2020;44(2):525–38.
Lee WJ, Wu CS, Lin H, Lee IT, Wu CM, Tseng JJ, et al. Visfatin-induced expression of inflammatory mediators in human endothelial cells through the NF-κB pathway. International Journal of Obesity. 2009;33(4):465–72.
Okan G, Baki AM, Yorulmaz E, Doğru-Abbasoğlu S, Vural P. Serum Visfatin, Fetuin-A, and Pentraxin 3 Levels in Patients With Psoriasis and Their Relation to Disease Severity. J Clin Lab Anal. 2016;30(4):284–9.
Stefan N, Häring HU, Cusi K. Non-alcoholic fatty liver disease: causes, diagnosis, cardiometabolic consequences, and treatment strategies. The lancet Diabetes & endocrinology. 2019;7(4):313–24.
Dervisoglu E, Kir HM, Kalender B, Caglayan C, Eraldemir C. Serum fetuin–a concentrations are inversely related to cytokine concentrations in patients with chronic renal failure. Cytokine. 2008;44(3):323–7.
Gangneux C, Daveau M, Hiron M, Derambure C, Papaconstantinou J, Salier JP. The inflammation-induced down-regulation of plasma Fetuin-A (alpha2HS-Glycoprotein) in liver results from the loss of interaction between long C/EBP isoforms at two neighbouring binding sites. Nucleic Acids Res. 2003;31(20):5957–70.
Acknowledgements
We are grateful to Cecilie Wium who initiated these studies and sadly passed away recently. We greatly acknowledge the staff engineer Anne-Randi Engset for performing the NEFA analyses for our study. We also thank the study nurses Åse Halsne and Gøril Vinje at the Diabetes Research Laboratory, Hormone Laboratory, Oslo University Hospital, and medical students Ruben Jensen and Thorbjørn Sandem, for their invaluable help in performing the study procedures. We thank BLS Lise-Marit Amlie, Hormone Laboratory, for her kind assistance during the planning and performing the study. We thank Dr. Anh T. Tran for sharing her data, used for background evaluation of our patient sample. We acknowledge LifeScan Inc. for supplying test strips for the OneTouch Ultra glucose monitoring device. The study was funded by the University of Oslo and the Eastern Norway Regional Health Authority, with contributions from Aker University Hospital, the Norwegian Diabetes Association, and Freia Chokolade Fabrik’s Medical Foundation. We also acknowledge generous support to our research from the Simon Fougner Hartmanns familiefond. The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
CW and KIB conceived DIPI, participated in its design and coordination, and researched data. CW, SL, and KIB initiated this sub-study. SL performed the statistics and wrote the manuscript. CAD researched data and critically revised the manuscript. ETA researched data and critically revised the manuscript. TU performed analyses of inflammation markers and contributed to the discussion. BH and AEM performed analyses of inflammation markers. performed analyses of inflammation markers. PMT participated in the design of the study and revised the manuscript. IFL conceived of the study and participated in patient recruitment. PAT provided the insulin and adipokine analyses and revised the manuscript. PA contributed to the discussion and critically revised the manuscript. KIB conceived of the study, participated in its design, contributed to discussion, and critically revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained from each participant before enrolment and the study was carried out according to the Helsinki Declaration and approved by the Eastern Norway Regional Committee for Medical and Health Research Ethics.
Consent for publication
The authors give the publisher license of the copyright which provides the publisher with the exclusive right to publish and sell the research findings in all languages, in whole or in part.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lee-Ødegård, S., Ueland, T., Thorsby, P.M. et al. Fetuin-A mediates the difference in adipose tissue insulin resistance between young adult pakistani and norwegian patients with type 2 diabetes. BMC Endocr Disord 22, 208 (2022). https://doi.org/10.1186/s12902-022-01127-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-022-01127-y