
Abstract
Background
Pronolis®HD mono 2.5% is a novel, one-shot, high-density sterile viscoelastic solution, recently available in Spain, which contains a high amount of intermediate molecular weight hyaluronic acid (HA), highly concentrated (120 mg in 4.8 mL solution: 2.5%). The objective of the study was to analyze the efficacy and safety of this treatment in symptomatic primary knee osteoarthritis (OA).
Methods
This observational, prospective, multicenter, single-cohort study involved 166 patients with knee OA treated with a single-shot of Pronolis®HD mono 2.5% and followed up as many as 24 weeks.
Results
Compared with baseline, the score of the Western Ontario and McMaster Universities Arthritis Osteoarthritis Index (WOMAC) pain subscale reduced at the 12-week visit (primary endpoint, median: 9 interquartile range [IQR]: 7–11 versus median: 4; IQR: 2–6; p < 0.001). The percentage of patients achieving > 50% improvement in the pain subscale increased progressively from 37.9% (at 2 weeks) to 66.0% (at 24 weeks). Similarly, WOMAC scores for pain on walking, stiffness subscale, and functional capacity subscale showed significant reductions at the 12-week visit which were maintained up to the 24-week visit. The EuroQol visual analog scale score increased after 12 weeks (median: 60 versus 70). The need for rescue medication (analgesics/nonsteroidal anti-inflammatory drugs) also decreased in all post-injection visits. Three patients (1.6%) reported local adverse events (joint swelling) of mild intensity.
Conclusions
In conclusion, a single intra-articular injection of the high-density viscoelastic gel of HA was associated with pain reduction and relief of other symptoms in patients with knee OA.
Trial registration
ClinicalTrial# NCT04196764
Similar content being viewed by others


Background
Knee osteoarthritis (OA) is one of the most frequent causes of disability in elderly individuals [1]. The prevalence of symptomatic knee OA among men and women aged 60 or over is approximately 10% and 13%, respectively. However, the prevalence is increasing along with the raising of older and obese populations [2]. Knee OA is characterized by diverse pathophysiological changes, including decreased synovial fluid elastoviscosity and hyaluronan concentration [3]. The treatment of knee OA is mainly focused on the control of symptoms, especially pain [4]. Treatment guidelines recommend the use of nonoperative treatments before surgery [2]. The first approach for the relief of symptoms typically involves conservative therapies including exercise, physical therapy, and weight loss [2]. If it fails, analgesics (nonsteroidal anti-inflammatory drugs—NSAIDs -, or acetaminophen), symptomatic slow action drugs for osteoarthritis (SYSADOA; such as glucosamine, chondroitin), or intra-articular therapies (corticosteroids, hyaluronic acid -HA-, platelet-rich plasma) are commonly prescribed [5]. If none of those treatments work, joint replacement would be the final solution. Unfortunately, to date, there are no approved disease-modifying drugs for OA [6]. Although effective for pain relief, analgesics and NSAIDs are accompanied by adverse effects (AEs) [7]. A summary of different treatments for knee osteoarthritis is provided in Fig. 1.

Different available treatments for knee osteoarthritis
Regarding intra-articular injections with HA, they are getting attraction for the treatment of knee OA. Diverse randomized clinical trials have demonstrated the efficacy and safety of HA for the relief of symptoms in knee OA [8,9,10]. Bellamy et al., [8] in a Cochrane systematic review, evaluated the effects of diverse HA products for the treatment of knee OA in 76 randomized, controlled clinical trials. Pooled analyses versus placebo highlighted the efficacy of HA injections on pain, patient global assessment, and function after the injection, especially at the 5 to 13-week. Overall, the efficacy of HA injections was comparable with NSAIDs; however, the effect of HA injections was more durable than intra-articular corticosteroids. The HAs are frequently classified according to their molecular weight (MW): low (500–730 kDa), intermediate (800–2,000 kDa), or high (2,000–6,000 kDa) [11]. High-MWHAs have been associated with greater anti-inflammatory and proteoglycan synthesis effects, viscoelasticity maintenance, and joint lubrication. Comparative studies have revealed a greater improvement for pain relief with high-MWHAs than low-MWHAs and intra-articular placebo [12, 13]. In addition, high-MWHAs have been correlated to a higher percentage of AEs. Accordingly, injection site flare-ups with swelling, pain, and increased warmth [12, 14]. Overall, to minimize the risk of AEs, there is still a need for optimizing the HA treatment toward being single-shot and having a longer duration of action at the same time.
Pronolis®HD mono 2.5% (Procare Health, Spain/KD Intra-Articular® Gel 2.5%) is a novel, one-shot, high-density sterile viscoelastic solution, recently marketed in Spain, which contains a high amount of intermediate-MWHA, highly concentrated (120 mg in 4.8 mL solution: 2.5%) [15,16,17].
The objective of the present study was to analyze the efficacy and safety of a single-shot of this novel high-density viscoelastic gel of HA for the treatment of symptomatic primary knee OA.
Methods
Study design
This observational, prospective, multicenter, single-cohort study involved patients with knee OA who initiated treatment with Pronolis®HD mono 2.5% following manufacturer instructions (No-dolor study; ClinicalTrial# NCT04196764). A total of 29 healthcare centers from Spain (including Services of Rheumatology, Traumatology, Sports Medicine, and Pain Medicine) participated in the study. Main inclusion criteria were: adult men and women (aged over 18); with the diagnosis of primary knee OA, according to American College of Rheumatology criteria [18]; having performed a radiographic assessment of knee OA within the previous 18 months to study inclusion; showing a visual analog scale (VAS) score for pain ≥ 4 (out of 10) at study inclusion; having started treatment with Pronolis®HD mono 2.5% (prescribed as part of routine clinical practice) at the time of the study inclusion; and signing informed consent. Main exclusion criteria were: patients with intolerance to HA; hypersensitivity to intra-articular injections; infection in the knee joint; skin disorders or infections, either at the injection site or systemic; coagulation disorders that contraindicate the injection; prescription of intra-articular injections in both knees; diagnosis of autoimmune rheumatic diseases, connective tissue conditions, or microcrystalline disorders; and history of traumas in the knee joint; previous surgery in the knee joint. The complete list of inclusion and exclusion criteria is shown in Supplementary Table 1. The treatment consisted of a single-shot of Pronolis®HD mono 2.5% [14].
Endpoints and Measures
Patients were followed up for as many as 24 weeks. Visits were scheduled after 2, 4, 12, and 24 weeks of the injection. Visits were undergone in-person (face-to-face) at the hospital, except the 2-week visit that consisted of a phone call. The primary endpoint included the change of scores in the pain subscale from the Spanish version of the Western Ontario and McMaster Universities Arthritis Osteoarthritis Index (WOMAC) at the 12-week visit, compared with baseline. The minimal perceptible clinical improvement (MPCI) was analyzed by following the Ehrich et al. methodology [19]. OMERACT-OARSI rate of responders was calculated according to Pham et al. [20]. Secondary endpoints comprised the evaluation of pain (item evaluating pain on walking), joint stiffness, and functional capacity (by WOMAC subscales), the quality of life of patients, the need for rescue medication (analgesics/NSAIDs), the satisfaction with the treatment, and the development of AEs during the study period. Each WOMAC item was assessed with a 0–4 Likert scale, where 0 represented “none” and 4 indicated “very much”. The patient’s quality of life was determined at the 12-week visit by using the EuroQol-5D-5L (EQ-5D-5L) questionnaire [21]. The EQ-VAS is scored between 0 (the worst patient’s self-rated health) and 100 (the best). Satisfaction with the treatment was analyzed at all post-injection visits with a 1–5 Likert scale, where 1 represented “very satisfied” and 5 indicated “very unsatisfied”. Only patients with available data at the 12-week visit were considered for the efficacy analysis.
Determination of the sample size
The primary objective included score changes in the WOMAC pain subscale, from baseline. Studies by Zhang et al. [22] and Pavelka et al. [23] assumed 20 mm and 21 mm as a standard deviation (SD) of change, respectively, on a 100 mm VAS. Furthermore, Raynauld et al. [24] reported a mean change of -4.4 after 12 months of treatment, compared to baseline, using a Likert scale, and an SD of 3.9 (equivalent to 19.4 on a 100 mm VAS). Calculations estimated that a sample size of 270 patients could provide a precision of ± 2.4 mm (on 0–100 scale) for the change, with a 95% confidence interval (95%CI, confidence interval for one mean), an alpha of 0.05, and assuming an SD of 20 mm. Considering 10% of the loss to follow-up, the estimated number of patients to be recruited was 300. These estimations were carried out with PASS software (2011 version). Given the lack of available participants, the period of recruitment was extended from eight months (initially planned in the protocol) to one year and 10 months.
Statistical analysis
Categorical variables were expressed as absolute and relative frequencies; whereas continuous ones with the mean, SD, median, 95%CI, or interquartile range (IQR, i.e. percentile 25–75). Comparisons in variables between baseline and post-injection visits were performed using the paired-samples Student’s t-test or Wilcoxon test, when appropriate. Linear mixed models were used to calculate the estimation (95%CI) of the effect of the studied variables in the primary variable (WOMAC A at 12-week visit). Statistical significance was established when p < 0.05. All statistical procedures were carried out with SAS 9.4 software.
Results
Patient characteristics at baseline
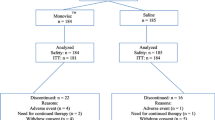
A total of 189 patients were initially recruited; however, 23 were not evaluable for the primary objective (Fig. 2). Patients were predominantly females (75.9% of total) and aged over 60 years (66.9%). Baseline sociodemographic and clinical characteristics of patients are shown in Table 1. Their mean age was 63.2 years (SD: 11.1). Considering the body mass index, 49.3% were overweight (25—< 30 kg/m2), 34.5% were obese (≥ 30 kg/m2), and 16.2% were normal weight (< 25 kg/m2). The mean time from the diagnosis of knee OA to the current HA treatment was 7.2 years (SD: 7.5). Regarding pain, 12.0% of patients considered to control adequately the pain, whereas 79.5% indicated that the treatment, followed to that time (baseline), was not enough for controlling the pain and living a normal life. A total of 150 patients (90.4%) completed the study, however 16 (9.6%) did not so. Information about the early discontinuation was available in seven of them (six due to lost to follow-up and one due to patient decision).

Flowchart of patients and design of the study
WOMAC results
Compared with baseline, the score of the WOMAC pain subscale was reduced at the 12-week visit (primary endpoint) in 4.78 points (95%CI: -5.4;—4.12) representing a mean relative reduction of 48.2% (95%CI: 41.4–55.0). No association was observed between this improvement and other variables relevant to WOMAC score (Supplementary Table 2). The median observed score for this variable was: 9 (IQR: 7–11) at the baseline visit versus 4 (IQR: 2–6) at the 12-week visit (Table 2 and Fig. 3). The percentage of patients achieving > 50% improvement in the pain subscale (with respect to baseline) increased from the 2-week (37.9%) to the 4-week (52.4%), 12-week (61.4%), and 24-week visits (66.0%; Supplementary Fig. 1). Similarly, scores for pain on walking item, stiffness subscale, and functional capacity subscale showed reductions at the 12-week visit (p < 0.001 in all; Table 2 and Fig. 3). Mean relative reductions were 47.1% (95%CI: 38.9–55.4), 45.9% (95%CI: 39.0–52.9), and 42.4% (95%CI: 36.0–48.9), respectively. A total of 61.5% of patients (for pain on walking item), 74.7% (for joint stiffness subscale), and 84.8% (for functional capacity subscale) achieved an improvement in WOMAC scores at the 12-week visit, compared with baseline. Furthermore, the clinical benefit in WOMAC pain, stiffness, functional capacity subscales, and pain on walking item was maintained up to the 24-week visit (Table 2). The complete information about efficacy outcomes, relative reductions, and change in WOMAC result at all post-injection visits compared with baseline are shown in Supplementary Tables 3-5. The treatment achieved a MPCI in all WOMAC subscales at the 12-week visit (Supplementary Table 6). The OMERACT-OARSI rate of responders at the 12-week visit was 72.9%.

Boxplots showing the evolution of WOMAC scores WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index The rhombus shows the mean value of the respective subscale/item. Asterisks represent statistical differences (Wilcoxon test) found with respect to baseline (p < 0.001). Data for WOMAC joint stiffness and functional capacity subscales at the 2-week visit were no collected.
Quality of life, rescue medication and patient satisfaction results
Scores from all dimensions in EQ-5D-5L reduced from baseline to the 12-week visit: mobility (median: 3, IQR: 2–3 at baseline versus median: 2, IQR: 1–3 at the 12-week visit; p < 0.001), self-care (median: 2, IQR: 1–3 versus median: 1, IQR: 1–2; p < 0.001), usual activities (median: 3, IQR: 2–3 versus median: 2, IQR: 1–2; p < 0.001), pain/discomfort (median: 3, IQR: 3–4 versus median: 2, IQR: 2–3; p < 0.001), and anxiety/depression (median: 2, IQR: 1–3 versus median: 1, IQR: 1–2; p < 0.001). Similarly, the EQ-VAS score increased after 12 weeks (median: 60, IQR: 40–75 versus median: 70, IQR: 60–85; p < 0.001). The need for rescue medication (analgesics/NSAIDs) also decreased in all post-injection visits (p = 0.007 at the 2-week and p < 0.001 at the remaining visits), compared with baseline (Fig. 4). Of patients, 56.6% were very satisfied or satisfied with the treatment at the 2-week visit. This percentage increased to 64.5%, 79.5%, and 82.7% at the 4-, 12-, and 24-week visits, respectively. Median scores for satisfaction were 2 (IQR: 2–3) in all post-injection visits.

Evolution of need for rescue medication during the post-injection visits McNemar test: * p = 0.007, ** p < 0.001
The safety profile of the treatment
Three patients (1.6%) reported 4 local AEs (joint swelling, n = 3; and ligament sprain, n = 1). None of the AEs was serious, and all of them were mild in severity. A total of 150 patients (90.4%) completed the study; however, 16 did not so. Loss to follow-up was the reason for early withdrawal in 6 out of 7 patients with available information (85.7%).
Discussion
In our study, the use of a novel high-density viscoelastic gel of HA has been associated with a clinical efficacy (in terms of pain relief) for patients with symptomatic knee OA. This benefit was achieved early (two weeks after the injection) and maintained for, at least, 24 weeks. In general, clinical improvement has been established with a minimum difference of 20% in efficacy outcomes [25], like scores in the WOMAC questionnaire. With the cautelous of involving different methodologies and HA gels among studies, our results agree with the literature implicating diverse HA products [8,9,10, 12, 26, 27]. For instance, Berenbaum et al., [24] in a randomized, double-blind, controlled trial compared the efficacy of 3-weekly injections between an intermediate- versus a low-MWHA in 426 patients with symptomatic knee OA. The decrease in WOMAC pain score at the 24-week (after the end of treatment) was significantly greater with the intermediate-MWHA preparation (mean: 22.9 mm, SD: 1.4) than the low one (mean: 18.4, SD: 1.5 mm). Moreover, the proportion of responders (OMERACT-OARSI criteria) with the intermediate-MWHA was also significantly higher (73% versus 58%). The percentage of patients reporting AEs was similar in both groups (35.2% versus 33.2%). Raman et al., [27] in a prospective, randomized, clinical trial compared the effectiveness of a high- versus low-MWHA in 392 patients with knee OA. Compared with baseline, scores in the WOMAC pain subscale at the 24-week post-injection visit were significantly lower with the high-MWHA (mean: 9.2 versus 5.1) than with the low one (mean: 8.8 versus 8.3). Nevertheless, the number of patients suffering from treatment-related AEs was higher with the high-MWHA (n = 39) than the low one (n = 30). In fact, one patient receiving the high- MWHA experienced a serious AE (pseudo-sepsis in the knee) and required hospitalization [27]. Our study also revealed the efficacy of the high-density viscoelastic gel of HA regarding pain on walking, joint stiffness, functional capacity, and quality of life, in agreement with previous studies [8,9,10, 12, 24]. Raynauld et al. [24], in a prospective, randomized, multicenter study compared the effectiveness of a high-MWHA product versus conventional care in 255 patients with knee OA. Changes at 12-month post-injections were significantly greater for the high-MWHA in WOMAC pain score (-38.4% versus -13.3% with conventional care), stiffness (-34.7% versus -10.4%), and physical function (-31.4% versus -14.5%). Nonetheless, the percentage of patients experiencing AEs was numerically greater with high-MWHA (96%) than conventional care (90%).
Overall, the efficacy of high-MWHA has been demonstrated to be superior to intermediate- and low-MWHA. Altman et al., [12] in a meta-analysis determined the efficacy of HA products according to their MW in 11 randomized clinical trials and 2,094 patients. Pooled efficacy results revealed a greater pain relief for high-MWHA (effect size: -0.52, 95%CI: -0.56 to -0.48) than intermediate- (effect size: -0.31, 95%CI: -0.42 to -0.20) and low-MWHA (effect size: -0.18, 95%CI: -0.19 to -0.17). By contrast, the percentage of AEs is also higher in products with high-MWHA [26, 27]. Reichenbach et al., [28] in a systematic review and meta-analysis, revealed a double risk for local AEs and post-injection flares with high-MW, cross-linked HA formulations than with intermediate- or low-MWHA preparations. In addition, pseudosceptic reactions (granulomatous inflammation of the synovium) have been reported in few cases, especially with cross-linked formulations of the highest-MWHA [9, 29]. In our study, only mild AEs were reported and were predominantly resolved within few days.
On the other hand, most HA preparations implicate between 3 and 5 injections, nevertheless, there are cross-linked formulations that require a single-shot, delivering the same HA dose as multi-injection preparations. Petterson et al., [30] in a multicenter, double-blind, randomized, placebo-controlled trial demonstrated the superior success rate (≥ 50% improvement and ≥ 20 mm absolute improvement, concerning baseline, in WOMAC pain subscale at the 26-week) with a 4-mL single HA injection than with saline. The clinically meaningful reduction of pain was evidenced within the 2-week post-injection. Although studies specifically designed are required, single-shots formulations of HA may also contribute to minimizing the risk for the development of AEs.
In our opinion, the notable results obtained in our study (presumably associated with the HA), especially the 48% reduction in WOMAC pain subscale, 66.0% of patients achieving more than 50% improvement in pain subscale, the early initiation of the clinical benefit (within 2 weeks), and its maintenance for a long-term period of time (24 weeks, at least), are greater than expected by an intermediate-MWHA preparation. These superior results might be associated with the high concentration and amount of HA, and thus to the high-density of the viscoelastic gel. In HA-based aqueous solutions, higher concentrations of HA are correlated (linear relationship) with higher densities of the viscoelastic solution [31, 32]. Therefore, it could be hypothesized that high-density viscoelastic gels of HA provide higher efficacy (similar to high-MWHA) while avoiding the higher incidence of AEs. To our knowledge, to date, none of the studies have specifically evaluated the value of HA products considering the density of the viscoelastic gel.
The main limitation of our study was the absence of a control or comparator group. Although the treatment of OA has an important placebo effect [33], and acknowledging that a control group would have strengthened the conclusions, results are in concordance with controlled studies, revealing a superior impact of HA injections. Another limitation was related to the limited sample size of the study (n = 166), not fulfilling the estimated one in the protocol (n = 300). Despite extending considerably the recruitment period, the availability of patients was insufficient. Yet, results found in our study are in concordance with other HA products [8,9,10, 12, 26, 27].
Conclusions
In conclusion, a single intra-articular injection of the high-density viscoelastic gel of HA was associated with pain reduction and relief of other symptoms in patients with knee OA. Further long-term studies, with a larger cohort of patients, and head-to-head non-inferiority analyses should be performed to corroborate the present results.
Authors' contributions
All authors contributed to the study conception and design, material preparation, data collection and analysis. All authors commented on previous versions of the manuscript and read and approved the final manuscript.
Availability of data and materials
The dataset(s) supporting the conclusions of this article is(are) included within the article (and its additional file(s)).
Abbreviations
- HA:
-
Hyaluronic acid
- IQR:
-
Interquartile Range
- MW:
-
Molecular weight
- NSAIDs:
-
Nonsteroidal anti-inflammatory drugs
- OA:
-
Osteoarthritis
- WOMAC:
-
The Western Ontario and McMaster Universities Osteoarthritis Index
References
Primorac D, Molnar V, Jeleč RE, Ž, Čukelj F, Matišić V, Vrdoljak T, Hudetz D, Hajsok H, Borić I,. Knee osteoarthritis: A review of pathogenesis and state-of-the-art non-operative therapeutic considerations. Genes (Basel). 2020;11:854. https://doi.org/10.3390/genes11080854.
Van Manen MD, Nace J, Mont MA. Management of primary knee osteoarthritis and indications for total knee arthroplasty for general practitioners. J Am Osteopath Assoc. 2012;112:709–15.
Vincent HK, Percival SS, Conrad BP, Seay AN, Montero C, Vincent KR. Hyaluronic acid (HA) viscosupplementation on synovial fluid inflammation in knee osteoarthritis: A pilot study. Open Orthop J. 2013;7:378–84. https://doi.org/10.2174/1874325001307010378.
Guermazi A, Neogi T, Kwoh KJN, CK, Conaghan PG, Felson DT, Roemer FW,. Intra-articular corticosteroid injections for the treatment of hip and knee osteoarthritis-related pain: Considerations and controversies with a focus on imaging-radiology scientific expert panel. Radiology. 2020;297:503–12. https://doi.org/10.1148/radiol.2020200771.
Vannabouathong C, Bhandari M, Bedi A, et al. Nonoperative treatments for knee osteoarthritis: An evaluation of treatment characteristics and the intra-articular placebo effect: A systematic review. JBJS Rev. 2018;6: e5. https://doi.org/10.2106/JBJS.RVW.17.00167.
Van Spil WE, Kubassova O, Boesen M, Bay-Jensen AC, Mobasheri A. Osteoarthritis phenotypes and novel therapeutic targets. Biochem Pharmacol. 2019;165:41–8. https://doi.org/10.1016/j.bcp.2019.02.037.
Zhang Q, Young L, Li F. Network meta-analysis of various nonpharmacological interventions on pain relief in older adults with osteoarthritis. Am J Phys Med Rehabil. 2019;98:469–78. https://doi.org/10.1097/PHM.0000000000001130.
Bellamy N, Campbell J, Robinson V, Gee T, Bourne R, Wells G (2006) Viscosupplementation for the treatment of osteoarthritis of the knee. Cochrane Database Syst Rev CD005321. https://doi.org/10.1002/14651858.CD005321.pub2
Maheu E, Rannou F, Reginster JY. Efficacy and safety of hyaluronic acid in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Semin Arthritis Rheum. 2016;45:S28-33. https://doi.org/10.1016/j.semarthrit.2015.11.008.
Hermans J, Bierma-Zeinstra SMA, Bos PK, Niesten DD, Verhaar JAN, Reijman M. The effectiveness of high molecular weight hyaluronic acid for knee osteoarthritis in patients in the working age: a randomised controlled trial. BMC Musculoskelet Disord. 2019;20:196. https://doi.org/10.1186/s12891-019-2546-8.
Testa G, Giardina SMC, Culmone A, Vescio A, Turchetta M, Cannavò PV. Intra-articular injections in knee osteoarthritis: A review of literature. J Funct Morphol Kinesiol. 2021;6:15. https://doi.org/10.3390/jfmk6010015.
Altman RD, Bedi A, Karlsson J, Sancheti P, Schemitsch E. Product differences in intra-articular hyaluronic acids for osteoarthritis of the knee. Am J Sports Med. 2016;44:2158–65. https://doi.org/10.1177/0363546515609599.
Hummer CD, Angst F, Ngai W, Whittington C, Yoon SS, Duarte L, Manitt C, Schemitsch E. High molecular weight Intraarticular hyaluronic acid for the treatment of knee osteoarthritis: a network meta-analysis. BMC Musculoskelet Disord. 2020;21:702. https://doi.org/10.1186/s12891-020-03729-w.
Hussain S, Rather H, Qayoom A. Efficacy, tolerability and adverse events of single-shot intra-articular hyaluronic acid injection in knee osteoarthritis. J Trauma Treat. 2015;4:1000256. https://doi.org/10.4172/2167-1222.1000256.
PronolisHD. Procare Health. Available from: https://www.pronolis.com/home Accessed: 29 August 2021
Monfort J, Combalia J, Emsellem C, Gaslain Y, Khorsandi D. Report Review: Pronolis HD®, the first high density hyaluronic acid gel for intra-articular in osteoarthritis: Complete and innovative range of viscosupplementation for all synovial joints. Available from: https://www.ecronicon.com/ecor/pdf/ECOR-09-00257.pdf Accessed: 29 August 2021
Balsalobre J, Combalia J, Emsellem C, Gaslain Y, Khorsandi D (2018) Effect of a monoshot injection of a high-density hyaluronic acid gel in patients with primary knee osteoarthritis. Preliminary results of the “No-Dolor” study. J Bone Res 6:2. https://doi.org/10.4172/2572-4916.1000189
Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, Christy W, Cooke TD, Greenwald R, Hochberg M, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986;29:1039–49. https://doi.org/10.1002/art.1780290816.
Ehrich EW, Davies GM, Watson DJ, Bolognese JA, Seidenberg BC, Bellamy N. Minimal perceptible clinical improvement with the Western Ontario and McMaster Universities osteoarthritis index questionnaire and global assessments in patients with osteoarthritis. J Rheumatol. 2000;27(11):2635–41.
Pham T, Van Der Heijde D, Lassere M, Altman RD, Anderson JJ, Bellamy N, Hochberg M, Simon L, Strand V, Woodworth T, Dougados M. Outcome variables for osteoarthritis clinical trials: The OMERACT-OARSI set of responder criteria. J Rheumatol. 2003;30(7):1648–54.
EuroQol Research Foundation. EQ-5D. Available from: https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/ Accessed: 29 August 2021
Zhang H, Zhang K, Zhang X, Zhu Z, Yan S, Sun T, Guo A, Jones J, Steen RG, Shan B, Zhang J, Lin J. Comparison of two hyaluronic acid formulations for safety and efficacy (CHASE) study in knee osteoarthritis: a multicenter, randomized, double-blind, 26-week non-inferiority trial comparing Durolane to Artz. Arthritis Res Ther. 2015;17:51. https://doi.org/10.1186/s13075-015-0557-x.
Pavelka K, Uebelhart D. Efficacy evaluation of highly purified intra-articular hyaluronic acid (Sinovial®) vs hylan G-F20 (Synvisc®) in the treatment of symptomatic knee osteoarthritis. A double-blind, controlled, randomized, parallel-group non-inferiority study. Osteoarthritis Cartilage. 2011;19:1294–300. https://doi.org/10.1016/j.joca.2011.07.016.
Raynauld JP, Torrance GW, Goldsmith BPA, CH, Tugwell P, Walker V, Schultz M, Bellamy N,. A prospective, randomized, pragmatic, health outcomes trial evaluating the incorporation of hylan G-F 20 into the treatment paradigm for patients with knee osteoarthritis (Part 1 of 2): clinical results. Osteoarthritis Cartilage. 2002;10:506–17. https://doi.org/10.1053/joca.2002.0798.
Rezende MR, Brito NLR, Farias FES, Silva CAC, Cernigoy CHA, Rodrigues da Silva JM, et al. Improved function and strength in patients with knee osteoarthritis as a result of adding a two-day educational program to usual care. Prospective randomized trial Osteoarthr Cartil Open. 2021;3: 100137. https://doi.org/10.1016/j.ocarto.2020.100137.
Berenbaum F, Grifka J, Cazzaniga S, D’Amato M, Giacovelli G, Chevalier X, Rannou F, Rovati LC, Maheu E. A randomised, double-blind, controlled trial comparing two intra-articular hyaluronic acid preparations differing by their molecular weight in symptomatic knee osteoarthritis. Ann Rheum Dis. 2012;71:1454–60. https://doi.org/10.1136/annrheumdis-2011-200972.
Raman R, Dutta A, Day N, Sharma HK, Shaw CJ, Johnson GV. Efficacy of Hylan G-F 20 and Sodium Hyaluronate in the treatment of osteoarthritis of the knee – a prospective randomized clinical trial. Knee. 2008;15:318–24. https://doi.org/10.1016/j.knee.2008.02.012.
Reichenbach S, Blank S, Rutjes AW, Shang A, King EA, Dieppe PA, Jüni P, Trelle S. Hylan versus hyaluronic acid for osteoarthritis of the knee: a systematic review and meta-analysis. Arthritis Rheum. 2007;57:1410–8. https://doi.org/10.1002/art.23103.
Chen AL, Desai P, Adler EM, Di Cesare PE. Granulomatous inflammation after Hylan G-F 20 viscosupplementation of the knee: a report of six cases. J Bone Joint Surg Am. 2002;84:1142–7.
Petterson SC, Plancher KD. Single intra-articular injection of lightly cross-linked hyaluronic acid reduces knee pain in symptomatic knee osteoarthritis: a multicenter, double-blind, randomized, placebo-controlled trial. Knee Surg Sports Traumatol Arthrosc. 2019;27:1992–2002. https://doi.org/10.1007/s00167-018-5114-0.
Kargerová A, Pekař M. Densitometry and ultrasound velocimetry of hyaluronan solutions in water and in sodium chloride solution. Carbohydr Polym. 2014;106:453–9. https://doi.org/10.1016/j.carbpol.2014.01.020.
Snetkov P, Zakharova K, Morozkina S, Olekhnovich R, Uspenskaya M. Hyaluronic acid: The influence of molecular weight on structural, physical, physico-chemical, and degradable properties of ciopolymer. Polymers (Basel). 2020;12:1800. https://doi.org/10.3390/polym12081800.
Zhang W. The powerful placebo effect in osteoarthritis. Clin Exp Rheumatol. 2019;37:118–23.
Acknowledgements
The authors thank all the investigators that collaborated in developing this project: Rafael Andrés Osuna González (Granada), Alejandro Muñoz Jiménez (Sevilla), Ana Conde Albarracín (Sevilla), Francisco José Lara Pulido (Sevilla), Manuel Romero Jurado (Córdoba), Mario León García (Badajoz), Jerónimo Balsalobre Aznar (Santa Cruz de Tenerife), José Luis Rosales Alexander (Santa Cruz de Tenerife), Artur Valls Elías (Barcelona), Christian Abel Schindler (Lleida), Eric Margalet Romero (Málaga), Rosa Cortes Bosh (Vilafranca del Penedés, Barcelona), Laia Orpinell Palacio (Barcelona), Pilar Santo Panero (Barcelona), Jone Llorente Onaindia (Barcelona), Francisco Manuel Moran Asensi (Alicante), Javier Mur Marín (Alicante), Jenaro Graña Gil (A Coruña), Adrián Barrera Flores (Madrid), Antonio González-Concheiro Santos (Pontevedra), Antonio Tristano Romano (Madrid), Carlos Horas Barrera (Santa Cruz de Tenerife), Carlos Tomás Simorte Moreno (Madrid), Rodrigo García Crespo (Madrid), Samantha Kanaffo Castelblanco (Madrid), Sara Arango Uribe (Madrid) and Silvia Pérez Alvarez (Madrid).
The authors would like to thank Pablo Vivanco from Meisys for the support in the medical writing of this manuscript and Procare Health Iberia SL for financially supporting the project and its total transparency in all proceedings.
Funding
This study was supported by Procare Health Iberia.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design, material preparation, data collection and analysis. All authors commented on previous versions of the manuscript and read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Hospital del Mar in Barcelona (CEIC-Parc de Salut Mar) and have been performed in accordance with the Declaration of Helsinki. Patients signed informed consent to participate in the study.
Consent for publication
Patients gave their consent for publication of the data included in the present study.
Competing interests
Authors declare: JC has received financial support from Procare Health for training sessions. DK has received research grants from Procare Health. LT declares no conflict of interest. JM has received financial support from Procare Health for scientific lectures and attending to medical congresses.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additiona file 1:Supplementary Figure 1
. Improvement in the painsubscale score of the Western Ontario and McMaster Universities ArthritisOsteoarthritis Index (WOMAC) at different post-injection visits with respect tothe baseline. Supplementary Table1. Inclusion and exclusioncriteria. Supplementary Table2. Linear mixed models fromvisit effect on WOMAC A absolute change, considering patient effect. Supplementary Table 3. Efficacy outcomesduring all post-injection visits. Supplementary Table 4. Relative reductions of WOMAC results at allpost-injection visits compared with baseline. Supplementary Table5. Changein WOMAC results at all post-injection visits compared with baseline. Supplementary Table6. Calculations to analyze theminimal perceptible clinical improvement** with the treatment at the 12-week visit
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Calvet, J., Khorsandi, D., Tío, L. et al. Evaluation of a single-shot of a high-density viscoelastic solution of hyaluronic acid in patients with symptomatic primary knee osteoarthritis: the no-dolor study. BMC Musculoskelet Disord 23, 442 (2022). https://doi.org/10.1186/s12891-022-05383-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05383-w