
Abstract
Background
Patients with chronic obstructive pulmonary disease (COPD) often require hospital readmission because of exacerbation of their condition. These frequent exacerbations reduce quality of life, work performance, and emotional health. However, few studies have investigated the risk factors for readmission and readmission rates in Asian patients with COPD. We conducted a systematic review to identify and understand the major risk factors for readmission in patients with COPD in Asia and the readmission rate.
Method
We searched PubMed, MEDLINE, Embase, China National Knowledge Infrastructure, Wanfang Data Knowledge Service Platform, and China Biomedical Literature Database from database inception to September 2023 to identify studies on the readmission rate and risk factors for COPD in Asian patients. Chinese search terms included “COPD,” “chronic obstructive pulmonary disease,” “risk factors,” “recurrence,” “readmission,” and “acute exacerbation.” English search terms included “chronic obstructive pulmonary disease,” “COPD,” “lung emphysema,” “hospital admission,” “patient readmission,” and “readmission.” We extracted first author, publication year, research area, sample size, sex, risk factors, and readmission rates. The included studies’ quality was evaluated using the Agency of Healthcare Research and Quality. Meta-synthesis was conducted on readmission rates and risk factors for readmission. Subgroups were formed by age, research area, sample size, and research type, and meta-regression analysis was conducted on the 30-day, 90-day, and 365-day readmission rates of patients to determine the source of heterogeneity. Finally, the results’ robustness was evaluated using sensitivity analysis. Begg and Egger tests were used to evaluate publication bias.
Results
Meta-analysis of 44 studies, with 169,255 participants, indicated that risk factors for COPD readmission in Asia included: history of multiple hospital admissions, ≥ 3 comorbidities, male sex, ratio of eosinophils percentage ≥ 2%, body mass index < 18.5, smoking history, pulmonary heart disease comorbidity, COPD assessment test score > 20, nutritional disorder, Neutrophil-to-Lymphocyte ratio > 7, and FEV1 < 50. The 30-, 90-, and 365-day readmission rates of patients were 19%, 31%, and 42%, respectively.
Conclusions
Patients with COPD in Asia generally have high readmission rates and different risk factors. To reduce healthcare, economic, and social burdens, interventions should address major risk factors, early prevention, and screening.
Similar content being viewed by others

Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by progressive airflow restriction and decreased lung function. According to the Global Burden of Disease Study [1], approximately 600 million people worldwide have COPD. Meanwhile, mortality attributed to COPD has shown an increasing trend and has become the third leading cause of death globally. The frequent exacerbation of COPD can greatly reduce quality of life and seriously affect the work performance and emotional health of patients. Moreover, repeated acute COPD exacerbations are closely associated with increased mortality. An earlier study [2] reported that a new exacerbation of COPD significantly increases the risk of subsequent exacerbations; specifically, patients were 25 times more likely to be readmitted after their 10th COPD hospital admission than after their first COPD admission.Patients with COPD may be hospitalized repeatedly owing to worsening respiratory symptoms, which poses a significant economic and social burden on medical resources and society as a whole. Currently, the top ten countries with the highest number of patients with COPD (China, India, Indonesia, the United States, Bangladesh, Japan, Pakistan, Russia, Vietnam, and Germany) have reported a total of 25.54 billion cases (65.2% of the world’s total). Asia accounts for a large proportion of COPD cases [3], but there is currently a lack of research on the readmission rate and risk factors for COPD in Asia. Although understanding of the risk factors for COPD readmission has improved, existing investigations have primarily focused on populations in Europe and North America [4], while research targeting Asian populations is rare. In this context, this study systematically retrieved related studies on the risk factors for COPD and readmission rates in Asia to provide insights to help inform clinical interventions.
Material and methods
Literature Search Strategy
A systematic literature search was conducted using PubMed, Medline, Embase, China National Knowledge Infrastructure, Wanfang Data, and SinoMed databases from inception to September 2023 to identify studies focusing on the readmission rate and risk factors for COPD in Asia. The search strategy adopted a combination of subjects and free words. The Chinese search terms included “COPD,” “chronic obstructive pulmonary disease,” “risk factors,” “recurrence,” “readmission,” and “acute exacerbation”; the English search terms included “chronic obstructive pulmonary disease,” “COPD,” “lung emphysema,” “hospital admission,” “patient readmission,” and “readmission.” Taking MEDLINE as an example, the specific search strategy is presented in Table 1.
Inclusion and exclusion criteria
The inclusion criteria were (1) Studies with COPD as the primary diagnosis for readmission and (2) Studies focusing on the readmission rate, risk factors, and predictive factors for COPD. The exclusion criteria were (1) Conference abstracts, editorial reports and letters, master’s dissertations or comments, and duplicate publications; (2) Studies describing the implementation of interventions or programs beyond routine care; and (3) Studies conducted outside Asia.
Literature screening and data extraction
Two researchers independently screened the studies retrieved from a preliminary literature search based on the inclusion and exclusion criteria and extracted the desired data. Subsequently, a cross-check was conducted. Any disputes were resolved by consulting a third researcher. During the literature search, unrelated studies were excluded by examining titles and abstracts. Subsequently, full texts of the remaining studies were reviewed to determine the final inclusion criteria. The main data extracted included the first author, year of publication, region of research, sample size, gender ratio, risk factors, and readmission rate.
Quality assessment
The risk of bias of each study was assessed based on the cross-sectional study evaluation criteria recommended by the Agency of Healthcare Research and Quality in the U.S., which consists of 11 items. Each item was answered as “yes” (score 1), “no” (score 0), or “unclear” (score 0), resulting in a maximum score of 11 points. A study was rated as low quality if it received a score of 0–3, moderate quality if it received a score of 4–7, and high quality if it received a score of 8–11.
Statistical method
In this study, meta-analysis was conducted using Stata 17.0, and the effect statistics were set as the readmission rate and 95% CI. Heterogeneity of the research results was determined using I2. A low level of heterogeneity was indicated if I2 < 50% and P > 0.10, and a fixed-effects model was used for meta-analysis; otherwise, a random-effects model was used. Subsequently, parallel meta-regression to find sources of heterogeneity in the readmission rate of patients with COPD was conducted according to age, study area, sample size, and research subgroups, at 30, 90, and 365 days. P < 0.05 was considered statistically significant, and sensitivity analysis was performed to determine whether the results of COPD readmission rates in Asia were robust. Finally, the publication bias of the included studies was assessed using the Begg and Egger tests.
Results
Literature screening
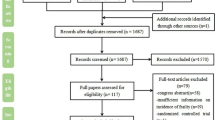
A preliminary literature search of the Chinese and English databases yielded 29,840 relevant articles. After screening the titles and abstracts, 400 studies met our criteria for further review. After full-text review and quality assessment, 44 articles were included in our meta-analysis. A literature screening flowchart is shown in Fig. 1.

Literature screening flow and results
Study characteristics and risk of bias assessment
The 44 studies [5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48] included a total sample size of 169,255 individuals. The basic study characteristics and risk-of-bias assessment results are summarized in Table 2.
Meta-analysis results
Meta-analysis results for risk factors for COPD readmission
Thirty-nine studies reported the risk factors for COPD readmission. The meta-analysis identified a total of 11 risk factors with statistical significance, namely history of ≥ 2 hospital admissions (OR: 2.8; 95% CI: 1.96–4.27; P < 0.001), ≥ 3 comorbidities (OR: 1.17; 95% CI: 1.05–1.31; P = 0.005), male sex (OR: 1.56; 95% CI: 1.25–1.94; P < 0.001), ratio of eosinophils percentage (EOS%) ≥ 2% (OR: 3.01; 95% CI: 1.87, 4.85; P < 0.001), body mass index (BMI) < 18.5 (OR: 3.51; 95% CI: 2.24–5.0; P < 0.001), smoking history (OR: 1.9; 95% CI: 1.37–2.64; P < 0.001), pulmonary heart disease comorbidity (OR: 2.71; 95% CI: 1.82–4.02; P < 0.001), COPD assessment test (CAT) score > 20 (OR: 1.43; 95% CI: 1.15–17.78; P = 0.001), nutritional disorder (OR: 2.93; 95% CI: 2.17–3.96; P < 0.001), Neutrophil-to-Lymphocyte ratio (NLR) > 7 (OR: 1.93; 95% CI: 1.35–2.77; P < 0.001), and FEV1 < 50 (OR: 2.43; 95% CI: 1.6–3.67; P < 0.001). In contrast, a high education level was identified as a protective factor (OR: 0.73; 95% CI: 0.59–0.89; P < 0.05). Additionally, comorbidities of diabetes, coronary heart disease, congestive heart failure, and PaCO2 ≥ 50 had no statistical significance (P > 0.05). The details are presented in Table 3.
Readmission rate for persons with COPD in Asia
In 17 studies, the 30-day readmission rate for persons with COPD ranged from 6% to 39%; in 10 studies, the 90-day readmission rate ranged from 16% to 61%; and in 11 studies, the 365-day readmission rate ranged from 29% to 53%. The combined 30-, 90-, and 365-day readmission rates were 19% (95% CI: 0.15–0.22; I2 = 99.8%), 31% (95% CI: 0.19–0.43; I2 = 98.3%), and 42% (95% CI: 0.37–0.47; I2 = 85.2%), respectively (Figs. 2, 3, 4).

Forest plot of 30 day readmission rate for COPD

Forest plot of 90 day readmission rate for COPD

Forest plot of 365 day readmission rate for COPD in Asia
Sensitivity analysis
Sensitivity analysis was performed by removing one study at a time. No abnormal values were found in the 30-, 90-, and 365-day readmission rates of Asian patients with COPD, indicating that the meta-analysis results were robust and reliable (Figs. 5, 6, 7).

Sensitivity analysis of included studies on 30-day readmission rate for COPD in Asia

Sensitivity analysis of included studies on 90 day readmission rate for COPD in Asia

Sensitivity analysis of included studies on 365 day readmission rate for COPD in Asia
Subgroup analyses
Owing to the high heterogeneity among the included studies, subgroup analyses were conducted by age, region of research, sample size, investigation area, and study type. As the level of heterogeneity remained significant in the subgroups, a random-effects model was used for the meta-analysis. The results showed that: (1) Regarding the region of research, the 30- and 90-day readmission rates of patients with COPD in China were 20% and 26%, respectively, and the 365-day readmission rates in southern and northern China were 39% and 45%, respectively. (2) Regarding study type, the 30-, 90-, and 365-day readmission rates were 18%, 38%, and 40%, respectively, in retrospective studies, and 22%, 23%, and 43%, respectively, in prospective studies. (3) Regarding sample size, the 30-, 90-, and 365-day readmission rates in studies with a sample size of 0–499 were 21%, 27%, and 43%, respectively, whereas the 30-day readmission rates in studies with a sample size of 500–999, 1000–10000, and ≥10000 were 14%, 20%, and 18%, respectively. (4) Regarding age, the 30-, 90-, and 365-day readmission rates of patients with COPD aged 60–69 years were 21%, 32%, and 45%, respectively; the 30-, 90-, and 365-day readmission rates of patients with COPD aged 70–79 years were 21%, 32%, and 45%, respectively; and the 30-day readmission rate of patients with COPD aged ≥80 years was 6%. Meta-regression analysis was performed to further explore the sources of heterogeneity. There were differences in the 30-day readmission rate in the age subgroup, the 90-day readmission rate in the research and sample size subgroups, and the 365-day readmission rate in the age subgroup (Table 4).
Publication bias
Funnel plots were drawn for 30-, 90-, and 365-day COPD readmission rates in Asia. The symmetry of the distribution was generally poor. However, the results of the Egger and Begg tests suggested no significant publication bias in the 30-day (P = 0.528 and P = 0.967), 90-day (P = 0.123 and P = 0.474), and 365-day (P = 0.075 and P = 0.436) readmission rates (Figs. 8, 9, 10).

Funnel plot of 30 day readmission rate for COPD in Asia

Funnel plot of 90 day readmission rate for COPD in Asia

Funnel plot of 365 day readmission rate for COPD in Asia
Discussion
The meta-analysis results of this study showed that among patients with COPD, readmission rates at 30, 90, and 365 days were 19%, 31%, and 42%, respectively. In a systematic review, Alqahtani et al [4] found that patients with COPD 30 and 90 days following the acute aggravation period had readmission rates of 8.8%-26%, 17.5%-39%, respectively. The results are similar to those of the current study, but the prior study considered only three areas in Asia and did not execute a meta-analysis of readmission rate on different days. The readmission rate range is relatively wide and rather poor, owing to acute exacerbation readmission in patients with COPD in Asia. Another review [49] of 42 studies, including three from Asia, found that patients with COPD had readmission rates 30, 60, 90, 180, and 365 days following acute aggravation of 11%, 17%, 17%, 30%, and 37%, respectively. This may [49] be contrasted with a study of Asian patients with COPD at 30, 90, and 365 days; the readmission rate was higher, showing that in patients with COPD in Asia, exacerbations repeatedly occur; this should not be ignored by Asian hospitals.
Regarding risk factors of readmission, Ruan et al [49] found that male sex, number of hospitalizations in the previous year, length of hospital stay, heart failure, tumor and other cancers, and diabetes and its complications were risk factors for readmission in patients with COPD, while obesity was a protective factor. Visible risk factors include male sex, history of hospitalization, and lower BMI. The difference is in the impact of comorbidities: This study found that only when the number of comorbidities was ≥3 was there a risk factor; the presence of a single disease was not a risk factor, but cor pulmonale was one risk factor. We believe that acute exacerbation of COPD is a complex process that may be affected by many factors, including comorbidities, environmental factors, and lifestyle. When a certain number of complications is exceeded, such as three or higher, there may be a cumulative effect; namely, the combination of complications in patients with multiple diseases increases the risk of exacerbations. This effect may not be a simple linear relationship but rather a result of the interaction of multiple factors. Cor pulmonale may directly affect heart function and, thus, have a direct impact on the acute exacerbation of COPD. Even if the number of comorbidities is low, the presence of cor pulmonale may significantly increase the risk of acute exacerbations.
The reason men are exposed to a higher risk of COPD than women may be related to higher smoking rates in men. Smoking is an important factor in the occurrence, development, and readmission of patients with COPD. This may be because tobacco can induce systemic inflammation, impair endothelial function, and exert oxidative stress on the human body, which have sustained impacts on lung structure, respiratory immune function, and lung function. We also found that comorbidity with pulmonary heart disease and ≥ 3 comorbidities were closely related to COPD readmission. This is consistent with Chen et al. [41], who indicated that the average probability of COPD readmission within one month after discharge for patients with cardiovascular disease, diabetes, or bronchial asthma was nearly twice as high as that for patients without comorbidities. Spece et al. [50] found that for every one percent increase in the comorbidity index, the risk of readmission or death increased by 24%. Furthermore, malnutrition is an important factor that affects prognosis and is associated with a significantly increased risk of 30-day readmission. Consistently, BMI < 18.5, was also indicated as a risk factor for COPD readmission. Therefore, patients with COPD should maintain good nutritional status to reduce the risk of readmission. Moreover, it has been reported that multiple acute hospital admissions due to acute COPD attacks in the previous year is a key risk factor for readmission. Two earlier studies [51, 52] found that the risk of 30-day readmission in patients with COPD who had a history of repeated deterioration and those who had a history of hospital admission in the previous year was significantly increased by 53–54% and 60–64%, respectively. Additionally, we also found that NLR > 7, EOS% ≥ 2%, and FEV1 < 50 were risk factors for COPD readmission in Asia, which may be related to worse lung conditions and poor treatment for severe pulmonary infections.
This meta-analysis included 44 studies. The results showed that the 30-, 90-, and 365-day readmission rates of patients with COPD in Asia were 19%, 31%, and 42%, respectively. Alqahtani et al. [4] reported that the incidence of readmission during acute COPD was 2.6–82.2% at 30 days, 11.8–44.8% at 31–90 days, 17.9–63.0% at 180 days, and 25.0–87.0% at 365 days after discharge. These data are consistent with our results. In the age subgroup analysis, we noticed that the age group of 60–69 years was associated with the highest 30-, 90-, and 365-day readmission rates, while the age groups of 70–79 years and ≥ 80 years had lower readmission rates. This may be because older patients have more serious underlying diseases and may die outside the hospital (such as at home or in a nursing home), resulting in no readmission. Further, subgroup differences were detected in the regression of 30- and 365-day readmission rates (P < 0.05), indicating that age may contribute to differences in readmission rates. However, no heterogeneity was detected in the 365-day readmission rate, which may be explained by the availability of age data. Specifically, some age data were presented as median and mean deviations, resulting in a large and uneven age distribution, which may have affected our results to some extent. In the subgroup analysis, we found that prospective studies had higher 30- and 365-day readmission rates than retrospective studies. This is probably because the results of the retrospective studies were primarily derived from medical records and related databases and were subject to common limitations of retrospective designs, including selection bias and misclassification bias, leading to lower readmission rates. However, in the regression analysis, no subgroup differences were found according to study type for 30-, 90-, and 365-day readmission rates (P > 0.05), indicating that study type may not be a source of heterogeneity. However, this must be confirmed in future studies. In the sample size subgroup analysis, we found that studies with a sample size of 0–499 had the highest 30-day readmission rate, while the 30-day readmission rates of studies with a sample size of 1000–10,000 and ≥ 100,000 were closer to the overall meta-analysis data, indicating that the results derived from large-sample studies may better represent the real-world situation. Furthermore, in the subgroup regression analysis of 90-day readmission rate, there were subgroup differences according to sample size (P < 0.05). It is noteworthy that the number of studies with sample sizes ranging from 500 to 999 was too small; therefore, the effect of sample size on COPD readmission rate should be interpreted with caution. In the region of research subgroup analysis, patients in China and South Korea had higher readmission rates. For the 365-day readmission rate, patients from northern China had a higher readmission rate than those from southern China, which may be attributed to the poor air quality and low temperature in northern China, which are more likely to cause acute attacks and hospitalization. In the subgroup regression of 90-day readmission, subgroup differences were detected by region of research (P < 0.05). Nonetheless, there were very few studies from countries other than China and South Korea; therefore, this finding needs to be confirmed by further large-scale, multicenter, and prospective studies.
Limitations
This study had some limitations: (1) The studies included were retrospective studies, so we could not control for the impact of biases in research design, selection, and measurement. (2) The heterogeneity of the included studies was high. We performed subgroup analyses of study characteristics and detected heterogeneity in terms of age, sample size, and region of research. However, our subgroup analyses only covered available factors and not disease severity, GOLD classification, or comorbidities. This may have had an impact on the meta-analysis results, and the studies included in this meta-analysis had high heterogeneity. Through a subgroup analysis of the characteristics of the included studies, we found that age, sample size, and study area were the main factors leading to heterogeneity. These findings provide important suggestions for future research on readmission in patients with COPD risk factors. In particular, we recommend the following: 1) Improving study accuracy and representativeness. Future studies should focus on reducing heterogeneity. More precise and targeted results could be obtained by a more detailed stratified analysis of factors, such as age, sample size, and study region. This would lead to better understanding of how the risk factors for acute readmission in patients with COPD differ across populations. 2) Optimizing age groups. Given that the age span is large, future research on patients should be divided into different age groups. This approach could reveal the influence of age on the risk of readmission in patients with COPD, thereby enabling the development of targeted prevention and treatment strategies for patients of different ages. 3) Paying attention to regional differences. Research in different regions could explore the geography, the environment, and medical conditions, such as the influence of risk factors in patients with COPD readmission. This could help to develop more suitable prevention and management strategies for a particular region. 4) Exploring new risk factors in addition to known risk factors. Future research should explore potential new risk factors, such as environmental pollution, lifestyle changes, and emerging complications, to enable comprehensive understanding of the factors that influence readmission among patients with COPD. Standardized assessment tools developed via large sample studies could enable comprehensive and accurate understanding of the risk factors for readmission in patients with COPD. This would enable the development of scientifically informed prevention and management strategies, eventually improving the prognosis and quality of life of patients, and reducing the burden on the health care system.
Conclusion
The existing evidence shows that history of ≥ 2 hospital admissions, ≥ 3 comorbidities, male sex, EOS% ≥ 2%, BMI < 18.5, smoking history, pulmonary heart disease comorbidity, nutritional disorder, NLR > 7, and FEV1 < 50 are risk factors for COPD readmission. The high readmission rates of patients with COPD at 30, 90, and 365 days after discharge were likely related to age, sample size, and the region of research. Based on our findings, it is necessary to pay attention to the prevention, screening, and intervention for relevant population groups and risk factors for COPD to reduce the risk of readmission and healthcare and economic burdens.
Availability of data and materials
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Abbreviations
- COPD:
-
Chronic obstructive pulmonary disease
- EOS:
-
Ratio of eosinophils
- CAT:
-
COPD assessment test
- NLR:
-
Neutrophil-to-Lymphocyte ratio
- BMI:
-
Body mass index
- FEV1:
-
Forced expiratory volume in one second
References
Mathers CD, Loncar D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Medicine. 2006;3(11):e442. https://doi.org/10.1371/journal.pmed.0030442.
Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957. https://doi.org/10.1136/thoraxjnl-2011-201518.
Adeloye D, Chua S, Lee C, et al. Global and regional estimates of COPD prevalence: Systematic review and meta-analysis. J Global Health. 2015;5(2):020415. https://doi.org/10.7189/jogh.05.020415.
Alqahtani JS, Njoku CM, Bereznicki B, et al. Risk factors for all-cause hospital readmission following exacerbation of COPD: a systematic review and meta-analysis. Eur Respir Rev. 2020;29(156):190166. https://doi.org/10.1183/16000617.0166-2019.
Chang C, Zhu H, Shen N, et al. Utility of the combination of serum highly-sensitive C-reactive protein level at discharge and a risk index in predicting readmission for acute exacerbation of COPD. J Bras Pneumol. 2014;40(5):495–503. https://doi.org/10.1590/s1806-37132014000500005.
Shani M, Comaneshter D, Segel MJ. The importance of having good quality indicators for care of patients with COPD: a look at hospital readmission rates. Isr J Health Policy Res. 2022;11(1):17. https://doi.org/10.1186/s13584-022-00528-7.
Kim TW, Choi ES, Kim WJ, et al. The Association with COPD Readmission Rate and Access to Medical Institutions in Elderly Patients. Int J Chron Obstruct Pulmon Dis. 2021;16:1599–606. https://doi.org/10.2147/COPD.S302631.
Li J, Liang L, Cao S, et al. Secular trend and risk factors of 30-day COPD-related readmission in Beijing, China. Scientific Reports. 2022;12(1):16589. https://doi.org/10.1038/s41598-022-20884-3.
Wei X, Ma Z, Yu N, et al. Risk factors predict frequent hospitalization in patients with acute exacerbation of COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:121–9. https://doi.org/10.2147/COPD.S152826.
Bing H, Xinhui Y, Yiyao B, et al. The predictive value of CT pulmonary artery to aortic ratio for the risk of readmission during acute exacerbation of chronic obstructive pulmonary disease. Chinese Med Sci. 2020;10(18):189–91.
Zhou M, Mingfang D. Risk factors for secondary exacerbation and readmission within one month after discharge in patients with acute exacerbation of COPD. Chinese Health Eng. 2022;21(4):586–587590. https://doi.org/10.19937/j.issn.1671-4199.2022.04.018.
Guimei Z, Shu C, Yunhua S, et al. Analysis of risk factors and construction of predictive models for re admission of AECOPD patients. J Kunming Med Univ. 2022;43(8):184–90. https://doi.org/10.12259/j.issn.2095-610X.S20220830.
Jiani Ye, Xinxin Fan, Ting Li. Analysis of risk factors for re admission of AECOPD patients. Zhejiang Clin Med. 2023;25(4):565–7.
Ruiyang Ding, Guxiang Zhang, Wenzhu Yang, et al. The predictive value of the ratio of serum hypersensitive C-reactive protein to prealbumin for 30-day readmission in patients with acute exacerbation of chronic obstructive pulmonary disease. J Clin Intern Med. 2022;39(7):468–72. https://doi.org/10.3969/j.issn.1001-9057.2022.07.009.
Li J, Ma X, Zeng X, et al. Risk Factors of Readmission Within 90 Days for Chronic Obstructive Pulmonary Disease Patients with Frailty and Construction of an Early Warning Model. Int J Chron Obstruct Pulmon Dis. 2023;18:975–84. https://doi.org/10.2147/COPD.S400638.
Chan FWK, Wong FYY, Yam CHK, et al. Risk factors of hospitalization and readmission of patients with COPD in Hong Kong population: analysis of hospital admission records. BMC Health Serv Res. 2011;11:186. https://doi.org/10.1186/1472-6963-11-186.
Jo YS, Rhee CK, Kim KJ, et al. Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease. Ther Adv Respir Dis. 2020;14:1753466620961688. https://doi.org/10.1177/1753466620961688.
Kim MH, Lee K, Kim KU, et al. Risk Factors Associated with Frequent Hospital Readmissions for Exacerbation of COPD. Tubercul Resp Dis. 2010;69(4):243. https://doi.org/10.4046/trd.2010.69.4.243.
Lin J, Xu Y, Wu X, et al. Risk factors associated with chronic obstructive pulmonary disease early readmission. Curr Med Res Opin. 2014;30(2):315–20. https://doi.org/10.1185/03007995.2013.858623.
Jingjing Y, Wei Z, Ming Z, et al. The relationship between peripheral blood eosinophils and clinical characteristics and short-term prognosis in elderly patients with acute exacerbation of chronic obstructive pulmonary disease. Pract J Card Cerebr Pneum Vasc Dis. 2023;31(5):45–9. https://doi.org/10.12114/j.issn.1008-5971.2023.00.107.
Xiaoyi F, Qinxue L, Binmiao L, et al. The predictive value of peripheral blood eosinophils on readmission during recovery in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Resp Sci. 2022;42(24):1895–901. https://doi.org/10.3760/cma.j.cn131368-20220711-00596.
Hao H, Zheng F, Bing D, et al. Analysis of the predictive effect of peripheral blood human cartilage glycoprotein 39 combined with eosinophils on the risk of acute exacerbation and readmission of chronic obstructive pulmonary disease. J Clin Military Med. 2023;51(1):23–6. https://doi.org/10.16680/j.1671-3826.2023.01.07.
Jing W, Bi C, Shuyang Z. The relationship between the percentage of eosinophils in peripheral blood at admission and the short-term acute exacerbation and recurrence of chronic obstructive pulmonary disease in patients with acute exacerbation after discharge. Pract J Card Cerebr Pneum Vasc Dis. 2019;27(7):46–50. https://doi.org/10.3969/j.issn.1008-5971.2019.07.009.
Ying L, Lei X, Wei B, et al. Analysis of readmission status and influencing factors of patients with chronic obstructive pulmonary disease in a tertiary hospital within one year after discharge. Chinese J Gen Pract. 2023;21(1):70-72,111. https://doi.org/10.16766/j.cnki.issn.1674-4152.002814.
Choi J, Oh JY, Lee YS, et al. Pseudomonas aeruginosa infection increases the readmission rate of COPD patients. Int J Chronic Obstruct Pulmon Dis. 2018;13:3077–83. https://doi.org/10.2147/COPD.S173759.
Chen L, Chen S. Prediction of readmission in patients with acute exacerbation of chronic obstructive pulmonary disease within one year after treatment and discharge. BMC Pulmon Med. 2021;21(1):320. https://doi.org/10.1186/s12890-021-01692-3.
Li M, Cheng K, Ku K, et al. Modelling 30-day hospital readmission after discharge for COPD patients based on electronic health records. NPJ Prim Care Respir Med. 2023;33(1):16. https://doi.org/10.1038/s41533-023-00339-6.
Goto T, Jo T, Matsui H, et al. Machine Learning-Based Prediction Models for 30-Day Readmission after Hospitalization for Chronic Obstructive Pulmonary Disease. COPD. 2019;16(5–6):338–43. https://doi.org/10.1080/15412555.2019.1688278.
Al Aqqad SMH, Tangiisuran B, Hyder Ali IA, et al. Hospitalisation of multiethnic older patients with AECOPD: exploration of the occurrence of anxiety, depression and factors associated with short-term hospital readmission. Clin Respir J. 2017;11(6):960–7. https://doi.org/10.1111/crj.12448.
Liqing Y, Lingyun G, Lingjing Y, et al. Analysis of risk factors for re hospitalization within one year in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease. J Southwest Med Univ. 2022;45(5):404–8. https://doi.org/10.3969/j.issn.2096-3351.2022.05.008.
Rongrong ZY, Yidan H, et al. Analysis of influencing factors and construction of Nomogram model for readmission within 30 days after discharge in patients with acute exacerbation of chronic obstructive pulmonary disease. Pract J Card Cerebr Pneumal Vasc Dis. 2020;28(8):57–63. https://doi.org/10.3969/j.issn.1008-5971.2020.08.011.
Haoyu N, Xuejun L, Li Q. Analysis of risk factors related to hospitalization treatment in patients with acute exacerbation of chronic obstructive pulmonary disease. Chinese Med. 2013;8(11):1558–60. https://doi.org/10.3760/cma.j.issn.1673-4777.2013.11.016.
Cao C, Tan WC. N g T P. Frequent readmission and risk factors in patients with acute exacerbation of chronic obstructive pulmonary disease. Chinese J Clin Healthcare. 2005;8(1):14–6. https://doi.org/10.3969/j.issn.1672-6790.2005.01.005.
Yusheng Y, Yuling T, Lv Y. Analysis of factors related to readmission of patients with chronic obstructive pulmonary disease. Chinese J Clin Phys. 2014;15:2910–2. https://doi.org/10.3877/cma.j.issn.1674-0785.2014.15.033.
Peng J, Yu Q, Fan S, et al. High Blood Eosinophil and YKL-40 Levels, as Well as Low CXCL9 Levels, are Associated with Increased Readmission in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Int J Chronic Obstruct Pulmon Dis. 2021;16:795–806. https://doi.org/10.2147/COPD.S294968.
Tomioka R, Kawayama T, Suetomo M, et al. “Frequent exacerbator” is a phenotype of poor prognosis in Japanese patients with chronic obstructive pulmonary disease. Int J Chronic Obstruct Pulmon Dis. 2016;11:207–16. https://doi.org/10.2147/COPD.S98205.
Chen YJ, Narsavage GL. Factors related to chronic obstructive pulmonary disease readmission in Taiwan. Western J Nurs Res. 2006;28(1):105–24. https://doi.org/10.1177/0193945905282354.
Yang T, Cai B, Cao B, et al. Exacerbation in patients with stable COPD in China: analysis of a prospective, 52-week, nationwide, observational cohort study (REAL). Ther Adv Respir Dis. 2023;17:175346662311673. https://doi.org/10.1177/17534666231167353.
Xu T, Sun W, Zhao H, et al. Characteristics of 12-Month Readmission for Hospitalized Patients with COPD: A Propensity Score Matched Analysis of Prospective Multicenter Study. Int J Chron Obstruct Pulmon Dis. 2022;17:2329–41. https://doi.org/10.2147/COPD.S376909.
Lei W. Analysis of influencing factors on acute exacerbation and readmission of elderly COPD patients after discharge. Capital Food Med. 2023;30(9):44–6. https://doi.org/10.3969/j.issn.1005-8257.2023.09.017.
Yiping Chen, Wenfang He, Shuyun Xiong, et al. Investigation on the influencing factors of readmission within one month after discharge in patients with chronic obstructive pulmonary disease[J]. Nurs Pract Res. 2020;17(6):4–7. https://doi.org/10.3969/j.issn.1672-9676.2020.06.002.
Jing Zhang, Chun Chang, Wanzhen Yao. Analysis of risk factors for readmission within one year of chronic obstructive pulmonary disease. Int J Resp Sci. 2014;7:500–3. https://doi.org/10.3760/cma.j.issn.1673-436X.2014.07.005.
Ling L, Yeshan L, Zhaoyan W, et al. Correlation analysis between chronic obstructive pulmonary disease testing and the risk of readmission within 3 months after acute exacerbation after discharge. J CardiovascPulmon Dis. 2020;39(5):577–81. https://doi.org/10.3969/j.issn.1007-5062.2020.05.021.
Jianguang W, Bing G, Honghao Z. Correlation analysis of multiple factors such as 30-day readmission rate and body mass index in patients with chronic obstructive pulmonary disease. Int J Resp Sci. 2019;39(22):1707–11. https://doi.org/10.3760/cma.j.issn.1673-436X.2019.22.006.
Lu HY, Zhang R, Chang Y, et al. A structural equation model-based study on the status and influencing factors of acute exacerbation readmission of elderly patients with chronic obstructive pulmonary disease within 30 days. BMC Pulmon Med. 2022;22(1):299. https://doi.org/10.1186/s12890-022-02093-w.
Department of Pulmonary Diseases, Dokuz Eylul University, Faculty of Medicine, Izmir, Turkey, Alpaydin AO, Ozuygur SS. et al. 30-day Readmission After an Acute Exacerbation of Chronic Obstructive Pulmonary Disease is Associated with Cardiovascular Comorbidity. Turk Thorac J. 2021;22(5):369–75. https://doi.org/10.5152/TurkThoracJ.2021.0189.
Zhang Rui Wu, Zhenzhen Chang Yan, et al. Construction and validation of a 30 day acute exacerbation readmission risk prediction model for elderly patients with chronic obstructive pulmonary disease. Chinese J Resp Crit Care. 2021;20(7):457–64. https://doi.org/10.7507/1671-6205.202011079.
Yiqin, B, Bingbing W, Zhangmin B, et al. Constructing a risk prediction model for unplanned readmission within 90 days after discharge of patients with acute exacerbation of chronic obstructive pulmonary disease based on the 2002 nutritional risk screening score. J Clin Military Med. 2022;50(8):814--817+820. https://doi.org/10.16680/j.1671-3826.2022.08.11.
Ruan H, Zhang H, Wang J, et al. Readmission rate for acute exacerbation of chronic obstructive pulmonary disease: A systematic review and meta-analysis. Respir Med. 2023;206:107090. https://doi.org/10.1016/j.rmed.2022.107090.
Spece LJ, Epler EM, Donovan LM, et al. Role of Comorbidities in Treatment and Outcomes after Chronic Obstructive Pulmonary Disease Exacerbations. Ann Am Thoracic Soci. 2018;15(9):1033–8. https://doi.org/10.1513/AnnalsATS.201804-255OC.
Nguyen HQ, Chu L, Amy Liu IL, et al. Associations between Physical Activity and 30-Day Readmission Risk in Chronic Obstructive Pulmonary Disease. Ann Am Thorac Soc. 2014;11(5):695–705. https://doi.org/10.1513/AnnalsATS.201401-017OC.
Nguyen HQ, Rondinelli J, Harrington A, et al. Functional status at discharge and 30-day readmission risk in COPD. Respir Med. 2015;109(2):238–46. https://doi.org/10.1016/j.rmed.2014.12.004.
Acknowledgements
Not applicable.
Funding
This work was supported by grants from Guangxi Natural Science Foundation (2015GXNSFAA139116), from Guangxi Appropriate Health Technology Research and Development Project (Grant No. S201407), and Basic Ability Improvement Project for Young and Middle aged Teachers in Guangxi Zhuang Autonomous Region (Grant No. KY2016YB311). The sponsor had no role in the design or conduct of this research.
Author information
Authors and Affiliations
Contributions
ML designed the study. CCS,QPL and YRH performed literature search. JTZ and YFL performed study identification. AXH and XL finished quality evaluation. PL finished data extraction, statistical analysis, and results interpretation. PL drafted the manuscript. PL and ML revised the manuscript and approved the submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lin, P., Shen, C., Li, Q. et al. A systematic review and meta-analysis of chronic obstructive pulmonary disease in asia: risk factors for readmission and readmission rate. BMC Pulm Med 24, 388 (2024). https://doi.org/10.1186/s12890-024-03203-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-024-03203-6