
Abstract
Background
Neck pain is widespread among students in healthcare-related fields. Although neck pain is more prevalent in females, since most research involves mixed-sex samples we know very little about sex differences in contributors to neck pain. Thus, this study sought to explore sex differences in the risk factors for neck pain in this high-risk population.
Methods
This cross-sectional study was conducted in China in 2021 and included a sample of 1921 undergraduate healthcare students (693 males, 1228 females) from 7 health professional schools at Fujian Medical University. We collected data on neck pain symptoms, demographics, behavioral and psychological factors. Multiple regression analysis was conducted to examine sex differences in the risk factors of neck pain.
Results
The overall prevalence of neck pain was 41.6% with female students having a higher prevalence than male students (44.4% vs. 36.7%, respectively). The adjusted analyses showed that self-study time ≥ 6 h/day (OR = 1.44, 95% CI:1.13-1.83), flexed neck posture >20 degrees (OR = 2.19, 95% CI: 1.28-3.74), static duration posture >2 h (OR = 1.42, 95% CI: 1.02-1.97), and psychological distress (high: OR = 2.04, 95% CI:1.42-2.94; very high: OR = 2.50, 95% CI:1.57-3.74; respectively) were independent factors for neck pain in females. Among males, self-study time ≥ 6 h/day (OR = 1.43, 95% CI: 1.02-2.01) and psychological distress (moderate: OR = 2.04, 95% CI:1.28-3.25; high: OR = 2.37, 95% CI:1.49-3.79; very high: OR = 2.97, 95% CI:1.75-5.02; respectively) were significant risk factors for neck pain.
Conclusions
These findings suggest that the risk profiles of neck pain differ between females and males. The modifiable risk factors for neck pain, such as prolonged self-study time and elevated psychological distress, as well as poor posture among females, could be targeted through health promotion interventions in university settings.
Similar content being viewed by others

Introduction
Neck pain is a major health problem worldwide with an annual prevalence rates of 37.2% (range 16.7-75.1%) [1]. Healthcare professionals have developed various management and prevention measures for neck pain; paradoxically, neck pain is highly prevalent among healthcare professionals due to the nature of their work [2, 3]. However, it has been suggested that healthcare professionals experience neck pain even before they start working. An alarmingly high rate of musculoskeletal pain — especially neck pain — has been reported among undergraduate students studying to be healthcare professionals, with a reported annual prevalence ranging from 23.6 to 69.2% [4, 5]. Neck pain can pose a large burden to both individuals and society due to treatment costs, disruption of well-being, and loss of productivity [6, 7]. Thus, there is an urgent need to identify the risk factors of neck pain and develop effective interventions in this young, susceptible population.
The etiology of neck pain is complex and believed to be a biopsychosocial problem [1, 8]. Multiple risk factors for neck pain have been reported in previous studies, such as being female, an older age, a higher BMI, smoking, electronic devices overuse, awkward/sustained postures, physical inactivity, negative emotions, and lack of social support [1, 6, 8]. The global COVID-19 pandemic has posed huge changes to people’s daily routines, and healthcare students have been seriously affected. The pandemic and associated restrictions have negatively impacted their academic, lifestyle and mental health, which may precipitate or exacerbate neck pain [9,10,11]. However, studies of potential risk factors for neck pain are generally inconsistent, and evidence that can support the development of management strategies is limited [8, 12]. For example, some studies of healthcare students found that being female, an older age, and a higher BMI were not associated with neck pain [13,14,15,16,17]. Similarly, the findings regarding psychological factors associated with neck pain in healthcare students are mixed and thus inconclusive. Some studies report that psychological disorders are associated with an increased risk of neck pain, while others found no significant association [13,14,15,16].
Increasing studies have reported sex differences in lifestyle behaviors, and psychological status in healthcare students [18,19,20,21]. According to published reports, female students are less likely to be physically active than males and spend more time in sedentary activity [18, 19]. Additionally, under stressful conditions at medical universities, female students tend to suffer more from mental health problems (e.g. psychological distress, depression and anxiety) than their male counterparts [20, 21]. In this regard, some distinctions may exist in the association between neck pain and related factors. As most research on neck pain among healthcare students is based on combined analysis of mixed-sex samples, we know very little about sex differences in factors for neck pain. Sex differences in the prevalence of musculoskeletal pain, including neck pain among various population, has been reported in many studies, which is proposed to be due to sex differences in pain sensitivity and muscle anatomy and pain sensitivity [8, 22, 23]. Furthermore, some authors have noted that sex differences in behavioral and psychological risk factors can influence musculoskeletal pain, e.g., females report a higher likelihood of poor posture and higher rates of co-morbid psychological distress [24,25,26]. Such findings can help optimize individual prevention and treatment strategies for musculoskeletal pain since behavioral and psychological factors are potentially modifiable, unlike demographic characteristics.
To fill this research gap, the current study examined the occurrence of neck pain in relation to behavioral and psychological factors among healthcare students, with specific reference to sex specificity. We hypothesized that the factors associated with neck pain in this population may relate to sex differences.
Methods
Design and participants
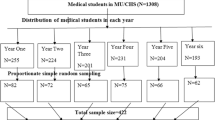
This cross-sectional study was conducted at the largest medical university in Fujian Province, which is located in southeast China, during the period of December 14 to 29, 2021. A cluster sampling approach was adopted to draw a 30% sample of 7931 healthcare students at this university. The target population was full-time students enrolled in years 1-3 from the School of Basic Medical Sciences, School of Stomatology, School of Nursing, School of Public Health, School of Medical Technology and Engineering, School of Health, and School of Pharmacy. All students in the selected classes were encouraged to participate in this survey. The purpose of the survey and fact that their anonymity and confidentiality would be maintained were explained to the students by the investigators before obtaining their informed consent. Students completed the questionnaires via the online platform Wenjuanxing (www.wjx.cn). Most students took approximately 6-10 minutes to complete the questionnaire. The same IP address could be used only once to complete the questionnaire to prevent multiple responses from the same student. This study was approved by the Research Ethics Committee of Fujian Medical University (file reference:2021-159).
Sample size
The sample size of the study was calculated by the formula: n = (za/2)2 p (1 − p) /d2, where, n = sample size, za/2 = 1.96, p = a previous rate of 29.2% proportion prevalence of neck pain among Chinese undergraduate students, and d = margin of error (3%), which produced a sample size of 883 [27]. Since a cluster sampling strategy was adopted with a design effect of 2, the final sample size estimated was 2355 subjects accounting for a 25% non-response rate.
Neck pain
Neck pain was assessed using the Nordic Musculoskeletal Questionnaire [28]. This questionnaire was validated and adapted for various population [4, 15, 29]. Specifically, participants were asked the following question: “During the past 12 months, have you at any time had ache, pain or discomfort in the neck?” A body map was included to allow students to report neck pain by referencing specific neck region [28, 29]. The response options were “no” or “yes”, with “yes” denoting relevant pain in the neck region.
Demographic, behavioral, and psychological questionnaires
Demographic characteristics, including age, gender (male or female), year of study (first year, second year, or third year), weight, and height, were collected from all participants using a questionnaire. Body mass index (BMI) was calculated as weight (kg)/height (meter)2 and then categorized as underweight (< 18.5), normal (18.5-24.9), overweight (25.0-29.9), and obese (> 30).
The following behaviors were assessed: smoking status (never, ex-smoker, or current smoker), computer usage (<2 h/day, or ≥ 2 h/day), smartphone usage (<6 h/day, or ≥ 6 h/day), self-study time (<6 h/day, or ≥ 6 h/day), sitting habitual neck posture (upright, slightly flexed 10-20 degrees, or sharply flexed >20 degrees; with a reference picture about sagittal neck posture), static duration posture (<1 h, 1-2 h, or >2 h), and leisure time physical activity (occasionally; regularly, 1-2 times/week, or regularly, ≥3 times/week; 1 time means continuous physical activity for at least 30 min per week, and feeling warm or sweaty) [10, 15,16,17, 30].
Psychological factors were assessed using the Kessler Psychological Distress Scale (K10). We used the K10 because it is an internationally validated, brief screening instrument to assess non-specific psychological symptoms in population-based epidemiological studies, with a focus on depression and anxiety [31]. Participants rated the 10 items on a 5-point Likert scale (ranging from none of the time to all the time). Scores range from 10 to 50, with a higher score indicating more psychological distress. The interpretation of K10 scores is based on a four-level categorization: low (10-15), moderate (16-21), high (22-29), and very high (30-50) [32]. The Cronbach’s alpha of the K10 in this sample was 0.925.
Statistical analysis
Statistical analysis was performed using the IBM Statistical Package for Social Science program, version 25.0. Categorical variables are presented as numbers and percentages. The chi-square test was used to compare categorical variables between groups with and without neck pain. Binary logistic regression analyses were conducted separately for male and female students to identify sex-specific risk factors associated with neck pain. Univariate logistic regression models were used to identify potential confounders. Variables with p < 0.1 in the univariate logistic regression were selected for multiple logistic regression model. The results are presented as crude odds ratios (cORs), adjusted ORs (aORs), and 95% confidential intervals (CIs). A p-value < 0.05 was considered to be statistically significant.
Results
A total of 2003 healthcare students completed the survey. Of these, 82 were excluded from analysis due to an overly short response duration (< 3 min) or errors in logic, resulting in a final sample of 1921 participants (a valid response rate = 95.9%). The characteristics of these participants are shown in Table 1. Participants’ ages ranged from 17 to 23 years with a median of 19 years; 37.1% were first year students, 31.3% were second year students, and 31.5% were third year students. The male: female sex ratio was approximately 1:2 (males: 36.1%, females: 63.9%), which may result from the sex imbalance at many Chinese colleges and universities [33]. The annual prevalence of neck pain was 41.6% (95% CI: 39.4-43.8) with female students having a higher prevalence than male students, 44.4% (95% CI: 41.6-47.2) and 36.7% (95% CI: 33.1-40.2), respectively.
There were statistically significant sex differences in the demographics, behavioral and psychological factors. Compared female respondents, a greater proportion of male respondents reported being “overweight/obese” and a “current smoker”. Significantly more males than females reported high computer usage time per day, whereas significantly more females than males reported high smartphone usage time per day (all p < 0.001). Furthermore, prolonged self-study time, a sitting flexed neck posture, prolonged static posture, physical inactivity, and psychological distress were reported more often by female students (all p < 0.05).
Table 2 shows that male students with neck pain were more likely to report a prolonged self-study time, a low level of physical activity, and an elevated level of psychological distress (all p < 0.05). The other variables did not differ significantly between males with and without neck pain. In the univariate analyses, self-study time (≥6 h/day: cOR = 1.47, p = 0.022) and psychological distress (moderate: cOR = 2.09, high: cOR = 2.51, very high: cOR = 3.22; all p < 0.01) were associated with increased neck pain.
Table 3 shows that female students with neck pain tended to have a prolonged self-study time, flexed neck posture, prolonged static posture, and elevated level of psychological distress compared with those without neck pain (all p < 0.05). Univariate analysis identified longer self-study time (≥ 6 h/day: cOR = 1.39, p = 0.006), sitting habitual neck posture (sharply flexed >20 degrees: cOR = 2.38, p = 0.001), static duration of posture (>2 h: cOR = 1.68, p = 0.001), and psychological distress (high: cOR = 2.19, very high: cOR = 2.81, respectively; all p < 0.001) as potential risk factors for neck pain.
Table 4 indicates that a self-study time ≥ 6 h/day was significantly associated with neck pain in both males and females (aOR = 1.43 and aOR = 1.44, respectively; all p <0.05). Notably, males with very high, high, and moderate psychological distress had a significantly increased risk of neck pain (aOR = 2.04, aOR = 2.37 and aOR = 2.97, respectively; all p<0.01). A similar association was observed in females, with the odds of neck pain increasing with high or very high psychological distress (aOR = 2.04 and aOR = 2.50, respectively; all p <0.001). Furthermore, a sitting habitual neck posture (sharply flexed >20 degrees: aOR = 2.19, p = 0.004), and static duration of posture were significantly associated with neck pain in female students (>2 h: aOR = 1.42, p = 0.036). However, there was no such relationship in male students.
Discussion
In current study, we found that a significant proportion of undergraduate healthcare students in China experienced neck pain in the previous 12 months, with female students having a higher prevalence than male students. Sex differences in the prevalence of neck pain among healthcare students have been reported in other studies [5, 14, 19]. We further identified sex-specific risk profiles for neck pain in this high-risk population, which supports our research hypothesis. Specifically, among female students, self-study time, habitual flexed neck posture, static duration of posture, and psychological distress were significantly associated with neck pain. In contrast, only self-study time and psychological distress were significantly associated with neck pain in the adjusted model for male students. To the best of our knowledge, this is the first study to explore sex different in risk factors with neck pain among healthcare students. Accordingly, some meaningful implications can be drawn from our findings.
The association between time spent on electronic devices and neck pain is debatable [12, 34]. According to a prior study, medical students with smartphone usage >6 h/day were 2.782 times more likely to report neck pain [17]. Among our participants, females tended to show greater use of smartphones, while males spent more time on computers than females. Our results are consistent with other research of university students reporting sex differences in the time spent on electronic devices [33]. However, no association was found with either daily duration of smartphone or computer use with neck pain in each sex. This may be partly because the data in our study were self-reported, which could have led to bias. This finding is, however, similar to that of a recent study reporting no significant association between increased time spent on electronic devices and musculoskeletal pain in medical students in Jordan during remote learning [11]. Furthermore, our results show no association of older age, year of study, BMI, and smoking status with neck pain in each sex. Future research is thus required to examine these associations.
Healthcare students frequently engage in studying activities because of their demanding academic load. Our results showed an independent association between prolonged studying and neck pain in males and females; specifically, students who spent ≥6 h/day in self-study were more likely to experience neck pain. Previous studies have reported that poor posture has a significant effect on neck pain among healthcare students [4, 16]. In particular, poorer posture was associated with a higher prevalence of neck pain while participating in remote learning during the pandemic [11]. In the present study, a habitual neck posture and static duration of posture apparently differed between males and females. Further, we found that a sitting habitual neck posture and static duration of posture were significantly associated with neck pain in females. However, there was no such relationship in males. Based on our findings, females with flexed neck posture (>20 degrees) and static posture over 2 hours had an increased risk of neck pain 2.19 times and 1.42 times, respectively. Previous studies have demonstrated that non-neutral postures contribute to cumulative biomechanical load on the cervical spine, while sustained postural loading affects these structures (e.g., strain muscles and ligaments, compress nerves) and can become a cause of neck pain [35, 36]. The present findings extend the literature regarding the association of poor posture and neck pain being female-specific, which could partially explain the higher prevalence of neck pain in females. A prospective study by Richards et al. also supports posture as a sex-specific risk factor; however, they found that females in late adolescence who sat with an upright sitting posture had a greater risk of persistent neck pain as young adults than those with a thorax/forward head or intermediate posture [37]. More research is thus warranted to determine the optimal posture to prevent and treat neck pain.
Generally, regular physical activity has benefits for overall physical and mental health. Based on leisure time physical activity reported by our participants, almost two thirds had irregular physical activity and females were less physically active than males. This is consistent with findings from other studies showing sex differences in physical activity levels [18, 19, 38]. Contrary to the hypothesis, our results showed that physical activity was not associated with neck pain in each sex. The results of this study are thus discordant with those of prior studies reporting that healthcare students with regular physical activity have a reduced occurrence of neck pain compared with those who were physical inactive [5, 16, 17]. A possible explanation for this discrepancy might be that we collected data during the pandemic, and the various restrictions may have dissuaded students from engaging in the recommended levels of physical activity. However, the evidence for the role of physical activity in neck pain in the existing literature has been mixed, with some studies suggesting regular physical activity can be beneficial while others indicate no effect or even harmful effects [10, 12, 39, 40]. From a public health perspective, specific types and intensities of physical activity could be developed and promoted to help prevent neck pain.
Psychological distress among healthcare students has become a global concern — especially during the pandemic [9, 20, 21]. In this study, psychological distress was found to be more prevalent in females compared to males, which is consistent with sex differences in the prevalence of psychological distress in this population [20, 21]. Further, our study showed that psychological distress was positively associated with neck pain in both males and females; specifically, those with higher levels of psychological distress were more likely to experience neck pain. Our results are compatible with other studies that investigated the association between psychological distress and neck pain, despite the different assessment scales for psychological distress [41,42,43]. Some prospective studies have suggested that psychological distress as a meaningful predictor of the development and persistence in neck pain [26, 44, 45]. To our knowledge, few studies prior to this work have examined this association among healthcare students, despite the high prevalence of psychological distress and neck pain in this population. Due to increased recognition of the important role of psychological factors in neck pain, psychological interventions are increasingly being used in the management of neck pain [46,47,48]. It is also important to note that psychological distress was more strongly associated with neck pain in males than in females, as shown in our study, although females reported higher levels of psychological distress than males. This finding is supported by several studies in adolescents and the general population showing that males report a higher association with musculoskeletal pain-related emotions (e.g., depression and catastrophizing) than females [49, 50]. However, it is unclear how sex influences the underlying mechanism of this observation. Nevertheless, these findings suggest that raising awareness among healthcare providers about psychological interventions for males is recommended to prevent males with neck pain from being treated less aggressively than females.
Limitations and strengths
Some limitations of this study need to be noted. Firstly, as we did not differentiate between acute and chronic neck pain, the findings need to be interpreted with caution. Secondly, as the data were collected using a self-report questionnaire, there may be discrepancies between what the students reported and their actual experiences. Thirdly, our cross-sectional design prevents drawing causal inferences from the associations. Future prospective studies are required to confirm our results. Fourthly, other neck pain-related factors were not accounted for, such as medication use, past pain experience, socioeconomic status, and social support. Thus, generalization is limited. Finally, since recruitment was restricted to undergraduate students at one medical university, our sample might not be representative of all Chinese healthcare students and students from other countries.
The strengths of the current study are its relatively large sample, which allowed us to identify sex differences in several factors associated with neck pain in healthcare students and offer potential implications for healthcare providers. Of further concern is the fact that neck pain during this period of life may adversely affect the long-term health of healthcare students. It is thus imperative to increase awareness among healthcare students during medical education about risk factors for neck pain and encourages healthy lifestyle habits, especially informing female students of proper posture. On the other hand, our study highlights the importance of accounting for psychological components: identifying and addressing psychological distress in healthcare students may be an effective intervention to prevent and control neck pain. Lastly, additional research is needed to obtain a better understanding of the mechanisms underlying the sex differences in these associations.
Conclusions
In conclusion, our findings indicated that prolonged self-study time and elevated psychological distress were significantly associated with neck pain in both sexes. In addition, poor posture in females is likely to increase the risk of neck pain. Early management of neck pain based on sex-related differences in risk factors should be considered in university settings to minimize the burden of neck pain among future healthcare professionals.
Availability of data and materials
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy reasons.
Abbreviations
- BMI:
-
Body mass index
- Ref.:
-
Reference
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- cOR:
-
Crude odds ratio
- aOR:
-
Adjusted odds ratio
References
Cohen SP, Hooten WM. Advances in the diagnosis and management of neck pain. BMJ. 2017;358:j3221. https://doi.org/10.1136/bmj.j3221.
Long MH, Bogossian FE, Johnston V. The prevalence of work-related neck, shoulder, and upper back musculoskeletal disorders among midwives, nurses, and physicians: a systematic review. Workplace Health Saf. 2013;61:223-9. https://doi.org/10.1177/216507991306100506.
Dong H, Zhang Q, Liu G, Shao T. Prevalence of neck/shoulder pain among public hospital workers in China and its associated factors: a cross-sectional study. Sci Rep. 2020;23(10):12311. https://doi.org/10.1038/s41598-020-69382-4.
Penkala S, El-Debal H, Coxon K. Work-related musculoskeletal problems related to laboratory training in university medical science students: a cross sectional survey. BMC Public Health. 2018;18:1208. https://doi.org/10.1186/s12889-018-6125-y.
Felemban RA, Sofi RA, Alhebshi SA, Alharbi SG, Farsi NJ, Abduljabbar FH, et al. Prevalence and predictors of musculoskeletal pain among undergraduate students at a dental School in Saudi Arabia. Clin Cosmet Investig Dent. 2021;13:39-46. https://doi.org/10.2147/CCIDE.S292970.
Hogg-Johnson S, van der Velde G, Carroll LJ, Holm LW, Cassidy JD, Guzman J, et al. The burden and determinants of neck pain in the general population: results of the bone and joint decade 2000-2010 task force on neck pain and its associated disorders. J Manip Physiol Ther. 2009;32:S46-60. https://doi.org/10.1016/j.jmpt.2008.11.010.
Safiri S, Kolahi AA, Hoy D, Buchbinder R, Mansournia MA, Bettampadi D, et al. Global, regional, and national burden of neck pain in the general population, 1990-2017: systematic analysis of the global burden of disease study 2017. BMJ. 2020;368:m791. https://doi.org/10.1136/bmj.m791.
Kazeminasab S, Nejadghaderi SA, Amiri P, Pourfathi H, Araj-Khodaei M, Sullman MJM, et al. Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord. 2022;23:26. https://doi.org/10.1186/s12891-021-04957-4.
Li Y, Wang Y, Jiang J, Valdimarsdóttir UA, Fall K, Fang F, et al. Psychological distress among health professional students during the COVID-19 outbreak. Psychol Med. 2021;51:1952-4. https://doi.org/10.1017/S0033291720001555.
Ogunlana MO, Govender P, Oyewole OO. Prevalence and patterns of musculoskeletal pain among undergraduate students of occupational therapy and physiotherapy in a south African university. Hong Kong Physiother J. 2021;41(1):35-43. https://doi.org/10.1142/S1013702521500037.
Salameh MA, Boyajian SD, Odeh HN, Amaireh EA, Funjan KI, Al-Shatanawi TN. Increased incidence of musculoskeletal pain in medical students during distance learning necessitated by the COVID-19 pandemic. Clin Anat. 2022;35(4):529-36. https://doi.org/10.1002/ca.23851.
Jahre H, Grotle M, Smedbråten K, Dunn KM, Øiestad BE. Risk factors for non-specific neck pain in young adults. A systematic review. BMC Musculoskelet Disord. 2020;21(1):366. https://doi.org/10.1186/s12891-020-03379-y.
Smith DR, Wei N, Ishitake T, Wang RS. Musculoskeletal disorders among Chinese medical students. Kurume Med J. 2005;52:139-46. https://doi.org/10.2739/kurumemedj.52.139.
Almhdawi KA, Mathiowetz V, Al-Hourani Z, Khader Y, Kanaan SF, Alhasan M. Musculoskeletal pain symptoms among allied health professions' students: prevalence rates and associated factors. J Back Musculoskelet Rehabil. 2017;30:1291-301. https://doi.org/10.3233/BMR-169669.
Chan L, Wong A, Wang MH, Cheung K, Samartzis D. The prevalence of neck pain and associated risk factors among undergraduate students: a large-scale cross-sectional study. Int J Ind Ergonom. 2020;76:102934. https://doi.org/10.1016/j.ergon.2020.102934.
Weleslassie GG, Meles HG, Haile TG, Hagos GK. Burden of neck pain among medical students in Ethiopia. BMC Musculoskelet Disord. 2020;21:14. https://doi.org/10.1186/s12891-019-3018-x.
Ayhualem S, Alamer A, Dabi SD, Bogale KG, Abebe AB, Chala MB. Burden of neck pain and associated factors among smart phone user students in University of Gondar, Ethiopia. PLoS One. 2021;16(9):e0256794. https://doi.org/10.1371/journal.pone.0256794.
Ge Y, Xin S, Luan D, Zou Z, Liu M, Bai X, et al. Association of physical activity, sedentary time, and sleep duration on the health-related quality of life of college students in Northeast China. Health Qual Life Outcomes. 2019;17:124. https://doi.org/10.1186/s12955-019-1194-x.
Sklempe Kokic I, Znika M, Brumnic V. Physical activity, health-related quality of life and musculoskeletal pain among students of physiotherapy and social sciences in eastern Croatia - cross-sectional survey. Ann Agric Environ Med. 2019;26(1):182-90 https://doi.org/10.26444/aaem/102723.
Merlo LJ, Curran JS, Watson R. Gender differences in substance use and psychiatric distress among medical students: a comprehensive statewide evaluation. Subst Abus. 2017;38(4):401-6. https://doi.org/10.1080/08897077.2017.1355871.
Rodríguez-Roca B, Subirón-Valera AB, Gasch-Gallén Á, Calatayud E, Gómez-Soria I, Marcén-Román Y. Gender self-perception and psychological distress in healthcare students during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(20):10918. https://doi.org/10.3390/ijerph182010918.
Paananen M, O'Sullivan P, Straker L, Beales D, Coenen P, Karppinen J, et al. A low cortisol response to stress is associated with musculoskeletal pain combined with increased pain sensitivity in young adults: a longitudinal cohort study. Arthritis Res Ther. 2015;17:355. https://doi.org/10.1186/s13075-015-0875-z.
Nagai T, Schilaty ND, Krause DA, Crowley EM, Hewett TE. Sex differences in ultrasound-based muscle size and mechanical properties of the cervical-flexor and -extensor muscles. J Athl Train. 2020;55:282-8. https://doi.org/10.4085/1062-6050-482-18.
Côté JN. A critical review on physical factors and functional characteristics that may explain a sex/gender difference in work-related neck/shoulder disorders. Ergonomics. 2012;55:173-82. https://doi.org/10.1080/00140139.2011.586061.
Bento TPF, Genebra CVDS, Maciel NM, Cornelio GP, Simeão SFAP, Vitta A. Low back pain and some associated factors: is there any difference between genders? Braz J Phy Ther. 2020;24:79-87. https://doi.org/10.1016/j.bjpt.2019.01.012.
Paanalahti K, Holm LW, Magnusson C, Carroll L, Nordin M, Skillgate E. The sex-specific interrelationship between spinal pain and psychological distress across time in the general population. Results from the Stockholm public health study. Spine J. 2014;14:1928-35. https://doi.org/10.1016/j.spinee.2013.11.017.
Yang G, Cao J, Li Y, Cheng P, Liu B, Hao Z, et al. Association between internet addiction and the risk of musculoskeletal pain in Chinese college freshmen- a cross-sectional study. Front Psychol. 2019;10:1959. https://doi.org/10.3389/fpsyg.2019.01959.
Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18:233-7. https://doi.org/10.1016/0003-6870(87)90010-x.
Fejer R, Hartvigsen J. Neck pain and disability due to neck pain: what is the relation? Eur Spine J. 2008;17(1):80-8. https://doi.org/10.1007/s00586-007-0521-9.
Rasmussen-Barr E, Bohman T, Hallqvist J, Holm LW, Skillgate E. Do physical activity level and body mass index predict recovery from persistent neck pain in men and women of working age? A population-based cohort study. Eur Spine J. 2013;22(9):2077-83. https://doi.org/10.1007/s00586-013-2801-x.
Kessler RC, Barker PR, Colpe LJ, Epstein JF, Gfroerer JC, Hiripi E, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry. 2003;60:184-9. https://doi.org/10.1001/archpsyc.60.2.184.
Stallman HM. Psychological distress in university students: a comparison with general population data. Aust Psychol. 2010;45:249-57. https://doi.org/10.1080/00050067.2010.482109.
Lu L, Dong M, Jian S, Gao J, Ye L, Chen H, et al. Sex differences in the factors associated with sleep duration in university students: a cross-sectional study. J Affect Disord. 2021;290:345-52. https://doi.org/10.1016/j.jad.2021.04.025.
Xie Y, Szeto G, Dai J. Prevalence and risk factors associated with musculoskeletal complaints among users of mobile handheld devices: a systematic review. Appl Ergon. 2017;59:132-42. https://doi.org/10.1016/j.apergo.2016.08.020.
Vasavada AN, Nevins DD, Monda SM, Hughes E, Lin DC. Gravitational demand on the neck musculature during tablet computer use. Ergonomics. 2015;58(6):990-1004. https://doi.org/10.1080/00140139.2015.1005166.
Namwongsa S, Puntumetakul R, Neubert MS, Boucaut R. Effect of neck flexion angles on neck muscle activity among smartphone users with and without neck pain. Ergonomics. 2019;62(12):1524-33. https://doi.org/10.1080/00140139.2019.1661525.
Richards KV, Beales DJ, Smith AL, O'Sullivan PB, Straker LM. Is neck posture subgroup in late adolescence a risk factor for persistent neck pain in young adults? A prospective study. Phys Ther. 2021;101:pzab007. https://doi.org/10.1093/ptj/pzab007.
Mitáš J, Cerin E, Reis RS, Conway TL, Cain KL, Adams MA, et al. Do associations of sex, age and education with transport and leisure-time physical activity differ across 17 cities in 12 countries? Int J Behav Nutr Phys Act. 2019;16:121. https://doi.org/10.1186/s12966-019-0894-2.
Shahidi B, Curran-Everett D, Maluf KS. Psychosocial, physical, and neurophysiological risk factors for chronic neck pain: a prospective inception cohort study. J Pain. 2015;16(12):1288-99. https://doi.org/10.1016/j.jpain.2015.09.002.
Aartun E, Boyle E, Hartvigsen J, Ferreira PH, Maher CG, Ferreira ML, et al. The most physically active Danish adolescents are at increased risk for developing spinal pain: a two-year prospective cohort study. BMJ Open Sport Exerc Med. 2016;2:e000097. https://doi.org/10.1136/bmjsem-2015-000097.
Cho CY, Hwang IS, Chen CC. The association between psychological distress and musculoskeletal symptoms experienced by Chinese high school students. J Orthop Sports Phys Ther. 2003;33(6):344-53. https://doi.org/10.2519/jospt.2003.33.6.344.
Chen X, O'Leary S, Johnston V. Modifiable individual and work-related factors associated with neck pain in 740 office workers: a cross-sectional study. Braz J Phys Ther. 2018;22(4):318-27. https://doi.org/10.1016/j.bjpt.2018.03.003.
Derakhshanrad N, Yekaninejad MS, Mehrdad R, Saberi H. Neck pain associated with smartphone overuse: cross-sectional report of a cohort study among office workers. Neck pain associated with smartphone overuse: cross-sectional report of a cohort study among office workers. Eur Spine J. 2021;30(2):461-7. https://doi.org/10.1007/s00586-020-06640-z.
Dario AB, Kamper SJ, Williams C, Straker L, O'Sullivan P, Schütze R, et al. Psychological distress in early childhood and the risk of adolescent spinal pain with impact. Eur J Pain. 2022;26(2):522-30. https://doi.org/10.1002/ejp.1878.
Xie Y, Coombes BK, Thomas L, Johnston V. Time Course and Risk Profile of Work-Related Neck Disability: A Longitudinal Latent Class Growth Analysis. Phys Ther. 2022;102(6):pzac050. https://doi.org/10.1093/ptj/pzac050.
Lee H, Hübscher M, Moseley GL, Kamper SJ, Traeger AC, Mansell G, et al. How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. Pain. 2015;156(6):988-97. https://doi.org/10.1097/j.pain.0000000000000146.
Jeitler M, Brunnhuber S, Meier L, Lüdtke R, Büssing A, Kessler C, et al. Effectiveness of jyoti meditation for patients with chronic neck pain and psychological distress--a randomized controlled clinical trial. 2015;16(1):77-86. https://doi.org/10.1016/j.jpain.2014.10.009.
Coronado RA, Brintz CE, McKernan LC, Master H, Motzny N, Silva FM, et al. Psychologically informed physical therapy for musculoskeletal pain: current approaches, implications, and future directions from recent randomized trials. Pain Rep. 2020;5(5):e847. https://doi.org/10.1097/PR9.0000000000000847.
Myrtveit SM, Sivertsen B, Skogen JC, Frostholm L, Stormark KM, Hysing M. Adolescent neck and shoulder pain-the association with depression, physical activity, screen-based activities, and use of health care services. J Adolesc Health. 2014;55(3):366-72. https://doi.org/10.1016/j.jadohealth.2014.02.016.
Wijnhoven HA, de Vet HC, Picavet HS. Explaining sex differences in chronic musculoskeletal pain in a general population. Pain. 2006;124(1-2):158-66. https://doi.org/10.1016/j.pain.2006.04.012.
Acknowledgments
The authors would like to thank all of the participants in the study and the staff at the participating schools.
Funding
This research was funded by the National Natural Science Foundation of China (No. 81874501).
Author information
Authors and Affiliations
Contributions
BZ and LZ conceptualized the study and designed data collection tools. BZ drafted this manuscript. YZ, LJ, RY, YG and XL participated in the data collection. ML and JL contributed to analysis and interpretation of data. SW critically reviewed and approved the final manuscript. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Research Ethics Committee of Fujian Medical University (file reference:2021-159). The study protocol was clearly explained to all participants before the data was collected. Online informed consent was obtained from all participants included in the study. The collected data were used only for this study purpose.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zheng, B., Zheng, L., Li, M. et al. Sex differences in factors associated with neck pain among undergraduate healthcare students: a cross-sectional survey. BMC Musculoskelet Disord 23, 842 (2022). https://doi.org/10.1186/s12891-022-05782-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05782-z