
Abstract
Objective
Glycosylated hemoglobin (HbA1c) has obvious clinical value in the diagnosis of diabetes, but the conclusions on the diagnostic value of diabetic retinopathy (DR) are not consistent. This study aims to comprehensively evaluate the accuracy of glycosylated hemoglobin in the diagnosis of diabetic retinopathy through the meta-analysis of diagnostic tests.
Methods
Cochrane Library, Embase, PubMed, Web of Science, China National Knowledge Infrastructure (CNKI), China Wanfang Database, Chinese Biomedical Literature Database (CBM) were searched until November, 2020. The Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool was used to assess the quality of the included studies. The pooled sensitivity, specificity, positive likelihood ratio (+LR), negative likelihood ratio (-LR), diagnostic odds ratio (DOR) and areas under the receiver operating characteristic (ROC) curve were calculated by Stata 15.0 software.
Results
After screening, 18 high-quality papers were included. The results of meta-analysis showed that the combined DOR = 18.19 (95% CI: 10.99–30.11), the sensitivity= 0.81 (95% CI): 0.75 ~ 0.87), specificity = 0.81 (95%CI: 0.72 ~ 0.87), +LR = 4.2 (95%CI: 2.95 ~ 6.00), −LR = 0.23 (95%CI: 0.17 ~ 0.31), and the area under the Summary ROC curve was 0.88 (95%CI: 0.85 ~ 0.90).
Conclusion
The overall accuracy of HbA1cC forin diagnosing diabetic retinopathy is good. As it is more stable than blood sugar and is not affected by meals, it may be a suitable indicator for diabetic retinopathy.
Similar content being viewed by others

Introduction
Diabetes mellitus (DM) is a global pandemic. According to statistics, the number of diabetes in the world reached 366 million in 2011 and 422 million in 2014 (accounting for 8.5% of the population). The International Diabetes Federation predicts [1] that the number of diabetes will rise to 552 million by 2030, of which type 2 diabetes mellitus (T2DM) will accounts for 90%, while the situation in developing countries will be even more severe. According to the current clinical disease and case statistics, diabetic retinopathy is not only one of the serious complications of diabetes, but also the main cause of blindness in adults. A recent analysis report shows that about 93 million people (35%) of diabetic patients worldwide have diabetic retinopathy (DR), and 28 million (10%) of whose vision has already been affected [2]. Among patients with type 2 diabetes, an average of about 50% of them will develop diabetic retinopathy, 20 years after the onset of the disease, and about 10% will have proliferative diabetic retinopathy or exudative macular degeneration [3]. According to statistics, among the patients with diabetes in China, the prevalence rate of diabetic retinopathy is close to 40%. With the prolongation of the course of diabetes, the prevalence rate of diabetic retinopathy has increased to 54% [4]. A number of foreign studies have shown that among patients with type 2 diabetes, the possibility of diabetic retinopathy increases year by year with the continuous prolongation of the course of disease. About 30 to 60% of patients with diabetes will develop DR [5, 6]. The occurrence of diabetic retinopathy not only affects people’s life to a great extent, but also affects people’s quality of life, which increases the social and economic pressure of the country and patients’ families as well as patients themselves [7].It has also been found that retinopathy in patients with type 2 diabetes is not diagnosed until at least 7 years after patients get retinopathy. Due to the slow onset of diabetic retinopathy, if the disease does not invade the macula, it is not easy to be diagnosed until the patient comes to see a doctor with symptoms such as blurred vision and decreased vision. At this time, the disease has developed to the stage of irreversible and severe microangiopathy, when it has well past the best period of treatment, so it is very difficult to treat it, and the treatment effect is relatively poor, which eventually results in patients’ blindness. Therefore, it is imperative to detect and treat the risk factors that affect the disease in the early stage.
Studies have shown that a variety of risk factors are closely related to the occurrence and development of diabetic retinopathy, such as hyperglycemia, course of disease [8], hypertension, dyslipidemia and so on [9, 10]. United Kingdom Prospective Diabetes Study (UKPDS) and Diabetes Control and Complications Trial (DCCT) have been followed up for 10 years, showing that early and continuous hyperglycemia control is beneficial for improving diabetic retinopathy [11, 12]. In addition, studies have shown that for every 1% reduction in glycosylated hemoglobin, the risk of microvascular complications (mainly diabetic retinopathy) can be reduced by 37% [13]. For many years, the relationship between hyperglycemia and DR has been studied mainly through the determination of glycosylated hemoglobin and / or fasting plasma glucose [14] and other metabolic indexes. Glycosylated hemoglobin (HbA1c) is the product of the combination of hemoglobin and blood sugar. Its concentration in blood is stable and is not affected by short-term blood glucose concentration. It can effectively reflect the level of glucose metabolism in only 3 months. At present, it is internationally recognized as the gold standard for long-term blood glucose control [15]. Some studies have shown that the occurrence and development of DR is closely related to the level of HbA1c [16].
In order to objectively evaluate the diagnostic value of HbA1c in diabetic retinopathy, this study used the meta-analysis method to systematically analyze the published tests of HbA1c in the diagnosis of diabetic retinopathy home and abroad, so as to provide reference for clinical application in the future.
Methods
Retrieval strategy
Two researchers independently searched Cochrane Library, Embase, PubMed, Web of Science, China Knowledge Network China National Knowledge Infrastructure (CNKI), China Wanfang Database, Chinese Biomedical Literature Database (CBM) from inception to November 2020 to evaluate the value of HbA1C in the diagnosis of diabetic retinopathy. The search strategy was as follows: (“HbA1c” OR “HBALc” OR “glycosylated hemoglobin” OR “glycated hemoglobin”) AND (“DR” OR “diabetic retinopathy” ). There was no language limitation. When necessary, we looked for additional references from review articles, guides and conferences.
Literature selection criteria
Inclusion criteria
1) Studies using HbA1c to diagnose diabetic retinopathy; 2) Studies that include a clear sensitivity and specificity, or a four-grid table that can list diagnostic tests through reported data. 3) when it came to studies with the same or overlapping data for the same author, studies with a relevantly recent publication time or a larger number of subjects were selected.
Exclusion criteria
1) repeated studies or papers with incomplete document or wrong data; 2) studies that cannot extract effective data indicators; 3)Research on the diagnosis of diabetes by HbA1c; 4) case study with less than 20 samples; 5) the type of papers included basic research, review, conference abstract, etc.
Quality assessment
The Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) was adopted to evaluate the quality of all included studies [17]. Two researchers scored the studies separately according to the evaluation form, and if there were differences in the results, a decision was made through discussion to ensure the quality of the included studies.
Data extraction
All data were independently extracted by two researchers, cross-checked, and they made a decision through discussion when disagreement occurred. The following information was extracted: 1) author, year of publication, country, race and sample size, etc. 2) diagnostic parameters: the cut-off value ofHbA1c for diagnosing diabetic retinopathy and the four-grid table parameters of the diagnostic test: including true positive value (TP), false positive (FP), true negative (TN), false negative value (FN).
Statistical analysis
Meta-analysis was carried out by Stata15.0 software. The sensitivity, specificity, positive likelihood ratio (+LR), negative likelihood ratio (-LR) and diagnostic odds ratio (DOR) of HbA1c in the diagnosis of diabetic retinopathy were summarized by the bivariate mixed-effects regression model, and heterogeneity was analyzed. Meta-regression and subgroup analysis waswere used to explore the sources of heterogeneity. The summary receiver operatingor characteristic (SROC) curve, was used to calculate the area under the curve (AUC). A funnel plot was drawn to detect the publication bias. At the same time, a sensitivity analysis was used to verify the robustness of the findings.
Results
Literature research, characteristic and quality of studies
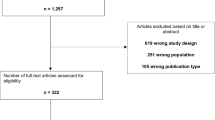
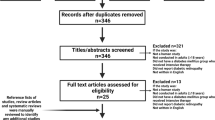
After preliminary search, a total of 1071 papers were obtained, 407 repeated papers were excluded, 579 papers were removed after reading abstracts, and 67 of them were excluded after further reading the full text. Therefore, this meta-analysis finally included 18 published papers studies [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35], containing 20 studies. The screening flow diagram was shown in Fig. 1. For an overview of the included literature, see Table 1. Among the included studies, 7 were from China, 3 from the United States, 2 from South Korea, 2 from Japan, 1 from France, 1 from India, 1 from Thailand and 1 from Iran. The quality of the included literature is shown in Fig. 2 (a, b) The overall quality was high, and only when the threshold was set in advance, there was a high risk of deviation.

A flow diagram of the study selection process

Results of literature quality evaluation according to QUADAS-2. (a: Risk of bias summary; b: Risk of bias graph)
The results of the meta-analysis
In the included papers, the sensitivity logarithm and the (1-specificity) logarithm were analyzed by Spearman correlation, with the correlation coefficient 0.208 (P = 0.380) and the SROC curve did not show a typical “shoulder-arm-like” distribution (Fig. 3), indicating that there was no threshold effect in this study. The heterogeneity across the studies was assessed. The DOR (P = 0.00, I2 = 100.00%), sensitivity (P = 0.00, I2 = 95.53%), specificity (P = 0.00, I2 = 99.62%), +LR (P = 0.00, I2 = 99.45%), -LR (P = 0.00, I2 = 98.13%) were all heterogeneous. The Bbivariate mixed-effects regression model was used for data merging. The results showed that the DOR was 18.19 (95% CI: 10.99 ~ 30.11) (Fig. 4a), sensitivity = 0.81 (95%CI: 0.75 ~ 0.87), specificity = 0.81 (95%CI: 0.72 ~ 0.87) (Fig. 4b), +LR = 4.2 (95%CI: 2.95 ~ 6.00), -LR = 0.23 (95%CI: 0.17 ~ 0.31) (Fig. 4c), and AUC was 0.88 (95%CI = 0.85 ~ 0.90). The Fagan’s Nomogram results showed that when the current test probability was 20%, the post-test probability of +LRwas 51%, and the post-test probability of Personality -LR was 5% (Fig. 4d). The Deeks’ funnel plotshowed p = 0.10, indicating no obvious publication bias (Fig. 5). The results of subgroup analysis of publication year, ethnic population, test sample size and cut-off value showed that (Fig. 6), the influence of publication year test sample size and cut-off value on sensitivity results was statistically significant. The effect of test sample size on specificity results was extremely significant (P < 0.01), indicating that these factors might be the main sources of heterogeneity. From the above results, HbA1cC is of good value in the diagnosis of diabetic retinopathy.

The SROC curve for the accuracy of HbA1c in the diagnosis of diabetic retinopathy. SROC: summary receiver operating characteristic

Forest plots of HbA1c in the diagnosis of diabetic retinopathy (a: Diagnostic odds ratio; b: Sensitivity and specificity; c: Positive likelihood ratio and negative likelihood ratio; d: Fagan’s Nomogram)

Deeks’ funnel plot of HbA1c for the diagnosis of diabetic retinopathy

Univariable meta-regression & subgroup analyses of HbA1c for the diagnosis of diabetic retinopathy
Sensitivity analysis
The sensitivity analysis results of HbA1c diagnostic accuracy for diabetic retinopathy were shown in Fig. 7 (a,b,c,d). The Goodness-of-fit and bivariate normal analysis showed that the bivariate mixed-effects model was robust for meta-analysis. Furthermore, the robustness of the meta-analysis was determined by influence analysis and outlier detection analysis. After excluding outliers, there was no significant change in overall sensitivity (0.81 vs. 0.82), specificity (0.81 vs. 0.82), +LR(4.2 vs. 4.6), -LR(0.23 vs. 0.21), DOR (18.19 vs. 21) and AUC (0.88 vs. 0.88), which showed that the conclusions of the meta-analysis were robust.

The results of sensitivity analysis (a: Goodness of fit. b: Bivariate normality. c: Influence analysis. d: Outlier detection)
Discussion
Along with the increase in the number of diabetic patients and the increasing prevalence in various regions of the world, diabetic retinopathy has become one of the main eye diseases that cause blindness in China [36]. The Wiscnsin Epidmiologic Study of Diabetic retinopathy (WESDR), a world-renowned USA study, has reported that the incidence of DR is 50.1%, and the incidence of retinopathy is related to the duration of diabetes. That is, the longer the course of diabetes, the higher the incidence of retinopathy [37]. It has been reported that there is a significant correlation between the incidence of diabetic retinopathy and the level of HbA1c. The UKPDS study has shown that for patients with type 2 diabetes, their HbA1c levels are reduced by 1%, and the risk of retinopathy can be reduced by about 21% [38]. In a 2004 observation on retinal thickness and blood-retinal barrier in patients with type 2 diabetes [39], after 3 years of follow-up, it was found that high HbA1c levels were an independent risk factor for blood-retinal barrier. Therefore, attaining the standard of HbA1c can improve or delay the development of diabetic retinopathy. Patients with persistently high glycosylated hemoglobin levels have poor blood glucose control and a significant increase in basal metabolic rate, resulting in a significant increase in tissue oxygen demand, which makes their tissues often in the state of hypoxia. At the same time, there is a kind of glycosylated hemoglobin with high affinity to oxygen in erythrocytes, which can prevent hemoglobin from binding to 2-3DPG, which makes the oxygen not easy to dissociate, resulting in tissue hypoxia and the proliferation of vascular growth factor, which is the basis of the occurrence and progression of diabetic retinopathy [40]. It is also believed that the aggregation rate of red blood cells has a significant impact on the level of glycosylated hemoglobin. When the level of glycosylated hemoglobin in patients with diabetes is higher, a large number of red blood cells in the body will gather with each other at a faster speed, making fundus micro-vessels easy to form thrombus, which is the pathophysiological basis of early diabetic retinopathy. Su SC [41] and other studies have found that type 2 diabetic patients with higher HbA1c levels have a significantly higher prevalence rate of retinopathy than diabetic patients with normal HbA1c. And when HbA1c ≥ 7.0%, the incidence of retinopathy is about 85%. Studies have shown that there is no significant difference in the prevalence rate of diabetic retinopathy in diabetic patients with HbA1c of 6.0–8.0%, but the incidence of diabetic retinopathy in patients with HbA1c ≥ 8.0% is significantly higher than that in patients with HbA1c < 8.0% [42].
In order to obtain more accurate data about the diagnostic value of HbA1c for diabetic retinopathy, this meta-analysis was carried out. This study included 18 papers and a total of 2345 patients with diabetic retinopathy. The results showed that HbA1c is an effective indicator for the diagnosis of diabetic retinopathy. The overall sensitivity and specificity were 0.8, suggesting that the missed diagnosis rate and misdiagnosis rate of HbA1c in the diagnosis of diabetic retinopathy were both 19%. The area under the SROC curve is an index to measure the accuracy of the diagnostic test. The closer the area under the curve is to 1, the better the diagnostic effect is. In this study, the AUC was 0.88, indicating that HbA1c is more effective in the diagnosis of diabetic retinopathy. Sensitivity analysis showed that the results of this study did not change significantly with the elimination of a single study, indicating that the results of this study are relatively robust and reliable. Bias is the most important challenge in the process of Meta-analysis. The publication bias evaluation results of this study showed that P > 0.05, indicating that the results of this meta-analysis were integrated, comprehensive, objective and true revealing of the 20 studies included, and have high credibility and practical significance. The results are consistent with the results of a meta-analysis study conducted by Martínez-Vizcaíno et al. [43] in 2015, The research results of whom have shown that HbA1c and 2 h-PG have similar diagnostic accuracy, which is better than fasting blood-glucose (FBG) and 2-h post-meal blood glucose (2 h-PG) is always the first choice for clinical diagnosis of diabetes, but because of its time-consuming and laborious, HbA1c is considered to be a better substitute. Our study increased the number of studies included and the number of cases on his basis, and further verified and supported this conclusion.
This study also has certain limitations: 1) The number of included papers was small, only Chinese and English papers were available, while high-quality papers in other languages were likely to be missed. 2) there was great heterogeneity among the results of this study, and only some indicators were analyzed by subgroup analysis, which was not enough to well explore the source of heterogeneity. 3) Different studies had different diagnostic thresholds, which might result in bias in the results.
In conclusion, HbA1c has a good diagnostic valueeffectiveness for diabetic retinopathy and may be used for preliminary screening of clinical diabetic retinopathy. In future studies, the diagnostic effectiveness of HbA1c may be increased by adjusting the appropriate diagnostic threshold, or combing it with some other biochemical indicators such as FPG, 2 h-PG and other biochemical indicators to improve its diagnostic effectiveness. More clinical data are still needed to further verify the above conclusions.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- HbA1c:
-
Glycosylated hemoglobin
- DR:
-
Diabetic retinopathy
- AUC:
-
Area under the curve
- DM:
-
Diabetes Mellitus
- T2DM:
-
type 2 diabetes mellitus
- QUADAS-2:
-
Quality assessment of diagnostic accuracy studies-2
- SROC:
-
Summary receiver operatingoperator characteristic
- FBG:
-
Fasting blood-glucose
- 2 h-PG:
-
2-h post-meal blood glucose
References
Whiting DR, Guariguata L, Weil C. IDF diabetes atlas:global estimates of the pr evalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011;94(3):311–21. https://doi.org/10.1016/j.diabres.2011.10.029.
Yau JW, Rogers SL, Kawasaki R. Global prevalence and major risk factors of di abetic retinopathy. Diabetes Care. 2012;35(3):556–64. https://doi.org/10.2337/dc11-1909.
Stefánsson E, Bek T, Porta M, Larsen N, Kristinsson JK, Agardh E. Screening and prevention of diabetic blindness. Acta Ophthalmol Scand. 2000;78(4):374–85. https://doi.org/10.1034/j.1600-0420.2000.078004374.x.
Xie XW, Xu L, Jonas JB, Wang YX. Prevalence of diabetic retinopathy among subjects with known diabetes in China: the Beijing eye study. Eur J Ophthalmol. 2008;19(1):91–9.
Khandekar R. Diabetic retinopathy in Oman: a hospital-based study. Brit J Ophthalmol. 2003;87(9):1061–4. https://doi.org/10.1136/bjo.87.9.1061.
Knudsen LL, Lervang HH, Lundbye Christensen S, Gorst RA. The North Jutland County diabetic retinopathy study: population characteristics. Acta Ophthalmol. 2006;90(4):1404.
Merchant ML, Klein JB. Proteomic discovery of diabetic nephropathy biomarkers. Adv Chronic Kidney Dis. 2010;17(6):480–6. https://doi.org/10.1053/j.ackd.2010.09.001.
Zhang X, Saaddine JB, Chou CF, Cotch MF, Cheng YJ, Geiss LS, et al. Prevalence of diabetic retinopathy in the United States, 2005-2008. JAMA. 2010;304(6):649–56. https://doi.org/10.1001/jama.2010.1111.
Chew EY. Association of Elevated Serum Lipid Levels With Retinal Hard Exudate in Diabetic Retinopathy. Arch Ophthalmol. 1996;114(9):1079.
Klein R, Klein BEK, Moss SE, Davis MD, Demets DL. Is blood pressure a predictor of the incidence or progression of diabetic retinopathy? Arch Intern Med. 1989;149(11):2427–32. https://doi.org/10.1001/archinte.1989.00390110033008.
Rury R Holman, Sanjoy K Paul, Angelyn M Bethel, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. New Engl J Med. 2008;359:1577–8.
Matthews DR, Stratton IM, Aldington SJ, Holman RR, Kohner EM. Risks of progression of retinopathy and vision loss related to tight blood pressure control in type 2 diabetes mellitus: UKPDS 69. Arch Ophthalmol. 2004;122(11):1631–40. https://doi.org/10.1001/archopht.122.11.1631.
White NH, Sun W, Cleary PA, Danis RP, Davis MD, Hainsworth DP, et al. Prolonged effect of intensive therapy on the risk of retinopathy complications in patients with type 1 diabetes mellitus: 10 years after the diabetes control and complications trial. Arch Ophthalmol. 2008;126(12):1707–15. https://doi.org/10.1001/archopht.126.12.1707.
Miki E, Kikuchi M. Diabetic retinopathy and control of diabetes with special reference to blood glucose levels. Diab Res Clin Pract. 1994;24(Suppl):S177.
Zhou Y, LZ, Wen JH. The value of serum homocysteine and glycosylated hemoglobin in the diagnosis of diabetic retinopathy. Pract Clin Med. 2017;18(8):35–6.
Zhang LQ. Significance of detection of glycosylated hemoglobin and C-reactive protein in type 2 diabetic retinopathy. Contemp Med. 2014;20(24):107–8.
Whiting PF. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann Intern Med. 2011;155(8):529.
Mccance DR, Hanson RL, Charles MA, Jacobsson LTH, Knowler WC. Comparison of tests for glycated haemoglobin and fasting and two hour plasma glucose concentrations as diagnostic methods for diabetes. BMJ. 1994;309(6940):841.
Miyazaki M, Kubo M. Comparison of diagnostic methods for diabetes mellitus based on prevalence of retinopathy in a Japanese population: the Hisayama study. Diabetologia. 2004;47(8):1411–5. https://doi.org/10.1007/s00125-004-1466-8.
Cheng YJ, Gregg EW, Geiss LS, Imperatore G, Saaddine JB. Association of A1C and Fasting Plasma Glucose Levels With Diabetic Retinopathy Prevalence in the U.S. Population. Diab Care. 2009;32(11):2027.
Massin P, Lange C, Tichet J, Vol S, Erginay A, Cailleau, M, et al. Hemoglobin A1c and fasting plasma glucose levels as predictors of retinopathy at 10 years: the French DESIR study. Arch Ophthalmol. 2011;129(2):188-95.
Xin Z, Yuan MX, Li HX, Hua L, Feng JP, Shi J, et al. Evaluation for fasting and 2-hour glucose and HbA1c for diagnosing diabetes based on prevalence of retinopathy in a Chinese population. Plos One. 2012;7(7):e40610. https://doi.org/10.1371/journal.pone.0040610.
Cho NH, Kim TH, Woo SJ, Park KH, Lim S. Optimal HbA1c cutoff for detecting diabetic retinopathy. Acta Diabetol. 2013;50(6):837–42. https://doi.org/10.1007/s00592-013-0452-3.
Park YM, Ko SH, Lee JM, Kim DJ, Kim DJ, Han K, et al. Glycaemic and haemoglobin A1c thresholds for detecting diabetic retinopathy: the fifth Korea National Health and nutrition examination survey (2011). Diab Res Clin Pract. 2014;104(3):435–42. https://doi.org/10.1016/j.diabres.2014.04.003.
Mukai N, Yasuda M, Ninomiya T, Hata J, Hirakawa Y. Thresholds of various glycemic measures for diagnosing diabetes based on prevalence of retinopathy in community-dwelling Japanese subjects: the Hisayama study. Cardiovasc Diabetol. 2014;13(1):45. https://doi.org/10.1186/1475-2840-13-45.
Sabanayagam C, Eric YH, Khoo, Weng K, Lye, Kamran M, et al. Diagnosis of diabetes mellitus using HbA1c in Asians: relationship between HbA1c and retinopathy in a multiethnic Asian population. J Clin Endocr Metab. 2015;100:689-96.
Tangjai P, Chingchana P, Taweerutchana R. Glycated Haemoglobin and Diabetic Retinopathy in Type 2 Diabetic Patients in HRH Princess Maha Chakri Sirindhorn Medical Center. J Med Assoc Thailand. 2015;98(Suppl 10):S135.
Wang B, Liu MC, Li XY, Liu XH, Gao ZN. Cutoff point of HbA1c for diagnosis of diabetes mellitus in Chinese individuals. Plos One. 2016;11(11):e166597.
Xu J, Yuan S, Fu H. Influence of glycosylated hemoglobin on diabetic retinopathy--Beijing Community Diabetes Study 18. Ophthalmol CHN. 2016;25(5):321–5.
Okosun IS, Turbow S, Mcjenkin K, Monique Davis-Smith Y, Seale JP. Diagnostic performance of glycated hemoglobin for diabetic retinopathy in non-diabetic older overweight/obese African-Americans. Diab Res Clin Pract. 2016;120:124–31. https://doi.org/10.1016/j.diabres.2016.07.021.
Zhang R, Li YF, Zhang SM. The Association of Retinopathy and Plasma Glucose and HbA1c: a validation of diabetes diagnostic criteria in a Chinese population. J Diabetes Res. 2016;2016:1–7. https://doi.org/10.1155/2016/4034129.
Aidenloo NS, Mehdizadeh A, Valizadeh N, Abbaszadeh M, Qarequran S, Khalkhali H. Optimal glycemic and hemoglobin A1c thresholds for diagnosing diabetes based on prevalence of retinopathy in an Iranian population. Iran Red Crescent Med J. 2016;18(8):e31254.
Ji X, Shao J, Lu S. Diagnostic value of Glycocsylated hemoglobin A1c and Glycated albumin levels in diabetic Retinopany. Mod Lab Med. 2018;33(05):83–7.
Zheng L, Chen S, Wang A. Levels and significances of serum MDA, SOD and HbAl c in patients with type 2 diabetic combined retinopathy. J Med Res. 2019;48(6):76–9.
Kang ML, Yuan SQ, Zhao C. Value of glycosylated hemoglobin in the diagnosis of diabetic retinopathy. Clin Med. 2020;40(1):29-31.
Luo C. Diabetic retinopathy: an urgent task to be explored in the new century. Chinese J Ocular Fundus Dis. 2000;16(3):139–40.
Aiello L. Diabetic retinopathy (technical review). Diabetes Care. 1998;21(1):143–56. https://doi.org/10.2337/diacare.21.1.143.
Stratton IM, Cull CA, Adler AI, Matthews DR, Neil HAW, Holman RR. Additive effects of glycaemia and blood pressure exposure on risk of complications in type 2 diabetes: a prospective observational study (UKPDS 75). Diabetologia. 2006;49(8):1761–9. https://doi.org/10.1007/s00125-006-0297-1.
Lobo CL, Bernardes RC, Figueira JP, de Abreu JR, Cunha-Vaz JG. Three-year follow-up study of blood-retinal barrier and retinal thickness alterations in patients with type 2 diabetes mellitus and mild nonproliferative diabetic retinopathy. Arch Ophthalmol. 2004;122(2):211–7.
Tian Q. Relationship between glycosylated hemoglobin and diabetic retinopathy. J Mil Surg Southwest China. 2008;10(004):93–4.
Su SC, Pei D, Hsieh CH, Hsiao FC, Wu CZ, Hung YJ. Circulating pro-inflammatory cytokines and adiponectin in young men with type 2 diabetes. Acta Diabetol. 2011;48(2):113–9. https://doi.org/10.1007/s00592-009-0171-y.
Aiello LP, Davis MD, Girach A, Kles KA, Xin EZ. Effect of ruboxistaurin on visual loss in patients with diabetic retinopathy. Ophthalmology. 2006;113(12):2221–30. https://doi.org/10.1016/j.ophtha.2006.07.032.
Vicente M, Iván C, Celia Á, Fernando R, Christopher BN. The accuracy of diagnostic methods for diabetic retinopathy: a systematic review and Meta-analysis. PLoS One. 2016;11(4):e154411.
Acknowledgements
None.
Funding
Our study is supported by Beijing Huashang Kunlun Health Management Co., Ltd. the financial support for Research of the protective effect and mechanism of regulating microglial mGluRs on neuron; Supported by the Department of Science and Technology of Jilin Province (No. 20200404161YY;YDZJ202101ZYTS098).
Author information
Authors and Affiliations
Contributions
ZB,ZBJ,WD: Critical revision of the manuscript;ZB,ZBJ,WD: Substantial contribution to the conception and design of the work, manuscript drafting;ZB,ZZL,GYT: Acquisition, analysis, and interpretation of the data;ZB,ZBJ,ZZL,GYT,WD: Revising the manuscript critically, final approval of the version to be published. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was not needed because this is a meta-analysis.
Consent for publication
Not applicable.
Competing interests
All the authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, B., Zhang, B., Zhou, Z. et al. The value of glycosylated hemoglobin in the diagnosis of diabetic retinopathy: a systematic review and Meta-analysis. BMC Endocr Disord 21, 82 (2021). https://doi.org/10.1186/s12902-021-00737-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-021-00737-2