
Abstract
Background
Femoral posterior condylar offset (PCO) and posterior tibial slope (PTS) are important for postoperative range of motion after total knee arthroplasty (TKA). However, normative data of PCO and PTS and the correlation between them among healthy populations remain to be elucidated. The purpose of this study was to determine PCO and PTS in normal knees, and to identify the correlation between them.
Methods
Eighty healthy volunteers were recruited. CT scans were performed followed by three-dimensional reconstruction. PCO and PTS were measured and analyzed, as well as the correlation between them.
Results
PTS averaged 6.78° and 6.11°, on the medial and lateral side respectively (P = 0.002). Medial PCO was greater than lateral (29.2 vs. 23.8 mm, P < 0.001). Both medial and lateral PCO of male were larger than female. On the contrary, male medial PTS was smaller than female, while there was no significant difference of lateral PTS between genders. There was an inverse correlation between medial PCO and PTS, but not lateral.
Conclusions
Significant differences exhibited between medial and lateral compartments, genders, and among individuals. An inverse correlation exists between PCO and PTS in the medial compartment. These results improve our understanding of the morphology and biomechanics of normal knees, and subsequently for optimising prosthetic design and surgical techniques.
Similar content being viewed by others


Background
Total knee arthroplasty (TKA) is an effective procedure for advanced disorders of the knee joint, such as osteoarthritis [1]. It is important to reconstruct anatomical alignment of the operative limb during TKA procedures, to obtain maximum range of motion (ROM) [2]. Femoral posterior condylar offset (PCO) and sagittal posterior tibial slope (PTS) are two of the most important variables during TKA procedures, utilized to determine intra-operative osteotomy.
PCO is defined as the maximum thickness of posterior condyle projecting to the tangent of the posterior cortex of femoral shaft. PTS is the postero-caudal inclination of the tibial plateau in the sagittal plane. PCO and PTS may affect ROM during flexion in different ways [3,4,5,6]. A 3-mm decrease of PCO may reduce knee flexion by 10 degrees [6], and there is an increase of 2.6 degrees of flexion with each degree of PTS [5].
In order to avoid impingement between the posterior border of the tibial plateau and femur, PCO should be restored to avoid overresecting the posterior condyle during TKA [3, 4]. An appropriate PTS provides sufficient space during knee flexion to prevent the knee joint becoming too tight [5].
There have been investigations evaluating the importance of restoring PCO and PTS after TKA [7,8,9,10,11,12,13]. PCO and PTS counterbalance their respective effects on ROM and dynamic stability [6]. Thus the understanding of normative data of PCO and PTS is of critical importance. However, most of the publishded studies had focused on measuring PCO and PTS in knees with osteoarthritis. Currently there are few studies exploring PCO and PTS in knees without pathologic changes [8].
In our previous study, we have identified different PTS based on different referential axes [2]. As recently reported, PCO is not restored using standard instrumentation of different manufacturers, imparing pain and functional improvements after TKA [14]. Thus the current study further focused on the variability of PCO between medial and lateral condyles, and the correlation between PCO and PTS, based on multi-slice CT scans and 3D reconstructions of knee joints of healthy volunteers. These results will be benificial to TKA prosthesis design and selection, preoperative planning, and computer-assisted surgeries [15].
Methods
After approved by ethical committee (NFEC-2013-177) and written informed consents, healthy volunteers were recruited in this study. All the participants declared that they did not fit any of the following exclusion criteria: knee pain, deformity, abnormal movement, claudication, rheumatic fever, rickets, rheumatoid arthritis, osteoarthritis, fracture or previous surgeries. The sample size was calculated before the study, which revealed that a minimum of 61 cases was needed to establish 90% power.
CT scans and 3D reconstruction were conducted as described previously [2]. Briefly, 64-slice multi slice spiral CT scans were performed for all participants, from the femoral head to the heel of both lower limbs. Reconstructions were then performed using Mimics 10.01 software (MATERIALISE, Belgium).
PCO measurement was performed according to a published protocol [8]. First, transepicondylar axis (TEA) was defined as the line through the most prominent center of the femoral epicondyles in the axial plane. The true-sagittal plane (tsP) was defined as the sagittal plane perpendicular to TEA (Fig. 1) [16]. Two points located 5 cm apart, at the middle of the distal diaphyseal shaft were identified. The sagittal longitudinal axis of the femur was defined by the above two points [8], which was posteriorly shifted to tangent to posterior femoral cortex (Fig. 2a).

The anatomical transepicondylar axis (TEA) was defined as the straight line connecting the most prominent aspects of the medial and lateral epicondyle (orange line). The sagittal plane perpendicular to the TEA was defined as the true-sagittal plane (tsP) (green line)

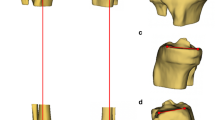
Measurement of posterior condylar offset (PCO). a translation of the sagittal longitudinal axis (fine arrow) to femoral posterior cortex (thick arrow). b translation of tsP (dotted line) alone TEA (dash-dot line). c PCO measurement using the largest circle fitting the peripheral border of the posterior condyle
Then along TEA, the tsP was moved laterally to the middle of the lateral condyle, and medially to the middle of the medial condyle, on which scan PCO measurements were performed (Fig. 2b). The largest circle fitting the peripheral border of the posterior condyle was determined. PCO was then determined by the vertical distance between the translated femoral axis and the foregoing circle (Fig. 2c).
As previously described [2], for PTS measurement, the sagittal axis and the tangential line of tibial plateau were used [17] (Fig. 3). Briefly, the tangential line of tibial plateau was defined as the line passing through the center and both the anterior and posterior edge. The sagittal axis was defined as the straight line connecting midpoints of outer cortical diameter at 5 and 15 cm distal to the knee joint. Then the PTS was determined by the angle between the two lines.

Measurement of sagittal posterior tibial slope (PTS). a confirmation of proximal tibial long axis (orange line) in tsP. b and c measurement of PTS, at medial and lateral side respectively
Forty cases were randomly selected, in which measurement was repeated twice by two authors in 1 month. The intraclass correlation coefficient (ICC) was applied to assess the reliability: 0.00 to 0.20, poor; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61to 0.80, substantial; and 0.81 to 1.00, perfect.
For statistical analysis, the data were tested for normality. Data in accordance with normal distribution were compared with paired (left and right) or unpaired (male and female) t-tests, otherwise non-parametric tests were applied. Pearson correlations were used to determine the relations between PCO and PTS. P-values< 0.05 were considered to be significant. SPSS 20.0 (IBM, USA) was used for the statistical analysis.
Results
A total of eighty healthy volunteers (40 males and 40 females) were recruited in this study, with an average age of 31.4 (20–45) years, average height of 167.3 (151–185) cm, and average weight of 60.0 (40–80) kg.
There were satisfactory measurements reliability with an ICC of 0.82 for medial PCO, 0.79 for lateral PCO, 0.93 for medial PTS and 0.80 for lateral PTS. Both PCO and PTS showed a normal distribution in the medial and lateral compartments. Medial PCO and PTS were greater than lateral ones regardless of genders. The mean PCO was 29.2 mm on the medial, and 23.8 mm on the lateral side (P < 0.001) (Fig. 4). The mean PTS was 6.78° and 6.11° on the medial and lateral side respectively (P = 0.002) (Fig. 4).

The distribution of PCO (left panel) and PTS (right panel) showing significant differences between medial and lateral compartment
There was no significant difference between left and right knee within the same individual (Table 1). Both medial and lateral PCO of male were larger than female (P < 0.001) (Table. 2). On the contrary, male medial PTS was smaller than female (P = 0.016), while there was no significant difference of lateral PTS between genders (Table 2).
In the medial compartment, an inverse correlation was detected between PCO and PTS (r = − 0.315; P = 0.026) (Fig. 5). However, no significant correlation was detected in the lateral compartment.

The linear correlation analysis between PCO and PTS in the medial (left panel) and lateral compartment (right panel)
Discussion
Conservation of the PCO and PTS has been regarded as a major factor to optimize ROM [6]. It was reported that decrease of PCO by 1 mm might result in a ROM reduction of 3.3–6.2° [5]. Correspondingly, each degree reduction in PTS might decrease ROM by 1.0–2.6° [4,5,6, 18]. Thus it is critical to understand the “normal” PCO and PTS.
PCO and PTS had been measured on conventional plain X-rays, which provides an acceptable level of accuracy under limited conditions [2]. As its imprecision can be impaired by magnification and incorrect positioning [19]. Thus, CT has been chosen as a more accurate method for measurement [20]. In our study, PCO and PTS were measured based on CT scans and 3D reconstruction, presenting differences between the medial and lateral sides which was neglected on plain radiographs [20, 21]. Further, the application of 3D reconstruction made it possible to rotate without restraint and to work in a straight forward way [2].
Gender difference has been suggested to be taken into consideration for designing knee prothesis [22]. Compared with female, male has significant greater PCO and smaller PTS in the medial compartment. As increased PCO or PTS are associated with increased ROM, and decreased PCO or PTS are associated with early tibiofemoral impingement [5], it is therefore reasonable to take this gender difference into account to obtain a maximum ROM and joint stability.
As for the relationship between medial PCO and PTS, Cinotti et al. [8] detected a significant correlation in the medial compartment but not in the lateral compartment, in magnetic resonance images. This correlation was attributed to anatomical structures: In the medial, the concave shape of the tibial plateau, the firm attachment between meniscus and tibia, and the tight medial collateral ligament, collaboratively generate a constrained articulation. While in the lateral compartment, greater laxity was exhibited due to the flatter shape of the tibial plateau, the greater mobility of the lateral meniscus and the lower tension of the lateral collateral ligament [23, 24]. However, our study demonstrated an inverse correlation between PCO and PTS in the medial compartment. Although currently we do not know the mechanism of this inverse correlation between medial PCO and PTS, the absence of meniscus during measurement, ethnic variation, and knees from healthy volunteers but not osteoarthritis patients may contribute to this finding. Consistent with our result, a previous cadaveric study [15] reported that the inverse correlation between PCO and PTS in the medial compartment, and assumed that this inverse correlation served as sagittal balance between flexion (increased PCO, increased PTS) and stability (decreased PCO, decreased PTS) [15].
PCO exhibited a variation coefficient of 8.3 and 9.2% on the medial and lateral side. And PTS showed a variation coefficient of 35.0 and 41.7% on the medial and lateral side, with the extreme values being − 0.3°and 14.99° respectively. This implies the complex anatomy features and asymmetric articular surface geometry of the knee which is necessary for physiologic motions [25, 26]. During TKA precudures, PCO should be conserved as much as possible to avoid an unbalanced knee in flexion. However, there is a trend in over-resection of the medial condyle and the under-resection of the lateral posterior condyle [14]. Thus the sagittal tibial cut during TKA should be performed parallel to the intrinsic tibial slope [6] but not perpendicular to the tibial sagittal mechanical axis [25] in patients with pronounced PCO to avoid a tight knee in flexion [15]. Further, current prosthetic design of the knee universally ignores the asymmetry articular surface, which may be the reasons for non-physiologic, paradoxical kinematics [26, 27]. Introducing asymmetry may allow advantages to control sagittal plane motion, thus the medial-pivot concept has been proved to have many advantages [28]. The medial-pivot TKA is characterized by equal radius of distal and posterior femoral condylar, and asymmetrical polyethylene insert [29]. Constraints on the medial side of the insert cause the medial compartment to act a pivot during movement in the sagittal plane. Thus, when the knee flexes, posterior translation of the femur is restricted to the unconstrained lateral compartment [29]. Clinically, according to a published meta-analysis, the pivot system presents better longevity and outcome than other systems [30].
The present study has several limitations: First, only volunteers from South China were included, whose measurements can not be widely generalized to all populations. However, these results will be useful to study ethnic variations. Second, the subjects were from young population (20–45 years old), rather than a wide range of ages. For this reason, these data were not influenced by pathologically altered bone (such as age-related degeneration) and help understanding kinematics of normal knees.
Conclusions
This study reports normative data of PCO and PTS in the knee joint. Differences were exhibited between medial and lateral compartments, genders, and among individuals. An inverse correlation exists between PCO and PTS in the medial compartment, probably serving as sagittal balance between flexion and stability. The results of this study improve our understanding of the morphology of normal knees. This is important for better understanding the biomechanics of the knee, and subsequently for optimising prosthetic design and surgical techniques. These represent potential areas for future research.
Availability of data and materials
The datasets during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PCO:
-
Posterior condylar offset
- PTS:
-
Posterior tibial slope
- TKA:
-
Total knee arthroplasty
- ROM:
-
Range of motion
- TEA:
-
Transepicondylar axis
- tsP:
-
True-sagittal plane
- ICC:
-
Intraclass correlation coefficient
References
Wang J, Zhu HL, Shi ZJ, Zhang Y. The application of Thromboelastography in understanding and Management of Ecchymosis after Total Knee Arthroplasty. J Arthroplast. 2018 Dec;33(12):3754–8. https://doi.org/10.1016/j.arth.2018.08.024.
Zhang Y, Wang J, Xiao J, Zhao L, Li ZH, Yan G, et al. Measurement and comparison of tibial posterior slope angle in different methods based on three-dimensional reconstruction. Knee. 2014 Jun;21(3):694–8. https://doi.org/10.1016/j.knee.2014.01.008.
Arabori M, Matsui N, Kuroda R, Mizuno K, Doita M, Kurosaka M, et al. Posterior condylar offset and flexion in posterior cruciate-retaining and posterior stabilized TKA. J Orthop Sci. 2008 Jan;13(1):46–50. https://doi.org/10.1007/s00776-007-1191-5.
Bellemans J, Banks S, Victor J, Vandenneucker H, Moemans A. Fluoroscopic analysis of the kinematics of deep flexion in total knee arthroplasty. Influence of posterior condylar offset. J Bone Joint Surg Br. 2002 Jan;84(1):50–3. https://doi.org/10.1302/0301-620X.84B1.0840050.
Malviya A, Lingard EA, Weir DJ, Deehan DJ. Predicting range of movement after knee replacement: the importance of posterior condylar offset and tibial slope. Knee Surg Sports Traumatol Arthrosc. 2009 May;17(5):491–8. https://doi.org/10.1007/s00167-008-0712-x.
Massin P, Gournay A. Optimization of the posterior condylar offset, tibial slope, and condylar roll-back in total knee arthroplasty. J Arthroplast. 2006 Sep;21(6):889–96. https://doi.org/10.1016/j.arth.2005.10.019.
Bauer T, Biau D, Colmar M, Poux X, Hardy P, Lortat-Jacob A. Influence of posterior condylar offset on knee flexion after cruciate-sacrificing mobile-bearing total knee replacement: a prospective analysis of 410 consecutive cases. Knee. 2010 Dec;17(6):375–80. https://doi.org/10.1016/j.knee.2009.11.001.
Cinotti G, Sessa P, Ripani FR, Postacchini R, Masciangelo R, Giannicola G. Correlation between posterior offset of femoral condyles and sagittal slope of the tibial plateau. J Anat. 2012 Nov;221(5):452–8. https://doi.org/10.1111/j.1469-7580.2012.01563.x.
Hashemi J, Chandrashekar N, Gill B, Beynnon BD, Slauterbeck JR, Schutt RC Jr, et al. The geometry of the tibial plateau and its influence on the biomechanics of the tibiofemoral joint. J Bone Joint Surg Am. 2008 Dec;90(12):2724–34. https://doi.org/10.2106/JBJS.G.01358.
Kang KT, Koh YG, Son J, Kwon OR, Lee JS, Kwon SK. A computational simulation study to determine the biomechanical influence of posterior condylar offset and tibial slope in cruciate retaining total knee arthroplasty. Bone Joint Res. 2018 Jan;7(1):69–78. https://doi.org/10.1302/2046-3758.71.BJR-2017-0143.R1.
Laskin RS, Riegèr MA. The surgical technique for performing a total knee replacement arthroplasty. Orthop Clin North Am. 1989;20(1):31–48.
Malek IA, Moorehead JD, Abiddin Z, Montgomery SC. The correlation between femoral condyle radii and subject height. Clin Anat. 2009 May;22(4):517–22. https://doi.org/10.1002/ca.20787.
Matsuda S, Miura H, Nagamine R, Urabe K, Ikenoue T, Okazaki K, et al. Posterior tibial slope in the normal and varus knee. Am J Knee Surg. 1999;12(3):165–8.
Wuertele N, Beckmann J, Meier M, Huth J, Fitz W. Posterior condylar resections in total knee arthroplasty: current standard instruments do not restore femoral condylar anatomy. Arch Orthop Trauma Surg. 2019;139(8):1141–7. https://doi.org/10.1007/s00402-019-03221-8.
Weinberg DS, Gebhart JJ, Wera GD. An Anatomic Investigation Into the Relationship Between Posterior Condylar Offset and Posterior Tibial Slope of One Thousand One Hundred Thirty-Eight Cadaveric Knees. J Arthroplasty. 2017;32(5):1659–1664.e1.
Balcarek P, Hosseini ASA, Streit U, Brodkorb TF, Walde TA. Sagittal magnetic resonance imaging-scan orientation significantly influences accuracy of femoral posterior condylar offset measurement. Arch Orthop Trauma Surg. 2018 Feb;138(2):267–72. https://doi.org/10.1007/s00402-017-2838-0.
Yoo JH, Chang CB, Shin KS, Seong SC, Kim TK. Anatomical references to assess the posterior tibial slope in total knee arthroplasty: a comparison of 5 anatomical axes. J Arthroplast. 2008 Jun;23(4):586–92. https://doi.org/10.1016/j.arth.2007.05.006.
Bellemans J, Robijns F, Duerinckx J, Banks S, Vandenneucker H. The influence of tibial slope on maximal flexion after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2005 Apr;13(3):193–6. https://doi.org/10.1007/s00167-004-0557-x.
Rubin PJ, Leyvraz PF, Aubaniac JM, Argenson JN, Estève P, de Roguin B. The morphology of the proximal femur. A three-dimensional radiographic analysis. J Bone Joint Surg Br. 1992;74(1):28–32.
Han HS, Chang CB, Seong SC, Lee S, Lee MC. Evaluation of anatomic references for tibial sagittal alignment in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2008 Apr;16(4):373–7. https://doi.org/10.1007/s00167-008-0486-1.
Voleti PB, Stephenson JW, Lotke PA, Lee GC. Plain radiographs underestimate the asymmetry of the posterior condylar offset of the knee compared with MRI. Clin Orthop Relat Res. 2014 Jan;472(1):155–61. https://doi.org/10.1007/s11999-013-2946-2.
Xie X, Zhong Y, Lin L, Li Q. No clinical benefit of gender-specific total knee arthroplasty: a systematic review and meta-analysis of 6 randomized controlled trials. Acta Orthop. 2015 Apr;86(2):274–5. https://doi.org/10.3109/17453674.2015.1022107.
Deep K. Collateral ligament laxity in knees: what is normal? Clin Orthop Relat Res. 2014 Nov;472(11):3426–31. https://doi.org/10.1007/s11999-014-3865-6.
Victor J, Bellemans J. Physiologic kinematics as a concept for better flexion in TKA. Clin Orthop Relat Res. 2006 Nov;452:53–8. https://doi.org/10.1097/01.blo.0000238792.36725.1e.
Bai B, Baez J, Testa N, Kummer FJ. Effect of posterior cut angle on tibial component loading. J Arthroplast. 2000 Oct;15(7):916–20. https://doi.org/10.1054/arth.2000.9058.
Ranawat CS, Komistek RD, Rodriguez JA, Dennis DA, Anderle M. In vivo kinematics for fixed and mobile-bearing posterior stabilized knee prostheses. Clin Orthop Relat Res. 2004 Jan;418:184–90. https://doi.org/10.1097/00003086-200401000-00030.
Stiehl JB, Komistek RD, Cloutier JM, Dennis DA. The cruciate ligaments in total knee arthroplasty: a kinematic analysis of 2 total knee arthroplasties. J Arthroplast. 2000 Aug;15(5):545–50. https://doi.org/10.1054/arth.2000.4638.
Minoda Y, Kobayashi A, Iwaki H, Miyaguchi M, Kadoya Y, Ohashi H, et al. Polyethylene wear particles in synovial fluid after total knee arthroplasty. Clin Orthop Relat Res. 2003 May;410:165–72. https://doi.org/10.1097/01.blo.0000063122.39522.c2.
Iwaki H, Pinskerova V, Freeman MA. Tibiofemoral movement 1: the shapes and relative movements of the femur and tibia in the unloaded cadaver knee. J Bone Joint Surg Br. 2000;82(8):1189–95. https://doi.org/10.1302/0301-620X.82B8.0821189.
Fitch DA, Sedacki K, Yang Y. Mid- to long-term outcomes of a medial-pivot system for primary total knee replacement: a systematic review and meta-analysis. Bone Joint Res. 2014 Oct;3(10):297–304. https://doi.org/10.1302/2046-3758.310.2000290.
Acknowledgements
None.
Funding
Writing and revision of the manuscript were supported by the grants from the Natural Science Foundation of Guangdong Province (2021A1515011628), Science and Technology Program of Guangzhou (202102020957). The data collection and analysis were supported by the National Natural Science Foundation of China (No.81873763).
Author information
Authors and Affiliations
Contributions
ZY designed this study. ZY, RS and WJ finished the manuscript. BL revised the manuscript. BL, RS and SZ collected and analyzed the data. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the IRB of Nanfang Hospital (NFEC-2013-177). Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bao, L., Rong, S., Shi, Z. et al. Measurement of femoral posterior condylar offset and posterior tibial slope in normal knees based on 3D reconstruction. BMC Musculoskelet Disord 22, 486 (2021). https://doi.org/10.1186/s12891-021-04367-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-021-04367-6