
Abstract
Background
In rectal cancer surgery, recent studies have found associations between clinical factors, especially pelvic parameters, and surgical difficulty; however, their findings are inconsistent because the studies use different criteria. This study aimed to evaluate common clinical factors that influence the operative time for the laparoscopic anterior resection of low and middle rectal cancer.
Methods
Patients who underwent laparoscopic radical resection of low and middle rectal cancer from January 2018 to December 2020 were retrospectively analyzed and classified according to the operative time. Preoperative clinical and magnetic resonance imaging (MRI)-related parameters were collected. Logistic regression analysis was used to identify factors for predicting the operative time.
Results
In total, 214 patients with a mean age of 60.3 ± 8.9 years were divided into two groups: the long operative time group (n = 105) and the short operative time group (n = 109). Univariate analysis revealed that the male sex, a higher body mass index (BMI, ≥ 24.0 kg/m2), preoperative treatment, a smaller pelvic inlet (< 11.0 cm), a deeper pelvic depth (≥ 10.7 cm) and a shorter intertuberous distance (< 10.1 cm) were significantly correlated with a longer operative time (P < 0.05). However, only BMI (OR 1.893, 95% CI 1.064–3.367, P = 0.030) and pelvic inlet (OR 0.439, 95% CI 0.240–0.804, P = 0.008) were independent predictors of operative time. Moreover, the rate of anastomotic leakage was higher in the long operative time group (P < 0.05).
Conclusion
Laparoscopic rectal resection is expected to take longer to perform in patients with a higher BMI or smaller pelvic inlet.
Similar content being viewed by others


Introduction
Colorectal cancer is the third most common cancer and the second leading cause of cancer-related death among all malignant tumors in the world [1]. Total mesorectal excision (TME) is the standard of radical surgery for rectal cancer and directly affects the local recurrence and overall survival [2, 3]. Laparoscopic rectal resection has been shown to be comparable to open surgery in terms of safety and long-term prognosis but is less invasive and allows faster recovery [4,5,6,7]. Especially in patients with low and middle rectal cancer, laparoscopic surgery provides a better view of the surgical field and finer anatomy [8], which is conducive to improving the quality of TME. Nevertheless, laparoscopic TME can be challenging in some patients with a narrow pelvis [9].
In addition to the surgical technique, surgical difficulty may be affected by body mass index (BMI), sex, tumor location, tumor size, and pelvic size [10]. Preoperative magnetic resonance imaging (MRI) can be used to determine the depth of tumor invasion, circumferential resection margin (CRM) involvement, vascular invasion, and lymph node enlargement; as such, it is an essential tool for determining the optimal treatment strategy for rectal cancer. Moreover, an MRI evaluation of pelvic shape and tumor position is also helpful for surgical resection planning. A recent meta-analysis showed that MRI-based pelvic measurements could effectively predict the surgical difficulty of TME [11]. However, the pelvic measurement parameters reported in the relevant literature are inconsistent. Previous studies mostly used the criteria proposed by Escal [12] for evaluation, but we found they had some limitations rendering them unsuitable for all centers.
The operative time was utilized as the primary indicator of intraoperative difficulty, as in previous studies [13, 14]. In this study, a group analysis was conducted based on the median operative time of different surgeons. This approach could reflect the complexity of surgery more objectively. We focused on evaluating common clinical factors, including pelvic parameters measured by MRI, influencing the operative time for the laparoscopic anterior resection of low and middle rectal cancer.
Patients and methods
Patients
Between January 2018 and December 2020, consecutive patients with rectal cancer who underwent laparoscopic radical resection at Peking University Cancer Hospital were identified. Patients with mid/low rectal adenocarcinoma (within 10 cm of the anal verge) were included. Patients who had undergone a more extensive surgery, including pelvic exenteration, combined evisceration or lateral pelvic lymph node dissection, abdominal perineal resection (APR), or transanal TME (TaTME), and those with insufficient preoperative MRI data were excluded. This study was approved by the Medical Ethics Committee of Peking University Cancer Hospital.
Study design
All surgeons belonged to the same department and received structured training on laparoscopic surgery. Each patient was placed in the lithotomy position under general anesthesia. Five ports were used to conduct laparoscopic tumor-specific TME. The rectum was transected at least 2 cm distal to the tumor, while mesorectal tissue was resected at a position at least 5 cm distal from the tumor or to the levator ani. Then, end-to-end anastomosis was completed with the double-stapling technique. All operations were performed by experienced surgeons who had completed over 100 laparoscopic rectal cancer surgeries. Moreover, the surgical teams were relatively stable.
In this study, some patients underwent ileostomy simultaneously with resection. To reduce the impact of this extra procedure, the operative time for these patients was defined as the originally recorded time minus 15 min. Then, the median operative time of each surgeon was set as the cutoff value. Patients whose operative time was longer than the cutoff value of the corresponding surgeon were assigned to the long operative time (LOT) group, and the others to the short operative time (SOT) group. Then the clinical data were compared.
Pelvic MRI measurements
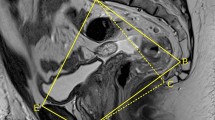
All patients analyzed underwent an abdominopelvic MRI examination before the operation. T2-weighted imaging (T2WI) was used to measure the pelvimetric parameters, including eight on the sagittal view and two on the transverse view (Fig. 1). The following measurements were obtained: (1) pelvic inlet: distance from the sacral promontory to the superior aspect of pubic symphysis; (2) pubococcygeal distance: distance between the tip of the coccyx and superior aspect of pubic symphysis; (3) pelvic length: distance from the tip of the coccyx to the sacral promontory; (4) sacral depth: perpendicular distance from the sacrococcygeal line to the deepest point of the sacrococcygeal hollow; (5) pelvic depth: perpendicular distance from the tip of the coccyx to the pelvic inlet line; (6) pelvic outlet: distance from the tip of the coccyx to the inferior aspect of the pubic symphysis; (7) interspinous distance: distance between the tips of the ischial spines; (8) intertuberous distance: distance between the lowest points of the ischial tuberosities; (9) anorectal angle: angle between the rectum and anal canal; and (10) sacrococcygeal angle: angle between the deepest point of the sacrococcygeal hollow to the sacral promontory and the tip of the coccyx.

MRI-based pelvimetry. A: pelvic inlet; B: pubococcygeal distance; C: pelvic length; D: sacral depth; E: pelvic depth; F: pelvic outlet; G: interspinous distance; H: intertuberous distance; α: anorectal angle; β: sacrococcyx angle
Outcome measures
The primary outcome was predictors of the operative time. The secondary outcome was the early morbidity rate within 30 days after surgery.
Statistical analysis
The statistical analysis was performed using SPSS version 22.0. Categorical variables are expressed as the mean ± standard deviation and were evaluated using a χ2 test or Fisher’s exact test. Continuous variables are presented as numbers and percentages and were evaluated using an independent t test or the Mann–Whitney U test. Logistic regression was performed to determine predictors of the operative time. The cutoff points for MRI pelvimetric parameters were defined as their median values. A two-sided P < 0.05 was considered statistically significant.
Results
Patient characteristics
Six hundred and three patients with rectal cancer who underwent laparoscopic radical resection were identified. And 214 patients with a mean age of 60 years were enrolled in the final analysis (Fig. 2). Most patients were male (63.6%). The median BMI, distance from the anal verge, and tumor size were 24.1 kg/m2, 7.0 cm, and 3.0 cm, respectively. A total of 53.3% of patients received neoadjuvant treatment, and 59.8% underwent ileostomy. Among all patients, 28 patients (13.1%) had a prior history of abdominal surgery.

Flow chart of patient selection
Comparison of parameters between the SOT and LOT groups
Based on the above definitions, 109 and 105 cases were included in the SOT and LOT groups, respectively, with a median operative time of 119.3 ± 25.0 min and 170.3 ± 30.8 min, respectively (P < 0.05). As illustrated in Table 1, the patients in the LOT group were mostly male, had a higher BMI, more preoperative treatment, a smaller pelvic inlet, a shorter intertuberous distance, and a deeper pelvis (P < 0.05) (Table 1).
Predictors of operative time
Univariate analysis revealed that the male sex, a higher BMI (≥ 24.0 kg/m2), preoperative treatment, a smaller pelvic inlet (< 11.0 cm), a deeper pelvic depth (≥ 10.7 cm) and a shorter intertuberous distance (< 10.1 cm) were significantly correlated with a longer surgical duration (P < 0.05). However, only BMI (OR 1.893, 95% CI 1.064–3.367, P = 0.030) and pelvic inlet (OR 0.439, 95% CI 0.240–0.804, P = 0.008) were independent predictors of operative time (Table 2).
Complications in different groups
Complications in the different groups were analyzed. There were no differences in pulmonary infection, pelvic infection, postoperative ileus, or anastomotic bleeding. However, the anastomotic leakage rate was higher in the LOT group (P < 0.05) (Table 3).
Discussion
Recent studies have shown that several parameters are associated with the surgical difficulty of laparoscopic anterior resection for low and middle rectal cancer, but the results are inconsistent [15,16,17,18]. The present study demonstrated that a higher BMI and smaller pelvic inlet could help predict the duration of surgery, which might be helpful for preoperative assessment.
Operating rooms currently account for 35–40% of hospital costs and 60–70% of hospital revenues [19]. The improvement of operating room productivity has an important impact on the financial performance and ultimately the ethical performance of the hospital [20]. Therefore, hospital management focuses on the effectiveness of schedules and plans. In our study, the results showed that we could use BMI and pelvic inlet to predict the operative time. These are two common parameters that can be easily obtained. We believe that a simple preoperative evaluation to measure BMI and pelvic inlet can help to determine more effective operating room arrangements, especially in centers that are short on surgical resources [21].
The criteria for grading surgical difficulty proposed by Escal [12] include duration of surgery > 300 min, conversion to open procedure, use of transanal dissection, postoperative hospital stay > 15 days, blood loss > 200 ml, and morbidity (grades II and III). The surgical difficulty grade ranged from 0 to 12, and patients scoring six or higher were considered to have high surgical difficulty. However, we found that the critical value of the criteria varies significantly from center to center. Yamamoto [15] analyzed the data of 121 patients undergoing minimally invasive rectal surgery and found that the median blood loss was only 30 ml, which is lower than the 200 ml proposed by Escal [12]. Therefore, Yamamoto [15] changed the threshold for blood loss to 100 ml. Moreover, the median operative time and postoperative hospital stay were 310 min and 18 days, respectively, so those criteria were also adjusted accordingly. However, in the studies by Sun [18] and Chen [16], the average postoperative hospital stay was 8.0 days and 7.7 days, respectively. As a result, these authors adjusted the standard critical value of postoperative hospital stay to 7 days for analysis. In addition, they defined difficult operations with an overall score greater than 3 points, rather than the six used in the previous study. Although different centers reported adopting Escal’s grading standards, most of them adopted adjusted standards, indicating that there are still limitations inherent to these grading criteria. In our opinion, the criteria can be influenced by many factors, such as the surgeon’s style and behavior, the availability of rapid rehabilitation, and medical resources. Therefore, we thought none of the criteria could exactly reflect the surgical difficulty until now. In this study, we compared differences in the operative time, which could be accurately obtained, between different patients. Moreover, we proposed that individual grouping based on the operative times of different surgeons would be more beneficial to make the results more objective and repeatable.
Anastomotic leakage is one of the most common postoperative complications of surgery for rectal cancer and can prolong the hospital stay, delay the adjuvant treatment, increase the financial burden, and even lead to death in serious cases [22]. In addition, anastomotic leakage has been found to be related to increased local recurrence and decreased overall survival, cancer-specific survival, and disease-free survival [23]. This study showed that the rate of anastomotic leakage after rectal cancer surgery was higher in the LOT group, which is consistent with results reported by Qu [24]. Therefore, these patients merit more attention in clinical work and timely monitoring when necessary. Moreover, the operative time was found to be related to obesity and to a small pelvic inlet. Obese patients have a thick mesorectum, which leads to a relatively narrow pelvic cavity that makes the surgery difficult. During the procedure, to fully expose the surgical field, repeated strong pulling of the proximal intestinal tube and tissues surrounding the site of anastomosis would increase additional damage, resulting in poor postoperative anastomotic healing. In addition, the small pelvic inlet makes it challenging to insert the stapler into the deep pelvis or necessitates more stapler firings for rectal transection, both of which are risk factors for anastomotic leakage [25].
Obesity has been found to be associated not only with increases in operative time and blood loss [14, 26, 27] but also with higher rates of anastomotic leakage, surgical-site infection (SSI), urinary tract infection (UTI), sepsis, and venous thromboembolism (VTE) [28,29,30]. The increased visceral obesity volume and mesenteric fat area (MFA) in obese patients makes performing laparoscopic surgery for rectal cancer a unique challenge [31]. In this study, the patient BMI ranged from 16.2 to 31.4 kg/m2, with a mean 24.1 kg/m2, which is lower than that in Western populations. Nevertheless, our results agreed with those of previous reports that found a positive association between BMI and operative time [13, 32].
On the other hand, studies have shown that the bony structure of the pelvis, such as the depth and length of the sacrum, the pelvic inlet and outlet, and the angle of the pelvis, are independent predictors of the duration of surgery and can be used as surrogate markers of TME difficulty [11, 15, 33]. In our study, the univariate analysis results showed differences in three bone indices, i.e., the pelvic inlet, ischial intertuberous diameter, and pelvic depth, suggesting that a deep and narrow pelvis did affect the duration of surgery. Restricted working space directly affects how difficult it is to perform surgery safely and quickly; in addition, visibility and coordination are required for surgery in these spaces to be optimized. Moreover, multivariate analysis showed that the pelvic inlet was an independent risk factor; thus, this metric merits special attention in rectal resection patients. In our retrospective review of surgical videos of some patients who underwent prolonged surgery, we found that several techniques might help to reduce the operative time, such as suspending the uterus or peritoneal reflection, lifting the upper rectum with a string, and wiping the lenses with iodophor to prevent fog. However, what mattered most was teamwork. We believe that these issues should not be a major problem for professional surgical teams because they have more experience in creating suitable surgical areas and are able to identify and anatomize structures even in a restricted pelvic working space.
Not surprisingly, there are some limitations to this study. This was a retrospective analysis, and the operative time was measured from the beginning of anesthesia to the end of surgery, rather than as the pelvic anatomy time. However, the inclusion criteria were strict, and cases of high rectal cancer, lateral lymph node dissection, multivisceral resection, and transanal dissection were excluded to minimize the influence of confounding factors. In addition, pelvic measurements in this study were made by a single observer; as such, quantification of interobserver variability could not be performed.
Conclusions
In conclusion, our findings indicate that a higher BMI and smaller pelvic inlet are significantly associated with a longer operative time. These two parameters, BMI and pelvic inlet, are helpful for predicting the duration of TME for low and middle rectal cancer and should be evaluated preoperatively.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author.
Abbreviations
- TME:
-
Total mesorectal excision
- CRM:
-
Circumferential resection margin
- APR:
-
Abdominal perineal resection
- TaTME:
-
Transanal total mesorectal excision
- LOT:
-
Long operative time
- SOT:
-
Short operative time
- BMI:
-
Body mass index
- SSI:
-
Surgical-site infection
- UTI:
-
Urinary tract infection
- VTE:
-
Venous thromboembolism
- MFA:
-
Mesenteric fat area
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin. 2018;68(6):394–424.
Sung S, Kim SH, Lee JH, et al. Continuous effect of radial resection margin on recurrence and survival in rectal cancer patients who receive preoperative chemoradiation and curative surgery: a multicenter retrospective analysis. Int J Radiat Oncol Biol Phys. 2017;98(3):647–53.
Madbouly KM, Hussein AM, Abdelzaher E. Long-term prognostic value of mesorectal grading after neoadjuvant chemoradiotherapy for rectal cancer. Am J Surg. 2014;208(3):332–41.
Fleshman J, Branda ME, Sargent DJ, et al. Disease-free survival and local recurrence for laparoscopic resection compared with open resection of stage II to III rectal cancer: follow-up results of the ACOSOG Z6051 Randomized Controlled Trial. Ann Surg. 2019;269(4):589–95.
Bonjer HJ, Deijen CL, Haglind E, Group CIS. A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med. 2015;373(2):194.
Chen K, Cao G, Chen B, et al. Laparoscopic versus open surgery for rectal cancer: a meta-analysis of classic randomized controlled trials and high-quality nonrandomized studies in the last 5 years. Int J Surg. 2017;39:1–10.
Kethman WC, Bingmer KE, Ofshteyn A, et al. Effects of surgical approach on short- and long-term outcomes in early-stage rectal cancer: a multicenter, propensity score-weighted cohort study. Surg Endosc. 2022. https://doi.org/10.1007/s00464-022-09033-z.
Hasegawa S, Nagayama S, Nomura A, Kawamura J, Sakai Y. Multimedia article. Autonomic nerve-preserving total mesorectal excision in the laparoscopic era. Dis Colon Rectum. 2008;51(8):1279–82.
Baik SH, Kim NK, Lee KY, et al. Factors influencing pathologic results after total mesorectal excision for rectal cancer: analysis of consecutive 100 cases. Ann Surg Oncol. 2008;15(3):721–8.
Leonard D, Penninckx F, Fieuws S, et al. Factors predicting the quality of total mesorectal excision for rectal cancer. Ann Surg. 2010;252(6):982–8.
Hong JS, Brown KGM, Waller J, Young CJ, Solomon MJ. The role of MRI pelvimetry in predicting technical difficulty and outcomes of open and minimally invasive total mesorectal excision: a systematic review. Tech Coloproctol. 2020;24(10):991–1000.
Escal L, Nougaret S, Guiu B, et al. MRI-based score to predict surgical difficulty in patients with rectal cancer. Br J Surg. 2018;105(1):140–6.
McKechnie T, Ramji K, Kruse C, et al. Posterior mesorectal thickness as a predictor of increased operative time in rectal cancer surgery: a retrospective cohort study. Surg Endosc. 2021. https://doi.org/10.1007/s00464-021-08674-w.
Yamaoka Y, Yamaguchi T, Kinugasa Y, et al. Mesorectal fat area as a useful predictor of the difficulty of robotic-assisted laparoscopic total mesorectal excision for rectal cancer. Surg Endosc. 2019;33(2):557–66.
Yamamoto T, Kawada K, Kiyasu Y, et al. Prediction of surgical difficulty in minimally invasive surgery for rectal cancer by use of MRI pelvimetry. BJS Open. 2020;4(4):666–77.
Chen J, Sun Y, Chi P, Sun B. MRI pelvimetry-based evaluation of surgical difficulty in laparoscopic total mesorectal excision after neoadjuvant chemoradiation for male rectal cancer. Surg Today. 2021;51(7):1144–51.
Deangelis N, Pigneur F, Martinez-Perez A, et al. Assessing surgical difficulty in locally advanced mid-low rectal cancer: the accuracy of two MRI-based predictive scores. Colorectal Dis. 2019;21(3):277–86.
Sun Y, Chen J, Ye C, et al. Pelvimetric and nutritional factors predicting surgical difficulty in laparoscopic resection for rectal cancer following preoperative chemoradiotherapy. World J Surg. 2021;45(7):2261–9.
Ramme AJ, Hutzler LH, Cerfolio RJ, Bosco JA. Applying systems engineering to increase operating room efficiency. Bull Hosp Jt Dis. 2020;78(1):26–32.
Gur S, Eren T. Application of operational research techniques in operating room scheduling problems: literature overview. J Healthcare Eng. 2018;2018:5341394. https://doi.org/10.1155/2018/5341394.
Boggs SD, Tan DW, Watkins CL, Tsai MH. OR management and metrics: how it all fits together for the healthcare system. J Med Syst. 2019;43(6):147.
Bostrom P, Haapamaki MM, Rutegard J, Matthiessen P, Rutegard M. Population-based cohort study of the impact on postoperative mortality of anastomotic leakage after anterior resection for rectal cancer. BJS Open. 2019;3(1):106–11.
Yang J, Chen Q, Jindou L, Cheng Y. The influence of anastomotic leakage for rectal cancer oncologic outcome: a systematic review and meta-analysis. J Surg Oncol. 2020;121(8):1283–97.
Qu H, Liu Y, Bi DS. Clinical risk factors for anastomotic leakage after laparoscopic anterior resection for rectal cancer: a systematic review and meta-analysis. Surg Endosc. 2015;29(12):3608–17.
Balciscueta Z, Uribe N, Caubet L, et al. Impact of the number of stapler firings on anastomotic leakage in laparoscopic rectal surgery: a systematic review and meta-analysis. Tech Coloproctol. 2020;24(9):919–25.
Ri M, Aikou S, Seto Y. Obesity as a surgical risk factor. Ann Gastroenterol Surg. 2018;2(1):13–21.
Tjeertes EK, Hoeks SE, Beks SB, Valentijn TM, Hoofwijk AG, Stolker RJ. Obesity—a risk factor for postoperative complications in general surgery? BMC Anesthesiol. 2015;15:112.
Wahl TS, Patel FC, Goss LE, Chu DI, Grams J, Morris MS. The obese colorectal surgery patient: surgical site infection and outcomes. Dis Colon Rectum. 2018;61(8):938–45.
Bell S, Kong JC, Wale R, et al. The effect of increasing body mass index on laparoscopic surgery for colon and rectal cancer. Colorectal Dis. 2018;20(9):778–88.
Fung A, Trabulsi N, Morris M, et al. Laparoscopic colorectal cancer resections in the obese: a systematic review. Surg Endosc. 2017;31(5):2072–88.
Boyle KM, Chalmers AG, Finan PJ, Sagar PM, Burke D. Morphology of the mesorectum in patients with primary rectal cancer. Dis Colon Rectum. 2009;52(6):1122–9.
Zhou XC, Su M, Hu KQ, et al. CT pelvimetry and clinicopathological parameters in evaluation of the technical difficulties in performing open rectal surgery for mid-low rectal cancer. Oncol Lett. 2016;11(1):31–8.
Lee JM, Han YD, Cho MS, et al. Prediction of transabdominal total mesorectal excision difficulty according to the angle of pelvic floor muscle. Surg Endosc. 2020;34(7):3043–50.
Acknowledgements
Not applicable.
Funding
This study was sponsored by the Beijing Municipal Science & Technology Commission Capital Clinical Research Special Fund (Grant No. Z151100004015105); National Natural Science Foundation of China (Grant No. 81773214); Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support (Grant No. ZYLX202116); Fund of Fujian Cancer Hospital (Grant No. 2021YN06); Startup Fund for Scientific Research, Fujian Medical University (Grant No. 2018QH1223); and Bethune Ethicon Excellent Surgery Foundation (Grant No. HZB-20181119-46).
Author information
Authors and Affiliations
Contributions
Conception and design: AW, WT; administrative support: AW, WT; provision of study materials or patients: AW, WZ; collection and assembly of data: WT, MC, JL; data analysis and interpretation: WT, JL, WZ; manuscript writing: all authors. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee of Peking University Cancer Hospital. All the subjects provided written informed consent. And the methods were carried out in accordance with Ethical standards in the 1964 Declaration of Helsinki and its subsequent amendments.
Consent for publication
Informed consent to publish this work has been received from all participants.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Teng, W., Liu, J., Chen, M. et al. BMI and pelvimetry help to predict the duration of laparoscopic resection for low and middle rectal cancer. BMC Surg 22, 402 (2022). https://doi.org/10.1186/s12893-022-01840-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-022-01840-4