
Abstract
Objective
Polymorphisms of the fatty acid desaturase (FADS) gene cluster have been associated with obesity and its-related consequences. This cross-sectional study aimed to investigate whether the adherence to dietary non-enzymatic antioxidant capacity (NEAC), reflecting the antioxidant potential of the whole diet, modifies the association of FADS2 rs174583 polymorphism with cardio-metabolic risk factors in obese adults.
Methods
The present study included 347 healthy obese adults (aged 20–50 years). Dietary NEAC was assessed by a validated food frequency questionnaire with 147 items and estimated through total radical-trapping antioxidant parameters (TRAP), oxygen radical absorbance capacity (ORAC), and ferric reducing ability of plasma (FRAP) with the use of published databases. FADS2 rs174583 polymorphism was characterized using PCR–RFLP. ANCOVA multivariate interaction model was used to analyze gene-diet interactions.
Results
after adjustment for the confounding variables (age, physical activity, SES and WC), this study showed significant interactions between rs174583 polymorphism and adherence to dietary ORAC on the serum cholesterol (P Interaction = 0.029), LDL-C (P Interaction = 0.025) and HDL-C levels (P Interaction = 0.049) among the male group; minor allele carriers who had the highest adherence to the NEAC (ORAC) showed a better metabolic profile (lower TG and LDL-C and higher HDL-C) (P < 0.05). Among women, the dietary ORAC-rs174583 interactions were statistically significant for the serum insulin concentration (P Interaction = 0.020), QUICKI (P Interaction = 0.023) and HOMA-IR (P Interaction = 0.017); the highest QUICKI and the lowest HOMA-IR and serum insulin levels were observed in the CC homozygote carriers with the moderate compliance with the dietary ORAC (P < 0.05). In addition, the dietary TRAP modified the association between FADS2 variant and change in LDL-C levels (P Interaction = 0.037); the homozygous wild-type (CC) women who placed in the top tertile of TRAP had significantly the lowest LDL-C levels than those in the second tertile (P < 0.05).
Conclusion
These data indicate that the FADS2 rs174583 polymorphism interacts with the dietary NEAC to influence cardio-metabolic risk factors in obese subjects. Replication in prospective cohort studies among other populations is required to confirm the results of our study.
Similar content being viewed by others

What is already known about this topic?
The role of fatty acid desaturase 2 genetic variants in promoting obesity and obesity-related disorders like insulin resistance and dyslipidemia is reported in previous studies. However, it is unknown that how dietary indices particularly dietary antioxidants can alleviate the role of these genetic variants in the obesity-related comorbidities.
What does this article add?
In the current work, for the first time, we evaluated the effects of dietary non-enzymatic antioxidant capacity (NEAC) on cardio-metabolic risk factors among different genotypes of the fatty acid desaturase 2 genetic variant in obese individuals to further highlight the role of dietary antioxidant indices in prevention of genetic susceptibility to obesity-associated disorders.
Introduction
Obesity, as a major global health problem, is increasing at an alarming rate worldwide [1]. It has been estimated that globally, more than 13% of the world's adult population are obese. Similarly, based on available national data, approximately 22% of Iranian adults were affected by obesity in 2016 [2]. There is accumulating evidence showing that plasma fatty acids composition has significant effects on development of obesity-related non-communicable diseases [3]. On the other hand, both experimental and clinical studies have suggested that oxidative stress which is characterized by reduced antioxidant capacity and/or overproduction of reactive oxygen species (ROS) plays an important role in the development of obesity-related health outcomes [4].
Obesity is a multifactorial abnormality caused by both environmental and genetic factors and complex interactions between them [5]. Diet, as a key environmental factor, can interact with genetic background to affect the susceptibility to plenty of diseases [6]. Several studies have provided evidence that intake of dietary compounds with antioxidant activity is inversely associated with oxidative stress–induced conditions such as obesity [7]. Recently, the concept of dietary total antioxidant capacity (TAC) has been introduced to estimate the cumulative effects of antioxidants in the overall diet [8]. Dietary non-enzymatic total antioxidant capacity (NEAC), also known as TAC, can be measured through different chemical assays: oxygen radical absorbance capacity (ORAC), ferric reducing ability of plasma (FRAP) and total radical-trapping antioxidant parameters (TRAP) [9]. Numerous studies have indicated that dietary NEAC values are inversely related to cardio-metabolic risk factors [10] and other diet-related non-communicable diseases such as cardiovascular disease (CVD) [11], type 2 diabetes (T2D) [12], and cancers [13]. Nevertheless, the current evidence with regard to the relationship between NEAC and health outcomes is far from conclusive [14]. In addition, research regarding the effects of dietary NEAC on health outcomes has mostly been carried out in the western countries [15] and limited information is available from the middle-eastern populations [16].
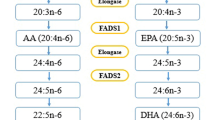
Interestingly, fatty acids status has been related to the risk of multiple diet-related chronic diseases [17] and, accordingly, the determinants of fatty acid metabolism such as genetic variants in fatty acid desaturases (FADS) should be completely understood. Recently, genome wide association studies (GWAS) have indicated that polymorphisms in the FADS gene cluster have a main effect on obesity and other metabolic diseases [18, 19]. The FADS1 and FADS2 genes, located closely on the chromosome 11 (11q12–13.1), encode delta-5-desaturase (D5D) and delta-6-desaturase (D6D), respectively; the essential enzymes involved in the homeostasis of polyunsaturated fatty acids (PUFA) [20, 21]. Reports indicate that changes in the activity of D5D and D6D enzymes can lead to alteration in the profile of endogenous fatty acids and subsequently, development of non-communicable diseases, such as obesity, T2D, metabolic syndrome (MetS), and CVDs [22, 23]. A number of recent studies have revealed that the activities of these enzymes can be affected by single‐nucleotide polymorphisms (SNPs) of FADS1 and FADS2 genes [24, 25]. However, the results of studies are not consistent enough to approve the outcomes of SNP association studies; this suggests that interactions between genetic and environmental factors such as diet may be influential. On the other hand, a number of studies have demonstrated that oxidative stress is involved in the pathogenesis of psychiatric diseases which may cause development of obesity and its-related metabolic complications [26]. Therefore, a diet high in antioxidants may protect against oxidative stress and result in improvement of the mental health [27]. In other words, obesity-related consequences are affected by the interactions between psychological parameters, obesogenic environment such as unhealthy dietary intakes and sedentary lifestyle [28]. Hence, assessment of gene-diet interactions is important as it helps to generate individualized effective dietary strategies [29]. So, we aimed to examine how dietary antioxidant capacity interacts with genetic variant of FADS2 (rs174583) in relation to changes in cardio-metabolic risk factors of obese adults.
Materials and methods
Participants
This cross-sectional study was conducted in Tabriz city, one of the major cities in the northwest of Iran, during November 2017 to October 2018. Individuals were enrolled using convenience sampling method through announcements and posters placed in public areas of the city. Participants were included if they met the following criteria: good health, obesity (body mass index (BMI) ≥ 30) and ages of 20–50 years. At the beginning of the study, 400 participants were willing to participate in the study. The exclusion criteria were pregnancy, lactation, menopause, a history of CVDs, T2D, cancer, renal disease, hypertension, hyperlipidemia and hepatic disorders or taking any medications and supplements which influence weight and variables studied such as loop diuretics, cortico-steroids, antidepressants, antihypertensive agents and statins, any recent surgery such as bariatric, and daily energy intake outside the range of 800–4200 kcal/day [30, 31]. Finally, all these exclusions left 347 subjects for analysis. To calculate the sample size, the association between dietary quality indices and obesity was considered as a key dependent variable. For this purpose, with regard to the correlation coefficient (r) of 0.25 [32], α = 0.05 and power of 80%, using G-power software, the minimum sample size was estimated at 160. To perform sex-stratified analyses, the final sample size of 340 was considered for our study. Written informed consent was obtained from each participant before taking part in this study and the study protocol was approved by the ethics committee of the Tabriz University of Medical Sciences (registration code IR.TBZMED.REC.1400.889).
Definition of MetS
The presence of MetS was identified based on criteria established by the Iranian National Committee of Obesity [33]. Participants with three or more of the following criteria were considered to have MetS: waist circumference > 95 cm (men and women), high blood pressure (systolic blood pressure (SBP) ⩾130 mmHg or diastolic blood pressure (DBP) ⩾85 mmHg, fasting triglyceride (TG) level ⩾150 mg/dl, fasting high-density lipoprotein cholesterol (HDL-C) level less than 40 mg/dl (men) or 50 mg/dl (women), and fasting blood sugar ⩾100 mg/dl.
Dietary intake and dietary non-enzymatic antioxidant capacity assessment
Usual dietary intake during the previous year was assessed via face-to-face interviews using a valid and reliable 147-items semi-quantitative food-frequency questionnaire (FFQ) [34, 35]. All information was collected by trained dietitians. Participants were asked to report their frequency and amount of the intake of each food item during the last year based on a daily, weekly, monthly basis and then by using household measures, portion sizes of consumed foods were converted to gram/day. Daily intake of energy and nutrients collected through the FFQ were analyzed using Iranian Food Composition Table (FCT) [35] and complemented with the USDA FCT [36].
The values of NEAC, as a marker of dietary antioxidant potential, were calculated using the following indicators [9, 37, 38]: FRAP which measures the in vitro reduction of the ferric ion to ferrous ion in the presence of antioxidants, TRAP which measures the chain-breaking antioxidant potential to scavenge peroxyl radicals and ORAC that estimates the antioxidant capacity against peroxyl radicals by measuring the area under the curve of radical-induced fluorescence decay. Since there was no available database to calculate the quantity of antioxidants in Iranian foods, ORAC, FRAP and TRAP values assigned to each food item were obtained from previously published databases [37, 39, 40]. We assigned the NEAC for 100, 59, and 57 food items in the FFQ by ORAC, FRAP, and TRAP, respectively. We calculated dietary NEAC without the contribution of coffee since it remains unclear whether the main contributors to the in vitro antioxidant capacity of coffee; the Maillard products from the coffee roasting process, are absorbed efficiently due to their high molecular weight and if the same antioxidant activity is displayed in vivo [41]. To calculate total daily dietary NEAC for every participant, the frequency of consumption of each food item was multiplied by its corresponding NEAC values and, then, they were summed up. Subjects were categorized based on tertiles of ORAC, FRAP and TRAP.
Socio-demographic, blood pressure and anthropometric measurements
General information such as age, gender, marital status, smoking, medical history, and socioeconomic status (SES) was collected using questionnaires which were administered to individuals by face-to-face interviews [42]. SES was determined through the following questions: educational status, occupational position, house ownership, and family size which were considered as individual indicators. In the current study, education was measured as a categorical variable where participants were asked to specify their highest level of educational attainment. This variable was recorded on a 5-point scale ranging from 0 to 5 (illiterate: 0, less than diploma: 1, diploma and associate degree: 2, bachelors: 3, masters: 4 and higher: 5). Female subjects’ occupational class was categorized into five groups (housewife, employee, student, self-employed and others). Occupational status of male subjects was categorized as follow: unemployed: 1, worker, farmer and rancher: 2, others: 3, employee: 4 and self-employed: 5. Accordingly, participants were categorized as ≤ 3, 4–5, ≥ 6 in terms of family size. Besides, they were given scores 1 and 2 if they were tenant and landlord, respectively. Next, each participant received a score between zero and 15 for the whole SES score and, then, individuals were classified into 3 categories: low, middle, and high according to SES tertiles. A short version of the International Physical Activity Questionnaire (IPAQ) was used to assess the physical activity level of participants [43]. Body weight of participants was measured in light clothing using a Seca scale (Seca, Germany) with an accuracy of 0.1 kg. A tape measure with a precision of 0.1 cm was used to measure height while subjects were standing in the normal position without shoes. Participants’ body composition measurements were conducted through bioelectrical impedance analysis (BIA) technology (Tanita, BC-418 MA, Tokyo, Japan). Waist circumference was obtained in the slimmest area while participants were at the end of a normal exhalation, using an unscratched tape and was recorded to the nearest 0.1 cm. SBP and DBP were measured using a mercury sphygmomanometer twice, after 15 min rest in a sitting position and finally, the average of the two measurements was recorded.
Mental health and appetite assessments
The severity of the various mental disorders was determined using a validated self-administered the Depression, Anxiety and Stress Scale-21 Items (DASS-21) questionnaire [44, 45]. The Cronbach’s alpha (internal consistency) for the DASS questionnaire in Iranian population has been reported as follows: 0.77 for depression, 0.79 for anxiety, and 0.78 for stress [44]. This questionnaire consists of 21 items comprising 3 subscales of 7 items which assess the emotional states of depression, anxiety and stress over the last week. Each item in this instrument was rated based on a Likert scale from 0 “did not apply to me at all” to 3 “applied to me very much or most of the time” through individual structured interviews with the subjects. The related items scores for each subscale were summed and multiplied by a factor 2 to give a total score that ranges from 0 to 42 and then participants were divided into 5 categories: normal, mild, moderate, severe and extremely severe, according to cut-off scores which have been proposed by Lovibond and Lovibond [46]. Higher subscale scores reflect more severe psychological disorders.
To assess participant’s appetite level, a 10-cm visual analog scale (VAS) questionnaire, with prior evidence of validity and reliability, was applied [47]. This tool includes different questions about feeling of hunger, satiation, fullness, prospective food consumption, thirst, and the desire to eat something sweet, salty, or fat. Participants were asked to complete this questionnaire by making a mark across a 100 mm horizontal line corresponding to their feelings and, subsequently, VAS score was determined by measuring the distance from the left side of the line to the mark. For the rest of information about technical methodology, see the supplementary data.
Statistical analysis
Normal distribution of data was checked by descriptive measures such as coefficients of skewness and kurtosis, mean and standard deviation [48]. Data were presented as means ± standard deviations for normally distributed quantitative variables, the median (25th and 75th percentile) for variables with skewed distributions and the frequency (%) for discrete variables. The comparison of categorical variables was performed by Chi-square test. Quantitative variables with normal and non-normal distribution were compared with Analysis of variance (ANOVA) and the Kruskal–Wallis tests, respectively. Sex-stratified multivariable multinomial logistic regression analysis was applied to test the associations between dietary NEAC and rs174583 polymorphism of FADS2 gene. The potential interactions between FADS2 polymorphism (rs174583) and dietary NEAC on cardio-metabolic risk factors based on sex groups were examined by ANCOVA multivariate interaction model, after controlling for confounding variables (age, physical activity, SES and WC). Since the interaction effects are difficult to explain, all significant interactions were depicted as graphs to help their interpretations. All statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS, Inc., Chicago, IL, version 21). A P-value less than 0.05 was considered to be statistically significant in all analyses.
Results
Study population characteristics
Briefly, after application of the exclusion criteria, 53 potential subjects were excluded from the study and, consequently, 347 healthy obese adults (58.2% male, 41.8% female) aged 20 to 50 years were recruited.
Comparisons between FADS2 rs174583 genotypes
The general characteristics of participants based on FADS rs174583 genotypes are provided in Table 1. No significant differences were found regarding anthropometric, socio-demographic, dietary and mental health parameters across FADS2 rs174583 genotypes; neither in men nor in women.
Associations of FADS2 rs174583 with dietary NEAC
Table 2 presents sex-stratified analysis for the relationship between dietary NEAC and FADS rs174583 genotypes. No statistically significant association was found between NEAC indicators and FADS2 polymorphism; neither in crude nor in the adjusted models among both female and male subjects.
Differences in distribution of MetS and means of cardio-metabolic variables between FADS2 rs174583 genotypes according to gender
Sex-stratified analysis for the association between laboratory and clinical parameters and FADS rs174583 genotypes are displayed in Table 3. As shown in this Table, male TT-genotype carriers had higher mean values of TG (P = 0.037) and AIP (P = 0.041) compared to other genotype categories (CT, CC), whereas no significant associations were revealed among female participants.
Sex-stratified interaction analysis between dietary NEAC and FADS2 rs174583 in relation to cardio-metabolic risk factors
We performed sex-stratified covariance analyses to verify whether adherence to the dietary NEAC modifies the association of the FADS2 rs174583 polymorphism with cardio-metabolic risk factors. Subsequently, statistically significant interactions are illustrated in Figs. 1 and 2. Among male participants, after adjustment for confounding variables (age, physical activity, SES and WC), the interactions between rs174583 polymorphism and adherence to dietary ORAC on serum cholesterol (P Interaction = 0.029), LDL-C (P Interaction = 0.025) and HDL-C levels (P Interaction = 0.049) were statistically significant. In male CT-genotype carriers, the serum levels of cholesterol (P = 0.004) and LDL-C (P = 0.001) in subjects who assigned to the highest tertile of ORAC were significantly lower than subjects in the first category. Additionally, male subjects with homozygous minor allele genotype had higher means of HDL-C when had the highest compliance with dietary ORAC (P = 0.029). From our analyses among women, the dietary ORAC-rs174583 interactions were statistically significant for serum insulin concentrations (P Interaction = 0.020), QUICKI (P Interaction = 0.023) and HOMA-IR (P Interaction = 0.017) even after adjustment for confounding variables. According to these interactions, in CC genotype group, serum insulin levels (P = 0.026) and HOMA-IR (P = 0.010) were significantly lower in female participants who were assigned in the second tertile of dietary ORAC in comparison with the first category. In contrast, the highest QUICKI was observed in the female CC-genotype carriers who had moderate compliance with the dietary ORAC (P = 0.018). Moreover, we found a relevant interaction between adherence to the dietary FRAP in relation to serum HDL-C concentrations (P Interaction = 0.039) among women, whereas adjustment for potential confounders eliminated this significant interaction. In addition, the dietary TRAP modified the association between FADS2 variant and change in LDL-C levels (P Interaction = 0.037); the homozygous wild-type (CC) women who placed in the top tertile of TRAP had significantly the lowest LDL-C levels than those in the second tertile (P = 0.018).

Interaction between FADS2 rs174583 and dietary ORAC on serum concentration of cholesterol (A), LDL-C (B) and HDL-C (C) among men. Interaction between FADS2 rs174583 and dietary ORAC on serum insulin level (D)

Interaction between FADS2 rs174583 and dietary ORAC on QUICKI (E) and HOMA-IR among women (F). Interaction between FADS2 rs174583 and dietary TRAP on serum LDL-C level among women (G) and all P-values of interactions were adjusted for age, WC, physical activity and socio-economic status. Interaction between FADS2 rs174583 and dietary FRAP on serum concentration of HDL-C among women in crude model (H). The bars indicate mean. Error bars: SE of means
Discussion
To the best of our knowledge, this is the first study that has investigated the interactions between FADS2 gene polymorphism (rs174583) and dietary NEAC in relation to cardio-metabolic risk factors. We documented the interactions of FADS2 gene rs174583 SNP with dietary NEAC (ORAC), in changing serum lipid profiles among male subjects; minor allele carriers who had the highest adherence to the NEAC showed a better metabolic profile (lower TG and LDL-C and higher HDL-C). Among female subjects, dietary ORAC intake modified the relationship of FADS2 variant with glycemic indices; the highest QUICKI and the lowest HOMA-IR and serum insulin levels were observed in the CC homozygote carriers with moderate compliance with the dietary ORAC. Additionally, being in the highest tertiels of TRAP could show beneficial effects in decreasing LDL-C in homozygous females for the major allele (CC).
The frequency of T minor allele of FADS2 rs174583 polymorphism was 36% which was lower than what had been previously reported in European (HapMap database) and Taiwanese population [49]. Differences in study design, sample size, dietary habits, lifestyle and population characteristics such as ethnicity may partly explain the discrepancies in allele frequencies among different studies.
Although no association was found between psychiatric variables and rs174583 in the current research, it has been shown that minor allele of the FADS2 rs174583 has a positive relationship with perinatal depressive disorders risk among Canadian women [50]. Besides, it is generally supposed that abnormalities exist in the composition of fatty acids particularly ω-3 PUFAs in human tissues, play an important role in the pathogenesis of both mood disorders and chronic diseases such as CVDs [51, 52]. In the present study, we documented significant differences in serum TG level and AIP between different genotypes; TT genotype group had a higher TG and AIP compared to other genotype categories, which were in accordance with some previous studies [53, 54]. For instance, a recent publication by Mazoochian et al. reported a higher level of TG in minor allele homozygote group (TT) of rs174583 than CT heterozygote carriers with T2D [53]. Despite the fact that exact mechanisms contribute to the association between FADS genetic variants and disease development remain unknown; current evidence has suggested that FADS genetic variations may impair desaturases leading to changes in n-3/n-6 PUFA status which has been associated with the risk of several chronic diseases [49, 55].
Generally, the present study showed that improving adherence to dietary NEAC (reflected in ORAC and TRAP) can significantly attenuate the genetic association with cardio-metabolic risk factors. These findings propose that male carriers of the minor allele (CT and TT) and female homozygous carriers of the major allele (CC) of FADS2 rs174583 appear to be protected against increase in metabolic risk factors when they consume antioxidant-rich foods. As mentioned above, some of the significant interactions were found to be sex-specific. There is no clear mechanism to explain these gender-dependent heterogeneities; however, difference in regional depots of adipose tissue and hormonal status may be reasons for these sex-based differences [56]. Besides, it seems that the non-significant higher dietary NEAC score may help to describe, in part, these inconsistences. For example, men with TT genotype had a non-significant higher median of ORAC compared with other genotypes (CT and CC). A wealth of evidence has accumulated about gender differences in dietary intakes and eating behavior; compared to men, women had healthier dietary pattern, lifestyle and food choices [57]. To date, there is no study in the literature regarding the interactions between FADS2 rs174583 and dietary antioxidant intakes, as measured by overall NEAC scores, in relation to health outcomes with which we can directly compare our findings. Nonetheless, our results are supported by some observational studies in which a modulation by diet on the association of the FADS1 and FADS2 genes with metabolic disorders like MetS has been reported [55, 58]. In a recent cross-sectional genome wide association study (GWAS) on Korean population, Park et al. revealed statistically significant interactions between total fat intake and the FADS1 rs174547 and haplotype of FADS1 rs174547 and FADS2 rs2845573 on MetS risk and it seemed that intermediate fat intake protected carriers of the FADS1 major alleles against the risk of MetS [58]. Additionally, these findings are consistent with our previous study in which good adherence to the dietary NEAC could attenuate the association of melanocortin 4 receptor (MC4R) gene polymorphism with some of metabolic risk factors [59]. Since the majority of studies which have documented a protective role for dietary NEAC against obesity [10] and other health outcomes such as MetS [60], cancers [13] and T2D [12], it is not surprising that high intakes of NEAC neutralize detrimental effects of greater genetic predisposition to cardio-metabolic risk factors in FADS2 minor allele carriers that this means these individuals are more likely to respond to high intakes of dietary antioxidants. These protective influences of antioxidant-rich foods on metabolic status may happen through increasing insulin sensitivity and thermogenesis, regulation of appetite and modification of lipids and carbohydrate metabolism [61]. Nonetheless, in the present study, no significant difference in mean of appetite score was found between rs174583 genotypes and different tertiles of NEAC (data have not shown). It is worth noting that regulation of appetite is a complex mechanism involving the connections between hypothalamus and the brainstem within the central nervous system (CNS), gastrointestinal tract and adipose tissue [62]. Thus, it didn’t appear that antioxidant-rich foods lonely have favorable effects on appetite in our study. However, it has been shown that high intake of foods rich in bioactive redox substances such as vegetables and fruits exert health benefits not only by protecting against oxidative damages, but also through providing magnesium, fiber, potassium, and other phytochemicals which may have synergetic effects on prevention of human diseases [63].
The present study had some potential limitations that should to be taken into account when interpreting the results. First, since it was a cross-sectional, causation cannot be inferred, while these results can provide the hypothesis that can then be assessed more rigorously via prospective cohort or other studies. Second, the relatively small sample size of studied subjects was a serious and major limitation of the present research which may restrict the achievement of an adequate statistical power. Thus, our results need to be taken with caution and replicated in large longitudinal studies. Third, as obese adults tend to underreport their dietary intakes, it may cause misclassifications in dietary variables and this potential bias may consequently result in an underestimate of the true effect. For this reason, subjects with extreme dietary intake values were removed from the analyses. Forth, although we controlled carefully for several confounders in the analyses, residual unknown confounders that might distort the findings could not be fully eliminated. Fifth, to calculate NEAC, the international databases were used as there were no NEAC values for the local foods. It should be notice that due to different growing conditions and geographic location, using antioxidant values from other countries may not be appropriate and these figures may not be the same for Iranian foods. Nevertheless, it has been shown that the assessment of dietary NEAC through FFQ is a valuable and valid measure in epidemiological studies [63, 64]. Sixth, the assessment of dietary NEAC does not take into account metabolism or antioxidant bioavailability. Furthermore, other variants within the FADS gene cluster, as well as variants in other genes contribute to the pathogenesis of obesity and related- metabolic phenotypes. Last, since this study was carried out among population from Tabriz city, the generalizability cannot be taken for granted.
Conclusion
Our findings for the first time suggest that the dietary NEAC intakes may modify the association of the genetic variation in FADS2 with cardio-metabolic risk factors. So, our results provide more evidence that recommendation of antioxidant-rich foods can be a suitable strategy for disease prevention and health promotion particularly in people with susceptible genotypes; however replication in large cohort of other population is required.
Availability of data and materials
Data used in the study cannot be deposited publically because of some institutional restrictions; however, data could be available by reasonable from the corresponding author.
Abbreviations
- AIP:
-
The atherogenic index of plasma
- ANOVA:
-
Analysis of variance
- BIA:
-
Bioelectrical impedance analysis
- BMI:
-
Body mass index
- CVD:
-
Cardiovascular disease
- DASS-21:
-
Depression, Anxiety and Stress Scale-21 Items
- DBP:
-
Diastolic blood pressure
- D5D:
-
Delata-5-desaturase
- D6D:
-
Delta-6-desaturase
- ELISA:
-
Enzyme-linked immunosorbent assay
- FADS :
-
Fatty acid desaturases
- FCT:
-
Food Composition Table
- FFQ:
-
Food-frequency questionnaire
- FRAP:
-
Ferric reducing ability of plasma
- GWAS:
-
Genome wide association study
- HDL-C:
-
High-density lipoprotein cholesterol
- HOMA-IR:
-
Homeostasis model assessment-insulin resistance index
- IPAQ:
-
International Physical Activity Questionnaire
- LDL-C:
-
Low-density lipoprotein-cholesterol
- MC4R:
-
Melanocortin 4 receptor
- MetS:
-
Metabolic syndrome
- NEAC:
-
Non-enzymatic total antioxidant capacity
- ORAC:
-
Oxygen radical absorbance capacity
- PUFA:
-
Polyunsaturated fatty acids
- PCR–RFLP:
-
Polymerase chain reaction-restricted length polymorphism
- QUICKI:
-
Quantitative insulin sensitivity check index
- ROS:
-
Reactive oxygen species
- SBP:
-
Systolic blood pressure
- SES:
-
Socioeconomic status
- SNPs:
-
Single‐nucleotide polymorphisms
- SPSS:
-
Statistical Package for Social Sciences
- TAC:
-
Total antioxidant capacity
- TG:
-
Triglyceride
- TRAP:
-
Total radical-trapping antioxidant parameters
- T2D:
-
Type 2 diabetes
- VAS:
-
Visual analog scale
References
Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15(5):288–98. https://doi.org/10.1038/s41574-019-0176-8.
Djalalinia S, Saeedi Moghaddam S, Sheidaei A, Rezaei N, Naghibi Iravani SS, Modirian M, et al. Patterns of Obesity and Overweight in the Iranian Population: Findings of STEPs 2016. Front Endocrinol. 2020;11:42. https://doi.org/10.3389/fendo.2020.00042.
Steffen LM, Vessby B, Jacobs DR Jr, Steinberger J, Moran A, Hong CP, et al. Serum phospholipid and cholesteryl ester fatty acids and estimated desaturase activities are related to overweight and cardiovascular risk factors in adolescents. Int J Obes (2005). 2008;32(8):1297–304. https://doi.org/10.1038/ijo.2008.89.
Maritim AC, Sanders RA, Watkins JB 3rd. Diabetes, oxidative stress, and antioxidants: a review. J Biochem Mol Toxicol. 2003;17(1):24–38. https://doi.org/10.1002/jbt.10058.
Herrera BM, Lindgren CM. The genetics of obesity. Curr DiabRep. 2010;10(6):498–505. https://doi.org/10.1007/s11892-010-0153-z.
Grosso G. Impact of nutritional risk factors on chronic non-communicable diseases. Eur J Public Health. 2019;29(Supplement_4):ckz185-197. https://doi.org/10.1093/eurpub/ckz185.197.
Frei B. Efficacy of Dietary Antioxidants to Prevent Oxidative Damage and Inhibit Chronic Disease. J Nutr. 2004;134(11):3196S-S3198. https://doi.org/10.1093/jn/134.11.3196S.
Carlsen MH, Halvorsen BL, Holte K, Bøhn SK, Dragland S, Sampson L, et al. The total antioxidant content of more than 3100 foods, beverages, spices, herbs and supplements used worldwide. Nutr J. 2010;9:3. https://doi.org/10.1186/1475-2891-9-3.
Pellegrini N, Serafini M, Colombi B, Del Rio D, Salvatore S, Bianchi M, et al. Total antioxidant capacity of plant foods, beverages and oils consumed in Italy assessed by three different in vitro assays. J Nutr. 2003;133(9):2812–9. https://doi.org/10.1093/jn/133.9.2812.
Hermsdorff HH, Puchau B, Volp AC, Barbosa KB, Bressan J, Zulet M, et al. Dietary total antioxidant capacity is inversely related to central adiposity as well as to metabolic and oxidative stress markers in healthy young adults. Nutr Metab. 2011;8:59. https://doi.org/10.1186/1743-7075-8-59.
Rossi M, Praud D, Monzio Compagnoni M, Bellocco R, Serafini M, Parpinel M, et al. Dietary non-enzymatic antioxidant capacity and the risk of myocardial infarction: a case-control study in Italy. Nutr Metab Cardiovasc Dis. 2014;24(11):1246–51. https://doi.org/10.1016/j.numecd.2014.06.007.
Mancini FR, Affret A, Dow C, Balkau B, Bonnet F, Boutron-Ruault MC, et al. Dietary antioxidant capacity and risk of type 2 diabetes in the large prospective E3N-EPIC cohort. Diabetologia. 2018;61(2):308–16. https://doi.org/10.1007/s00125-017-4489-7.
Amiano P, Molina-Montes E, Molinuevo A, Huerta JM, Romaguera D, Gracia E, et al. Association study of dietary non-enzymatic antioxidant capacity (NEAC) and colorectal cancer risk in the Spanish Multicase-Control Cancer (MCC-Spain) study. Eur J Nutr. 2019;58(6):2229–42. https://doi.org/10.1007/s00394-018-1773-3.
Kashino I, Serafini M, Kurotani K, Akter S, Mizoue T, Ishihara J, et al. Relationship between dietary non-enzymatic antioxidant capacity and type 2 diabetes risk in the Japan Public Health Center-based Prospective Study. Nutrition (Burbank, Los Angeles County, Calif). 2019;66:62–9. https://doi.org/10.1016/j.nut.2019.03.011.
Hantikainen E, Löf M, Grotta A, Trolle Lagerros Y, Serafini M, Bellocco R, et al. Dietary non-enzymatic antioxidant capacity and risk of stroke: The Swedish Women’s Lifestyle and Health Cohort. Nutrition (Burbank, Los Angeles County, Calif). 2020;73:110723. https://doi.org/10.1016/j.nut.2020.110723.
Sotoudeh G, Abshirini M, Bagheri F, Siassi F, Koohdani F, Aslany Z. Higher dietary total antioxidant capacity is inversely related to prediabetes: A case-control study. Nutrition (Burbank, Los Angeles County, Calif). 2018;46:20–5. https://doi.org/10.1016/j.nut.2017.08.005.
Sergeant S, Hugenschmidt CE, Rudock ME, Ziegler JT, Ivester P, Ainsworth HC, et al. Differences in arachidonic acid levels and fatty acid desaturase (FADS) gene variants in African Americans and European Americans with diabetes or the metabolic syndrome. Br J Nutr. 2012;107(4):547–55. https://doi.org/10.1017/s0007114511003230.
Marklund M, Morris AP, Mahajan A, Ingelsson E, Lindgren CM, Lind L, et al. Genome-Wide Association Studies of Estimated Fatty Acid Desaturase Activity in Serum and Adipose Tissue in Elderly Individuals: Associations with Insulin Sensitivity. Nutrients. 2018;10(11):1791. https://doi.org/10.3390/nu10111791.
Aulchenko YS, Ripatti S, Lindqvist I, Boomsma D, Heid IM, Pramstaller PP, et al. Loci influencing lipid levels and coronary heart disease risk in 16 European population cohorts. Nat Genet. 2009;41(1):47–55. https://doi.org/10.1038/ng.269.
Cho HP, Nakamura MT, Clarke SD. Cloning, expression, and nutritional regulation of the mammalian Delta-6 desaturase. J Biol Chem. 1999;274(1):471–7. https://doi.org/10.1074/jbc.274.1.471.
Cho HP, Nakamura M, Clarke SD. Cloning, expression, and fatty acid regulation of the human delta-5 desaturase. J Biol Chem. 1999;274(52):37335–9. https://doi.org/10.1074/jbc.274.52.37335.
Vaittinen M, Walle P, Kuosmanen E, Männistö V, Käkelä P, Ågren J, Schwab U, Pihlajamäki J. FADS2 genotype regulates delta-6 desaturase activity and inflammation in human adipose tissue. J Lipid Res. 2016;57(1):56–65. https://doi.org/10.1194/jlr.M059113.
Merino DM, Ma DW, Mutch DM. Genetic variation in lipid desaturases and its impact on the development of human disease. Lipids Health Dis. 2010;18(9):63. https://doi.org/10.1186/1476-511X-9-63.
Nakayama K, Bayasgalan T, Tazoe F, Yanagisawa Y, Gotoh T, Yamanaka K, et al. A single nucleotide polymorphism in the FADS1/FADS2 gene is associated with plasma lipid profiles in two genetically similar Asian ethnic groups with distinctive differences in lifestyle. Hum Genet. 2010;127(6):685–90. https://doi.org/10.1007/s00439-010-0815-6.
Huang T, Sun J, Chen Y, Xie H, Xu D, Huang J, et al. Genetic variants in desaturase gene, erythrocyte fatty acids, and risk for type 2 diabetes in Chinese Hans. Nutrition (Burbank, Los Angeles County, Calif). 2014;30(7–8):897–902. https://doi.org/10.1016/j.nut.2014.01.006.
Ng F, Berk M, Dean O, Bush AI. Oxidative stress in psychiatric disorders: evidence base and therapeutic implications. Int J Neuropsychopharmacol. 2008;11(6):851–76.
Milajerdi A, Keshteli AH, Afshar H, Esmaillzadeh A, Adibi P. Dietary total antioxidant capacity in relation to depression and anxiety in Iranian adults. Nutrition. 2019;1(65):85–90.
Hamer M, Molloy GJ, Stamatakis E. Psychological distress as a risk factor for cardiovascular events: pathophysiological and behavioral mechanisms. J Am Coll Cardiol. 2008;52(25):2156–62.
Ahmad S, Fatima SS, Rukh G, Smith CE. Gene Lifestyle Interactions With Relation to Obesity, Cardiometabolic, and Cardiovascular Traits Among South Asians. Front Endocrinol. 2019;10:221. https://doi.org/10.3389/fendo.2019.00221.
Willett W. Nutritional epidemiology. 2nd ed. New York: Oxford University Press; 1998. p. 321–46.
Khodarahmi M, Azadbakht L, Daghaghzadeh H, Feinle-Bisset C, Keshteli AH, Afshar H, et al. Evaluation of the relationship between major dietary patterns and uninvestigated reflux among Iranian adults. Nutrition (Burbank, Los Angeles County, Calif). 2016;32(5):573–83. https://doi.org/10.1016/j.nut.2015.11.012.
Murray AE, McMorrow AM, O’Connor E, Kiely C, Mac Ananey O, O’Shea D, et al. Dietary quality in a sample of adults with type 2 diabetes mellitus in Ireland; a cross-sectional case control study. Nutr J. 2013;12:110. https://doi.org/10.1186/1475-2891-12-110.
Azizi F, Khalili D, Aghajani H, Esteghamati A, Hosseinpanah F, Delavari A, et al. Appropriate Waist Circumference Cut-off Points among Iranian Adults: The First Report of the Iranian National Committee of Obesity. Arch Iran Med. 2010;13:243–4.
Mirmiran P, Esfahani FH, Mehrabi Y, Hedayati M, Azizi F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 2010;13(5):654–62. https://doi.org/10.1017/s1368980009991698.
Esfahani FH, Asghari G, Mirmiran P, Azizi F. Reproducibility and relative validity of food group intake in a food frequency questionnaire developed for the Tehran Lipid and Glucose Study. J Epidemiol. 2010;20(2):150–8. https://doi.org/10.2188/jea.je20090083.
Asghari G, Yuzbashian E, Mirmiran P, Azizi F. The association between Dietary Approaches to Stop Hypertension and incidence of chronic kidney disease in adults: the Tehran Lipid and Glucose Study. Nephrol Dial Transplant. 2017;32(suppl_2):i224–30. https://doi.org/10.1093/ndt/gfw273.
Wu X, Beecher GR, Holden JM, Haytowitz DB, Gebhardt SE, Prior RL. Lipophilic and hydrophilic antioxidant capacities of common foods in the United States. J Agric Food Chem. 2004;52(12):4026–37. https://doi.org/10.1021/jf049696w.
Pellegrini N, Serafini M, Salvatore S, Del Rio D, Bianchi M, Brighenti F. Total antioxidant capacity of spices, dried fruits, nuts, pulses, cereals and sweets consumed in Italy assessed by three different in vitro assays. Mol Nutr Food Res. 2006;50(11):1030–8. https://doi.org/10.1002/mnfr.200600067.
Pellegrini N, Serafini M, Colombi B, Del Rio D, Salvatore S, Bianchi M, et al. Total antioxidant capacity of plant foods, beverages and oils consumed in Italy assessed by three different in vitro assays. J Nutr. 2003;133(9):2812–9.
Pellegrini N, Serafini M, Salvatore S, Del Rio D, Bianchi M, Brighenti F. Total antioxidant capacity of spices, dried fruits, nuts, pulses, cereals and sweets consumed in Italy assessed by three different in vitro assays. Mol Nutr Food Res. 2006;50(11):1030–8.
Morales FJ, Somoza V, Fogliano V. Physiological relevance of dietary melanoidins. Amino Acids. 2012;42(4):1097–109. https://doi.org/10.1007/s00726-010-0774-1.
Khodarahmi M, Asghari-Jafarabadi M, Abbasalizad FM. A structural equation modeling approach for the association of a healthy eating index with metabolic syndrome and cardio-metabolic risk factors among obese individuals. PLoS ONE. 2019;14(7):e0219193. https://doi.org/10.1371/journal.pone.0219193.
Booth M. Assessment of physical activity: an international perspective. Res Q Exerc Sport. 2000;71(Suppl 2):114–20. https://doi.org/10.1080/02701367.2000.11082794.
Sahebi A, Asghari M, Salari R. Validation of depression anxiety and stress scale (DASS-21) for an Iranian population. J Dev Psychol. 2005;1(4):12–22. [In Persian].
Samani S, Joukar B. A study on the reliability and validity of the short form of the depression anxiety stress scale (dass-21). J Soc Sci Hum Shiraz Univ. 2007;26(3, S52):65–77.
Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335–43. https://doi.org/10.1016/0005-7967(94)00075-u.
Flint A, Raben A, Blundell JE, Astrup A. Reproducibility, power and validity of visual analogue scales in assessment of appetite sensations in single test meal studies. Int J Obes Relat Metab Disord. 2000;24(1):38–48. https://doi.org/10.1038/sj.ijo.0801083.
Das K. A Brief Review of Tests for Normality. Am J Theor Appl Stat. 2016;5:5. https://doi.org/10.11648/j.ajtas.20160501.12.
Huang MC, Chang WT, Chang HY, Chung HF, Chen FP, Huang YF, et al. FADS gene polymorphisms, fatty acid desaturase activities, and HDL-C in type 2 diabetes. Int J Environ Res Public Health. 2017;14(6):572. https://doi.org/10.3390/ijerph14060572.
Xie L, Innis S. Association of Fatty Acid Desaturase Gene Polymorphisms with Blood Lipid Essential Fatty Acids and Perinatal Depression among Canadian Women: A Pilot Study. J Nutrigenet Nutrigenomics. 2009;2:243–50. https://doi.org/10.1159/000255636.
Severus WE, Littman AB, Stoll AL. Omega-3 fatty acids, homocysteine, and the increased risk of cardiovascular mortality in major depressive disorder. Harv Rev Psychiatry. 2001;9(6):280–93.
Hibbeln JR, Salem N Jr. Dietary polyunsaturated fatty acids and depression: when cholesterol does not satisfy. Am J Clin Nutr. 1995;62(1):1–9.
Mazoochian L, Sadeghi HM, Pourfarzam M. The effect of FADS2 gene rs174583 polymorphism on desaturase activities, fatty acid profile, insulin resistance, biochemical indices, and incidence of type 2 diabetes. J Res medical Sci. 2018;23:47.
Sone Y, Kido T, Ainuki T, Sonoda M, Ichi I, Kodama S, et al. Genetic variants of the fatty acid desaturase gene cluster are associated with plasma LDL cholesterol levels in Japanese males. J Nutri Sci Vitaminol. 2013;59(4):325–35.
Merino DM, Ma DW, Mutch DM. Genetic variation in lipid desaturases and its impact on the development of human disease. Lipids Health Dis. 2010;9:63. https://doi.org/10.1186/1476-511x-9-63.
Fuente-Martín E, Argente-Arizón P, Ros P, Argente J, Chowen JA. Sex differences in adipose tissue: It is not only a question of quantity and distribution. Adipocyte. 2013;2(3):128–34. https://doi.org/10.4161/adip.24075.
Leblanc V, Bégin C, Corneau L, Dodin S, Lemieux S. Gender differences in dietary intakes: what is the contribution of motivational variables? J Hum Nutr Diet. 2015;28(1):37–46. https://doi.org/10.1111/jhn.12213.
Zolfaghari R, Ross AC. Recent advances in molecular cloning of fatty acid desaturase genes and the regulation of their expression by dietary vitamin A and retinoic acid. Prostaglandins Leukot Essent Fatty Acids. 2003;68(2):171–9.
Mohammadi M, Khodarahmi M, Kahroba H, Farhangi MA, Vajdi M. The interaction between dietary Non-Enzymatic Antioxidant Capacity (NEAC) with variants of Melanocortin-4 receptor (MC4R) 18q21.23-rs17782313 locus on hypothalamic hormones and cardio-metabolic risk factors in obese individuals from Iran. Nutr Neurosci. 2020;23(10):824–37. https://doi.org/10.1080/1028415X.2020.1780738.
Bahadoran Z, Golzarand M, Mirmiran P, Shiva N, Azizi F. Dietary total antioxidant capacity and the occurrence of metabolic syndrome and its components after a 3-year follow-up in adults: Tehran Lipid and Glucose Study. Nutr Metab. 2012;9(1):70. https://doi.org/10.1186/1743-7075-9-70.
Meydani M, Hasan ST. Dietary polyphenols and obesity. Nutrients. 2010;2(7):737–51. https://doi.org/10.3390/nu2070737.
Yu JH, Kim MS. Molecular mechanisms of appetite regulation. Diabetes Metab J. 2012;36(6):391–8.
Rautiainen S, Serafini M, Morgenstern R, Prior RL, Wolk A. The validity and reproducibility of food-frequency questionnaire-based total antioxidant capacity estimates in Swedish women. Am J Clin Nutr. 2008;87(5):1247–53. https://doi.org/10.1093/ajcn/87.5.1247.
Pellegrini N, Salvatore S, Valtueña S, Bedogni G, Porrini M, Pala V, et al. Development and validation of a food frequency questionnaire for the assessment of dietary total antioxidant capacity. J Nutr. 2007;137(1):93–8. https://doi.org/10.1093/jn/137.1.93.
Acknowledgements
The authors thank the participants of the current study. The work has been supported by a grant from Research Undersecretary of Tabriz University of Medical Sciences; (Identifier: IR.TBZMED.REC.1400.889 and Grant number: 68623)
Funding
The current study has been financially supported by a grant from Tabriz University of Medical Sciences (Identifiers: IR.TBZMED.REC.1400.889 and Grant number: 68623).
Author information
Authors and Affiliations
Contributions
MK contributed to data collection and manuscript writing. MK performed the statistical analysis and data interpretation. MA conceptualized and designed the study, was involved in hypothesis generation. She also revised the final manuscript as submitted. HK and PJ were involved in lab works and genetic assays. AH was involved in hypothesis generation and primary data’s collection. All of the authors approved the final revised manuscript to be submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained from all participants. Besides, the study protocol was approved by the ethics committee of Tabriz University of Medical Sciences (Ethics numbers: IR.TBZMED.REC.1400.889). All methods were performed in accordance with declaration of Helsinki with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Khodarahmi, M., Javidzade, P., Farhangi, M.A. et al. Interplay between fatty acid desaturase2 (FADS2) rs174583 genetic variant and dietary antioxidant capacity: cardio-metabolic risk factors in obese individuals. BMC Endocr Disord 22, 167 (2022). https://doi.org/10.1186/s12902-022-01075-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-022-01075-7