
Abstract
Background
During the COVID-19 epidemic, the prevalence of neck pain among college students has increased due to the shift from offline to online learning and increasing academic and employment pressures. Therefore, this systematic review aimed to identify the personal, occupational, and psychological factors associated with the development of neck pain to promote the development of preventive strategies and early intervention treatment.
Methods
Seven electronic databases were searched from inception to December 2022 for cross-sectional studies, cohort studies, case-control studies, and randomized controlled trials (RCTs) on neck pain. The quality of the selected studies were assessed by American Agency for Healthcare Research and Quality (AHRQ) or the Newcastle-Ottawa Scale (NOS). Pooled odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were calculated to evaluate the effects of the included risk factors on neck pain.
Results
Thirty studies were included, including 18,395 participants. And a total of 33 potentially associated risk factors were identified. Ultimately, 11 risk factors were included in the meta-analysis after assessing, and all results were statistically significant (P < 0.05). The factors supported by strong evidence mainly include the improper use of the pillow (OR = 2.20, 95% CI: 1.39 to 3.48), lack of exercise (OR = 1.88, 95% CI: 1.53 to 2.30), improper sitting posture (OR = 1.97, 95% CI: 1.39 to 2.78), history of neck and shoulder trauma (OR = 2.32, 95% CI: 1.79 to 3.01), senior grade (OR = 2.86, 95% CI: 2.07 to 3.95), staying up late (OR = 1.80, 95% CI: 1.35 to 2.41), long-time electronic product usage daily (OR = 1.53, 95% CI: 1.33 to 1.76), long-time to bow head (OR = 2.04, 95% CI: 1.58 to 2.64), and emotional problems (OR = 2.09; 95% CI: 1.66 to 2.63). Risk factors supported by moderate evidence were high stress (OR = 1.61, 95% CI: 1.02 to 2.52) and female gender (OR = 1.69, 95% CI: 1.52 to 1.87).
Conclusion
This study obtained 11 main risk factors affecting college students neck pain, including improper use of the pillow, lack of exercise, improper sitting posture, history of neck and shoulder trauma, senior grade, staying up late, long-term electronic product usage daily, long time to bow head, high stress, emotional problems and female gender.
Similar content being viewed by others


Background
Neck pain is one of the most commonly reported musculoskeletal disorders, causing a substantial economic burden to healthcare systems [1], and the 2018 Global Burden of Disease report listed neck pain as one of the leading causes of long-term dysfunction [2]. In the general population, the average prevalence of neck pain is 23.1% [3], and the incidence of neck pain is very high in college students (48%-78%) [4,5,6]. The incidence of cervical spondylosis in college students is increasing rapidly, with an annual growth rate twice that of the 50-year-old group [7]. As studying at home became normal during the COVID-19 pandemic, the shift from offline to online learning styles seriously affected students' musculoskeletal health [8, 9]. With the emergence of online teaching, students spend more time using electronic devices to support their academic and leisure activities. Consequently, prolonged bowing at desks increases the incidence of neck pain in students [10,11,12]. Studies have revealed that neck pain is the leading cause of illness, decreased concentration, lower educational attainment, and college students skipping classes, thereby affecting students' future career prospects [13]. Thus, early recognition of the risk factors for neck pain is important for prevention and early intervention treatment.
The occurrence of neck pain is thought to be multifactorial, with individual, physical, and psychosocial factors that aggravate its onset and persistence [14]. Many risk factors, such as poor posture, obesity, trauma history, sex, age, and poor lifestyle, may contribute to the occurrence and development of neck pain [12, 15,16,17]. However, it is difficult to confirm the risk factors for neck pain in college studies owing to the unknown methodological quality. Accordingly, this meta-analysis was conducted to explore the risk factors for neck pain in college students to provide a basis for formulating preventive education and taking preventive and therapeutic measures.
Method
Protocol and registration
This meta-analysis was based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [18] (Additional File 1). The PROSPERO registration number for this systematic review is CRD42022333624.
Search strategy
The databases PubMed, Web of Science, Cochrane Library, Embase database, China National Knowledge Information Database (CNKI), WanFang Database, and Chinese Scientific Journal Database (VIP) were systematically and independently searched from databases establishment to December 2022 using the following MeSH terms and all related free search terms: (((((((((((((((neck pain[MeSH Terms]) OR (neck pain)) OR (neck discomfort[MeSH Terms])) OR (neck discomfort)) OR (neck ache[MeSH Terms])) OR (neck ache)) OR (cervicalgia[MeSH Terms])) OR (cervicalgia)) OR (nuchal pain[MeSH Terms])) OR (nuchal pain)) OR (cervical region discomfort[MeSH Terms])) OR (cervical region discomfort)) OR (cervical spondylosis[MeSH Terms])) OR (cervical spondylosis)) AND ((factor[MeSH Terms]) OR (factor))) AND ((((((((((((college students[MeSH Terms]) OR (college students)) OR (university students[MeSH Terms])) OR (university students)) OR (young adults[MeSH Terms])) OR (young adults)) OR (higher education students[MeSH Terms])) OR (higher education students)) OR (undergraduates[MeSH Terms])) OR (undergraduates)) OR (academic learners[MeSH Terms])) OR (academic learners)).
Inclusion and exclusion criteria
The titles and abstracts were first screened, and then the full text of the eligible literature was further examined independently by two reviewers. Any disagreement in the selection process was resolved through a full consultation with a third reviewer. Studies included in this meta-analysis met the following criteria: (1) cross-sectional, cohort studies, case–control studies, or RCTs (2) studies with original clear OR values (Odds Ratio) and 95% confidence interval (CI) that could be extracted or calculated with OR values and 95% CI (3) research subjects were college students, and (4) studies published in Chinese or English. The following studies were excluded: (1) studies that lacked data or did not analyze factors (2) full texts were unavailable (3) non-journal articles such as dissertations and conference papers, and (4) republished studies.
Data extraction and quality assessment
Two reviewers independently extracted the following information: first author, publication year, geographic region, study design, sample size, mean age, relevant risk factors, and OR (95% CI). The same two reviewers independently used the American Agency for Healthcare Research and Quality (AHRQ) to evaluate cross-sectional studies and the Newcastle-Ottawa Scale (NOS) to evaluate case-control and cohort studies [19, 20]. The AHRQ included 11 items that answered "yes,” "no, " or "unclear" [21]. If the answer is "no" or "unclear,” the score is 0, and if the answer is "yes,” a score of 1-3 indicates low quality, 4-7 indicated medium quality and 8-11 indicated high quality. The NOS included eight items in three blocks: subject selection, comparability between groups, and outcome measurement. The full score was 9, with 0-4 being low quality, 5-6 being moderate quality, and 7-9 being high quality. Any disagreement regarding data extraction or quality assessment was resolved through a full discussion with a third reviewer.
Strength of evidence
To determine the level of evidence for each influencing factor, and based on the quality of the studies, the existing evidence scales were used for assessment [22, 23] and were defined as follows: (1) strong evidence: the results come from a pool of three or more studies, at least two of which are high-quality homogeneous studies or synthesis of multiple high-quality studies (2) moderate evidence: statistically significant results from a combination of one high-quality study and one or more studies of moderate or low quality (3) limited evidence: the results come from a high-quality study or a combination of one or more moderate or low-quality studies, and (4) very limited evidence: the no evidence: significantly pooled results from multiple studies where heterogeneity findings were unrelated to quality.
Statistical analysis
Articles were grouped according to the type of risk factor using forest plots presenting results for the same factors. To ensure the reliability of the pooled effect estimates size, we only performed a meta-analysis of the risk factors assessed in at least three different studies. Data from two or fewer studies or factors with different results were presented in tables without summary analysis [24, 25]. Pooled ORs with corresponding 95% CIs were calculated to estimate the effect of risk factors on the occurrence of neck pain. If there were no OR values, the software was used for conversion. Heterogeneity across all included studies was assessed and quantified using Cochrane Q statistics and I2 statistics [26]. The greater the I2 value, the greater the heterogeneity. The low, moderate, and high degrees of heterogeneity were represented by I2 statistics of 25%, 50%, and 75%, respectively [27]. For results with high heterogeneity, sensitivity analysis was performed to determine the stability of the conclusions by excluding each study from the meta-analysis [28]. Funnel plot analysis was performed when at least ten studies were included in the analysis [29].
Results
Study selection
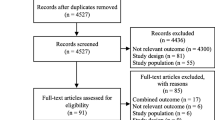
A total of 4869 related studies were identified by searching seven electronic databases, which were reduced to 3519 articles after removing duplicates; 3440 were excluded after reading the titles and abstracts. The reasons for exclusion included reviews, dissertations, conference papers, and research objects other than college students. After carefully reading the full text of the remaining 79 articles, 46 studies were excluded for the following reasons: (1) a lack of OR values and 95% CI or unable to convert (n = 24) (2) reporting outcomes with constituent ratio or frequency (n = 15), and (3) no full-text articles (n = 10). Finally, 30 studies were included, with 15 in English and 15 in Chinese. A PRISMA flow diagram was illustrated in Fig. 1.

Flowchart of the search process for the articles
Study characteristics and quality assessment
The basic characteristics of the included studies and quality assessment results were summarized in Table 1. A total of 30 studies were included [12, 30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58], including 24 cross-sectional studies, 2 cohort studies, and 4 case-control studies. Of these, 16 were rated as high quality and 14 as medium quality, with an overall average score of 7.67. The overall quality of the study was good.
Risk factors for neck pain in college students
Overall, 33 potential risk factors were extracted from the 30 eligible studies, including improper use of the pillow, staying up late, improper sitting posture, female gender, frequent alcohol consumption, history of neck and shoulder trauma, senior grade, history of pain, lack of exercise, obesity, history of psychosomatic symptoms, emotional problems, long-time electronic product usage daily, long-time to bow head, high stress, sedentariness, poor sleep quality, throat inflammation, improper keyboard position, heavy schoolbag, age, sleeping on a bus or car, feeling cold and wet wind, neck fatigue, poor head and neck posture, cigarette smoking, lack of rest, computer screen is not positioned at a level horizontal with the eyes, desks and chairs not matching height, many social media, major, the years of smartphone use and top-level sport. There were eleven risk factors, including improper use of the pillow, lack of exercise, improper sitting posture, history of neck and shoulder trauma, senior grade, staying up late, long time electronic product usage daily, long time to bow head, high stress, emotional problems and female gender that met the criteria for inclusion in the meta-analysis. The combined results and evidence levels are presented in Table 2.
Improper use of the pillow
Three studies [35, 36, 39] reported the effect of improper use of pillows on neck pain in college students, investigating a total of 1016 participants. Our results depicted that improper use of the pillow was one of the risk factors for neck pain in college students (OR = 2.20, 95% CI: 1.39 to 3.48, P = 0.0008). However, because the heterogeneity between studies was high (I2 = 66%) (Fig. 2A), a sensitivity analysis was performed. When excluding study of SuJ et al., 2013, the heterogeneity decreased significantly (I2 = 0%) (Additional File 2: Supplementary figure A), while the study conclusions remained statistically significant (P < 0.05).


Meta-analysis of risk factors for neck pain in college students (A:Improper use of the pillow, B:Lack of exercise, C:Improper sitting posture, D:History of neck and shoulder trauma, E:Senior grade, F:Staying up late, G:Long-time electronic product usage per day, H:Long-time to bow head, I:High stress, J:Emotional problems, K:Female gender)
Lack of exercise
Compared to regular exercise, five studies [12, 32, 35, 36, 43] found that physical inactivity was associated with a higher prevalence of neck pain in college students, with minimal heterogeneity (OR = 1.88, 95% CI: 1.53 to 2.30, P < 0.00001, I2 = 0%) (Fig. 2B).
Improper sitting posture
Seven studies [31, 34,35,36,37, 39, 53] analyzed the influence of improper sitting posture on neck pain in college students, investigated all 4002 participants, and found evidence of a positive correlation between this factor and neck pain. The combined analysis results revealed that improper sitting posture caused statistically significant harm to neck pain (OR = 1.97, 95% CI: 1.39 to 2.78, P = 0.0001). However, due to the high heterogeneity between the studies (I2 = 78%) (Fig. 2C), a sensitivity analysis was performed. When excluding the study by RenY et al., 2013, the heterogeneity decreased significantly (I2 = 0%) (Additional File 2: Supplementary figure B), while the study conclusions remained statistically significant (P < 0.05).
History of neck and shoulder trauma
Eight studies [36, 39, 41, 42, 46,47,48,49] investigated all 2947 participants, and all reported the impact of a history of neck and shoulder disease on neck pain in college students. Our pooled results demonstrated that college students with a history of neck and shoulder trauma were more likely to develop neck pain, with a high prevalence and less heterogeneity (OR = 2.32, 95% CI: 1.79 to 3.01, P < 0.00001, I2 = 22%) (Fig. 2D).
Senior grade
Five studies [31, 43, 45, 49, 51] analyzed the effect of grade differences on neck pain among 2287 college students. The combined results depicted that a higher probability and frequency of neck pain occurred at grade level (OR = 2.86, 95% CI: 2.07 to 3.95, P < 0.00001, I2 = 5%) (Fig. 2E).
Staying up late
Five studies [31, 34, 39, 40, 54] that evaluated the association between staying up late and neck pain in college students were included in the meta-analysis. The combined results revealed that a high prevalence of neck pain in college students was associated with often staying up late (OR = 1.80, 95% CI: 1.35 to 2.41, P < 0.0001). However, due to its high heterogeneity (I2 = 55%) (Fig. 2F), it was reduced by excluding the articles one by one. Finally, the heterogeneity decreased significantly when excluding HuY et al., 2018 (I2 = 0%) (Additional File 2: Supplementary figure C), while the results remained statistically significant (P < 0.00001).
Long-time electronic product usage per day
Eleven studies [30, 32, 36, 37, 41, 43, 47, 49, 53, 56, 57] analyzed the impact of a long-time electronic product used daily on neck pain in 10,314 college students. The results of the combined meta-analysis demonstrated that prolonged use of electronics was significantly associated with neck pain in college students (OR = 1.53, 95% CI: 1.33 to 1.76, P < 0.00001). Subgroup meta-analysis revealed that both smartphone and computer use could cause neck pain in college students (P < 0.0001 and P = 0.0002, respectively), but due to the combined heterogeneity (I2 = 78%) (Fig. 2G), the sensitivity analysis found that the overall heterogeneity was still relatively large regardless of which study was removed. The funnel plot shows almost bilateral symmetry and is less likely to be influenced by publication bias (Fig. 3).

Funnel plot about meta-analysis of risk factors about long-time electronic product usage per day
Long-time to bow head
Ten studies [12, 30, 33, 35, 37, 39, 40, 45, 52, 53] reported the impact of long bowing on neck pain in college students, investigating a total of 10,388 participants. The summary results demonstrated that a long time to bow head would lead to frequent neck pain among college students (OR = 2.04, 95% CI: 1.58 to 2.64, P < 0.00001). The results of the subgroup analysis revealed that both a single time and total time to bow the head had a certain impact on neck pain in college students (P = 0.0007 and P < 0.00001). However, due to the large heterogeneity of the combined results (I2 = 82%), the heterogeneity could not be reduced by excluding studies individually (Fig. 2H). The funnel plot depicted bilateral asymmetries, which may have a publication bias (Fig. 4).

Funnel plot about meta-analysis of risk factors about long-time to bow head
High stress
Four studies [34, 44, 47, 55] analyzed the effects of high stress on neck pain among college students. The combined results showed that the greater the stress, the more likely they were to cause neck pain (OR = 1.61, 95% CI: 1.02 to 2.52, P < 0.00001, I2 = 88%) (Fig. 2I). Due to the large heterogeneity, sensitivity analysis found that the heterogeneity decreased significantly when excluding the study of Lin Y et al., 2022 (I2 = 0%) (Additional File 2: Supplementary figure D), and the results remained statistically significant (P < 0.00001).
Emotional problems
Five studies [35, 36, 38, 46, 48] that evaluated the relationship between emotional problems and neck pain in college students were included in the meta-analysis. The combined results demonstrated that college students with emotional problems were more likely to have neck pain than happy people (OR = 2.09; 95% CI: 1.66,2.63, P < 0.00001, I2 = 0%) (Fig. 2J).
Female gender
Three studies [30, 33, 55] concluded that female gender are one of the risk factors for neck pain in college students. The comprehensive analysis results showed that the prevalence of neck pain among female gender was much higher than that of male students (OR = 1.69; 95% CI: 1.52,1.87, P < 0.00001, I2 = 0%) (Fig. 2K).
Other risk factors
Although other risk factors, such as age, obesity, and frequent alcohol consumption, were found in their respective studies to be neck pain among college students, it was worth noting that these factors were only evaluated in one or two studies, indicating that there may not be enough evidence to prove the association with neck pain. Therefore, they are not in summary analysis, but the data was presented in the form of a table (Additional File 3).
Discussion
This study explored the risk factors for neck pain in college students and conducted a meta-analysis of 11 risk factors, including 30 studies. Meta-analysis revealed that 11 risk factors were closely related to neck pain in college students. Although the remaining 22 factors also revealed a significant association with the occurrence of neck pain, they were not included in the meta-analysis due to the limited number of studies. There were eight previous reviews [1, 23, 59,60,61,62,63,64] and four meta-analyses [16, 65–67] on the risk factors of neck pain. However, the eight reviews lacked quantitative analysis, and the four meta-analyses included only English studies. Furthermore, the study subjects were not college students but mainly office workers, fighter aircrews, and so on [1, 16, 23, 59,60,61,62,63,64,65,66,67]. Only one study [65] included young people aged 18–29 years, which may have involved a small proportion of college students. In addition, the research results depicted that depression, physical inactivity, history of trauma, female gender, prolonged computer use, bowing your head for a long time at your desk, obesity, and incorrect sitting posture were closely related to the occurrence of neck pain, similar to the results of the present study results [1, 16, 23, 59, 60, 62, 63]. However, there are a few studies that are inconsistent with the results of this study. Jun et al. [65, 66] found that the duration of computer use, continuous head bowing, and obesity were not associated with the occurrence of neck pain. Ariëns et al. [64] found that sedentariness was also an important risk factor for neck pain. This may be due to the small sample size of these three studies, which was insufficient to explain the correlation with the occurrence of neck pain.
Zhu et al. demonstrated that improper pillow use is mainly related to improper pillow height [36, 39], while appropriate height, moderate softness, and hardness could prevent neck discomfort. A previous systematic review and meta-analysis reflected exercise as a protective factor and reported a negative correlation between physical activity and musculoskeletal problems [68]. Ren et al. revealed that exercise time < 3 h per week [36, 37] or exercise frequency ≤ 5 times per week [35] could cause neck pain. Therefore, regular and moderate exercise could be used as a measure to prevent neck diseases [69, 70]. Improper sitting posture is mainly manifested in jittering and bumping of the legs or crossed legs [34], incorrect sitting posture [36, 39], and head-neck lateral deviation, flexion, and rotation [37] when sitting. This affects the dynamic and static balance of the neck and causes neck pain [71]. Studies have indicated that common histories of neck and shoulder trauma mainly include discomfort, such as being directly hit, head landing when falling from a height, sprains, or experiencing pain and stiffness of the head and neck due to a sudden brake [41]. Trauma can cause damage to the neck muscles, tendons, fascia, and ligaments, which can impact the cervical spine [72]. The high incidence of neck pain among college students is also partly due to the heavy workload and pressures of work and postgraduate entrance examinations, as students may stay up late more frequently, and excessive working hours may cause deformation of the neck and shoulders, leading to soft tissue damage and increasing the risk of neck pain [6, 48].
Studies have revealed that total daily electronic product use of ≥ 3 h and a long time to bow your head ≥ 1 h is likely to lead to neck pain [12, 30, 33, 36, 40, 43, 45, 47, 56, 57]. Therefore, with the increased use of electronic products and the academic burden, the prevalence of neck pain among college students is also increasing.
Among emotional problems, the most common risk factor for neck pain was depressive symptoms. Several studies have demonstrated that neck pain in college students is closely associated with a history of depression [35, 38, 46, 48]. Moreover, feeling low or nervous frequently is also a major risk factor for neck disease in college students [36]. It is clear that the influence of psychological factors on neck diseases may be the same as that of physical risk factors, and there is a significant positive correlation with neck pain [16].
Strengthens and limitations
This is the first systematic review and meta-analysis of risk factors for neck pain in college students to specifically address and prevent the development of risk factors for college students with neck pain. This review summarized the results of 30 prospective studies, the quality of which was moderate or above.
However, this systematic review and meta-analysis had some limitations. Firstly, we only included studies published in English and Chinese, and there may be potential publication and language biases; therefore, future studies should include a wider range of languages. Secondly, most included studies were cross-sectional, so no causal relationship between exposure factors and outcomes was established, and recall bias is likely to exist. Thirdly, there is no consensus on the definition of neck pain duration ranging from 3 to 12 months. Fourthly, most of the included studies only gave the risk factors without specific evaluation criteria. Finaly, some of the studies were conducted online, so it may exist self-selection or volunteer bias.
Conclusion
To sum up, although there were many studies in investigating the risk factors of neck pain, and found a large number of risk factors, but our study summarized eleven strong evidence risk factors, including the improper use of the pillow, lack of exercise, improper sitting posture, a history of neck and shoulder trauma, senior grade, staying up late, female gender, long time electronic product usage daily, long time to bow head, high stress and emotional problems. These eleven risk factors may lay a foundation for future neck disease prevention. However, there were still many factors that couldn't conduct meta-analysis due to few included studies. Therefore, it is recommended that more multicente and large-sample original studies closely related to these 11 risk factors could be conducted in the future to provide early warning for clinical practice and prevent neck pain in college students.
Availability of data and materials
All data are included in this manuscript.
Abbreviations
- OR:
-
Odds Ratio
- 95% CI:
-
95% Confidence Interval
- AHRQ:
-
American Agency for Healthcare Research and Quality
- NOS:
-
Newcastle-Ottawa Scale
- RCT:
-
Randomized Controlled Trial
- CNKI:
-
China National Knowledge Information Database
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
References
Kazeminasab S, Nejadghaderi SA, Amiri P, Pourfathi H, Araj-Khodaei M, Sullman MJM, et al. Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord. 2022;23(1):26. https://doi.org/10.1186/s12891-021-04957-4.
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–858. https://doi.org/10.1016/S0140-6736(18)32279-7.
Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24(6):783–92. https://doi.org/10.1016/j.berh.2011.01.019.
Hanvold TN, Wærsted M, Mengshoel AM, Bjertness E, Twisk J, Veiersted KB. A longitudinal study on risk factors for neck and shoulder pain among young adults in the transition from technical school to working life. Scand J Work Environ Health. 2014;40(6):597–609. https://doi.org/10.5271/sjweh.3437.
Crawford RJ, Volken T, Schaffert R, Bucher T. Higher low back and neck pain in final year Swiss health professions’ students: worrying susceptibilities identified in a multi-centre comparison to the national population. BMC Public Health. 2018;18(1):1188. https://doi.org/10.1186/s12889-018-6105-2.
Nawrocka A, Mynarski W, Powerska-Didkowska A, Grabara M, Garbaciak W. Musculoskeletal pain among Polish music school students. Med Probl Perform Art. 2014;29(2):64–9. https://doi.org/10.21091/mppa.2014.2015.
Zhao Jie Wu, Kunwei HW, Xiaoyu Hu, Xianyue Z. Influencing factors and preventive measures of spondylosis in college students. Healthmust-Readmagazine. 2020;22:244.
Majumdar P, Biswas A, Sahu S. COVID-19 pandemic and lockdown: cause of sleep disruption, depression, somatic pain, and increased screen exposure of office workers and students of India. Chronobiol Int. 2020;37(8):1191–200. https://doi.org/10.1080/07420528.2020.1786107.
Fallon N, Brown C, Twiddy H, Brian E, Frank B, Nurmikko T, et al. Adverse effects of COVID-19-related lockdown on pain, physical activity and psychological well-being in people with chronic pain. Br J Pain. 2021;15(3):357–68. https://doi.org/10.1177/2049463720973703.
Woo EHC, White P, Lai CWK. Musculoskeletal impact of the use of various types of electronic devices on university students in Hong Kong: An evaluation by means of self-reported questionnaire. Man Ther. 2016;26:47–53. https://doi.org/10.1016/j.math.2016.07.004.
Rakhadani P, Goon D, Mandeya A. Musculoskeletal problems associated with university students computer users: A cross-sectional study. Online J Health Allied Sci. 2017;16(2).
Weleslassie GG, Meles HG, Haile TG, Hagos GK. Burden of neck pain among medical students in Ethiopia. BMC Musculoskelet Disord. 2020;21(1):14. https://doi.org/10.1186/s12891-019-3018-x.
Al-Hadidi F, Bsisu I, AlRyalat SA, Al-Zu’bi B, Bsisu R, Hamdan M, et al. Association between mobile phone use and neck painin university students: A cross-sectional study using numeric rating scale for evaluation of neck pain. PLoS One. 2019;14(5):e0217231. https://doi.org/10.1371/journal.pone.0217231.
Guzman J, Hurwitz EL, Carroll LJ, Haldeman S, Côté P, Carragee EJ, et al. A new conceptual model of neck pain: linking onset, course, and care: the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. J Manipulative Physiol Ther. 2009;32(2 Suppl):S17-28. https://doi.org/10.1016/j.jmpt.2008.11.007.
Mahmoud NF, Hassan KA, Abdelmajeed SF, Moustafa IM, Silva AG. The Relationship Between Forward Head Posture and Neck Pain: a Systematic Review and Meta-Analysis. Curr Rev Musculoskelet Med. 2019;12(4):562–77. https://doi.org/10.1007/s12178-019-09594-y.
Kim R, Wiest C, Clark K, Cook C, Horn M. Identifying risk factors for first-episode neck pain: A systematic review. Musculoskelet Sci Pract. 2018;33:77–83. https://doi.org/10.1016/j.msksp.2017.11.007.
Bubric K, Hedge A. Differential patterns of laptop use and associated musculoskeletal discomfort in male and female college students. Work. 2016;55(3):663–71. https://doi.org/10.3233/WOR-162419.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hofmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:103–12. https://doi.org/10.1136/bmj.n71.
Zeng XT, Liu H, Chen X, Leng WD. Meta-analysis Series Four: Quality Assessment Tools for Observational Studies. Chin J Evid Based Cardiovasc Med. 2012;4(4):297–9. https://doi.org/10.3969/j.1674-4055.2012.04.004.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5. https://doi.org/10.1007/s10654-010-9491-z.
Rostom A, Dubé C, Cranney A. Celiac Disease. Rockville (MD): Agency for Healthcare Research and Quality (US); 2004 Sep. (Evidence Reports/Technology Assessments, No. 104.) Appendix D. Quality Assessment Forms. Available from: http://www.ncbi.nlm.nih.gov/books/NBK35156/
Van Tulder M, Furlan A, Bombardier C, Bouter L, Editorial Board of the Cochrane Collaboration Back Review Group. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine (Phila Pa 1976). 2003;28(12):1290–9. https://doi.org/10.1097/01.BRS.0000065484.95996.AF.
McLean SM, May S, Klaber-Moffett J, Sharp DM, Gardiner E. Risk factors for the onset of non-specific neck pain: a systematic review. J Epidemiol Community Health. 2010;64(7):565–72. https://doi.org/10.1136/jech.2009.090720.
Zhang J, Perret JL, Chang AB, Idrose NS, Bui DS, Lowe AJ, Abramson MJ, Walters EH, Lodge CJ, Dharmage SC. Risk factors for chronic cough in adults: A systematic review and meta-analysis. Respirology. 2022;27(1):36–47. https://doi.org/10.1111/resp.14169.
Favril L, Yu R, Hawton K, Fazel S. Risk factors for self-harm in prison: a systematic review and meta-analysis. Lancet Psychiatry. 2020;7(8):682–91. https://doi.org/10.1016/S2215-0366(20)30190-5.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58. https://doi.org/10.1002/sim.1186.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Wang D, Zhai JX, Mou ZY, Zong HX, Zhao XD, Wang XY, Gu P. Discussing on the Research of Heterogeneity inMeta-analysis. Chin J Evid Based Med. 2009;9(10):1115–8. https://doi.org/10.3969/j.issn.1672-2531.2009.10.013.
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097.
Li YW, Zhai Y, Liu ZY, Yan YR, Xia JY, Deng GY. Effects of the use of electronic products on neck and shoulder pain of university students. Modern Prev Med. 2020;47(17):3197–201.
Hu YY, Li DK. Survey to the Neck and Shoulder Pain and Its Risk Factors among Clinical College Students—Taking Zhuhai Campus of Zunyi Medical University for an Example. Phys Educ Rev. 2018;37(10):67–9. https://doi.org/10.3969/j.issn.1004-2644.2018.10.030.
Meng FY, Tang X, Chen MX, Wang Y, Li JX, Bao WL. Analysis of Neck Pain and Related Factors in Medical Students. J Kunming Med Univ. 2020;41(12):11–7. https://doi.org/10.12259/j.issn.2095-610X.S20201208.
Ye F, Wu LY, Su DH, Wu SY. Comparative study on neck and shoulder pain and its influencing factors between medical and non-medical college students. Chin J School Doctor. 2016;30(7):524–6.
Sun Z, Lei LJ, Liu P, Cheng QY, Shi JP, Li DF. Analysis of cervical vertebra health status and influencing factors of college students. Chin J Sch Health. 2019;40(4):631–3. https://doi.org/10.16835/j.cnki.1000-9817.2019.04.044.
Su JT, Zhao WZ, He YQ, Ge WM. Clinical features and prevention of university students’ cervical spondylosis. Chin J Sch Health. 2013;34(12):1470–2. https://doi.org/10.16835/j.cnki.1000-9817.2013.12.024.
Zhu XT, Xv LJ, Li GF, Liu SX. Investigation on the influencing factors of cervical spondylosis among college students of a higher vocational college in Beijing. Pract Prev Med. 2021;28(4):470–2. https://doi.org/10.3969/j.issn.1006-3110.2021.04.016.
Ren YC, Lin XG, Xie X, C YX. Status of cervical sub-health and its risk factors among college students. Chin J Sch Health. 2013;34(03):324–6+329. https://doi.org/10.16835/j.cnki.1000-9817.2013.03.023.
Wang CL, Yang CM, Yue JY, Lin CY, Chen SJ, Nie C, et al. Investigation and Analysis of Related Factors of 330 College Students’Sub-Health Cervical Spine. J Liaoning Med Univ. 2014;5:71–3. https://doi.org/10.13847/j.cnki.lnmu.2014.05.026.
Tian ZY, Ma Z, Liu XJ. Epidemiological status of cervical spine sub- health in college students and its influencing factors. Acta Acad Med Weifang. 2019;41(1):72–4. https://doi.org/10.16846/j.issn.1004-3101.2019.01.024.
Jing LN, Meng L, Zhang K, Zhang XW, Liu C. Research on the present situation and influencing factors of cervical vertebra sub-health of medical students. J Jining Med Univ. 2021;44(1):44–7. https://doi.org/10.3969/j.issn.1000-9760.2021.01.011.
Wang Z, Wang C, Yang L, Lu HF, Ren YY, Yang BB. Analysis of the current status and influencing factors of cervical spine sub-health of medical students. China Med Herald. 2021;18(12):69–73.
Hashim R, Salah A, Mayahi F, Haidary S. Prevalence of postural musculoskeletal symptoms among dental students in United Arab Emirates. BMC Musculoskelet Disord. 2021;22(1):30. https://doi.org/10.1186/s12891-020-03887-x.
Ayhualem S, Alamer A, Dabi SD, Bogale KG, Abebe AB, Chala MB. Burden of neck pain and associated factors among smart phone user students in University of Gondar, Ethiopia. PLoS One. 2021;16(9):e0256794. https://doi.org/10.1371/journal.pone.0256794.
Daher A, Halperin O. Association between Psychological Stress and Neck Pain among College Students during the Coronavirus Disease of 2019 Pandemic: A Questionnaire-Based Cross-Sectional Study. Healthcare (Basel). 2021;9(11):1526. https://doi.org/10.3390/healthcare9111526.
Behera P, Majumdar A, Revadi G, Santoshi JA, Nagar V, Mishra N. Neck pain among undergraduate medical students in a premier institute of central India: A cross-sectional study of prevalence and associated factors. J Family Med Prim Care. 2020;9(7):3574–81. https://doi.org/10.4103/jfmpc.jfmpc_206_20.
Dighriri YH, Akkur MA, Alharbi SA, Madkhali NA, Matabi KI, Mahfouz MS. Prevalence and associated factors of neck, shoulder, and low-back pains among medical students at Jazan University, Saudi Arabia: A cross-sectional study. J Family Med Prim Care. 2019;8(12):3826–31. https://doi.org/10.4103/jfmpc.jfmpc_721_19.
Haroon H, Mehmood S, Imtiaz F, Ali SA, Sarfraz M. Musculoskeletal pain and its associated risk factors among medical students of a public sector University in Karachi. Pakistan J Pak Med Assoc. 2018;68(4):682–8.
Algarni AD, Al-Saran Y, Al-Moawi A, Bin Dous A, Al-Ahaideb A, Kachanathu SJ. The Prevalence of and Factors Associated with Neck, Shoulder, and Low-Back Pains among Medical Students at University Hospitals in Central Saudi Arabia. Pain Res Treat. 2017;2017:1235706. https://doi.org/10.1155/2017/1235706.
Alshagga MA, Nimer AR, Yan LP, Ibrahim IA, Al-Ghamdi SS, Radman Al-Dubai SA. Prevalence and factors associated with neck, shoulder and low back pains among medical students in a Malaysian Medical College. BMC Res Notes. 2013;6:244. https://doi.org/10.1186/1756-0500-6-244.
Ndetan HT, Rupert RL, Bae S, Singh KP. Epidemiology of musculoskeletal injuries among students entering a chiropractic college. J Manipulative Physiol Ther. 2009;32(2):134–9. https://doi.org/10.1016/j.jmpt.2008.12.011.
Kanchanomai S, Janwantanakul P, Pensri P, Jiamjarasrangsi W. Risk factors for the onset and persistence of neck pain in undergraduate students: 1-year prospective cohort study. BMC Public Health. 2011;11:566. https://doi.org/10.1186/1471-2458-11-566.
Liu HT, Jin LY, Wang YG, Wang JY. X-ray signs and risk factors analysis of cervical spondylosis in college students. Chin J Sch Health. 2014;35(04):639–40. https://doi.org/10.16835/j.cnki.1000-9817.2014.04.066.
Zhang JL, Bao BB, Hua J. Analysis on the related factors of abnormal cervical curvature of college students. Chin J Sch Health. 2009;30(3):272–272.
Huang ZH, Sun Z, Xi W. Investigation on the prevalence and influencing factors of cervical spondylosis among college students in Shanxi Province. Chinese Remedies Clin. 2016;16(4):516–8. https://doi.org/10.11655/zgywylc2016.04.023.
Lin Y, Zhang X, Li H, Huang Y, Zhang W, Zhang C. Musculoskeletal pain is prevalent in Chinese medical and dental students: A cross-sectional study. Front Public Health. 2022;10:1046466. https://doi.org/10.3389/fpubh.2022.1046466.
Wah SW, Chatchawan U, Chatprem T, Puntumetakul R. Prevalence of Static Balance Impairment and Associated Factors of University Student Smartphone Users with Subclinical Neck Pain: Cross-Sectional Study. Int J Environ Res Public Health. 2022;19(17):10723. https://doi.org/10.3390/ijerph191710723.
Puntumetakul R, Chatprem T, Saiklang P, Phadungkit S, Kamruecha W, Sae-Jung S. Prevalence and Associated Factors of Clinical Myelopathy Signs in Smartphone-Using University Students with Neck Pain. Int J Environ Res Public Health. 2022;19(8):4890. https://doi.org/10.3390/ijerph19084890.
Hodačová L, Pilbauerová N, Čermáková E, Machač S, Schmidt J, Hodač J, et al. The Prevalence and Development of Neck and Lower Back Pain and Associated Factors in Dentistry Students-A Long-Term Prospective Study. Int J Environ Res Public Health. 2022;19(14):8539. https://doi.org/10.3390/ijerph19148539.
Keown GA, Tuchin PA. Workplace Factors Associated With Neck Pain Experienced by Computer Users: A Systematic Review. J Manipulative Physiol Ther. 2018;41(6):508–29. https://doi.org/10.1016/j.jmpt.2018.01.005.
Paksaichol A, Janwantanakul P, Purepong N, Pensri P, van der Beek AJ. Office workers’ risk factors for the development of non-specific neck pain: a systematic review of prospective cohort studies. Occup Environ Med. 2012;69(9):610–8. https://doi.org/10.1136/oemed-2011-100459.
Ye CQ, Ling MY, Yu DR, Zhang XY. Research progress on risk factors and rehabilitation of neck pain in military pilots. Med J Air Force. 2021;37(2):162–6. https://doi.org/10.3969/j.issn.2095-3402.2021.02.020.
Wirth B, Potthoff T, Rosser S, Humphreys BK, de Bruin ED. Physical risk factors for adolescent neck and mid back pain: a systematic review. Chiropr Man Therap. 2018;26:36. https://doi.org/10.1186/s12998-018-0206-y.
Linton SJ. A review of psychological risk factors in back and neck pain. Spine (Phila Pa 1976). 2000;25(9):1148–56. https://doi.org/10.1097/00007632-200005010-00017.
Ariëns GA, van Mechelen W, Bongers PM, Bouter LM, van der Wal G. Physical risk factors for neck pain. Scand J Work Environ Health. 2000;26(1):7–19. https://doi.org/10.5271/sjweh.504.
Jahre H, Grotle M, Smedbråten K, Dunn KM, Øiestad BE. Risk factors for non-specific neck pain in young adults A systematic review. BMC Musculoskelet Disord. 2020;21(1):366. https://doi.org/10.1186/s12891-020-03379-y.
Jun D, Zoe M, Johnston V, O’Leary S. Physical risk factors for developing non-specific neck pain in office workers: a systematic review and meta-analysis. Int Arch Occup Environ Health. 2017;90(5):373–410. https://doi.org/10.1007/s00420-017-1205-3.
Wallace JB, Newman PM, McGarvey A, Osmotherly PG, Spratford W, Gabbett TJ. Factors associated with neck pain in fighter aircrew: a systematic review and meta-analysis. Occup Environ Med. 2021;78(12):900–12. https://doi.org/10.1136/oemed-2020-107103.
Shiri R, Falah-Hassani K, Viikari-Juntura E, Coggon D. Leisure-time physical activity and sciatica: A systematic review and meta-analysis. Eur J Pain. 2016;20(10):1563–72. https://doi.org/10.1002/ejp.885.
Zhou J, Lv Q, Zhang H. Intervention status of active exercise therapy on cervical spondylosis. China Med Herald. 2016;13(4):50–2.
Yan SJ, Li XQ, Du Y, Yang L. Efficacy analysis of conventional massage combined with lower cervical resistanceexercise in thetreatment of cervical spondylosis. J Cervicodynia Lumbodynia. 2018;39(4):482–4. https://doi.org/10.3969/j.issn.1005-7234.2018.04.003.
Noriega DC, Kreuger A, Brotat M, Ardura F, Hernandez R, Muñoz MF, et al. Long-term outcome of the Cloward procedure for single-level cervical degenerative spondylosis.Clinical and radiological assessment after a 22-year mean follow-up. Acta Neurochir (Wien). 2013;155(12):2339–44. https://doi.org/10.1007/s00701-013-1902-y.
Nolet PS, Côté P, Cassidy JD, Carroll LJ. The association between a lifetime history of a work-related neck injury and future neck pain: a population based cohort study. J Manipulative Physiol Ther. 2011;34(6):348–55. https://doi.org/10.1016/j.jmpt.2011.06.006.
Acknowledgements
We would like to thank the National Natural Science Foundation of China for financial support.
Funding
This work was funded by General project of National Natural Science Foundation of China (grant numbers 81874501), Youth Project of National Natural Science Foundation of China (grant numbers 81904317) and Finance Department Project of Fujian Provincial (grant numbers 22SCZZX006). The funders had no role in study conception and design,data collection and analysis,decision making for publication,or writing of the manuscript.
Author information
Authors and Affiliations
Contributions
GYF, WSZ and LJP participate in research conception and design; GYF, CZM and CSQ collect and analyse data; GYF and LJP are responsible for methodology; GYF and CZM prepare manuscript draft; LJP and WSZ revise manuscript; All authors have read and approved the manuscript for publication.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary table 1. PRISMA check list .
Additional file 2:
Supplementary figure 1. Sensitivity analysis of risk factors for neck pain in college students (A:Improper use of the pillow, B:Improper sitting posture, C:Staying up late, D:High stress).
Additional file 3:
Supplementary table 2. Other risk factors for neck pain in college students.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gao, Y., Chen, Z., Chen, S. et al. Risk factors for neck pain in college students: a systematic review and meta-analysis. BMC Public Health 23, 1502 (2023). https://doi.org/10.1186/s12889-023-16212-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16212-7