
Abstract
Background
Some medical conditions may increase the risk of developing pulmonary tuberculosis (PTB); however, no systematic study on PTB-associated comorbidities and comorbidity clusters has been undertaken.
Methods
A nested case-control study was conducted from 2013 to 2017 using multi-source big data. We defined cases as patients with incident PTB, and we matched each case with four event-free controls using propensity score matching (PSM). Comorbidities diagnosed prior to PTB were defined with the International Classification of Diseases-10 (ICD-10). The longitudinal relationships between multimorbidity burden and PTB were analyzed using a generalized estimating equation. The associations between PTB and 30 comorbidities were examined using conditional logistic regression, and the comorbidity clusters were identified using network analysis.
Results
A total of 4265 cases and 17,060 controls were enrolled during the study period. A total of 849 (19.91%) cases and 1141 (6.69%) controls were multimorbid before the index date. Having 1, 2, and ≥ 3 comorbidities was associated with an increased risk of PTB (aOR 2.85–5.16). Fourteen out of thirty comorbidities were significantly associated with PTB (aOR 1.28–7.27), and the associations differed by sex and age. Network analysis identified three major clusters, mainly in the respiratory, circulatory, and endocrine/metabolic systems, in PTB cases.
Conclusions
Certain comorbidities involving multiple systems may significantly increase the risk of PTB. Enhanced awareness and surveillance of comorbidity are warranted to ensure early prevention and timely control of PTB.
Similar content being viewed by others


Introduction
Pulmonary tuberculosis (PTB), accounting for almost 50% of all new tuberculosis (TB) cases reported globally in 2021, continues to pose a serious threat to global health due to its high morbidity and mortality [1]. Some immunocompromised states, including those produced by aging, chronic diseases (such as HIV/AIDS and diabetes mellitus), and immunosuppressive therapy, may contribute to the development of PTB [2, 3]. However, few studies have systematically analyzed the comorbidities associated with PTB and their potential clusters. Additionally, previous studies have mostly focused on a single medical condition through cross-sectional or cohort studies. Nested case-control studies allow us to simultaneously investigate the causative role of multiple risk factors in the development of an outcome. The exposure data are measured prior to the outcome occurring, and the design provides an efficient way to identify causal relationships [4]. Multi-source healthcare big data, involving all communicable and non-communicable diseases of an individual that occur during the study period [5], give us the chance to recognize the associations between PTB and multiple diseases, as well as the complex interactions among comorbidities.
Although China has the third highest TB burden in the world, with 7.4% of the incident cases [1], the influence of comorbidities on PTB has not yet been fully described. In the present study, we carried out a nested case-control study based on the Shandong Multi-Center Healthcare Big Data Platform (SMCHBDP). We aimed to investigate the relationships between PTB and prevalence of comorbidity, recognize the risk factors favoring the development of PTB, elaborate the comorbidity clusters in PTB patients, and thus devise targeted control efforts to fight against PTB in China.
Materials and methods
Study design and population
We conducted a nested case-control study using the Shandong Multi-Center Healthcare Big Data Platform (SMCHBDP) [5, 6]. Multi-stage sampling was used to select the potentially eligible participants in rural and urban areas of Shandong Province, based on their identity numbers registered on the SMCHBDP [6]. Multiple sources of health-related data, including electronic medical health records, basic public health records, and resident medical insurance payment systems, were integrated and linked using unique identity numbers. A total of five million participants in Shandong Province, China, were involved. Each eligible participant’s information concerning demographic characteristics (age, sex, and place of residence) and medical history (diagnoses, prescriptions, and past diseases) was extracted. Then, participants registered on the SMCHBDP from 1 January 2013 to 31 December 2017 were included, and those with duplicate or incorrect identity numbers were excluded. Furthermore, participants with evident outliers or logical errors in case information, making it impossible to link disease visit information to specific individuals, were also excluded. Additionally, since some participants were registered at multiple medical institutions, we used the earliest registration date as the personal finishing baseline filling date in the SMCHBDP. Finally, a total of 4,057,987 participants were included in the present study from 1 January 2013 to 31 December 2017. The follow-up time started at the date of the enrollment of participants (finishing baseline filling date) and ended at the time of incident PTB, death, or on 31 December 2017. This study was approved by the Ethics Committee of the School of Public Health, Shandong University, China. All individual information has been anonymized and informed consent was waived owing to the retrospective nature of the study.
Definitions of cases and controls
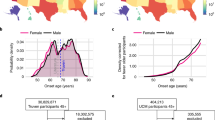
Confirmed PTB cases, based on symptoms, chest X-rays, and positive sputum smears or cultures, were diagnosed by qualified physicians according to the National Diagnostic Criteria for Pulmonary Tuberculosis [7] and the 10th revision of the International Statistical Classification of Diseases (ICD-10). The date of initial diagnosis for PTB served as the index date. There were a total of 19,824 patients with TB-related clinical records in the database. We then excluded the patients with missing diagnosis date (n = 242), without clear diagnosis (n = 2814), diagnosis of extrapulmonary tuberculosis (n = 6537), and prevalent PTB cases at baseline (n = 5966). For each case, four event-free controls (participants without TB-related clinical records) alive on the index date were identified using the propensity score matching (PSM) method [8], matching age (within 3 years), sex, enrollment year, and place of residence. In total, 4265 PTB cases and 17,060 controls were enrolled. The sampling process is depicted in Fig. 1.

Study flowchart for the selection of PTB cases and controls. PTB, pulmonary tuberculosis
Comorbidity
Comorbidity was defined as any distinct medical condition that existed before the occurrence of PTB. Diseases that met the following criteria were included in further analysis: (1) having a potential impact on the development of tuberculosis, (2) having a prevalence of > 0.1% in cases, and (3) having at least two diagnostic records. We finally selected 30 clinically important comorbidities in the present study, and all these diseases were defined according to the ICD-10 (Table S1). The date of the first diagnostic record of diseases served as the onset date. Multimorbidity was defined as the co-occurrence of at least 2 conditions from the above 30 comorbidities within a person. In addition, the Charlson-Deyo Comorbidity Index (CCI) was used to evaluate the burden of multimorbidity [9].
Statistical analysis
The normality of continuous data was tested using the Kolmogorov-Smirnov test. Skewed data were expressed as median (interquartile range, IQR) and compared using the Kruskal-Wallis test. Categorical variables were shown as frequency (%), and the differences were tested using a chi-squared test. The generalized estimating equation (GEE) was utilized to analyze the longitudinal relationships between multimorbidity burden and PTB. Conditional logistic regression analysis was used to examine the association between PTB and 30 comorbidities in the entire study population and in subgroups stratified by age (0–44 years, 45–64 years, and ≥ 65 years) and sex. Diseases with statistical significance in multifactorial conditional logistic regression (adjusting for age at index date, sex, and all comorbidities) were included to create an undirected weighted comorbidity network. The co-occurrence intensity between different diseases was measured using the observed-to-expected ratio (OER), and comorbidity clusters were recognized using the community detection algorithm Louvain [10]. The false discovery rate (FDR) was controlled for multiple testing with the Benjamini-Hochberg procedure [11]. All statistical analyses were performed using R software (version 4.1.2, R Foundation for Statistical Computing, Vienna, Austria), and a P value < 0.05 was considered statistically significant.
Results
Demographic characteristics and multimorbidity
The detailed information on characteristics of participants is displayed in Table 1. The median age of both cases and controls was 46 years (IQR 27–62), and 63.26% of them were male. There were no significant differences in matching variables between the two groups (P > 0.05). The median time from entrance into the cohort to the index date for the PTB and control groups was 2.54 years (IQR 1.26–3.68) and 2.58 years (IQR 1.30–3.72), respectively. Compared with the control group, PTB cases had a higher proportion of having comorbidities during the study period. In total, 849 (19.91%) cases and 1141 (6.69%) controls were multimorbid. The prevalence of multimorbidity increased with age, and the sex-specific prevalence was higher in female than in male in all age groups (Table S2). According to the CCI score, cases with PTB tended to have a moderate (20.42% vs. 6.73%) or high (4.92% vs. 1.27%) burden of multimorbidity compared with controls (Table 1).
Associations between PTB and multimorbidity
Compared with the controls, cases were more likely to have comorbidities at baseline and during follow-up (Fig. S1). The risk of PTB increased with the number of comorbidities from an adjusted odds ratio (aOR) of 2.85 (95% CI 2.58–3.15) for individuals with one comorbidity to 5.16 (95% CI 4.58–5.81) for those with three or more comorbidities (Fig. 2a). The predicted probabilities of PTB considerably increased over time among all individuals, and this trend was more obvious in individuals with multimorbidity (Fig. 2b).

Associations between PTB and multimorbidity burden. (a) Association between multimorbidity burden and risk of PTB is expressed as odds ratios. Age, sex, and year of follow-up were adjusted for in the generalized estimating equation, with no comorbidity used as the reference (aOR = 1); (b) longitudinal associations between multimorbidity burden and predicted probabilities of PTB were estimated using a generalized estimating equation. aOR, adjusted odds ratio; PTB, pulmonary tuberculosis
Comorbidity and risk of PTB
All comorbidities were more prevalent in patients with PTB compared with matched controls (Table 2). The top five diseases in PTB cases were hypertensive diseases (14.40%), chronic lower respiratory diseases (10.83%), chronic ischemic heart disease (9.52%), diabetes mellitus (9.21%), and cerebrovascular diseases (6.80%). Fourteen comorbidities were associated with an increased risk of PTB after adjusting for potential confounding variables. The two comorbidities with the strongest associations were interstitial lung diseases (aOR 7.27, 95% CI 3.61–14.64) and chronic lower respiratory diseases (aOR 7.25, 95% CI 5.98–8.80). Individuals with comorbidities, including connective tissue diseases, inflammatory diseases of the central nervous system, cancer, inflammatory diseases of female pelvic organs, chronic liver diseases, diabetes mellitus, and disorders of the peripheral nervous system, were two to three times as likely to have PTB compared with those without comorbidities. The risk of PTB for individuals with cerebrovascular diseases, disorders of the thyroid gland, noninfective enteritis and colitis, chronic ischemic heart disease, and metabolic disorders was slightly but significantly higher with an aOR of 1–2.
Subgroup analyses by sex and age at index date were carried out. The aOR was significantly higher in female with interstitial lung diseases (aOR 19.40, 95% CI 4.03–93.37), chronic lower respiratory diseases (aOR 9.58, 95% CI 6.60–13.92), and connective tissue diseases (aOR 6.00, 95% CI 2.21–16.29) than in male (Tables S3 and S4). Cardiac arrhythmias (aOR 6.63, 95% CI 1.62–27.17) and Intervertebral disc disorders (aOR 3.61, 95% CI 1.57–8.28) were significantly associated with PTB in individuals aged 44 years and younger, while anemias increased the risk of developing PTB within the group of those aged 45–64 years (aOR 5.68, 95% CI 1.92–16.78) (Tables S5 and S6). The two comorbidities with the strongest associations in patients over 65 were chronic lower respiratory diseases (aOR 6.67, 95% CI 5.16–8.62) and interstitial lung diseases (aOR 5.76, 95% CI 2.42–13.71) (Table S7).
Comorbidity network
Figure 3 depicts the network of the fourteen comorbidities significantly associated with PTB. Based on the degree centrality values, chronic lower respiratory diseases, diabetes mellitus, chronic ischemic heart disease, cerebrovascular diseases, and cancer were key conditions in the PTB comorbidity network (Table S8). The strongest links occurred among endocrine/metabolic, digestive, respiratory, nervous, and musculoskeletal/connective tissue diseases. For example, noninfective enteritis and colitis co-occurred with inflammatory diseases of the central nervous system, interstitial lung diseases co-occurred with connective tissue diseases, and diabetes mellitus co-occurred with disorders of the peripheral nervous system (Fig. 3) (Table S9). Modularity analysis revealed three clusters: (a) chronic lower respiratory diseases, interstitial lung diseases, connective tissue diseases, and metabolic disorders; (b) chronic ischemic heart disease, diabetes mellitus, cerebrovascular diseases, noninfective enteritis and colitis, and inflammatory diseases of the central nervous system; (c) cancer, disorders of the thyroid gland, disorders of the peripheral nervous system, inflammatory diseases of female pelvic organs, and chronic liver diseases (Fig. 3).

Comorbidity network in patients with PTB. Each node represents a disease. Color of each node indicates the disease category. Width of edge represents the strength of comorbidity association measured using observed-to-expected ratio. Three clusters of the comorbidity network are represented with dashed lines. PTB, pulmonary tuberculosis. OER, observed-to-expected ratio
Discussion
In this nested case-control study, a higher proportion of PTB cases were multimorbid before the index date. The increased number of comorbidities might lead to a higher risk of developing PTB. Among 30 comorbidities, 14 were found to be significantly positively associated with PTB, ranging from an aOR of 1.28 (cerebrovascular diseases) to 7.27 (interstitial lung diseases). Three clusters of comorbidities, affecting the respiratory, circulatory, and endocrine/metabolic systems, were observed. Our findings shed new light on the high-risk population of PTB and provide a scientific basis for targeted prevention policies for the disease.
Strong links between TB and other communicable diseases or noncommunicable diseases (NCDs) have been found in many countries, especially in developing countries, resulting in a “double burden of disease” [12]. Patients with PTB, which is considered the most common manifestation of TB, have concurrent various comorbidities in clinical practice. The present study found that 19.91% of PTB cases had at least two comorbidities before the index date, and the multimorbidity burden was particularly high in female and older cases. Both multimorbidity and PTB were associated with high mortality, declined physical function, and increased socioeconomic and medical burden [13]. A cross-sectional survey conducted in 48 low- and middle-income countries showed that people with 1, 2, 3, 4, and ≥ 5 noncommunicable diseases had from 2.61 to 19.89 times higher odds for TB [14]. A multicenter observational study indicated that having one or more comorbidities that weaken the immune response may cause patients to become pre-disposed to developing PTB [15]. Our nested case-control study in Shandong Province, China, found that the risk of PTB tended to increase with an increasing number of comorbidities, which was consistent with the previous reports. A better understanding of the associations between multimorbidity, comorbidities, and PTB is vital for reducing the double burden of diseases worldwide, in particular in developing countries.
After adjusting for age, sex, and other comorbidities, 14 comorbidities across 8 systems were significantly associated with the increasing risk of PTB, with odds ratios ranging from 1.28 to 7.27 in this study. Previous studies have demonstrated that diabetes mellitus was associated with an increased risk of PTB [16, 17]. The data here showed that individuals with diabetes mellitus were twice as likely to have PTB compared with those without diabetes mellitus (aOR 2.07, 95% CI 1.76–2.44). The morbidity and mortality of PTB and diabetes mellitus remain high, especially when these two diseases occur together [18]. Our findings strongly suggest that TB control measures should be integrated with diabetes mellitus control programs. We also demonstrated that the risk of PTB among patients with connective tissue diseases was significantly high (aOR 3.62, 95% CI 1.87–7.00). Previous studies have shown that patients with connective tissue diseases, such as rheumatoid arthritis [19, 20] and systemic lupus erythematosus [21], were at high risk for TB. The possible reasons for this may be due to the defective immunity resulting from the diseases or associated immunosuppressant therapy. These results indicate that healthcare workers need to be vigilant about the development of PTB among patients with connective tissue diseases. A review article on host-directed therapy suggests that the occurrence of NCDs could indicate a need for active TB screening for its early detection of TB and treatment outcomes improvement. And TB diagnosis provides a chance for clinicians to screen for NCDs like diabetes mellitus [22].
Globally, the associations between a history of chronic respiratory diseases and the presence of TB are inconsistent in different countries. One systematic review suggested an increased risk of TB in people with chronic obstructive pulmonary disease (COPD) in high-income countries [23]. In low- and middle-income countries with a high incidence of TB, information on the associations between TB and chronic respiratory diseases was limited. A Chinese cohort study involving 23,594 COPD cases and 47,188 control subjects revealed that COPD was an independent risk factor for developing PTB [24]. A study in India reported a significantly increased risk of TB in patients with asthma (adjusted odds ratio 2.5, 95% CI 1.8–3.7), while an inverse association was found in three countries in west Africa [25, 26]. Our results indicated the significant association between PTB and chronic lower respiratory diseases (aOR 7.25, 95% CI 5.98–8.80) after adjustment for age, sex, and other comorbidities. The possible reasons for such differences might include different Bacillus Calmette–Guérin (BCG) vaccination coverage, genetic and environmental factors among ethnic groups, and sample sizes [23]. These results suggested that the risk of PTB development in patients with chronic lung diseases needs further investigation. Additionally, we confirmed that patients with interstitial lung diseases had 7.27 times higher odds of developing PTB (aOR 7.27, 95% CI 3.61–14.64), which is consistent with the results of previous studies [27].
Previous studies have mainly focused on the impact of respiratory and endocrine/metabolic diseases on PTB development; the relationships between the comorbidities of other systems and PTB have received less attention. Big data derived from multiple sources made it possible to identify other potential risk factors of PTB. With regard to circulatory system diseases, Chidambaram et al. reported tuberculosis infection has been associated with acute myocardial infarction and atherothrombotic stroke [28]. Our study found that patients with chronic ischemic heart disease (aOR 1.58, 95% CI 1.31–1.90) and cerebrovascular diseases (aOR 1.28, 95% CI 1.05–1.57) had a higher risk of PTB. The possible reason for this association might be systemic inflammation and its mediation of chronic diseases [28]. For digestive system diseases, we found a strong association between noninfective enteritis and colitis and PTB after adjusting for confounding factors. The association between PTB and inflammatory bowel disease (IBD) was also reported in a recent study. Krusinski et al. found that biological agents for IBD may increase the susceptibility to TB [29]. Additionally, we found that some comorbidities demonstrated age discrepancies. Individuals with cardiac arrhythmias (aOR 6.63, 95% CI 1.62–27.17) or intervertebral disc disorders (aOR 3.61 95% CI 1.57–8.28) have a higher risk of PTB in the age group of 0–45 years. It is noted that these two diseases have not been considered as risk factors for PTB before. Anemias (aOR 5.68, 95% CI 1.92–16.78), a strong predictor of TB [30], had a significant association with PTB within the group of those aged 45–65 years in our study. Therefore, the increased risk of PTB among individuals with these conditions should be addressed.
To the best of our knowledge, this is the first study to systematically investigate the comorbidities and their complex associations in patients with PTB in China. Our results showed that chronic lower respiratory diseases, diabetes mellitus, chronic ischemic heart disease, cerebrovascular diseases, and cancer were more closely related to other diseases in the comorbidity network and contributed to a high risk of PTB. Some links between comorbidities should be emphasized, such as that between interstitial lung diseases and connective tissue diseases. Previous studies indicated that all patients with connective tissue diseases are at risk of interstitial lung diseases, and some connective tissue diseases (e.g., systemic sclerosis, antisynthetase syndrome, and rheumatoid arthritis) are more likely to be associated with interstitial lung diseases [31]. Modularity analysis in our study demonstrated three clusters, including diseases in the respiratory, circulatory, and endocrine/metabolic systems. Highly aggregated comorbidities in PTB patients may be the result of sharing the same gene or pathway of protein action or having similar risk factors or patterns of disease trajectory [32]. For instance, chronic ischemic heart disease, cerebrovascular diseases, and diabetes mellitus were classified into the same cluster. These are all complex, system-level diseases affecting many physiological and biomolecular processes; therefore, they co-occur with each other [33]. A recent network analysis showed that 86 key regulators were enriched by diverse biological processes and pathways, possibly connecting TB and NCDs, such as diabetes mellitus and cardiovascular diseases [34]. Analyzing comorbidity clusters may help us better understand associations between diseases rather than viewing them as isolated illnesses. Therefore, giving priority to controlling common risk factors in each cluster would be more efficient to reduce the comorbid burden with limited health resources, especially in high TB burden countries.
With the rapid development of computer science and information technology, healthcare big data provide a new approach to discover previously unappreciated relationships between communicable and non-communicable diseases. This nested case-control study using the SMCHBDP showed that having multiple comorbidities may increase the risk of developing PTB, and highlighted the complex interactions among comorbidities. Compared with traditional surveillance system, multi-source healthcare big data involved all medical conditions of an individual that occured during the study period. Additionally, the design of nested case-control study minimized selection bias and recall bias, making the causal association between PTB and comorbidities inferred from our study more reliable. Our research findings will enable healthcare workers to detect and prevent PTB at an early stage in populations with specific comorbidities. Due to the population-based nature of our study, we believe the results can be applied to other cities with comparable healthcare systems and accessibility to basic medical treatment. Future studies are required to understand the prevalence and distribution patterns of PTB comorbidity in the community.
This study has two main limitations. First, the lack of information on individual risk factors, including smoking habits, physical activities, socioeconomic status, drug resistance, and treatment outcome, might have affected the associations. Nonetheless, the most important variables influencing PTB development, including age, sex, and other comorbidities, were adjusted for in our analysis. Second, the sample size of PTB cases and some comorbidities was relatively small, and the follow-up time was relatively short. Therefore, this study might be underpowered. However, we still found associations between PTB and fourteen comorbidities. Future studies with a larger sample and a longer observation period will be needed to confirm the findings. Additionally, the design of nested case-control study minimized selection bias and recall bias. The causality inferred from the associations between PTB and comorbidities in our study could be more reliable.
Conclusions
In conclusion, the risk of PTB increased incrementally for each additional comorbidity from an aOR of 2.85 for one comorbidity to 5.16 for ≥ 3 comorbidities. Fourteen comorbidities, such as interstitial lung diseases, chronic lower respiratory diseases, and diabetes mellitus, were associated with an increased risk of developing PTB. Diseases of respiratory, circulatory, and endocrine/metabolic systems tend to co-occur and cluster with each other. Enhanced awareness and surveillance of comorbidity are warranted, especially in countries with a high tuberculosis burden. Authorities and healthcare workers should adopt inclusive strategies that take more diseases and risk factors into account to ensure early prevention and timely control of PTB.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due individual privacy of patients could be compromised, but are available from the corresponding author on reasonable request.
Abbreviations
- TB:
-
Tuberculosis
- PTB:
-
Pulmonary Tuberculosis
- PSM:
-
Propensity score matching
- ICD-10:
-
International Classification of Diseases-10
- aOR:
-
Adjusted odds ratio
- HIV:
-
Human Immunodeficiency Virus
- AIDS:
-
Acquired Immune Deficiency Syndrome
- SMCHBDP:
-
Shandong Multicenter Healthcare Big Data Platform
- CCI:
-
Charlson-Deyo Comorbidity Index
- IQR:
-
Interquartile range
- CI:
-
Confidence interval
- GEE:
-
Generalized estimating equation
- OER:
-
Observed-to-expected ratio
- FDR:
-
False discovery rate
- NCDs:
-
Noncommunicable diseases
- COPD:
-
Chronic obstructive pulmonary disease
- BCG:
-
Bacillus Calmette-Guérin
- IBD:
-
Inflammatory bowel disease
References
World Health Organization. Global Tuberculosis Report. World Health Organization. ; 2022. Available online: https://www.who.int/publications/i/item/9789240061729 (accessed on 3 December 2022).
Ugarte-Gil C, Carrillo-Larco RM, Kirwan DE. Latent Tuberculosis Infection and non-infectious co-morbidities: Diabetes Mellitus type 2, chronic Kidney Disease and rheumatoid arthritis. Int J Infect Dis. 2019;80S:29–S31. https://doi.org/10.1016/j.ijid.2019.02.018.
O’Garra A, Redford PS, McNab FW, Bloom CI, Wilkinson RJ, Berry MP. The immune response in Tuberculosis. Annu Rev Immunol. 2013;31:475–527. https://doi.org/10.1146/annurev-immunol-032712-095939.
Ernster VL. Nested case-control studies. Prev Med. 1994;23:587–90. https://doi.org/10.1006/pmed.1994.1093.
Zhao L, Wang HT, Ye RZ, et al. Profile and dynamics of infectious Diseases: a population-based observational study using multi-source big data. BMC Infect Dis. 2022;22:332. https://doi.org/10.1186/s12879-022-07313-6.
Du WY, Yin CN, Wang HT, et al. Infectious Diseases among elderly persons: results from a population-based observational study in Shandong province, China, 2013–2017. J Glob Health. 2021;11:08010. https://doi.org/10.7189/jogh.11.08010.
National Health and Family Planning Commission of the People’s Republic of China. Diagnostic criteria for Tuberculosis. Electron J Emerg Infect Dis. 2018;3:59–61. https://doi.org/10.19871/j.cnki.xfcrbzz.2018.01.017.
Elze MC, Gregson J, Baber U, et al. Comparison of Propensity score methods and Covariate Adjustment: evaluation in 4 Cardiovascular studies. J Am Coll Cardiol. 2017;69:345–57. https://doi.org/10.1016/j.jacc.2016.10.060.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83. https://doi.org/10.1016/0021-9681(87)90171-8.
Lee HA, Park H. Comorbidity network analysis related to obesity in middle-aged and older adults: findings from Korean population-based survey data. Epidemiol Health. 2021;43:e2021018. https://doi.org/10.4178/epih.e2021018.
Benjamini Y, Hochberg Y. Controlling the false discovery rate a practical and powerful approach to multiple testing. J R Stat Soc B Methodol. 1995;57:289–300. https://doi.org/10.1111/j.2517-6161.1995.tb02031.x.
Marais BJ, Lonnroth K, Lawn SD, et al. Tuberculosis comorbidity with communicable and non-communicable Diseases: integrating health services and control efforts. Lancet Infect Dis. 2013;13:436–48. https://doi.org/10.1016/S1473-3099(13)70015-X.
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380:37–43. https://doi.org/10.1016/S0140-6736(12)60240-2.
Stubbs B, Siddiqi K, Elsey H, et al. Tuberculosis and non-communicable Disease Multimorbidity: An Analysis of the World Health Survey in 48 low- and Middle-Income Countries. Int J Environ Res Public Health. 2021;18:2439. https://doi.org/10.3390/ijerph18052439.
Kang W, Du J, Yang S, et al. The prevalence and risks of major comorbidities among inpatients with pulmonary Tuberculosis in China from a gender and age perspective: a large-scale multicenter observational study. Eur J Clin Microbiol Infect Dis. 2021;40:787–800. https://doi.org/10.1007/s10096-020-04077-2.
Wu Q, Liu Y, Ma YB, Liu K, Chen SH. Incidence and prevalence of pulmonary Tuberculosis among patients with type 2 Diabetes Mellitus: a systematic review and meta-analysis. Ann Med. 2022;54:1657–66. https://doi.org/10.1080/07853890.2022.2085318.
Li Y, Guo J, Xia T, et al. Incidence of pulmonary Tuberculosis in Chinese adults with type 2 Diabetes: a retrospective cohort study in Shanghai. Sci Rep. 2020;10:8578. https://doi.org/10.1038/s41598-020-65603-y.
Bloomgarden Z, Misra A. Diabetes and Tuberculosis: an important relationship. J Diabetes. 2017;9:640–3. https://doi.org/10.1111/1753-0407.12547.
Baronnet L, Barnetche T, Kahn V, Lacoin C, Richez C, Schaeverbeke T. Incidence of Tuberculosis in patients with rheumatoid arthritis. A systematic literature review. Jt Bone Spine. 2011;78:279–84. https://doi.org/10.1016/j.jbspin.2010.12.004.
Lu MC, Lai CL, Tsai CC, Koo M, Lai NS. Increased risk of pulmonary and extra-pulmonary Tuberculosis in patients with rheumatic Diseases. Int J Tuberc Lung Dis. 2015;19:1500–6. https://doi.org/10.5588/ijtld.15.0087.
Balbi GGM, Machado-Ribeiro F, Marques CDL, Signorelli F, Levy RA. The interplay between Tuberculosis and systemic Lupus Erythematosus. Curr Opin Rheumatol. 2018;30:395–402. https://doi.org/10.1097/BOR.0000000000000493.
Baindara P. Host-directed therapies to combat Tuberculosis and associated non-communicable Diseases. Microb Pathog. 2019;130:156–68. https://doi.org/10.1016/j.micpath.2019.03.003.
Hamada Y, Fong CJ, Copas A, Hurst JR, Rangaka MX. Risk for development of active Tuberculosis in patients with chronic airway disease-a systematic review of evidence. Trans R Soc Trop Med Hyg. 2022;116:390–8. https://doi.org/10.1093/trstmh/trab122.
Lee CH, Lee MC, Shu CC, et al. Risk factors for pulmonary Tuberculosis in patients with chronic obstructive airway Disease in Taiwan: a nationwide cohort study. BMC Infect Dis. 2013;13:194. https://doi.org/10.1186/1471-2334-13-194.
Bhat J, Rao VG, Sharma RK, Muniyandi M, Yadav R, Bhondley MK. Investigation of the risk factors for pulmonary Tuberculosis: a case-control study among Saharia tribe in Gwalior district, Madhya Pradesh, India. Indian J Med Res. 2017;146:97–104. https://doi.org/10.4103/ijmr.IJMR_1029_16.
Lienhardt C, Fielding K, Sillah JS, et al. Investigation of the risk factors for Tuberculosis: a case-control study in three countries in West Africa. Int J Epidemiol. 2005;34:914–23. https://doi.org/10.1093/ije/dyi100.
Shachor Y, Schindler D, Siegal A, Lieberman D, Mikulski Y, Bruderman I. Increased incidence of pulmonary Tuberculosis in chronic interstitial lung Disease. Thorax. 1989;44:151–3. https://doi.org/10.1136/thx.44.2.151.
Chidambaram V, Ruelas Castillo J, Kumar A, et al. The association of atherosclerotic Cardiovascular Disease and statin use with inflammation and treatment outcomes in Tuberculosis. Sci Rep. 2021;11:15283. https://doi.org/10.1038/s41598-021-94590-x.
Krusinski A, Grzywa-Celinska A, Szewczyk K, Grzycka-Kowalczyk L, Emeryk-Maksymiuk J, Milanowski J. Various forms of Tuberculosis in patients with inflammatory bowel Diseases treated with Biological agents. Int J Inflammation. 2021;2021:6284987. https://doi.org/10.1155/2021/6284987.
Ashenafi S, Bekele A, Aseffa G, et al. Anemia is a strong predictor of Wasting, Disease Severity, and Progression, in clinical Tuberculosis (TB). Nutrients. 2022;14:3318. https://doi.org/10.3390/nu14163318.
Fischer A, du Bois R. Interstitial lung Disease in connective tissue disorders. Lancet. 2012;380:689–98. https://doi.org/10.1016/S0140-6736(12)61079-4.
Hidalgo CA, Blumm N, Barabasi AL, Christakis NA. A dynamic network approach for the study of human phenotypes. PLoS Comput Biol. 2009;5:e1000353. https://doi.org/10.1371/journal.pcbi.1000353.
Zhou D, Wang L, Ding S, Shen M, Qiu H. Phenotypic Disease Network Analysis To Identify Comorbidity Patterns in hospitalized patients with Ischemic Heart Disease using large-Scale Administrative Data. Healthcare. 2022;10:80. https://doi.org/10.3390/healthcare10010080.
Alam A, Abubaker Bagabir H, Sultan A, et al. An Integrative Network Approach to identify common genes for the therapeutics in Tuberculosis and its overlapping non-communicable Diseases. Front Pharmacol. 2021;12:770762. https://doi.org/10.3389/fphar.2021.770762.
Acknowledgements
Not applicable.
Funding
This study was supported by the Natural Science Foundation of China (82103897 and 81621005); the Natural Science Foundation of Shandong Province, China (ZR2020QH299); and the Cheeloo Young Scholar Program of Shandong University.
Author information
Authors and Affiliations
Contributions
BY W: Conceptualization, Methodology, Visualization, Writing original draft. L Z, K S and HT W: Writing review and editing, Investigation, Validation. SS W, WJ W, ZW L and WY D: Data curation, Software, Methodology. L Z and WC C: Funding acquisition, Supervision. FZ X and WC C: Resources, Project administration. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study complied with the Declaration of Helsinki. The study was approved by the Ethics Committee of the School of Public Health, Shandong University. The need for written informed consent was waived by the Ethics Committee of the School of Public Health, Shandong University, due to retrospective nature of the study. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, BY., Song, K., Wang, HT. et al. Comorbidity increases the risk of pulmonary tuberculosis: a nested case-control study using multi-source big data. BMC Pulm Med 24, 29 (2024). https://doi.org/10.1186/s12890-023-02817-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-023-02817-6