
Abstract
Background
This study aimed to examine whether the non-weight-bearing tunnel view X-ray is effective for short-term evaluation of medial meniscus posterior root tear (MMPRT) by assessing the X-ray characteristics at the initial and follow-up visits.
Methods
This was a retrospective longitudinal study of 26 enrolled knees diagnosed with MMPRT on magnetic resonance imaging. The distance between the medial tibial eminence and medial femoral condyle (MTE–MFC distance) and medial tibiofemoral joint (MTFJ) width were measured by obtaining non-weight-bearing tunnel view and frontal view X-ray radiographs. The initial and follow-up values at a median interval of 17 days were compared. Additionally, the correlations between the MTE–MFC distance increase rate and body mass index (BMI), age, femorotibial angle (FTA), and posterior tibial slope (PTS) were evaluated using linear regression analysis.
Results
The tunnel view images of the initial and follow-up X-rays showed a significant increase in the MTE–MFC distance and a significant decrease in the MTFJ width. Furthermore, a moderate correlation was observed between the change in the MTE–MFC distance and the time interval between X-rays. However, no substantial correlation was observed for the change in the MTFJ width over time. Moreover, no significant correlation was observed between the change in the MTE–MFC distance in the non-weight-bearing tunnel view and BMI, age, FTA, and PTS.
Conclusions
The non-weight-bearing tunnel view is highly beneficial for evaluating MMPRT progression in the short term.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
A medial meniscus posterior root tear (MMPRT) is defined as a radial tear < 10 mm from the medial meniscus posterior root attachment site, an oblique tear involving the root attachment, or an avulsion of the root attachment [1, 2]. Once MMPRT occurs, the hoop action breaks down, and posteromedial extrusion of the medial meniscus occurs [3]. Magnetic resonance imaging (MRI)-based studies have reported that medial meniscal extrusion (MME) progresses in the short term when MMPRT is triggered, and the more the MME progression, the worse the prognosis [4]. It is a disease that widely disrupts the structure and function of the knee joint and progresses to subchondral insufficiency fracture of the knee and rapid progression to osteoarthritis of the knee [5,6,7]. Furthermore, nonsurgical treatment of MMPRT has been shown to result in poor outcomes [8]. Therefore, proper evaluation and treatment selection are important.
MRI and ultrasonography have been reported to be methods for evaluating MME with MMPRT [9, 10]. It is possible to evaluate the meniscus and articular cartilage in detail using MRI [9]. However, MRI is expensive, not widely available, and unsuitable for frequent imaging [11]. Ultrasonography is useful for evaluating MME, but it is difficult to assess the bony nature of deep joints [10]. Conversely, X-ray is a simple, inexpensive, and widely used method. Thus, it is important to evaluate the usefulness of X-rays. Recently, Rosenberg and non-weight-bearing tunnel views have been reported to be useful methods for evaluating the initial diagnosis of MMPRT [12, 13]. These methods, which are based on imaging of knee flexion, reflect MME and have been reported to show a decrease in the medial tibiofemoral joint (MTFJ) width and an increase in the distance between the medial tibial eminence and medial femoral condyle (MTE–MFC distance) in the affected knee compared with the contralateral knee [12, 13]. However, no study has been conducted on short-term X-ray evaluation methods after MMPRT.
We hypothesized that the non-weight-bearing tunnel view could be a useful indicator for short-term evaluation in MMPRT. Therefore, this study aimed to investigate the X-ray characteristics, including the femorotibial angle (FTA) by the total length of the lower limbs, posterior tibial slope (PTS) by the lateral view, MTE–MFC distance by the frontal and non-weight-bearing tunnel views, and MTFJ width by the frontal and non-weight-bearing tunnel views, at the initial visit and next follow-up. Furthermore, the usefulness of the non-weight-bearing tunnel view in patients with MMPRT was examined by confirming the changes in the MTE–MFC distance and MTFJ width after MMPRT.
Methods
Study population
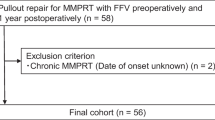
This was a retrospective longitudinal study using the medical records of 118 knees diagnosed with MMPRT using MRI in the outpatient clinic at Nihon Koukan Hospital, Japan, between April 2020 and June 2023 to investigate the X-ray characteristics at the initial visit and follow-ups. MMPRT was diagnosed using the ghost sign on the sagittal view and the cleft sign on the coronal view in MRI [14]. The inclusion criteria included (1) received within two months of clear popliteal painful popping, (2) Kellgren–Lawrence classification grade ≤ 2, (3) available X-ray radiography records for the frontal, total length of the lower limbs, lateral, and tunnel views, and (4) available follow-up X-ray within two months of the initial visit. After applying these criteria, 26 knees were included in the analysis. Of the 26 knees, 17 were treated surgically after MMPRTs were confirmed via arthroscopic procedures. Figure 1 shows a flow diagram of the patient selection process. The patients were without a previous ligament and/or meniscal injury, previous fracture around the knee, rheumatoid arthritis, or meniscus tear other than MMPRT diagnosed on MRI.

Flowchart of participant selection. BMI: body mass index, PP: P popliteal painful popping, and K–L grade: Kellgren–Lawrence classification grade
X-ray measurements
X-rays of the total length of the lower limbs on weight-bearing were taken (Sonialvision G4, Shimizu Medical Systems and Equipment, Japan) while the patient was standing with maximum knee extension with weight-bearing. FTA measurements of the affected side of the knee were performed using X-rays of the total length of the lower limbs. FTA is the angle between the femoral and tibial anatomical axes, which is particularly useful for diagnosing knee deformities such as osteoarthritis. The femoral anatomical axis is a line connecting the centers of the femoral shaft 10 cm above the intercondylar notch to the intercondylar notch, whereas the tibial anatomical axis is a line connecting the centers of the tibial shaft 10 cm below the tibial plateau to the tibial plateau. The angle measured at the point where these two axes intersect is considered the FTA.
X-rays of the lateral view of the knee were obtained with overlapping femoral condyles as true lateral X-ray projection. PTS measurements were performed using X-rays of the lateral view of the knee. PTS is the angle between the tangent to the medial tibial plateau and a line perpendicular to the posterior tibial cortex [15]. Despite its simplicity in measuring PTS, adjusting for overlapping femoral condyles plays an important role and is a reliable landmark for true lateral X-ray projection [16].
Several methodologies have been established for capturing the tunnel view, including the Holmblad method (non-weight-bearing, 70° flexion), Béclere method (non-weight-bearing, 60° flexion), Camp–Coventry method (non-weight-bearing, 40°–50° flexion), Rosenberg method (weight-bearing, 45° flexion), and Schuss view (weight-bearing, 30°–40° flexion) [17, 18]. The non-weight-bearing tunnel view was obtained by positioning the patient prone and flexing their knee 60° over an angle block and sandbag, thus facilitating an anteroposterior vantage point [13]. The X-ray beam was meticulously configured to be parallel to the tibial plateau.
According to the tunnel and frontal views, the MTE line was crafted to be perpendicular to the tangent line to both the medial and lateral condyles and pass through the apex of the medial tibial eminence. Similarly, the MFC line was established perpendicular to the tangent line of the medial and lateral condyles of the femur and through the posterior aspect of the medial femoral condyle. The MTE–MFC distance was assessed using these lines according to the Kodama method (Fig. 2). Finally, the MTFJ width was determined by measuring from the center of the MFC to the center of the medial tibial plateau (Fig. 3).

Frontal (a) and non-weight-bearing tunnel (b) view measurements. The MTE–MFC distance (black arrow) is the distance between the MTE and MFC. The MTE line is drawn perpendicular to the line tangent to the medial and lateral condyles. The MFC line, similar in its perpendicularity to the medial and lateral condyles of the femur, is drawn in tangent to the posterior aspect of medial femoral condyle

Frontal (a) and non-weight-bearing tunnel (b) view measurements. The MTFJ width was calculated. The black arrow signifies the distance taken to measure the MTFJ width from the center of the MFC to the medial tibial plateau center. MTFJ: medial tibiofemoral joint and MFC: medial femoral condyle
MME measurements on MRI
Only MME measurements at the level of the intercondylar eminence on coronal (T2*) scans were analyzed. They were taken by initially drawing a vertical line at the medial margin of the tibial plateau. MME was defined as the length of the second line extending from the first line to the medial margin of the meniscus [19]. Osteophytes were excluded when determining the medial margin of the tibial plateau [20].
Statistical analysis
Continuous variables were presented as median and interquartile range. Changes in X-ray measurements between the first and follow-up X-rays were evaluated using the Wilcoxon signed-rank test. Linear regression analysis was performed to evaluate changes in the MTE–MFC distance and MTFJ width in the tunnel view with X-ray interval (days). Furthermore, linear regression analysis using Pearson’s correlation coefficient was performed to evaluate the correlation between body mass index (BMI), age, FTA, and PTS and the MTE–MFC distance increase rate (mm/day). All statistical analyses were performed using StatFlex version 7 (Artech Co., Ltd.). P-values of < 0.05 indicated statistical significance. R2 ≥ 0.6, R2 ≥ 0.4, and R2 < 0.4 indicated good, moderate, and poor correlations, respectively. The sample size was estimated with a minimum statistical power of 80% (α = 0.05). The required sample size was 21, and 26 patients were finally included in this study. The sample size was calculated using G*Power version 3.1.9.7 (Universität Kiel, Kiel, Germany).
Reproducibility
The measurement of FTA, PTS, MTE–MFC distance, and MTFJ width were retrospectively assessed by two orthopedic surgeons who were blinded. These repeated assessments were conducted at a minimum of a 2-week interval. These measurements were evaluated using intraclass correlation coefficients to determine the intra- and interobserver reproducibility: intraobserver: 0.90–0.98; interobserver: 0.91–0.96.
Results
Table 1 shows the characteristics of the study participants. The median age of the participants was 65 years (59.0–76.0 years). Regarding physique, the median BMI was 25.6 kg/m2 (23.2–28.9 kg/m2). The median angles of FTA and PTS were 177.1° (172.7°–183.1°) and 8.0° (4.4°–9.2°), respectively. The median time elapsed from sustaining an injury to the first X-ray was 14 days (3–26 days). Additionally, the median time interval from the initial to follow-up X-rays was 17 days (13–31 days).
The comparison between the initial X-ray examination and subsequent follow-up frontal view radiographs revealed no notable alterations in the MTE–MFC distance or MTFJ width (P = 0.39 and P = 0.07, respectively; Table 2). In contrast, images obtained from the non-weight-bearing tunnel view showed a significant increase in the MTE–MFC distance and a significant decrease in the MTFJ width (P < 0.01 and P < 0.01, respectively; Table 2).
Figure 4 shows the linear regression analysis of ΔMTE–MFC distance and ΔMTFJ width in the non-weight-bearing tunnel view with the X-ray interval. A moderate correlation was observed between ΔMTE–MFC distance and the X-ray interval (R2 = 0.53, P < 0.01, slope = 0.009). However, poor correlation was observed between ΔMTFJ width and the X-ray interval (R2 = 0.18, P = 0.03, slope = 0.01).

Correlations using linear regression analysis between changes in the MTE–MFC distance and the MTFJ width in a non-weight-bearing tunnel view and the X-ray interval. (a) A moderate correlation was observed between the changes in the MTE–MFC distance and the X-ray intervals (R2 = 0.53). (b) The changes in the MTFJ width did not show a significant correlation with the X-ray intervals (R2 = 0.18). MTFJ: medial tibiofemoral joint, MFC: medial femoral condyle, and MTE: medial tibial eminence
Figure 5 shows the linear regression analysis of MTE–MFC distance increase rate in the non-weight-bearing tunnel view with BMI, age, FTA, and PTS. No slight correlation was observed between BMI, age, FTA, and PTS and the MTE–MFC distance.

Correlations using linear regression analysis between MTE–MFC distance increase rate in a non-weight-bearing tunnel view and BMI, age, FTA, and PTS. No noticeable correlation was observed between these variables and the MTE–MFC distance (R2 < 0.01 of all variables: a, b, c, d). MTE: medial tibial eminence, MFC: medial femoral condyle, BMI: body mass index, FTA: femorotibial angle, and PTS: posterior tibial angle
Discussion
In this study, significant increase in MTE–MFC distance and significant decrease in MTFJ width were observed within a short period of 17 days. Moreover, the amount of change in the MTE–MFC distance demonstrated a significant relationship with time, increasing by approximately 0.009 mm daily. In contrast, the MTFJ width did not show a substantial relationship with time. Furthermore, this study showed that factors such as BMI, age, FTA, and PTS did not significantly influence the radiographic progression of this condition.
A previous study examining a 5-year follow-up with conservative treatment of MMPRT reported an average narrowing of the joint fissure of 1.1 mm using X-ray frontal images [21]. Additionally, the same study reported the progression of the Kellgren–Laurence classification grade [21]. However, MMPRT is a type of injury that progresses relatively rapidly osteoarthritis and can cause subchondral insufficiency fracture of the knee. Therefore, appropriate short-term evaluation methods are necessary. To the best of our knowledge, no study has been conducted to investigate the short-term evaluation of X-rays in MMPRT. The Rosenberg view, Schuss method, and Camp–Coventry method have been reported as useful methods for evaluating knee osteoarthritis [17, 18]. These evaluation methods are considered superior for depicting the narrowing of the articular crease, posterior intercondylar notch, posterior femoral condyle, and tibial osteophytes [3, 17, 22, 23]. Recently, Rosenberg and non-weight-bearing tunnel views have been reported to be useful for diagnosing MMPRT [12, 13]. Both methods are useful for diagnosis because they show an increase in the MTE–MFC distance and a decrease in the MTFJ width compared with the contralateral knee, and both MTE–MFC distance and MTFJ width have been reported to be affected by MME progression [12, 13]. When MMPRT is triggered, MME shows rapid progression [24]. In longitudinal studies using MRI, MME has been reported to progress in an average of 48 days, and cross-sectional studies examining MME progression using MRI have reported MME progression in up to 12 months [4, 24].In this study, patients with MMPRT were observed over time to evaluate the usefulness of the non-weight-bearing tunnel view. The results showed that the MTE–MFC distance and MTFJ width did not significantly change in the frontal view. However, an increase in the MTE–MFC distance and a decrease in the MTFJ width were observed in the non-weight-bearing tunnel view, indicating that this method may be useful in the temporal evaluation of MMPRT progression.
The medial meniscus has multiple functions, such as shock absorption, joint stabilization, lubrication, and proprioception [25, 26]. When MMPRT is triggered, the hoop action of the medial meniscus collapses, the buttress effect of the lateral condyle of the femur breaks down, the medial condyle of the femur moves toward the posteromedial side, and consequently, the physiological function of the medial meniscus fails [3, 27]. In the normal knee, rollback motion of the femur occurs during knee flexion, and the medial meniscus moves posteromedially [28,29,30]. Previous studies evaluating the Cadaver from 0° to 90° flexed position have reported a larger MME and higher MTFJ pressure, especially in 60° flexion [3]. Furthermore, a study using MRI to evaluate 10° and 90° flexion positions reported a more posterior medial extrusion at 90° [31]. In this study, the non-weight-bearing tunnel view was in the 60° flexion, and the increase in the MTE–MFC distance and the decrease in the MTFJ width in the tunnel view were more pronounced than in the frontal view. Furthermore, significant progression was observed even in a short time, averaging 17 days. Okazaki et al. evaluated patients with MMPRT at a mean duration of 48 days and reported an average MME progression of 1.2 mm [24]. Further, they showed the absence of the MTFJ width progression [24]. In this study, the extent of change in the MTE–MFC distance was significantly associated with time. In contrast, the MTFJ width was not significantly associated with time. The MTFJ width is affected by the articular cartilage and meniscus [32]. Moreover, the MTE–MFC distance is not influenced by the articular cartilage, and therefore, is more sensitive than MME. These findings indicate that the non-weight-bearing tunnel view is a useful evaluation method after MMPRT in the short term.
MMPRT causes the progression of knee osteoarthritis, and better results have been reported with surgical treatment than with conservative treatment [33,34,35]. Particularly, MMPRT has been reported to be a poor prognostic factor for conservative treatment in cases of large MME [36]. However, the appropriate timing of the need for surgical treatment is unclear [4]. In the non-weight-bearing tunnel view, the decrease in the MTFJ width and the increase in the MTE–MFC distance are considered to reflect the MME itself [13]. This is a low-cost alternative and simple imaging method for evaluation using X-rays.
This study has several limitations. First, based on the inclusion criteria of this study, the diagnosis of MMPRT cannot be ruled out as an acute meniscus root tear. However, the patients presented with popliteal painful popping for approximately 2 months, and they presented with a K–L grade of ≤ 2. Thus, the probability of the conditions being an acute tear is high. Second, this was a retrospective study. Third, the sample size was small. Fourth, the follow-up period was short. Fifth, we were unable to evaluate the correlation between X-ray data and MRI evaluation, clinical outcomes, and subsequent treatment choices. Therefore, the possible usefulness of the non-weight-bearing tunnel view after MMPRT cannot be validated. Thus, future studies with larger sample sizes and longer follow-up durations should be conducted to evaluate the correlations between MMPRT and other parameters. Thus, it is necessary to study the correlation with other parameters with a larger sample size and long-term follow-up in future studies.
Conclusions
This study demonstrated the usefulness of the non-weight-bearing tunnel view in the short-term longitudinal evaluation of MMPRT. This imaging method may help detect the progression of meniscus extrusion and joint gap narrowing at an earlier stage.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MMPRT:
-
Medial meniscus posterior root tear
- MME:
-
Medial meniscal extrusion
- MRI:
-
Magnetic resonance imaging
- MTFJ:
-
Medial tibiofemoral joint
- MTE:
-
Medial tibial eminence
- MFC:
-
Medial femoral condyle
- FTA:
-
Femorotibial angle
- PTS:
-
Posterior tibial slope
- BMI:
-
Body mass index
References
Bin SI, Kim JM, Shin SJ. Radial tears of the posterior horn of the medial meniscus. Arthroscopy. 2004;20(4):373–8.
LaPrade CM, James EW, Cram TR, Feagin JA, Engebretsen L, LaPrade RF. Meniscal root tears: a classification system based on tear morphology. Am J Sports Med. 2015;43(2):363–9.
Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechanical consequences of a tear of the posterior root of the medial meniscus. Similar to total meniscectomy. J bone Joint Surg Am Volume. 2008;90(9):1922–31.
Furumatsu T, Kodama Y, Kamatsuki Y, Hino T, Okazaki Y, Ozaki T. Meniscal extrusion progresses shortly after the medial meniscus posterior root tear. Knee Surg Relat Res. 2017;29(4):295–301.
Guermazi A, Hayashi D, Jarraya M, Roemer FW, Zhang Y, Niu J, Crema MD, Englund M, Lynch JA, Nevitt MC, et al. Medial posterior meniscal root tears are associated with development or worsening of medial tibiofemoral cartilage damage: the multicenter osteoarthritis study. Radiology. 2013;268(3):814–21.
Chen BK, Lin YC, Liu YH, Weng PW, Chen KH, Chiang CJ, Wong CC. Correlation between subchondral insufficiency fracture of the knee and osteoarthritis progression in patients with medial meniscus posterior root tear. Diagnostics (Basel, Switzerland) 2023, 13(23).
Nukuto K, Matsushita T, Kamada K, Nishida K, Nagai K, Kanzaki N, Hoshino Y, Matsumoto T, Niikura T, Kuroda R. Development and analysis of mouse medial meniscus posterior root tear model. Calcif Tissue Int. 2023;112(1):55–65.
Krych AJ, Lamba A, Wang AS, Boos AM, Camp CL, Levy BA, Stuart MJ, Hevesi M. Nonoperative management of degenerative medial meniscus posterior root tears: poor outcomes at a minimum 10-year follow-up. Am J Sports Med. 2023;51(10):2603–7.
Chen E, Hou W, Wang H, Li J, Lin Y, Liu H, Du M, Li L, Wang X, Yang J, et al. Quantitative MRI evaluation of articular cartilage in patients with meniscus tear. Front Endocrinol. 2022;13:911893.
Sekiya I, Sasaki S, Miura Y, Aoki H, Katano H, Okanouchi N, Tomita M, Masumoto J, Koga H, Ozeki N. Medial tibial osteophyte width strongly reflects medial meniscus extrusion distance and medial joint space width moderately reflects cartilage thickness in knee radiographs. J Magn Reson Imaging: JMRI. 2022;56(3):824–34.
Wylie JD, Crim JR, Working ZM, Schmidt RL, Burks RT. Physician provider type influences utilization and diagnostic utility of magnetic resonance imaging of the knee. J bone Joint Surg Am Volume. 2015;97(1):56–62.
Kodama Y, Furumatsu T, Kamatsuki Y, Hiranaka T, Takahata T, Sadakane M, Ikuta H, Yasumitsu M, Ozaki T. Preliminary diagnosis of medial meniscus posterior root tears using the Rosenberg radiographic view. Knee Surg Relat Res. 2019;31(1):9.
Okamura H, Ishikawa H, Ohno T, Fujita S, Yamakami S, Akezuma H, Ishikawa K, Inagaki K. Potential of the non-weight-bearing tunnel view in diagnosing medial meniscus posterior root tear: a pilot study of X-ray characteristics. J Experimental Orthop. 2021;8(1):99.
Choi SH, Bae S, Ji SK, Chang MJ. The MRI findings of meniscal root tear of the medial meniscus: emphasis on coronal, sagittal and axial images. Knee surgery, sports traumatology, arthroscopy: official journal of the ESSKA 2012, 20(10):2098–2103.
Brazier J, Migaud H, Gougeon F, Cotten A, Fontaine C, Duquennoy A. [Evaluation of methods for radiographic measurement of the tibial slope. A study of 83 healthy knees]. Rev Chir Orthop Reparatrice Appar Mot. 1996;82(3):195–200.
Genin P, Weill G, Julliard R. The tibial slope. Proposal for a measurement method. Journal De Radiologie. 1993;74(1):27–33.
Babatunde OM, Danoff JR, Patrick DA Jr., Lee JH, Kazam JK, Macaulay W. The combination of the tunnel view and weight-bearing anteroposterior radiographs improves the detection of knee arthritis. Arthritis 2016, 2016:9786924.
Ballinger PW, Frank ED. Merrill’s atlas of radiographic positions and radiologic procedures. 2003, 1:320–325.
Szarmach A, Luczkiewicz P, Skotarczak M, Kaszubowski M, Winklewski PJ, Dzierzanowski J, Piskunowicz M, Szurowska E, Baczkowski B. Assessment of the relationship between the shape of the lateral meniscus and the risk of extrusion based on mri examination of the knee joint. PLoS ONE. 2016;11(7):e0159156.
Takahashi T, Yamanaka N, Ikeuchi M, Yamamoto H. Reproducibility of joint space width and the intermargin distance measurements in patients with medial osteoarthritis of the knee in various degrees of flexion. Skeletal Radiol. 2009;38(1):37–42.
Lee NH, Seo HY, Sung MJ, Na BR, Song EK, Seon JK. Does meniscectomy have any advantage over conservative treatment in middle-aged patients with degenerative medial meniscus posterior root tear? BMC Musculoskelet Disord. 2021;22(1):742.
Hing C, Raleigh E, Bailey M, Shah N, Marshall T, Donell S, Glasgow M. A prospective study of the diagnostic potential of the knee tunnel view radiograph in assessing anterior knee pain. Knee. 2007;14(1):29–33.
Ritchie JF, Al-Sarawan M, Worth R, Conry B, Gibb PA. A parallel approach: the impact of schuss radiography of the degenerate knee on clinical management. Knee. 2004;11(4):283–7.
Okazaki Y, Furumatsu T, Shimamura Y, Saiga K, Ohashi H, Uchino T, Kamatsuki Y, Okazaki Y, Ozaki T. Time-dependent increase in medial meniscus extrusion after medial meniscus posterior root tear analyzed by using magnetic resonance imaging. Knee Surg Relat Res. 2019;31(2):120–5.
Ozkoc G, Circi E, Gonc U, Irgit K, Pourbagher A, Tandogan RN. Radial tears in the root of the posterior horn of the medial meniscus. Knee Surg Sports Traumatol Arthroscopy: Official J ESSKA. 2008;16(9):849–54.
Villegas DF, Hansen TA, Liu DF, Donahue TL. A quantitative study of the microstructure and biochemistry of the medial meniscal horn attachments. Ann Biomed Eng. 2008;36(1):123–31.
Chung KS, Choi CH, Bae TS, Ha JK, Jun DJ, Wang JH, Kim JG. Comparison of tibiofemoral contact mechanics after various transtibial and all-inside fixation techniques for medial meniscus posterior root radial tears in a porcine model. Arthroscopy: J Arthroscopic Relat Surg : Official Publication Arthrosc Association North Am Int Arthrosc Association. 2018;34(4):1060–8.
Moro-oka TA, Hamai S, Miura H, Shimoto T, Higaki H, Fregly BJ, Iwamoto Y, Banks SA. Dynamic activity dependence of in vivo normal knee kinematics. J Orthop Research: Official Publication Orthop Res Soc. 2008;26(4):428–34.
Tanifuji O, Sato T, Kobayashi K, Mochizuki T, Koga Y, Yamagiwa H, Omori G, Endo N. Three-dimensional in vivo motion analysis of normal knees using single-plane fluoroscopy. J Orthop Science: Official J Japanese Orthop Association. 2011;16(6):710–8.
Vedi V, Williams A, Tennant SJ, Spouse E, Hunt DM, Gedroyc WM. Meniscal movement. An in-vivo study using dynamic MRI. J bone Joint Surg Br Volume. 1999;81(1):37–41.
Masuda S, Furumatsu T, Okazaki Y, Kodama Y, Hino T, Kamatsuki Y, Miyazawa S, Ozaki T. Medial meniscus posterior root tear induces pathological posterior extrusion of the meniscus in the knee-flexed position: an open magnetic resonance imaging analysis. Orthop Traumatol Surg Research: OTSR. 2018;104(4):485–9.
Beattie KA, Duryea J, Pui M, O’Neill J, Boulos P, Webber CE, Eckstein F, Adachi JD. Minimum joint space width and tibial cartilage morphology in the knees of healthy individuals: a cross-sectional study. BMC Musculoskelet Disord. 2008;9:119.
Ahn JH, Jeong HJ, Lee YS, Park JH, Lee JW, Park JH, Ko TS. Comparison between conservative treatment and arthroscopic pull-out repair of the medial meniscus root tear and analysis of prognostic factors for the determination of repair indication. Arch Orthop Trauma Surg. 2015;135(9):1265–76.
Chung KS, Ha JK, Ra HJ, Kim JG. A meta-analysis of clinical and radiographic outcomes of posterior horn medial meniscus root repairs. Knee Surg Sports Traumatol Arthroscopy: Official J ESSKA. 2016;24(5):1455–68.
Krych AJ, Reardon PJ, Johnson NR, Mohan R, Peter L, Levy BA, Stuart MJ. Non-operative management of medial meniscus posterior horn root tears is associated with worsening arthritis and poor clinical outcome at 5-year follow-up. Knee Surg Sports Traumatol Arthroscopy: Official J ESSKA. 2017;25(2):383–9.
Kwak YH, Lee S, Lee MC, Han HS. Large meniscus extrusion ratio is a poor prognostic factor of conservative treatment for medial meniscus posterior root tear. Knee surgery, sports traumatology, arthroscopy: official journal of the ESSKA 2018, 26(3):781–786.
Acknowledgements
The authors would like to thank Enago for the English language review.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conceptualization: HO and HI. Data curation: HO and Sho.Y. Formal analysis: HO. Investigation: HO and Sho.Y. Methodology: SF. Project administration: HI. Resources: TO. Software: Shi.Y. Supervision: YK. Validation: SF. Visualization: SF. Writing – original draft: HO and KN. Writing – review & editing: HI and KN.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study adhered to the tenets of the Declaration of Helsinki and was approved by the ethics committee of Nihon Koukan Hospital (no. 202317). The need of informed consent was waived by the ethics committee Nihon Koukan Hospital because this was a retrospective study using medical records.
Consent for publication
Informed consent for the publication of radiographic images was obtained from the participants.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Okamura, H., Ishikawa, H., Ohno, T. et al. Evaluation of the usefulness of non-weight-bearing tunnel view using X-ray in the short term after medial meniscus posterior root tear onset: a retrospective study. BMC Musculoskelet Disord 25, 628 (2024). https://doi.org/10.1186/s12891-024-07751-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07751-0