
Abstract
Background
Risk for non-contact anterior cruciate ligament (ACL) injury can be assessed based on drop vertical jump (DVJ). However, biomechanics of DVJ may differ with various sporting activities. The purpose of the present study was to clarify whether biomechanical features of DVJ are different among various sporting activities in female athletes.
Methods
A total of 42 female athletes, including 25 basketball, 8 soccer and 9 volleyball players, participated in the current investigation. DVJ was done for each female athlete using a three-dimensional motion analysis system which consisted of six cameras, two force plates and 46 retro-reflective markers. Kinematic and kinetic data were recorded for both limbs in each athlete. Simultaneously, frontal and sagittal plane views of the DVJ were recorded using two different high-resolution video cameras to evaluate Landing Error Scoring System (LESS) score. Three-dimensional biomechanical parameters at the knee joint and LESS were compared among three different sporting activities using ANOVA or Kruskal–Wallis test after confirming normality assumption. Thereafter post hoc Tukey or Steel–Dwass was utilized for multiple comparison.
Results
Soccer players had better LESS score, and peak knee flexion angle was significantly larger in soccer players compared to the other sports. In addition, knee abduction angle at initial contact (IC), peak knee abduction angle, knee internal rotation angle, and knee abduction moment within 40 ms from IC were significantly smaller in soccer players, compared to basketball players. In terms of volleyball players, knee abduction angle at IC and knee internal rotation angle at IC were significantly larger than soccer players, whereas no significant biomechanical differences were found between basketball and volleyball players.
Conclusions
From the present study, female basketball and volleyball players have worse LESS score, smaller peak knee flexion angle, greater knee abduction angle at IC and greater knee internal rotation angle at IC, compared to female soccer players. Thus, female basketball and volleyball players may have an increased risk of non-contact ACL injury during the jump-landing task, compared to soccer players. Biomechanics of DVJ depends on characteristics of the athlete's primary sport.
Similar content being viewed by others


Background
Non-contact anterior cruciate ligament (ACL) injuries are common especially for young female athletes. Clinically, non-contact ACL injuries include deceleration, lateral pivoting, or landing tasks which are associated with high external knee joint loads. According to previous literature, drop vertical jump (DVJ) can be a useful screening tool to evaluate the risk for non-contact ACL injury in female athletes [1]. For example, Hewett et al. suggested that female athletes with larger knee abduction angle at initial contact (IC), peak knee abduction angle, and peak knee abduction moment during DVJ would be prone to non-contact ACL injury [1]. The DVJ has thus been used to assess the risk for non-contact ACL injury in many subsequent studies [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17]. On the other hand, Krosshaug et al. indicated that DVJ could be a poor screening tool for non-contact ACL injuries from a prospective cohort study [18]. So far, the reason of this difference has been unknown. The participant in Hewett’s study were 205 female adolescent soccer, basketball, and volleyball players [1], whereas those in Krosshaug’s study were elite 372 handball players and 338 soccer players [18]. Therefore, primary sporting activities were different between these studies. Although it is controversial as to whether DVJ is an important screening tool for non-contact ACL injury, little attention has been paid to the biomechanical differences of DVJ among various sporting activities.
The purpose of the current study was to assess whether the characteristics of different sporting activities would affect the biomechanics of DVJ in female athletes. It was hypothesized that biomechanical features would depend on the athlete's primary sport.
Methods
Participants
A sample of convenience of 42 female collegiate athletes were enrolled in the present study. They were comprised of twenty-five basketball players, eight soccer players and nine volleyball players. Tegner activity scales were 7 to 9. All of subjects were members of college sports team and their practice was longer than 18 h a week. None of the athletes had any history of surgeries to the trunk and lower extremities based on musculoskeletal problems such as fracture, ligament rupture, and cartilage damage. Female athletes are known to have greater risk of non-contact ACL injury than male athletes [19, 20], and thus, females were chosen in the present study. A written informed consent form approved by Institutional Review Board of our university was obtained from each athlete.
Test procedures
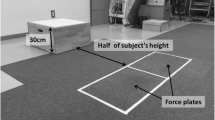
The jump-landing biomechanics during Drop Vertical Jump (DVJ) was examined. Participants were instructed to stand on top of the box with their feet shoulder width apart. Thereafter, they were instructed to drop off the box from a 30 cm high box forward to a distance of 50% of their height away from the box, land with one foot on each force plate, and then immediately upon landing jump as high as possible. Before data collection, instructions were given on how to perform DVJ. After performing DVJ several times as warm-ups, three successful trials were recorded for each athlete. DVJ was captured using a three-dimensional motion analysis system consisted of six cameras (120 frames/s; Oqus, Qualisys, Sweden) and two force plates (frequency 600 Hz; AM6110, Bertec, Columbus, OH, USA). The force plate collected ground reaction force (GRF) data at 600 Hz and were synchronized to the camera sampling rate of 120 Hz. The time at initial contact (IC) and toe-off (TO) from the jump was identified based on GRF data.
A total of 46 retro-reflective markers (14 mm in diameter) were placed on anatomic landmarks and specific locations. A set of anatomical landmarks were defined as follows; spinous process of vertebra at the level of C 7 and Th 10, jugular notch and xiphoid process of sternum, acromion, anterior superior and posterior superior iliac spine, greater trochanter, medial and lateral femoral epicondyles, medial and lateral malleoli, head of first and fifth metatarsal bone, scaphoid, and calcaneus. Additional specific markers were placed on the frontal and lateral aspects of thigh (4 markers) and shank (4 markers) [21, 22]. Marker trajectories were used to calculate joint centers and segment positions in standard quiet stance, and to track segment motion during the DVJ tests. Joint angles were calculated based on the cardan sequence of XYZ, equivalent to the joint coordinate system.
For each athlete, three-dimensional kinematic, kinetic and GRF data were assessed bilaterally during IC to TO. Marker movements were recorded by Qualisys Track Manager Software (version 2.7). To calculate biomechanical parameters at the knee joint, Visual 3D (C-motion Company, Rockville, MD) was used (Fig. 1). The following kinematic parameters were used: knee flexion angle at IC, peak knee flexion angle (IC-TO), knee abduction angle at IC, peak knee abduction angle (IC-TO), knee internal rotation angle at IC, and peak knee internal rotation angle (IC-TO). Knee internal rotation was defined as tibial rotation with respect to the femur. The following kinetic parameters were used: peak knee flexion, abduction, internal rotation moments within 40 ms from IC based on the previous study [21, 23]. Simultaneously, frontal and sagittal plane views of the DVJ were acquired using high resolution video cameras (120 frames/s; Oqus, Qualisys, Sweden) to evaluate Landing Error Scoring System (LESS) score.

Three-dimensional knee kinematics and kinetics were calculated during initial contact (IC) to Toe-off (TO) in DVJ
Statistical analysis
After Shapiro–Wilk test was performed to confirm normality assumption, ANOVA or Kruskal–Wallis test were used to compare biomechanical parameters between groups. Thereafter, post hoc Tukey or Steel–Dwass were used for multiple comparison. The statistical significance level was set at P = 0.05. Demographic data of athletes, kinematic and kinetic data were compared among groups. All statistical analyses were done with the Microsoft Excel Statistical Package, version 2015 (Social Survey Research Information, Tokyo).
Results
Athletes’ demographic data in each group are shown in Table 1. A total of 50 knees in 25 basketball players, 16 knees in 8 soccer players and 18 knees in 9 volleyball players, were analyzed. There were no significant differences among groups except for age. Soccer players were youngest among groups.
Kinematic and kinetic differences in each group are presented in Tables 2 and 3, respectively. LESS score was 4.8 ± 1.5 in basketball players, 3.3 ± 1.4 in soccer players, and 6.0 ± 2.8 in volleyball players. LESS score was significantly better in soccer players than in volleyball players (P = 0.009). In addition, in soccer players, peak knee flexion angle was significantly larger compared to basketball and volleyball players. Therefore, relative stiff landing (less knee flexion) was found in basketball and volleyball players. Moreover, knee abduction angle at IC, peak knee abduction angle, knee internal rotation angle at IC, and peak knee abduction moment within 40 ms from IC were significantly smaller in soccer players than in basketball players. In terms of volleyball players, knee abduction angle at IC and knee internal rotation angle at IC were significantly larger than soccer players, whereas no significant kinematic and kinetic differences were found between basketball and volleyball players.
Discussion
The results of the present study supported the hypothesis that biomechanical features during DVJ would depend on the athlete's primary sport. The most important finding of the current investigation was that female basketball and volleyball players were likely to perform stiff landing, compared to soccer players.
The LESS score can be evaluated using frontal and sagittal plane views of video data. Therefore, the score has clinically been shown to be a convenient assessment tool of jump-landing biomechanics. Currently, the score during DVJ has been used to evaluate the risk factor for ACL injury of female athletes. Padua et al. suggested that the LESS could be a valid and reliable tool for identifying potentially high-risk movement patterns during a jump-landing task [15], and 5 in LESS score was the optimal cut point, generating a sensitivity of 86% and a specificity of 64% for non-contact ACL injury [14]. In the present study, percentages of collegiate athletes with greater than 5 in the LESS were 64% (16/25) in basketball, 13% (1/8) in soccer, and 67% (6/9) in volleyball players, respectively. Therefore, the potential risk for non-contact ACL injury may be greater in female basketball and volleyball players, compared to soccer players.
Regarding DVJ as a screening test of non-contact ACL injury, controversy remains as described before. For instance, Hewett et al. reported that female athletes (205 female adolescent soccer, basketball, and volleyball players) with increased knee abduction angle or moment during DVJ would be prone to non-contact ACL injury [1]. However, Krosshaug et al. indicated that DVJ could be a poor screening test for ACL injuries in their prospective cohort study using elite 372 handball players and 338 soccer players, as knee abduction angle at IC, peak knee abduction moment, and peak knee flexion were not associated with the increased risk for ACL injury [18]. Although the true reason of this difference between these studies is unclear, absolute value of knee abduction moment during DVJ seemed to be greater in Hewett’s study than in Krosshaug’s study. Therefore, biomechanical features might be different based on participants' primary sport. Braun et al. assessed ACL biomechanical risk factors in female field hockey and lacrosse players to determine whether sport-specific posture might contribute to the increased incidence of ACL injury observed in lacrosse athletes [3]. They concluded that decreased knee flexion angle during landing, consistent with sport-specific playing postures, may contribute to the higher incidence of ACL injury in lacrosse players relative to field hockey. Similarly, from the present study, significant differences of kinematic and kinetic changes were found among three different sporting activities. In particular, less knee flexion was found during landing phase of DVJ in basketball and volleyball players, compared to soccer players.
Several limitations should be noted in the present study. First, the sample size was different for each sport. In particular, the sample sizes for soccer and volleyball were much smaller compared to basketball. Second, the present study was done using college athletes with Tegner activity scale 7 to 9. Thus, it is possible that the biomechanical parameters of high school or recreational athletes may be slightly different. Third, only three different sporting activities were included in the current study. The other kind of sports, like hockey, lacrosse, handball and so on, were still unknown. Lastly, although the risk of non-contact injury to the ACL was evaluated, the actual incidence of ACL injury could not be investigated. Nonetheless, the present results provide important information regarding the sport-specific characteristic of female knee kinematics and kinetics during jumping tasks.
Conclusion
The findings of this study showed that the biomechanics of DVJ depends on characteristics of the athlete's primary sport. In particular, female basketball and volleyball players are likely to perform a stiffer DVJ landing compared to soccer players, which may increase the risk of non-contact ACL injury in jumping tasks.
Availability of data and material
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- DVJ:
-
Drop vertical jump
- GRF:
-
Ground reaction force
- IC:
-
Initial contact
- LESS:
-
Landing error scoring system
- ms:
-
Milliseconds
- PKABDM:
-
Peak knee abduction moment
- PKFM:
-
Peak knee flexion moment
- PKIRM:
-
Peak knee internal rotation moment
- TO:
-
Toe-off
- vGRF:
-
Vertical ground reaction force
References
Hewett TE, Myer GD, Ford KR, Heidt RS Jr, Colosimo AJ, McLean SG, van den Bogert AJ, Paterno MV, Succop P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501.
Bates NA, Ford KR, Myer GD, Hewett TE. Timing differences in the generation of ground reaction forces between the initial and secondary landing phases of the drop vertical jump. Clin Biomech (Bristol, Avon). 2013;28(7):796–9.
Braun HJ, Shultz R, Malone M, Leatherwood WE, Silder A, Dragoo JL. Differences in ACL biomechanical risk factors between field hockey and lacrosse female athletes. Knee Surg Sports Traumatol Arthrosc. 2015;23(4):1065–70.
Cesar GM, Tomasevicz CL, Burnfield JM. Frontal plane comparison between drop jump and vertical jump: implications for the assessment of ACL risk of injury. Sports Biomech. 2016;15(4):440–9.
Dingenen B, Malfait B, Nijs S, Peers KH, Vereecken S, Verschueren SM, Staes FF. Can two-dimensional video analysis during single-leg drop vertical jumps help identify non-contact knee injury risk? A one-year prospective study. Clin Biomech (Bristol, Avon). 2015;30(8):781–7.
Dingenen B, Malfait B, Vanrenterghem J, Robinson MA, Verschueren SM, Staes FF. Can two-dimensional measured peak sagittal plane excursions during drop vertical jumps help identify three-dimensional measured joint moments? Knee. 2015;22(2):73–9.
Hewett TE, Myer GD, Kiefer AW, Ford KR. Longitudinal Increases in Knee Abduction Moments in Females during Adolescent Growth. Med Sci Sports Exerc. 2015;47(12):2579–85.
Husted RS, Bencke J, Andersen LL, Myklebust G, Kallemose T, Lauridsen HB, Holmich P, Aagaard P, Zebis MK. A comparison of hamstring muscle activity during different screening tests for non-contact ACL injury. Knee. 2016;23(3):362–6.
Malfait B, Sankey S, Firhad Raja Azidin RM, Deschamps K, Vanrenterghem J, Robinson MA, Staes F, Verschueren S. How reliable are lower-limb kinematics and kinetics during a drop vertical jump? Med Sci Sports Exerc. 2014;46(4):678–85.
Mueske NM, Patel AR, Pace JL, Zaslow TL, VandenBerg CD, Katzel MJ, Edison BR, Wren TAL: Improvements in landing biomechanics following anterior cruciate ligament reconstruction in adolescent athletes. Sports Biomech. 2020;19(6):738–49.
Munro A, Herrington L. The effect of videotape augmented feedback on drop jump landing strategy: Implications for anterior cruciate ligament and patellofemoral joint injury prevention. Knee. 2014;21(5):891–5.
Nichols JK, O’Reilly OM. Verifying the equivalence of representations of the knee joint moment vector from a drop vertical jump task. Knee. 2017;24(2):484–90.
Nyman E Jr, Armstrong CW. Real-time feedback during drop landing training improves subsequent frontal and sagittal plane knee kinematics. Clin Biomech (Bristol, Avon). 2015;30(9):988–94.
Padua DA, DiStefano LJ, Beutler AI, de la Motte SJ, DiStefano MJ, Marshall SW. The Landing Error Scoring System as a Screening Tool for an Anterior Cruciate Ligament Injury-Prevention Program in Elite-Youth Soccer Athletes. J Athl Train. 2015;50(6):589–95.
Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE Jr, Beutler AI. The Landing Error Scoring System (LESS) Is a valid and reliable clinical assessment tool of jump-landing biomechanics: The JUMP-ACL study. Am J Sports Med. 2009;37(10):1996–2002.
Satkunskiene D, Kamandulis S, Brazaitis M, Snieckus A, Skurvydas A: Effect of high volume stretch-shortening cycle exercise on vertical leg stiffness and jump performance. Sports Biomech. 2021;20(1):38–54.
Taylor JB, Nguyen AD, Shultz SJ, Ford KR: Hip biomechanics differ in responders and non-responders to an ACL injury prevention program. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1236–45.
Krosshaug T, Steffen K, Kristianslund E, Nilstad A, Mok KM, Myklebust G, Andersen TE, Holme I, Engebretsen L, Bahr R. The Vertical Drop Jump Is a Poor Screening Test for ACL Injuries in Female Elite Soccer and Handball Players: A Prospective Cohort Study of 710 Athletes. Am J Sports Med. 2016;44(4):874–83.
Hewett TE, Di Stasi SL, Myer GD. Current concepts for injury prevention in athletes after anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41(1):216–24.
Hewett TE, Ford KR, Hoogenboom BJ, Myer GD. Understanding and preventing acl injuries: current biomechanical and epidemiologic considerations - update 2010. N Am J Sports Phys Ther. 2010;5(4):234–51.
Harato K, Morishige Y, Niki Y, Kobayashi S, Nagura T. Fatigue and recovery have different effects on knee biomechanics of drop vertical jump between female collegiate and recreational athletes. J Orthop Surg Res. 2021;16(1):739.
Nishizawa K, Hashimoto T, Hakukawa S, Nagura T, Otani T, Harato K. Effects of foot progression angle on kinematics and kinetics of a cutting movement. J Exp Orthop. 2022;9(1):11.
Morishige Y, Harato K, Kobayashi S, Niki Y, Matsumoto M, Nakamura M, Nagura T. Difference in leg asymmetry between female collegiate athletes and recreational athletes during drop vertical jump. J Orthop Surg Res. 2019;14(1):424.
Acknowledgements
We acknowledge the contribution of the Keio female basketball team, Keio female soccer team, Keio Medical girls’ basketball team, Keio Medical girls’ volleyball team, Hiroo Osaki, Tomohiro Yanai, Keita Sonoda, Ryutaro Tanaka, Mayu Minemoto, Masayoshi Kurosawa, Rika Uchiyama, Ryuto Yoshida, Yuki Hoshi, Aiko Sakurai, Satoshi Imai, Ryoji Hayakawa and Sumi Yamashita for their help.
Funding
This study was not supported.
Author information
Authors and Affiliations
Contributions
KH and YM collected data and prepared the manuscript. KH and TK conceived and design the study and assisted with the statistical analysis. SK and YN developed the study design and interpretation of data. YN and TN assisted in the coordination of the study and manuscript preparation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the institutional review board of Keio University School of Medicine (IRB No. 20080054 and 20190116) and participants provided written informed consent to participate. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interest
None of the authors had any conflict of interest regarding this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Harato, K., Morishige, Y., Kobayashi, S. et al. Biomechanical features of drop vertical jump are different among various sporting activities. BMC Musculoskelet Disord 23, 331 (2022). https://doi.org/10.1186/s12891-022-05290-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05290-0