
Abstract
Background
Persistent or recurrent neck pain is associated with perturbations in the autonomic nervous system balance, and nociceptive stimulation has been seen to influence this balance. However, very few prospective studies have addressed the extent to which changes in pain associate with changes in autonomic cardiac regulation. Therefore, we investigated if changes in pain vary with changes in heart rate variability in a cohort of patients treated for persistent or recurrent neck pain.
Method
This analysis is based on data from a randomized controlled trial in which participants were given home stretching exercises with or without spinal manipulative therapy for two weeks. As the effectiveness of the intervention (home stretching exercises and spinal manipulative therapy) was found to be equal to the control (home stretching exercises alone), all 127 participants were studied as one cohort in this analysis. During the intervention, pain levels were recorded using daily text messages, and heart rate variability was measured in the clinics three times over two weeks. Two approaches were used to classify patients based on changes in pain intensity: 1) Clinically important changes in pain were categorized as either "improved" or "not improved" and, 2) Pain development was measured using pain trajectories, constructed in a data driven approach. The association of pain categories and trajectories with changes in heart rate variability indices over time were then analysed using linear mixed models.
Results
Heart rate variability did not differ significantly between improved and not-improved patients, nor were there any associations with the different pain trajectories.
Conclusions
In conclusion, changes in pain after home stretching exercises with or without spinal manipulative therapy over two weeks were not significantly associated with changes in heart rate variability for patients with persistent or recurrent neck pain. Future studies should rely on more frequent measurements of HRV during longer treatment periods.
Trial registration
The trial was registered at ClinicalTrials.gov, registration number: NCT03576846.
Similar content being viewed by others


Background
Chronic musculoskeletal pain-conditions, including persistent or recurrent neck pain (NP), are associated with altered sympathetic and parasympathetic activity of the autonomic nervous system (ANS) [1,2,3], commonly measured with heart rate variability (HRV) [4]. HRV is regarded as a biomarker for ANS dysregulation (as an indicator of autonomic cardiac modulation), and a low HRV has been associated with a range of poor health outcomes, such as cardiovascular disease, diabetes, mood disorders, and increased mortality [1, 5].
NP is a common reason to seek care [6] and current guidelines [7, 8] recommend a range of treatment options, including spinal manipulative therapy (SMT), defined as mobilization or manipulation of the spinal joints [9]. SMT alone or in combination with other approaches has been shown to reduce pain in both the short [10, 11] and the long term [12] in patients with NP. Stretching exercises alone or in combination with other treatments are also known to reduce musculoskeletal pain [7, 11, 13].
The mechanisms behind the pain-reducing effect of SMT and stretching are not clear. Thus, there are no objective biomarkers of treatment response. Different mechanisms have been suggested [14, 15], and it has been hypothesized that part of the pain-reducing effects is due to how the treatment influences the ANS balance [14,15,16]. A recent overview of systematic reviews have suggested that acute, short-term sympathetic upregulation can be observed with SMT [17] which has also been suggested with stretching exercises [18,19,20,21,22]. Further, a pain-reducing effect has been observed in a study of patients with persistent or recurrent NP treated with breathing exercises intended to normalize HRV. As improvements in both HRV and pain were observed [23], it suggests that it might be altered ANS balance as indicated by HRV per se that influences the pain, regardless of the type of treatment. In other words, changes in ANS balance following treatment precedes changes in pain perception. However, the proposed mechanism of SMT as having an acute positive effect on the ANS balance is questionable [17], and was challenged in two recent systematic reviews, which concluded that the evidence in favour of such a link was of low or very low quality [24, 25]. Also, a recently published randomized trial investigating acute effects of SMT on HRV using a successful sham treatment found no evidence of such an effect over placebo [26].
The long-term effects of manual therapy on HRV have not been rigorously investigated, but we recently conducted a trial and found no difference in HRV over two weeks between groups receiving SMT and home stretching exercises vs home stretching exercises alone [27].
Considering the fact that experimentally induced pain alters the patients' HRV [28], the mechanism in a clinical setting could perhaps be conceived as working in the opposite direction. In other words, changes in pain are causing the observed HRV changes.
Although our previous research found no significant group difference effect on pain [29] and HRV [27], large variability in both outcomes was found between patients across intervention groups. For example, the root mean squared successive differences (RMSSD) between normal heartbeats (the a primary outcome of HRV) showed both decreases and increases during the intervention period, with confidence intervals ranging from -3.23 ms to 0.28 ms [27], and the proportion of participants reaching a Minimal Clinically Important Difference (MCID) in pain intensity was 46/123 across intervention groups. It was important to explore whether changes in pain varied with changes in HRV in the intervention period as evidence of such an association could shed light on this relationship in a clinical setting and inform the use of HRV as an objective marker of treatment response.
Two strategies were employed to investigate changes in pain during the two-week treatment period. First, patients were categorized based on MCID in pain intensity. Then, patients were classified into detailed pain trajectories in a data driven approach. The two strategies complemented each other; both the actual difference in pain intensity from baseline to the end of the intervention period, and different pain developments throughout the intervention period, were explored.
As noted, an association between reduced HRV and persistent NP has been established. However, it is not known how HRV responds to changes in NP in a clinical setting.
The present study aimed to investigate the association between changes in pain intensity and changes in HRV in patients receiving treatment for NP. We hypothesized that patients experiencing a MCID improvement in pain intensity would show a beneficial increase in HRV over time, and that trajectories with consistent/fast improvement would show a beneficial increase in HRV compared to trajectories that were stable.
Method
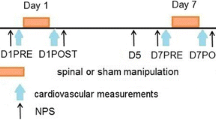
This study is a secondary analysis of data from a Swedish multicentre RCT [30]. The primary aim of the original RCT was to investigate the effect of a series of four treatments over two weeks of SMT plus home stretching exercises vs home stretching exercises alone on pain and HRV for patients with persistent or recurrent NP. The treatment effects on primary outcomes are reported in two previous publications [27, 29]. The study design, recruitment, randomization, and interventions have been described in detail in a published protocol [30] and are reported here in Additional file 1: Appendix A. The trial "The effect of spinal manipulative therapy on HRV and pain in patients with chronic neck pain: a randomized controlled trial " was registered at ClinicalTrials.gov, registration number: NCT03576846.
In the current analysis, we used all participants in the RCT, thus the study group consisted of 127 patients with persistent or recurrent NP residing in the Stockholm area. Participants were recruited through clinic advertisements and newsletters, public postings on the clinics' social media pages, and local newspapers. Patients seeking care at the clinics were also invited to participate. They had experienced persistent or recurrent NP for more than six months and must not have received chiropractic treatment during the previous six months. They had to be minimum 18 years of age and must be able to read and understand Swedish. This represents a relatively small proportion of chiropractic patients, as they more commonly seek care with low back pain and with a shorter duration of pain [31, 32].
Participants were excluded if they reported any of the following conditions: cardiovascular disease, hypertension, cancer, infection, acute cervical radiculopathy, dizziness, previous drop-attacks, or diabetes. They were also excluded if taking any of the following medications: Steroids, β-blockers, or antidepressants. Further, pregnancy, BMI above 30, or recent experience of severe trauma led to exclusion.
During the two-week intervention, clinical pain was measured daily, and HRV was measured on three separate occasions. Participants were categorised in relation to changes in pain using two strategies:
-
1.
On the basis of MCID in pain intensity, measured with 11-point Numeric Rating Scale (NRS-11), participants were categorized as "improved" (reduction ≥ 2/10 from the first measurement to the last) or "not improved" (no change or worsened, change ≤ 0/10)). This approach excluded patients experiencing only small, non-clinically significant clinical improvements from further analysis, ensuring a distinct difference in treatment response between the two categories.
-
2.
Four NP trajectories were identified based on daily text-message reports of pain intensity (NRS-11) during the two-week study period. A latent class analysis was used, and the pain trajectories were estimated with a linear regression model (for trajectories three and four), with a quadratic model (for trajectory one), and a fourth-order model (for trajectory two). The process of choosing the order of the models for the different trajectories was iterative, starting from the simplest (intercept only) model for all trajectories and adding complexity as long as the coefficients remained significant at the 0.05 level. Ordinary regression was chosen as the estimation method, in line with previous analysis [27, 29]. We chose the four-trajectories solution based on AIC (Akaike Information Criteria) and previous research [33]. Also, we achieved relatively detailed trajectories. Models with two or three trajectories were also explored but found to have no advantages over the four-trajectories model. The trajectories were labelled 1–4, based on their pain intensity. Trajectory 1 was chosen as the reference category as it represented the trajectory with the lowest level of pain and was chosen before trajectory 4 (highest level of pain) as it had a higher number of patients (Fig. 1).

Pain trajectories based on group-based trajectory models [34]. Pain is measured with NRS-11 (0–10) at baseline and each day for two weeks. Numbers in the box show the proportion of study patients belonging to each trajectory
Variables
The participants answered questionnaires covering the suggested domains in the International Classification of Functioning, Disability, and Health (ICF) [35] by measuring impairments, function (limitations), and restrictions to participating in activities. The questionnaires utilized were the Neck Disability Index (NDI) [36], the McGill Questionnaire [37, 38], and the Euroqol-5 dimensions (EQ-5D). In addition, the StarTBack tool [39] and attitudes towards participating were used as a baseline measurement.
Independent variable
Pain intensity was measured as a self-reported NRS-11 value, ranging from 0 ('No pain') to 10 ('Worst pain imaginable'). NRS-11 is a validated measure of pain intensity [40, 41] and was chosen due to the observed association between pain and HRV in previous studies [1, 2]. Pain intensity was measured at baseline and each day for two weeks (the intervention period) using daily text messages [42].
Dependent variable
HRV is a measure of the variability in time latency between heartbeats [43]. It is known to quickly adapt to changing circumstances [43] and is recognized as a reliable [44] measure of the function of the ANS, where a high HRV index indicates a well-functioning, responsive ANS and vice versa [1]. HRV was measured at baseline, one week and two weeks during the intervention using FirstBeat, a small, portable device attached to the chest measuring Electrocardiography (ECG). The participants were instructed to avoid caffeine, alcohol, tobacco, and strenuous exercise the same day as the measurements. The measurements were done prior to the interventions, to prevent any direct influence of treatment on HRV. The measurements were performed with the patient seated in a chair, wearing hearing protection, facing the wall, instructed to breath normally during this time. Efforts were also made to keep temperature and lighting in the room at the same level at each measurement. The measurement was undertaken during a normal working day (between the hours of 0700–1600). A five-minute relaxation period was used before HRV was obtained as resting HRV the following five minutes.
Data were extracted from the ECG recordings as time intervals between successive ECG R-waves (R-R intervals). Five minutes segments were used when analysing HRV indices in both time and frequency domains.
The HRV data were cleaned for artifacts and ectopic beats (i.e., common changes in a heartbeat involving an extra or skipped heartbeat) to ensure sufficient quality. The R-R intervals were visually inspected using Kubios software [45]. If the data had insufficient quality, different sensitivity filters, ranging from 0.45 to 0.05 s differing from the local average, were utilized to remove artifacts. If the proportion of excluded artifacts exceeded 5% when the data gained sufficient visual quality, the sample was excluded [46].
The Taskforce of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology [47] has developed standards of measurements of HRV, which were used with adaptations in this study. We did not include Low Frequency (LF) power and the LF/HF ratio as their physiological interpretation is unclear [48,49,50]. HRV measurements include various indices, measuring different parts of the ANS. These are summarized in Table 1.
Ethics
The study was conducted in accordance with the Helsinki declaration [51]. The Ethical Review Board (Stockholm) approved this study: 2018/2137–31. All participants signed a written informed consent form.
Ethical considerations informed the decision to use a two-week intervention period, as four treatments were not considered burdensome if no improvement was observed.
Statistical analysis
Missing data
For NRS-11, Last Observation Carried Forward (LOCF) was used. HRV measurements only had a total of 11.8% missing data due to dropouts, missed appointments and cleaning of data. As the longitudinal modelling strategy used every available datapoint in an efficient way, it was not considered necessary to impute data.
Changes in pain and the association with changes in heart rate variability
Initially, participants were categorized based on the two strategies 1) MCID pain improvement and 2) Pain trajectories, as described above. To explore associations between changes in pain (both strategies) and changes in HRV, a series of linear mixed regression models was employed, using each HRV index as the outcome, including a person specific random intercept. The models included the pain groups (improved vs not improved or trajectories), time (baseline, 1 week, and follow-up), and the interaction between pain group and time. The estimate (β) of the interaction effect is interpreted as the difference between groups in the change in HRV (i.e. slope) between each time point. A significant interaction would indicate that the pain groups differ in the change in HRV over time.
An analysis adjusted for age, sex, baseline pain, and type of intervention was performed as a sensitivity analysis.
We estimated β with 95% CIs and p-values < 0.05 were considered statistically significant. Due to multiple testing, adjusting the significance level was considered. As power is already low in a secondary analysis, such adjustments would further reduce power and were considered not to benefit the understanding of the results and not to be critical in an exploratory analysis like this [52].
Continuous variables were reported as means with standard deviations and categorical variables as counts and percentages.
Group differences were graphically presented using box plots.
The analysis was performed using SPSS 27 [53] and Stata version 15 (StataCorp. 2017). The trajectory models were estimated with Stata package traj [34].
Results
Participants
Overall, the study group consisted of slightly more female than male participants with a mean age of 56 years, and most had suffered pain for several years. Most of the participants were living in a partnership. Most also experienced pain in other regions of the body. In general, they had experienced good effect from chiropractic treatment in the past and the mean score of the expectation to improve (0–10) was 5.9. Six-point seven percent of the data were excluded due to measurement errors based on visual inspection.
MCID pain improvement
Data from 88 patients were used as those with a non-clinically significant improvement (1-point improvement) (n = 39) were excluded from this analysis. The two pain categories (clinically improved vs not improved) differed in baseline pain intensity (NRS-11), with a mean of 5.5 (SD = 1.7) for the "improved" category and of 3.6 (SD = 2.3) for the "not improved" category. There were no differences in mean age and sex distribution between the categories (p > 0.05). The "improved" category (mean change in pain intensity -3.2 (SD 1.1)) also showed improvement in the disability (NDI) and qualitative characteristics of pain (McGill Questionnaire) compared to the "not improved" category. Further, the "improved" category reported less sick leave; two participants (5%) had been on sick leave due to NP the previous year, compared to six (14%) of the "not improved" category. Also, a slightly larger proportion of participants were classified in the medium or high STarT Back risk group (indicating a higher risk for future physical disability) in the "not-improved" category [39]. A higher number of participants with mid-back or low back pain was reported among the individuals in this category compared to the "improved" as seen in Table 2. The baseline differences in HRV between categories are presented in Supplementary File 1, where no significant baseline differences were observed.
The mean change for RMSSD in both categories is presented in (Fig. 2). The HRV indices are presented in Supplementary files 2, 3, 4 and 5.

Mean change in RMSSD in the improved and not-improved categories
For the main HRV outcome RMSSD, a β-coefficient of the group-time interaction of 1.8 (CI = -2.2–5.7, p-value = 0.37) with the "not improved" category as the reference category was seen, meaning that the "improved" category showed an increased RMSSD of 1.8 units for each time point compared with the "not improved" category. All HRV indices are in favour of the "improved" category with small effect sizes, but estimates were not significant.
No significant changes between "improved" and "not-improved" categories were found for any of the HRV indices as seen in Table 3.
Adjustments for age, sex, baseline pain, and intervention did not affect our estimates. These results can be found in Supplementary File 6.
Pain trajectories
All participants from the RCT were included in the analysis (n = 127). As can be seen in (Fig. 1), a relatively stable pain course for all trajectories was observed from baseline to 14 days; the difference was mainly in pain intensity. Thus, there were no trajectories with a clear improvement or deterioration in pain over time. Overall, trajectory 1 had low levels of pain throughout the study, in contrast with trajectory 4, which had high levels of pain throughout. Trajectory 4 had a slight worsening in pain intensity over two weeks, while the other trajectories improved somewhat. The differences in the demographics of the trajectories are described in Table 4.
In short, there were more females in trajectory 4 (75% compared to 48–59% in the other trajectories) and these individuals were generally "worse", as 73% of the individuals in trajectory 4 had a STarT Back risk of medium or high (compared to the second-highest STarT Back risk group (trajectory 3) with 28% of individuals classified as medium or high risk), and half of the patients in trajectory 4 had been on sick leave the previous year (compared to below 11% of patients in all other trajectories).
Patients in trajectory 1 had a lower prevalence of pain in the arms, mid-back, or lower back compared to patients in the other trajectories and improved 3.9 points in the NDI, compared to the patients in the other trajectories who also improved, but only by 1.7 to 2.4.
In terms of the intervention and control groups in the RCT, patients were not evenly distributed among the trajectories. However, previous analyses on the same data set showed no significant differences between these groups for HRV and pain [27, 29]. No significant baseline differences in HRV between the trajectory groups were observed, (Supplementary File 7).
The mean change for RMSSD in all trajectories is presented in (Fig. 3). The rest of the HRV indices are presented in Supplementary Files 8, 9, 10 and 11.

Mean change in RMSSD for the four pain trajectories
The main HRV outcome, RMSSD, was not significantly different between trajectories 2–4 and 1, but a somewhat larger decrease in RMSSD over time was seen in trajectory 4, demonstrated by a β-coefficient of the group-time interaction of -3.8 (CI = -10.4 – 4.3, p = 0.26). The same non-significant estimates with a more substantial reduction on HRV with higher pain intensity was found for all HRV indices. The results are presented in Table 5 (linear mixed models).
Adjusting for age, sex, baseline pain, and intervention did not significantly affect the estimates (Supplementary File 12).
Discussion
The current study is an exploratory analysis of data from a RCT in which data from the randomization groups have been pooled, as no significant between-group differences were observed. We hypothesized that MCID in pain intensity would be associated with changes in HRV, but only small and statistically insignificant differences in HRV change were observed between patients with/without clinical improvement in pain intensity (NRS-11). Small and not statistically significant differences were also observed for HRV indices in individuals with different pain trajectories. However, due to the stability of the observed trajectories, the hypothesis that trajectories with consistent/fast improvement would show a beneficial increase in HRV compared to trajectories that were stable, could not be rejected or confirmed.
The study investigated patients with persistent or recurrent NP, a typically fluctuating condition [54,55,56,57]. The changes in pain during the course of treatment, which were the basis for the dichotomization into "improved" and "not improved", could have been due to normal fluctuations in pain and not a reflection of important clinical improvements as intended. We sought to minimize this random fluctuation by ignoring minor pain changes. Further, there was a difference in baseline pain between individuals who improved compared to those who did not. The base for the categorization of "improved" and "not improved" made it more likely for the patients with high initial pain scores to reach a pain reduction of 2/10 or more (flooring effect). Possibly, more patients would have reached this level if an inclusion criterion in the study was pain intensity of a certain (higher) level at baseline. Also, overall higher pain levels in this category may have had a stronger impact on HRV already at baseline. However, adjusting for baseline differences in pain intensity did not change the conclusion of this study.
Classifying different trajectories of pain during an intervention period is a way of investigating pain development during a given time period, used in previous studies in patients with NP in a clinical setting [57]. The identified pain trajectories had very different baseline pain intensities. This reflects the inclusion of participants with varying pain levels, as expected in the condition under investigation. However, the trajectories were all stable over time, which could not have been foreseen. The non-significant deterioration in HRV found in the trajectory with high pain intensity (trajectory 4) can be due to a relationship between persistent pain and HRV, possibly causing patients classified in this trajectory to be less susceptible to improvement. Certainly, the patients in this trajectory had several other known factors associated with poor outcomes.
It is possible that four treatments over two weeks were not enough to obtain pain relief sufficient to influence HRV in patients with chronic pain. The intervention period was chosen based on previous research on HRV and SMT which focuses on the immediate effects of manual therapy on HRV [24, 25, 58,59,60,61]. Four treatments over two weeks was considered sufficient to detect a change in pain based on previous research, which found that improvement after four treatments predicts improvement in persistent low back pain after three and twelve months [62]. In the study by Leboeuf-Yde et al. [62], it was also noted that a lack of an early treatment response was not remedied during the rest of the treatment programme. By delivering four treatments for persistent or recurrent NP, we therefore expected to identify responders to care. It is possible that NP sufferers differ from the persistent low back pain sufferers in response to treatment, but this is not supported by the literature [63]. It is even observable that low back pain sufferers are equally or more affected with regards to emotional situation and disability level, and often have longer pain duration than NP sufferers [64]. As reported in Table 2, most individuals also experienced pain in other body regions, and a lack of association between changes in NP and HRV may be partly explained by concomitant pain.
Treatment content was collected for, and all treatment modalities were in line with what has been reported in other studies [65,66,67]. The stretching exercises used were described in a previous study [11], but also found to be commonly used. The photographs used to illustrate the exercises were found on a Swedish chiropractic website (and used with permission). Thus, we believe that the interventions used are relevant for manual professions.
The results did not appear to support the proposed mechanism that changes in pain lead to changes in ANS. It is possible that any changes in HRV following pain relief have a latency extending beyond the two weeks observed in the current study, which is supported by previous research where a reduction of NP has been observed when patients received treatment aimed at improving HRV over ten weeks [23]. It is also possible that any mechanistic interrelatedness of pain and ANS balance is simply obscured by the multitude of other factors affecting one, the other, or both. Further, there were several limitations related to HRV measurement that may have influenced results, such as lack of 24-h assessment of HRV and few measurements over time, which may have yielded more stable measures of resting HRV.
The reliability of the 5-min HRV measurement of parasympathetic indices at rest, is, however, considered good [44].
Different strategies were used to reduce the risk of selection and attention bias, as described in Additional file 1: Appendix A and previously published articles [27, 29]. Any inter-relatedness of NP and HRV is possibly more complicated and confounding factors may exist which we are not aware of. The patients' internal factors such as emotions, unknown underlying diseases and stress influencing HRV [4, 68,69,70] could not be controlled for. Participation in the study may have led to more daily stress as time had to be set aside to participate. The initial study design also included a conditioned pain modulation test, where the hand was submerged in cold water. This was done after the HRV measurements to avoid any effect of the test on HRV, but it is possible that the anticipation of the uncomfortable test influenced HRV. The effect of these confounding factors would potentially reduce the observed association between reduction in pain and change in HRV over two weeks. This was addressed by applying a strict measuring protocol.
Methodological considerations
The measurement procedures were standardized and well-controlled, with two trained researchers performing all HRV measurements. The study utilized repeated measures of all outcomes. Two different strategies to classify pain over two weeks were used in order to investigate this relationship in a thorough manner. This is the first study of its kind investigating the relationship between changes in pain and changes in HRV during a two-week treatment intervention for this population.
As this is an exploratory analysis based on data from a trial with a power calculation for logarithmic values with larger group sizes [27], the analysis undertaken with smaller group sizes was underpowered. Therefore, caution is warranted when interpreting the estimates.
HRV is prone to measurement error. About 40% of the variance in HRV is known to be explained by situational effects and person-situation interaction [44]. It is also acknowledged that the HRV measurements are prone to be affected by factors such as psychological distress, training status, and time of the day the day measurements are taken, which are not possible to control for. HRV varies from day to day for each individual as well as between individuals, one measure each day at three occasions may have rendered uncertain results and may have reduced power further. [71, 72]. Considering the original RCT design of the study, measuring each patient’s individual HRV values over time, before the intervention period commenced, was not possible. If this had been possible, investigating whether the patients HRV changes from their “normal” would yield stronger certainty in the results.
Generalizability
Participants were mainly excluded from the main trial due to factors, conditions or medications known to influence HRV-measurements. These included medications such as antidepressants. Thus, the study participants may have been physically and psychologically healthy compared to the general population with persistent or recurrent NP. However, there is evidence that patients with pain and depression undergoing medical treatment for depression experience reduced pain and improved daily function [73, 74]. Hence, the excluded patients may not have differed in their pain response from other persistent or recurrent NP sufferers. The results in this study may be considered generalizable for chronic pain conditions based on previous research investigating chronic pain and HRV [1,2,3], even though strong conclusions cannot be drawn from the results in this study as the observed associations are weak and uncertain.
Conclusion
Changes in pain intensity during an intervention with SMT and/or home stretching exercises over two weeks was not significantly associated with changes in HRV for this study population with persistent or recurrent NP. The results do not favour the link between pain and HRV in this patient group. Future studies should rely on more frequent measurements of HRV during longer treatment periods.
Availability of data and materials
The data that support the findings of this study were used under license for the current study. Restrictions apply to the availability of these data, hence they are not publicly available. Data can, however, be obtained from the authors upon reasonable request to the main author (AGB), and with permission of Karolinska Institutet.
Abbreviations
- AIC:
-
Akaike Information Criteria
- ANS:
-
Autonomic Nervous System
- ECG:
-
Electrocardiography
- HRV:
-
Heart Rate Variability
- ICF:
-
International Classification of Functioning, Disability, and Health
- LOCF:
-
Last Observation Carried Forward
- MCID:
-
Minimal Clinical Important Difference
- NDI:
-
Neck Disability Index
- NP:
-
Neck Pain
- NRS-11:
-
11-Point Numeric Rating Scale
- RMSSD:
-
Root Mean Squared Successive Differences
- SMT:
-
Spinal Manipulative Therapy
References
Tracy LM, Ioannou L, Baker KS, Gibson SJ, Georgiou-Karistianis N, Giummarra MJ. Meta-analytic evidence for decreased heart rate variability in chronic pain implicating parasympathetic nervous system dysregulation. 2016;157(1):7–29.
andeira PM, Reis FJJ, Sequeira VCC, Chaves ACS, Fernandes O, Arruda-Sanchez T. Heart rate variability in patients with low back pain: a systematic review. Scand J Pain. 2021;21(3):426–33.
Santos-de-Araújo AD, Dibai-Filho AV, dos Santos SN, de AlcântaraEV,SouzaCdS, Gomes CAFdP, et al. Correlation Between Chronic Neck Pain and Heart Rate Variability Indices at Rest: A Cross-sectional Study. J Manipulative Physiol Ther. 2019;42(4):219–26.
Zhu J, Ji L, Liu C. Heart rate variability monitoring for emotion and disorders of emotion. Physiol Meas. 2019;40(6):064004.
Buijs RM, Swaab DF, Aminoff MJ, Boller PF, Swaab DF. Autonomic Nervous System : Handbook of Clinical Neurology (Series editors: Aminoff, Boller, Swaab). Oxford, NETHERLANDS, THE: Elsevier; 2013.
Beliveau PJH, Wong JJ, Sutton DA, Simon NB, Bussières AE, Mior SA, et al. The chiropractic profession: a scoping review of utilization rates, reasons for seeking care, patient profiles, and care provided. Chir Man Ther. 2017;25:35.
Bryans R, Decina P, Descarreaux M, Duranleau M, Marcoux H, Potter B, et al. Evidence-Based Guidelines for the Chiropractic Treatment of Adults With Neck Pain. J Manipulative Physiol Ther. 2014;37(1):42–63.
Corp N, Mansell G, Stynes S, Wynne-Jones G, Morsø L, Hill JC, et al. Evidence-based treatment recommendations for neck and low back pain across Europe: A systematic review of guidelines. Eur J Pain. 2021;25(2):275–95.
Hidalgo B, Hall T, Bossert J, Dugeny A, Cagnie B, Pitance L. The efficacy of manual therapy and exercise for treating non-specific neck pain: A systematic review. J Back Musculoskelet Rehabil. 2017;30(6):1149–69.
Häkkinen A, Salo P, Tarvainen U, Wirén K, Ylinen J. Effect of manual therapy and stretching on neck muscle strength and mobility in chronic neck pain. J Rehabil Med. 2007;39(7):575–9.
Ylinen J, Kautiainen H, Wiren K, Hakkinen A. Stretching exercises vs manual therapy in treatment of chronic neck pain: a randomized, controlled cross-over trial. J Rehabil Med. 2007;39(2):126–32.
Maiers M, Bronfort G, Evans R, Hartvigsen J, Svendsen K, Bracha Y, et al. Spinal manipulative therapy and exercise for seniors with chronic neck pain. Spine J. 2014;14(9):1879–89.
de Zoete RM, Armfield NR, McAuley JH, Chen K, Sterling M. Comparative effectiveness of physical exercise interventions for chronic non-specific neck pain: a systematic review with network meta-analysis of 40 randomised controlled trials. Br J Sports Med. 2020.
Behm D, Kay A, Trajano G, Alizadeh S, Blazevich A. Effects of Acute and Chronic Stretching on Pain Control. J Clin Exerc Physiol. 2021;10:150–9.
Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009;14(5):531–8.
Bialosky JE, Beneciuk JM, Bishop MD, Coronado RA, Penza CW, Simon CB, et al. Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. J Orthop Sports Phys Ther. 2018;48(1):8–18.
Roura S, Álvarez G, Solà I, Cerritelli F. Do manual therapies have a specific autonomic effect? An overview of systematic reviews. PLoS ONE. 2021;16(12):e0260642.
Inami T, Shimizu T, Baba R, Nakagaki A. Acute Changes in Autonomic Nerve Activity during Passive Static Stretching. American J Sports Sci and Med. 2014;2:166–70.
Wong A, Figueroa A. Effects of Acute Stretching Exercise and Training on Heart Rate Variability: A Review. 2021;35(5):1459–66.
Farinatti PT, Brandão C, Soares PP, Duarte AF. Acute effects of stretching exercise on the heart rate variability in subjects with low flexibility levels. J Strength Cond Res. 2011;25(6):1579–85.
Mueck-Weymann M, Janshoff G, Mueck H. Stretching increases heart rate variability in healthy athletes complaining about limited muscular flexibility. Clin Auton Res. 2004;14(1):15–8.
Saito T, Hono T, Miyachi M. Effects of stretching on cerebrocortical and autonomic nervous system activities and systemic circulation. J Phys Med. 2001;2001(12):2–9.
Hallman DM, Olsson EMG, von Schéele B, Melin L, Lyskov E. Effects of Heart Rate Variability Biofeedback in Subjects with Stress-Related Chronic Neck Pain: A Pilot Study. Appl Psychophysiol Biofeedback. 2011;36(2):71–80.
Picchiottino M, Leboeuf-Yde C, Gagey O, Hallman DM. The acute effects of joint manipulative techniques on markers of autonomic nervous system activity: a systematic review and meta-analysis of randomized sham-controlled trials. Chiropr Manual Ther. 2019;27:17.
Araujo FX, Ferreira GE, Angellos RF, Stieven FF, Plentz RDM, Silva MF. Autonomic Effects of Spinal Manipulative Therapy: Systematic Review of Randomized Controlled Trials. J Manipulative Physiol Ther. 2019;42(8):623–34.
Picchiottino M, Honoré M, Leboeuf-Yde C, Gagey O, Cottin F, Hallman DM. The effect of a single spinal manipulation on cardiovascular autonomic activity and the relationship to pressure pain threshold: a randomized, cross-over, sham-controlled trial. Chiropr Man ther. 2020;28(1):7.
Galaasen Bakken A, Eklund A, Hallman DM, Axén I. The effect of spinal manipulative therapy and home stretching exercises on heart rate variability in patients with persistent or recurrent neck pain: a randomized controlled trial. Chiropr ManTher. 2021;29(1):48.
Forte G, Troisi G, Pazzaglia M, Pascalis V, Casagrande M. Heart Rate Variability and Pain: A Systematic Review. Brain Sci. 2022;12(2).
Bakken AG, Eklund A, Warnqvist A, O’Neill S, Axén I. The effect of two weeks of spinal manipulative therapy and home stretching exercises on pain and disability in patients with persistent or recurrent neck pain; a randomized controlled trial. BMC Musculoskelet Disord. 2021;22(1):903.
Galaasen Bakken A, Axén I, Eklund A, O’Neill S. The effect of spinal manipulative therapy on heart rate variability and pain in patients with chronic neck pain: a randomized controlled trial. Trials. 2019;20(1):590.
Hartvigsen J, Sorensen LP, Graesborg K, Grunnet-Nilsson N. Chiropractic patients in Denmark: A short description of basic characteristics. J Manipulative Physiol Ther. 2002;25(3):162–7.
Rubinstein S, Pfeifle CE, van Tulder MW, Assendelft WJJ. Chiropractic patients in the Netherlands: A descriptive study. J Manipulative Physiol Ther. 2000;23(8):557–63.
Kongsted A, Kent P, Axen I, Downie AS, Dunn KM. What have we learned from ten years of trajectory research in low back pain? BMC Musculoskelet Disord. 2016;17(1):220.
Jones BL. Nagin DSJSM, Research. A note on a Stata plugin for estimating group-based trajectory models. 2013;42(4):608–13.
Threats TT. Towards an international framework for communication disorders: Use of the ICF. J Commun Disord. 2006;39(4):251–65.
Ackelman BH, Lindgren U. Validity and reliability of a modified version of the neck disability index. J Rehabil Med. 2002;34(6):284–7.
Dworkin RH, Turk DC, Trudeau JJ, Benson C, Biondi DM, Katz NP, et al. Validation of the Short-form McGill Pain Questionnaire-2 (SF-MPQ-2) in acute low back pain. J Pain. 2015;16(4):357–66.
Burckhardt CS, Bjelle A. A Swedish version of the short-form McGill Pain Questionnaire. Scand J Rheumatol. 1994;23(2):77–81.
Hill JC, Afolabi EK, Lewis M, Dunn KM, Roddy E, van der Windt DA, et al. Does a modified STarT Back Tool predict outcome with a broader group of musculoskeletal patients than back pain? A secondary analysis of cohort data. BMJ Open. 2016;6(10):e012445.
Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005;14(7):798–804.
Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain. 1986;27(1):117–26.
SMS-track [Available from: https://www.sms-track.com.
Rajendra Acharya U, Paul Joseph K, Kannathal N, Lim CM, Suri JS. Heart rate variability: a review. Med Biol Eng Compu. 2006;44(12):1031–51.
Bertsch K, Hagemann D, Naumann E, Schachinger H, Schulz A. Stability of heart rate variability indices reflecting parasympathetic activity. Psychophysiology. 2012;49(5):672–82.
Kubios [Available from: https://www.kubios.com/.
Hallman DM, Sato T, Kristiansen J, Gupta N, Skotte J, Holtermann A. Prolonged Sitting is Associated with Attenuated Heart Rate Variability during Sleep in Blue-Collar Workers. Int J Environ Res Public Health. 2015;12(11):14811–27.
Heart rate variability. standards of measurement, physiological interpretation and clinical use Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation. 1996;93(5):1043–65.
Heathers JA. Everything Hertz: methodological issues in short-term frequency-domain HRV. Front Physiol. 2014;5:177.
Goldstein DS, Bentho O, Park MY, Sharabi Y. Low-frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp Physiol. 2011;96(12):1255–61.
Quintana DS, Alvares GA, Heathers JA. Guidelines for Reporting Articles on Psychiatry and Heart rate variability (GRAPH): recommendations to advance research communication. Transl Psychiatry. 2016;6(5):e803.
Charlton E. Ethical guidelines for pain research in humans. Committee on Ethical Issues of the International Association for the Study of Pain. Pain. 1995;63(3):277–8.
Althouse AD. Adjust for Multiple Comparisons? It’s Not That Simple. Ann Thorac Surg. 2016;101(5):1644–5.
SPSS [Available from: https://www.ibm.com/products/spss-statistics.
Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333.
Axén I, Leboeuf-Yde C. Trajectories of low back pain. Best Pract Res Clin Rheumatol. 2013;27(5):601–12.
Raffaeli WTM, Corraro A, Malafoglia V, Ilari S, Balzani E, Bonci A. Chronic Pain: What Does It Mean? A Review on the Use of the Term Chronic Pain in Clinical Practice. J Pain Res. 2021;14:827–35.
Irgens P, Kongsted A, Myhrvold BL, Waagan K, Engebretsen KB, Natvig B, et al. Neck pain patterns and subgrouping based on weekly SMS-derived trajectories. BMC Musculoskelet Disord. 2020;21(1):678.
Chu J, Allen DD, Pawlowsky S, Smoot B. Peripheral response to cervical or thoracic spinal manual therapy: an evidence-based review with meta analysis. J Man Manip Ther. 2014;22(4):220–9.
Kingston L, Claydon L, Tumilty S. The effects of spinal mobilizations on the sympathetic nervous system: A systematic review. Man Ther. 2014;19(4):281–7.
Wirth B, Gassner A, de Bruin ED, Axen I, Swanenburg J, Humphreys BK, et al. Neurophysiological Effects of High Velocity and Low Amplitude Spinal Manipulation in Symptomatic and Asymptomatic Humans: A Systematic Literature Review. Spine (Phila Pa 1976). 2019;44(15):E914-e26.
Amoroso Borges BL, Bortolazzo GL, Neto HP. Effects of spinal manipulation and myofascial techniques on heart rate variability: A systematic review. J Bodyw Mov Ther. 2018;22(1):203–8.
Leboeuf-Yde C, Grønstvedt A, Borge JA, Lothe J, Magnesen E, Nilsson Ø, et al. The nordic back pain subpopulation program: demographic and clinical predictors for outcome in patients receiving chiropractic treatment for persistent low back pain. J Manipulative Physiol Ther. 2004;27(8):493–502.
Buchner M, Zahlten-Hinguranage A, Schiltenwolf M, Neubauer E. Therapy outcome after multidisciplinary treatment for chronic neck and chronic low back pain: a prospective clinical study in 365 patients. Scand J Rheumatol. 2006;35(5):363–7.
Altuğ F, Kavlak E, Kurtca MP, Ünal A, Cavlak U. Comparison of pain intensity, emotional status and disability level in patients with chronic neck and low back pain. J Back Musculoskelet Rehabil. 2015;28(3):505–8.
Kvammen OC, Leboeuf-Yde C. The chiropractic profession in Norway 2011. Chiropr Man Ther. 2014;22(1):44.
Beliveau PJH, Wong JJ, Sutton DA, Simon NB, Bussières AE, Mior SA, et al. The chiropractic profession: a scoping review of utilization rates, reasons for seeking care, patient profiles, and care provided. Chiropr Man Ther. 2017;25(1):35.
Leboeuf-Yde C, Hennius B, Rudberg E, Leufvenmark P, Thunman M. Chiropractic in Sweden: a short description of patients and treatment. J Manipulative Physiol Ther. 1997;20(8):507–10.
Kim H-G, Cheon E-J, Bai D-S, Lee YH, Koo B-H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018;15(3):235–45.
ChuDuc H, NguyenPhan K, NguyenViet D. A Review of Heart Rate Variability and its Applications. APCBEE Proc. 2013;7:80–5.
Mostoufi SM, Afari N, Ahumada SM, Reis V, Wetherell JL. Health and distress predictors of heart rate variability in fibromyalgia and other forms of chronic pain. J Psychosom Res. 2012;72(1):39–44.
Buchheit M. Monitoring training status with HR measures: do all roads lead to Rome? Front Physiol. 2014;5:73.
Plews DJ, Laursen PB, Le Meur Y, Hausswirth C, Kilding AE, Buchheit M. Monitoring training with heart rate-variability: how much compliance is needed for valid assessment? Int J Sports Physiol Perform. 2014;9(5):783–90.
Teh CF, Zaslavsky AM, Reynolds CF 3rd, Cleary PD. Effect of depression treatment on chronic pain outcomes. Psychosom Med. 2010;72(1):61–7.
Lin CH, Yen YC, Chen MC, Chen CC. Relief of depression and pain improves daily functioning and quality of life in patients with major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2013;47:93–8.
https://etikprovningsmyndigheten.se/ [Available from: https://etikprovningsmyndigheten.se/.
Acknowledgements
The authors report no conflict of interest.
A special thanks to www.kiropraktorcentrum.com for the permission to use their photos in the exercise diary.
Thanks to Professor Charlotte Leboeuf-Yde for constructive comments.
Thanks to IKON – (Institute for Chiropractic and Neuromuscular Skeletal Research) for financial support for this article as part of the main author’s PhD project.
Restrictions apply to the availability of the data which were used under license for the current study, which is consequently not publicly available. Karolinska Institutet can make the data available to researchers upon reasonable request.
Funding
Open access funding provided by Karolinska Institute. Financial support to this article was provided by IKON – (Institute for Chiropractic and Neuromusculoskeletal Research). The funding body had no role in the design of the study, analysis or interpretation of data, or writing of the manuscript.
Author information
Authors and Affiliations
Contributions
AGB designed the study, performed the main statistical analysis, prepared tables and wrote the main manuscript. IA designed the study and assisted in the writing of the manuscript. AE assisted in designing the study and writing of the manuscript. SO and DH assisted in reviewing the manuscript. AW assisted in performing the statistical analysis, prepared figures, and reviewed the manuscript's statistics section. The author(s) read and approved the final manuscript.
Authors’ information
This article is the third of a series of three articles as part of AGBs' doctoral degree. The overall aim is to investigate the relationship between changes in pain and changes in HRV.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants signed an informed consent form. The study was approved by the Stockholm Regional Ethical Swedish Ethical Review Authority [75] (reference approval no. 2018/2137–31).The study was conducted in accordance with the Helsinki declaration [51].
Consent for publication
Informed consent for the use of the photos of home stretching exercises was obtained from the participant.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix A.
Details about the RCT.
Additional file 2: Appendix B.
Stretch exercises to perform daily for 14 days.
Additional file 3: Supplementary file 1.
Association between pain groups (based on clinically relevant change in pain intensity) and differences in HRV at baseline, using "no change" as the reference category) (n=88).
Additional file 4: Supplementary file 2.
Mean change in R-R in the improved and not-improved categories.
Additional file 5: Supplementary file 3.
Mean change in SDNN in the improved and not-improved categories.
Additional file 6: Supplementary file 4.
Mean change in HF in the improved and not-improved categories.
Additional file 7: Supplementary file 5.
Mean change in Total Power in the improved and not-improved categories.
Additional file 8: Supplementary file 6.
Association between pain groups (based on clinically relevant change in pain intensity) and changes in HRV at each time point, using "no change" as the reference category) (n=87), adjusted for age, sex, baseline pain and intervention.
Additional file 9: Supplementary file 7.
Association between pain trajectories and HRV at baseline, using group 1. as the reference category (n=125).
Additional file 10: Supplementary file 8.
Mean change in R-R intervals for the four pain trajectories.
Additional file 11: Supplementary file 9.
Mean change in SDNN for the four pain trajectories.
Additional file 12: Supplementary file 10.
Mean change in HF for the four pain trajectories.
Additional file 13: Supplementary file 11.
Mean change in Total Power for the four pain trajectories.
Additional file 14: Supplementary file 12.
Association between pain trajectories and changes in HRV, using group 1. as the reference category (n=125), adjusted for age, sex, baseline pain and intervention.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bakken, A.G., Eklund, A., Warnqvist, A. et al. Are changes in pain associated with changes in heart rate variability in patients treated for recurrent or persistent neck pain?. BMC Musculoskelet Disord 23, 895 (2022). https://doi.org/10.1186/s12891-022-05842-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05842-4