
Abstract
Background
Associations between metabolic syndrome (MetS) and osteoporotic fracture have been reported. However, the epidemiological studies are not conclusive. The objective of the study was to determine whether metabolic syndrome associates with osteoporotic fracture.
Methods
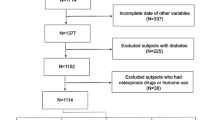
This was a cross-sectional study of 9930 Chinese adults aged 40 year or older in the Chongming District, Shanghai, China. A questionnaire, anthropometric measurements and laboratory tests were conducted. MetS was defined according to the updated National Cholesterol Education Program Adult Treatment Panel III criteria for Asian-Americans. A history of fractures was collected with an interviewer-assisted questionnaire. Osteoporotic fractures were defined as fractures that occurred due to low-trauma in 2 years prior to the study.
Results
Among women, the prevalence of osteoporotic fractures was significantly higher in those with MetS (3.5 vs. 2.6 %, P =0.028). However, the difference was not found in men (2.6 vs. 2.4 %, P =0.737). The presence of Mets was significantly associated with increased odds of osteoporotic fracture among women (odds ratio 1.22; 95 % confidence interval 1.12–1.54; P = 0.039) after controlling for potential confounders. The significant associations were not detected in men.
Conclusions
The presence of MetS was significantly associated with a recent history of osteoporotic fracture in middle-aged and elderly Chinese women.
Similar content being viewed by others


What’s new?
-
✓In this study we found the presence of MetS was significantly associated with a recent history of osteoporotic fracture in a large sample of middle-aged and elderly Chinese women.
-
✓We found central obesity seem to have the strongest associations with prevalence of osteoporotic facture in women.
-
✓Our study indicated bone metabolism seems to be more markedly affected in women than in men with metabolic syndrome.
Background
With the rapid economic growth and the ageing of its population in China, osteoporosis has become one of the most prevalent and debilitating chronic diseases. It has often been called “the silent epidemic” because bone loss is a slow asymptomatic process. Only when fractures occur does the disease become symptomatic. Recently, osteoporotic fracture has become an increasingly important problem in elderly populations and place a progressively heavy burden on health services [1, 2]. Nutritional, lifestyle, hormonal, metabolic, and genetic factors contribute to the occurrence of osteoporotic fracture [2].
Metabolic syndrome (MetS) is a cluster of cardiovascular risk factors has been defined as central obesity, hypertension, impaired glucose tolerance, and dyslipidemia (specifically hypertriglyceridemia, along with low levels of high-density lipoprotein cholesterol [HDL-c]). It is a public health problem because about 30–50 % of the middle-aged and elderly people has MetS in China [3, 4]. MetS is associated with a higher risk of cardiovascular morbidity and mortality and a higher risk of onset of type 2 diabetes. Although the relationship between cardiovascular disease and osteoporosis has been widely studied, the particular association between metabolic syndrome, a strong risk factor for cardiovascular disease, and osteoporotic fractures has not been so extensively addressed and present several studies results were inconsistent [5–15]. Epidemiological studies on fracture incidence or prevalence are therefore needed in order to show the real pattern of fractures in MetS. In addition, because metabolic syndrome consists of several single components that could have their own independent relationship with osteoporosis, the possible association of each of them with the osteoporotic fracture is also worth considering.
Thus, the present study intended to evaluate the association between MetS and osteoporotic fracture in a population-based survey of middle-aged and elderly Chinese people in Shanghai, China. We also examined the association of each of the individual components of metabolic syndrome with osteoporotic fracture.
Methods
Study population and design
In 2011 China a national survey of Risk Evaluation of cAncers in Chinese diabeTic Individuals: a lONgitudinal (REACTION) study, which was conducted among 259,657 adults, aged 40 years and older in 25 communities across mainland China, from 2011 to 2012 [16]. The data presented in this article are based on the baseline survey of subsamples from Shanghai in eastern China. All studied individuals came from the Chongming District in Shanghai, China [17–19]. Written consent was obtained from all the participants. The protocol was approved by the Ethics Committee of Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine.
Data collection
A standardized questionnaire was used by trained physicians to collect information such as age, sex, medications [17–19]. The methods of biochemical measurements refer as previous studies [17–19]. Physical activity at leisure time was estimated using the short form of the International Physical Activity Questionnaire by adding questions on frequency and duration of moderate and vigorous activities and walking [20]. For evaluation of total physical activity, separate metabolic equivalent hours per week (MET-h/wk) were calculated.
Anthropometric measurements were performed by the trained personnel using a standardized protocol [17–19]. BMI was calculated as body weight in kilograms divided by height squared in meters. The abbreviated Modification of Diet in Renal Disease formula recalibrated for Chinese [21].
Definition of MetS
The MetS was defined based upon the updated NCEP-ATPIII for Asian Americans as presenting 3 or more of the following components: 1) waist cirumference ≥90 cm for men or ≥80 cm for women; 2) triglycerides ≥1.7 mmol/l; 3) HDL cholesterol <1.03 mmol/l for men or <1.30 mmol/l for women; 4) blood pressure ≥130/85 mm Hg or current use of anti-hypertensive medications; and 5) fasting glucose ≥5.6 mmol/l or previously diagnosed type 2 diabetes or on oral antidiabetic agents or insulin [22].
Assessment of fractures
With an interviewer-assisted questionnaire, we collected information about the history of fractures. Fracture sites and the age of the participants when they had fractures were recorded. For the current study, osteoporotic fractures were defined as fractures that occurred due to low trauma in the 2 yr before the study [23]. All fractures that were considered to be nonosteoporotic (i.e. fractures due to cancer or an accident, such as a motor vehicle accident, and all fractures of the fingers, faces, skull, and toes) were excluded [24].
Statistical analysis
The statistical analysis was conducted using SPSS (version 13.0, SPSS Inc., Chicago, Illinois). Because sex is an important confounding factor of osteoporotic fractures, we performed analyses separately in men and women [25]. The following skewed variables were normalized by logarithmic transformation before analyses in which they were treated as continuous variables: TG, eGFR and MET-h/wk. All continuous variables were presented as means ± SD or medians (inter-quartile ranges), and all categorical variables were presented as proportions. The t test and Chi-square test were used to examine differences in continuous and categorical variables, respectively. To investigate the associations between metabolic syndrome and osteoporotic fracture, the unadjusted and multivariate adjusted logistic regression analyses were used to assess odds ratios (OR) and corresponding 95 % confidence intervals (CI). The statistical tests were two sided, and a P < 0.05 was considered statistically significant.
Results
Among the 9930 participants, the mean (±SD) age was 56.2 ± 7.8 yr, 32.5 % were men. The overall prevalence of osteoporotic fracture was 2.9 % (2.5 % in men and 3.1 % in women). The skeletal sites of the most common fractures were wrist in men (22.2 % of all fractures, n = 18) and ankle in women (20.2 % of all fractures, n = 42).
The clinical and biochemical characteristics stratified by metabolic syndrome status are shown for men and women in (Additional file 1: Table S1A and S1B). In men, participants with metabolic syndrome were older, more likely to be obese, and had significantly higher levels of TG, LDL-c, fasting plasma glucose (FPG), postprandial 2-h plasma glucose (PPG), HbA1c, waist circumference (WC), Hip circumference (HC), waist to hip ratio (WHR) and alcohol consumption habits and lower levels of HDL-c and eGFR (all p < 0.01). There was no significant difference between the two groups for TC, physical activity (MET-h/wk), and smoking. Similarly, in women, higher levels of age, BMI, WC, HC, WHR, TG, LDL-c, FPG, PPG, and alcohol consumption habits and lower levels of HDL-c were found in those with metabolic syndrome (all p < 0.05). Women with metabolic syndrome were less likely to be postmenopausal. However, the levels of serum TC in women with metabolic syndrome were higher in comparison with those without metabolic syndrome (p < 0.0001).
We further investigate the prevalence of osteoporotic fractures according to metabolic syndrome status for men and women. Among women, the prevalence of osteoporotic fractures was significantly higher in those with metabolic syndrome (3.5 vs. 2.6 %, P =0.028). However, the difference was not found in men (2.6 vs. 2.4 %, P =0.737).
As shown in Table 1, the presence of metabolic syndrome was significantly associated with increased odds of osteoporotic fracture among women (OR 1.38; 95 % CI 1.04–1.85; P =0.028). Further adjustment for age, smoking and alcohol consumption habits (yes/no), physical activity (MET-h/wk), eGFR, BMI, waist circumference and hip circumference, TG, TC, HDL-c, LDL-c, diabetes status (yes/no), FPG, HbA1c, menopause status (yes/no) and hormone replacement (yes/no) treatment did not materially change the association (OR 1.22; 95 % CI 1.12–1.54; P = 0.039). However, the significant associations were not detected in men.
Tables 2 and 3 shows that Ors for the fracture risk calculation according to increasing numbers of the metabolic syndrome by ATPIII and IDF criteria. The fracture risk significantly increased according to increasing numbers of the metabolic syndrome by ATPIII and IDF criteria in women, but not in men.
Table 4 shows the ORs for individual components of metabolic syndrome by NCEP-ATPIII for Asian associated with osteoporotic fractures. Of the five MetS components, hypertension and central obesity seem to have the positive associations with risk of osteoporotic fractures in women.
Discussion
In this study, we found that the presence of MetS was significantly associated with a recent history of osteoporotic facture in women aged 40 yr or older. Moreover, this association was independent of other potential traditional risk factors.
Metabolic syndrome (MetS) is a cluster of cardiovascular risk factors which have been grouped under this name because they coexist much more often than would be expected by chance. Whether it is a real clinical entity or not is the subject of much controversy, but in any case, apart from its cardiovascular consequences, a possible relationship with bone mass has been entertained [26–28]. Furthermore, some common mechanisms for both disorders have been proposed. For instance, low vitamin D levels are considered predisposing factors for osteoporosis, and have also been suggested to facilitate the development of MetS [29–32]. In addition, few studies have presented increased prevalence of osteoporosis fractures in subjects with MetS [11, 12]. In our study, after adjusted for potential cofounders, a positive association between MerS and a recent history of osteoporotic fracture was detected.
Our study indicated bone metabolism seems to be more markedly affected in women than in men with metabolic syndrome. The differences between men and women in bone structure and strength, body fat deposition, sex hormone levels, and risk of falls could be potential explanations for the inconsistency of associations between osteoporotic fracture and MetS by genders [32]. Potential sex-specific associations of MetS with osteoporotic fracture need to be elucidated further. Our findings lend support to the postulation that the presence of metabolic syndrome in middle-aged and elderly Chinese women may confer a higher osteoporotic fracture risk. These findings suggest an awareness of the need to screen women with MetS for the presence of osteoporosis in fracture prevention. Moreover, the potential contribution of metabolic syndrome to development of osteoporosis warrants further study. Furthermore, in order to investigate whether other definition of the MetS also confirm the finding, we have re-analyzed the results by definition of the MetS (IDF 2005), similarly, we also found that the presence of metabolic syndrome was significantly associated with increased odds of osteoporotic fracture among women. Simultaneously, we found he prevalence of fracture significantly increased for those with one to five components after adjustment for age, gender (P trends < 0.05).
To study the possible independent relationship between the five components of metabolic syndrome and osteoporotic facture, a logistic regression analysis was performed. Hypertension and central obesity seem to be the positive associations with risk of osteoporotic fractures in women. Consistent with our results, previous studies have found higher blood pressure in elderly women was associated with increased bone loss at the femoral neck [33]. Moreover, low fracture risk was observed among those using treatment for hypertension although it was not significant [34]. Recently, a large-scale case–control study have also demonstrated that hypertension seem to be the major cardiovascular risk factors for fractures [35]. Certainly, as most fractures occur in those elderly people and blood pressure increases with age, an increased risk of fractures for increasing blood pressure should be expected. Therefore, most available data point toward a positive association between both parameters, even if the pathogenetic mechanisms involved remain unclear.
We found central obesity seem to have the strongest associations with prevalence of osteoporotic facture in women. Although the pathophysiological mechanisms linking central obesity to osteoporotic fracture have not been well established, it is plausible to consider excessive accumulation of visceral fat could result in a higher secretion of proinflammatory cytokines, with a detrimental effect on bone; in fact, a negative relation between fat mass and bone mass for a given body weight has been reported [36–38].
From few bone histology studies in humans and experimental studies there is evidence that a decreased bone formation is one major mechanism leading to reduced bone mass in diabetics. Few studies address the role of diabetes and osteroporosis [39, 40]. However, we fail to replicate this results in our study. There is a need for further longitudinal studies, including the incidence and risk factors for osteoporotic fractures.
Several limitations of our study have to be addressed. First, due to the cross-sectional nature of the current study, admittedly, we could not determine whether MetS plays a causal role in the pathogenesis of osteoporotic fracture. Further prospective population-based studies are needed to clarify their precise interrelationship. Second, because the information of osteoporotic fracture is based on self-reports and no measurements of bone mineral density by dual-energy x-ray absorptiometry or other radiological methods were made, we could not identify asymptomatic osteoporotic fractures. Finally, although a wide spectrum of covariates were included in the adjustment, some residual or undetected confounding factors could not be ruled out, such as dietary calcium intake or serum 25-hydroxyvitamin D3 levels, which are other factors affecting osteoporosis [41].
Conclusions
We have found that the presence of MetS was significantly associated with a recent history of osteoporotic fracture in middle-aged and elderly Chinese women. Further longitudinal studies are expected to determine the role of MetS in the development of osteoporotic fracture.
Abbreviations
MetS, metabolic syndrome; HOMA-IR, Homeostasis model assessment of insulin resistance; BMI, body mass index; TG, triglycerides; TC, total cholesterol; LDL-c, low-density lipoprotein cholesterol; HDL-c, high-density lipoprotein cholesterol; eGFR, estimated glomerular filtration rate; ORs, odds ratios.
References
Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009;301:513–21.
Hippisley-Cox J, Coupland C. Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFracture Scores. BMJ. 2009;339:b4229.
He Y, Jiang B, Wang J, Feng K, Chang Q, Fan L, et al. Prevalence of the metabolic syndrome and its relation to cardiovascular disease in an elderly Chinese population. J Am Coll Cardiol. 2006;47:1588–94.
Gu D, Reynolds K, Wu X, Chen J, Duan X, Reynolds RF, et al. Prevalence of the metabolic syndrome and overweight among adults in China. Lancet. 2005;365:1398–405.
Kim KC, Shin DH, Lee SY, Im JA, Lee DC. Relation between obesity and bone mineral density and vertebral fractures in Korean postmenopausal women. Yonsei Med J. 2010;51:857–63.
Hernández JL, Olmos JM, de Juan J, Martínez J, Ramos C, Valero C, et al. Heel quantitative ultrasound parameters in subjects with the metabolic syndrome: the Camargo Cohort Study. Maturitas. 2011;69:162–7.
Hernández JL, Olmos JM, Pariente E, Martínez J, Valero C, García-Velasco P, et al. Metabolic syndrome and bone metabolism: the Camargo Cohort study. Menopause. 2010;17:955–61.
Yamaguchi T, Kanazawa I, Yamamoto M, Kurioka S, Yamauchi M, Yano S, et al. Associations between components of the metabolic syndrome versus bone mineral density and vertebral fractures in patients with type 2 diabetes. Bone. 2009;45:174–9.
Kinjo M, Setoguchi S, Solomon DH. Bone mineral density in adults with the metabolic syndrome: analysis in a population-based U.S. sample. J Clin Endocrinol Metab. 2007;92:4161–4.
von Muhlen D, Safii S, Jassal SK, Svartberg J, Barrett-Connor E. Associations between the metabolic syndrome and bone health in older men and women: the Rancho Bernardo Study. Osteoporos Int. 2007;18:1337–44.
Ahmed LA, Schirmer H, Berntsen GK, Fønnebø V, Joakimsen RM. Features of the metabolic syndrome and the risk of non-vertebral fractures: the Tromsø study. Osteoporos Int. 2006;17:426–32.
Szulc P, Varennes A, Delmas PD, Goudable J, Chapurlat R. Men with metabolic syndrome have lower bone mineral density but lower fracture risk--the MINOS study. J Bone Miner Res. 2010;25:1446–54.
El Maghraoui A, Rezqi A, El Mrahi S, Sadni S, Ghozlani I, Mounach A. Osteoporosis, vertebral fractures and metabolic syndrome in postmenopausal women. BMC Endocr Disord. 2014;14:93.
Sun K, Liu J, Lu N, Sun H, Ning G. Association between metabolic syndrome and bone fractures: a meta-analysis of observational studies. BMC Endocr Disord. 2014;14:13.
Sun M, Cao M, Fu Q, Zhu Z, Meng C, Mao J, et al. Association of calcaneal quantitative ultrasound parameters with metabolic syndrome in middle-aged and elderly Chinese: a large population-based cross-sectional study. BMC Endocr Disord. 2014;14:14.
Reaction NG, Group S. Risk Evaluation of cAncers in Chinese diabeTic Individuals: a lONgitudinal (REACTION) study. J Diabetes. 2012;4:172–3.
Niu Y, Yang Z, Li X, Zhang W, Lu S, Zhang H, et al. Association of osteoprotegerin with impaired glucose regulation and microalbuminuria: the REACTION study. BMC Endocr Disord. 2015;15:75.
Qin L, Yang Z, Gu H, Lu S, Shi Q, Xing Y, et al. Association between serum uric acid levels and cardiovascular disease in middle-aged and elderly Chinese individuals. BMC Cardiovasc Disord. 2014;14:26.
Qin L, Yang Z, Zhang W, Gu H, Lu S, Shi Q, et al. Association between metabolic syndrome and lung function in middle-aged and elderly Chinese individuals. Diabetes Res Clin Pract. 2015;108:e46–8.
Yang Z, Zhang Z, Wen J, Wang X, Lu B, Yang Z, et al. Elevated serum chemokine CXC ligand 5 levels are associated with hypercholesterolemia but not a worsening of insulin resistance in Chinese people. J Clin Endocrinol Metab. 2010;95:3926–32.
Ma YC, Zuo L, Chen JH, Luo Q, Yu XQ, Li Y, et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006;17:2937–44.
Liu J, Grundy SM, Wang W, Smith Jr SC, Vega GL, Wu Z, et al. Ethnic-Specific Criteria for the Metabolic Syndrome. Diabetes Care. 2006;29:1414–6.
Hsu YH, Venners SA, Terwedow HA, Feng Y, Niu T, Li Z, et al. Relation of body composition, fat mass, and serum lipids to osteoporotic fractures and bone mineral density in Chinese men and women. Am J Clin Nutr. 2006;83:146–54.
van Meurs JB, Dhonukshe-Rutten RA, Pluijm SM, van der Klift M, de Jonge R, Lindemans J, et al. Homocysteine levels and the risk of osteoporotic fracture. N Engl J Med. 2004;350:2033–41.
Stevens JA, Sogolow ED. Gender differences for non-fatal unintentional fall related injuries among older adults. Inj Prev. 2005;11:115–9.
Iacobellis G, Iorio M, Napoli N, Cotesta D, Zinnamosca L, Marinelli C, et al. Relation of adiponectin, visfatin and bone mineral density in patients with metabolic syndrome. J Endocrinol Invest. 2011;34:e12–15.
Manolagas SC, Almeida M. Gone with the Wnts: beta-catenin T-cell factor, forkhead box O, and oxidative stress in age-dependent diseases of bone, lipid, and glucose metabolism. Mol Endocrinol. 2007;21:2605–14.
McFarlane SI. Bone metabolism and the cardiometabolic syndrome: pathophysiologic insights. J Cardiometab Syndr. 2006;1:53–7.
Wimalawansa SJ. Vitamin D, in the new millennium. Curr Osteoporos Rep. 2012;10:4–15.
Navarro Mdel C, Saavedra P, Jódar E, Gómez de Tejada MJ, Mirallave A, Sosa M. Osteoporosis and metabolic syndrome according to socio-economic status; contribution of PTH, Vitamin D and body weight: The Canarian Osteoporosis Poverty Study (COPS). Clin Endocrinol (Oxf). 2012;78:681–6.
Parker J, Hashmi O, Dutton D, Mavrodaris A, Stranges S, Kandala NB, et al. Levels of vitamin D and cardiometabolic disorders: systematic review and meta-analysis. Maturitas. 2010;65:225–36.
Hernández JL, Olmos JM, González-Macías J. Metabolic syndrome, fractures and gender. Maturitas. 2011;68:217–23.
Cappuccio FP, Meilahn E, Zmuda JM, Cauley JA. High blood pressure and bone-mineral loss in elderly white women: a prospective study. Study of Osteoporotic Fractures Research Group. Lancet. 1999;354:971–5.
Rejnmark L, Vestergaard P, Mosekilde L. Treatment with beta-blockers, ACE inhibitors, and calcium-channel blockers is associated with a reduced fracture risk: a nationwide case–control study. J Hypertens. 2006;24:581–9.
Vestergaard P, Rejnmark L, Mosekilde L. Hypertension is a risk factor for fractures. Calcif Tissue Int. 2009;84:103–11.
Hung J, McQuillan BM, Chapman CM, Thompson PL, Beilby JP. Elevated inteleukin-18 levels are associated with the metabolic syndrome independent of obesity and insulin resistance. Artheriscl Thromb Vasc Biol. 2005;25:1268–73.
Zuliani G, Volpato S, Galvani M, Blè A, Bandinelli S, Corsi AM, et al. Elevated C-reactive protein levels and metabolic syndrome in the elderly: The role of central obesity data from the InChianti study. Atherosclerosis. 2009;203:626–32.
Dai SM, Nishioka K, Yudoh K. Interleukin (IL) 18 stimulates osteoclast formation through synovial T cells in rheumatoid arthritis: comparison with IL1 beta and tumour necrosis factor alpha. Ann Rheum Dis. 2004;63:1379–86.
Leidig-Bruckner G, Ziegler R. Diabetes mellitus a risk for osteoporosis? Exp Clin Endocrinol Diabetes. 2001;109 Suppl 2:S493–514.
Leidig-Bruckner G, Grobholz S, Bruckner T, Scheidt-Nave C, Nawroth P, Schneider JG. Prevalence and determinants of osteoporosis in patients with type 1 and type 2diabetes mellitus. BMC Endocr Disord. 2014;14:33.
Zuliani G, Volpato S, Galvani M, Blè A, Bandinelli S, Corsi AM, et al. Dietary calcium intake and risk of fracture and osteoporosis: prospective longitudinal cohort study. BMJ. 2011;342:d1473.
Acknowledgements
This work was supported by the Shanghai Science and Technology Commission (15411953200, 10411956600, 14ZR1427400), National Natural Science Foundation of China (81300667, 81370953, 81370935), Shanghai Health System Outstanding Young Talents Training Program (XYQ2013098), Shanghai Education Committee Key Program (14zz110). National Clinical Research Center for Metabolic Diseases (2013BAI09B13), National Key New Drug Creation and Manufacturing Program of Ministry of Science and Technology (2012ZX09303006-001). We thank the field workers for their contribution and the participants for their cooperation.
Availability of data and materials
The dataset supporting the conclusions of this article is included within the article and its additional file.
Authors’ contributions
Conceived and designed the experiments: QS. Analyzed the data: LQ, ZY. Contributed reagents/materials/analysis tools: LG, ZY, WZ, HG, XL, LZ, SL, YX, HZ, YN, GN. Wrote the paper: LQ, ZY. All authors read and approved the final manuscript.
Competing interests
The authors declared that there is no duality of interest associated with this manuscript.
Ethics approval
All procedures were approved by the Emory University Institutional Animal Care and Use Committee.
Author information
Authors and Affiliations
Corresponding authors
Additional file
Additional file 1:
Table S1A. Characteristics of Men and Women Stratified by Metabolic Syndrome Status (ATPIII criteria). Table S1B. Characteristics of Men and Women Stratified by Metabolic Syndrome Status (IDF criteria). (DOC 103 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Qin, L., Yang, Z., Zhang, W. et al. Metabolic syndrome and osteoporotic fracture: a population-based study in China. BMC Endocr Disord 16, 27 (2016). https://doi.org/10.1186/s12902-016-0106-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-016-0106-x