
Abstract
Background
Recent studies have shown an association between baseline arterial carbon dioxide pressure (PaCO2) and outcomes in patients with acute respiratory distress syndrome (ARDS). However, PaCO2 probably varies throughout the disease, and few studies have assessed the effect of longitudinal PaCO2 on prognosis. We thus aimed to investigate the association between time-varying PaCO2 and 28-day mortality in mechanically ventilated ARDS patients.
Methods
In this retrospective study, we included all adult (≥ 18 years) patients diagnosed with ARDS who received mechanical ventilation for at least 24 h at a tertiary teaching hospital between January 2014 and March 2021. Patients were excluded if they received extracorporeal membrane oxygenation (ECMO). Demographic data, respiratory variables, and daily PaCO2 were extracted. The primary outcome was 28-day mortality. Time-varying Cox models were used to estimate the association between longitudinal PaCO2 measurements and 28-day mortality.
Results
A total of 709 patients were eligible for inclusion in the final cohort, with an average age of 65 years, of whom 70.7% were male, and the overall 28-day mortality was 35.5%. After adjustment for baseline confounders, including age and severity of disease, a significant increase in the hazard of death was found to be associated with both time-varying PaCO2 (HR 1.07, 95% CI 1.03–1.11, p<0.001) and the time-varying coefficient of variation for PaCO2 (HR 1.24 per 10% increase, 95% CI 1.10–1.40, p<0.001) during the first five days of invasive mechanical ventilation. The cumulative proportion of exposure to normal PaCO2 (HR 0.72 per 10% increase, 95% CI 0.58–0.89, p = 0.002) was associated with 28-day mortality.
Conclusion
PaCO2 should be closely monitored in mechanically ventilated ARDS patients. The association between PaCO2 and 28-day mortality persisted over time. Increased cumulative exposure to normal PaCO2 was associated with a decreased risk of death.
Similar content being viewed by others
Background
Acute respiratory distress syndrome (ARDS), characterized by refractory hypoxemia, is a life-threatening disease with high incidence and high mortality [1, 2]. More than 70% of ARDS patients require invasive mechanical ventilation [1,2,3] to maintain oxygenation and ventilation. However, arterial carbon dioxide pressure (PaCO2), a frequently monitored parameter that is closely related to alveolar ventilation [4], has not been fully appreciated and emphasized in clinical studies. Indeed, PaCO2 derangements, including hypercapnia and hypocapnia, are pretty prevalent in ARDS patients [5], and numerous studies evaluating the association between PaCO2 and clinical outcomes have yielded different results [5,6,7]. To date, there are no definitive guidelines on how to manage PaCO2 in patients with ARDS.
However, published studies investigating the impact of PaCO2 on the prognosis of ARDS patients have merely focused on a single measurement, typically within 24 or 48 h after admission to the intensive care unit (ICU) or mechanical ventilation. Statistical analyses that only adjust for baseline confounders seem to be implausible, as PaCO2 possibly varies due to the evolution of the disease and the corresponding therapeutic regimens. Static assessments of PaCO2, which ignored the dynamic nature of the syndrome, may be incomprehensive and would fail to consider the relation of survival as a function of the change in the covariate [8]. In fact, compared with analyses based exclusively on cross-sectional data, the analysis of longitudinal data can sometimes yield additional or even different information to guide clinical decisions [9,10,11]. It is still unclear whether the association between time-varying PaCO2 and mortality is significant and remains persistent over time.
Therefore, we proposed to evaluate the effect of dynamic PaCO2 after the initiation of mechanical ventilation, as measured by either the time-varying daily PaCO2 or the coefficient of variation for PaCO2, on 28-day mortality in patients with acute respiratory distress syndrome. We also examined whether there was a cumulative effect of exposure to PaCO2 derangement over time.
Methods
Study design and patients
In this retrospective study, data were collected from the Department of Critical Care Medicine, Zhongda Hospital, Southeast University. Between January 2014 and March 2021, patients with ARDS meeting the Berlin definition [12] who were admitted to the ICU were screened. Eligible patients were 18 years of age or older and received invasive ventilation for at least 24 h. Patients who only received non-invasive ventilation support were excluded. Since ECMO can dramatically affect PaCO2 independent of other respiratory support [13], we excluded that subset of patients. The Research Ethics Commission of Zhongda Hospital approved the present study (approval number: 2022ZDSYLL279-P01) and waived the written informed consent since deidentified data were extracted from the medical record, and the personal information was kept confidential.
Data collection and outcomes
Demographic data, comorbidities, baseline severity scores, clinical outcomes, and laboratory tests were retrospectively collected. Variables at the initiation of mechanical ventilation were defined as the baseline. All results of arterial blood gas analysis during the first five days of invasive ventilation were extracted. The following definitions were applied: hypocapnia (PaCO2 < 35 mmHg), normocapnia (35 mmHg ≤ PaCO2 ≤ 45 mmHg), and hypercapnia (PaCO2 > 45 mmHg). Ventilator parameters, including tidal volume, respiratory rate, positive end-expiratory pressure (PEEP), plateau pressure (Pplat), and peak inspiratory pressure (Ppeak), were monitored and recorded hourly. The weighted average of each parameter was calculated every 8 h, referring to the previous literature [9]. The dynamic driving pressure, mechanical power, and ventilatory ratio were calculated. Therapeutic strategies were collected, including prone position, recruitment maneuvers, neuromuscular blockers, and vasopressors, from Day 1 to Day 5 since mechanical ventilation.
The primary outcome was overall 28-day mortality. Secondary outcomes were ICU and in-hospital mortality and ventilator-free days (VFDs) over 28 days. Patients who died before Day 28 were considered to have zero VFDs. The details of data collection and definition are presented in the supplement.
Statistical analysis
Categorical variables are reported as counts (proportions) and were compared with the chi-square or Fisher’s exact test. Continuous variables are presented as the mean (standard deviation, SD) or median [interquartile range (IQR)] and were compared with Student’s t-test or the Mann–Whitney U test as appropriate.
PaCO2 was measured repeatedly and changed over the follow-up period, which was considered a time-varying covariate. The coefficient of variation for PaCO2 (CV-PaCO2, defined as the percentage of standard deviation to the mean PaCO2 over a specific period), which could reflect the amplitude of change in PaCO2, was also considered a time-varying covariate. Respiratory variables which can influence CO2 elimination [14] and well-established markers of lung injury, such as driving pressure and mechanical power [15, 16] were included as time-varying covariates. To assess the impact of time-dependent PaCO2 exposure on 28-day mortality, the time-dependent Cox model was implemented to adjust for both time-fixed and time-varying covariates [8]. According to previous studies, we adjusted for the severity of illness by adding age, Acute Physiology and Chronic Health Evaluation (APACHE) II score, and PaO2/FiO2 ratio at baseline. Prespecified subgroup analyses were used to investigate whether the effects of time-varying PaCO2 differ in patients categorized by severity, etiology, ventilatory strategies, and ventilation impairment.
We also investigated the association between the cumulative effect of PaCO2 and 28-day mortality. The cumulative exposure of PaCO2 was quantified by the proportion of tests suggestive of normocapnia to the total number of arterial blood gas analyses. The adjusted association between potentially harmful exposure (PaCO2 derangements) and mortality was depicted by Loess smoothing analysis. The number of missing or censoring values is presented in Table S1. Variables with a missing ratio of more than 25% were excluded from the final analysis. Outliers were censored, and missing values of less than 25% were replaced using multiple imputations by chained equations. The statistical analyses were conducted using R version 4.0.2. The level of significance was set at 0.05 (two-tailed).
Results
Patient characteristics
A total of 975 ARDS patients were screened, and we identified 709 patients (Fig. 1) in the final cohort with a total of 10,883 PaCO2 measurements. By Day 5 sicne commencement of mechanical ventilation, 663 patients survived, 474 of whom were still mechanically ventilated. Most patients were men (70.7%), with a mean age of 65 (± 16) years. Pneumonia was the leading cause of lung injury, followed by non-pulmonary sepsis, and more than 80% of patients had a concurrent diagnosis of sepsis (Table 1). Patients exposed to hypocapnia, normocapnia, and hypercapnia at baseline accounted for 54.4%, 33.4%, and 12.1%, respectively.

Flowchart of patient enrolment
The characteristics of respiratory and hemodynamic parameters at baseline are described in Table 2. The mean PaO2/FiO2 and PaCO2 were 202.2 (± 88.5) mmHg and 35.8 (± 12.3) mmHg, respectively. All patients received an average tidal volume of no more than 8 mL/kg predicted body weight (PBW). 18.1% of patients received prone position ventilation, and no more than 10% of patients received recruitment maneuvers or neuromuscular blockers. Compared with the survivors, non-survivors had a lower PaO2/FiO2 and pH, while dynamic driving pressure and mechanical power were significantly higher in the non-survivors. Baseline PaCO2 was comparable in both groups, and the ventilatory ratio was higher in the non-survivors, but the difference was not statistically significant. The survivors were more hemodynamically stabilized, as indicated by the higher mean arterial pressure, lower serum lactate, and fewer requirement of vasopressors. More details about the population are shown in Table S2.
A total of 252 (35.5%) patients died within 28 days after invasive mechanical ventilation. ICU and hospital mortality rates were 26.0% and 27.9%, respectively (Table 1). The overall 28-day mortality was the highest in the hypercapnic patients, followed by the hypocapnic patients, and was the lowest in the normocapnic patients (Fig. 1).
Association between time-varying PaCO2 and 28-day mortality in ARDS patients
After adjusting for age, APACHE II score, PaO2/FiO2, respiratory rate, tidal volume, ventilatory ratio, PEEP, dynamic driving pressure, and mechanical power, both time-varying PaCO2 (HR 1.07, 95% CI 1.03–1.11, p < 0.001) and time-varying CV-PaCO2 (HR 1.24 per 10% increase, 95% CI 1.10–1.40, p < 0.001) were independently associated with an increased hazard of 28-day mortality (Table 3). Additionally, a higher APACHE II score at baseline was independently associated with increased 28-day mortality. The results were largely consistent across sensitivity analysis including patients who still received invasive mechanical ventilation on Day 5 (Table S3).
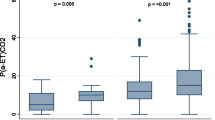
The longitudinal values of the mean daily PaCO2 and coefficient of variation for PaCO2 over the first five days after mechanical ventilation are shown in Fig. 2. There was no significant difference in the mean PaCO2 or CV-PaCO2 between survivors and non-survivors on the first day of mechanical ventilation. PaCO2 gradually increased over time in both groups and was significantly lower in the 28-day survivors than in non-survivors after Day 3 (Fig. 2A). The CV-PaCO2 showed a decreasing tendency in all patients, which meant that the PaCO2 gradually stabilized. Compared with the survivors, the daily CV-PaCO2 was higher in the non-survivors for most of the time (Fig. 2B).

Comparisons of time-varying PaCO2 over time between 28-day survivors and non-survivors at the same time point. A: daily mean PaCO2. B: daily coefficient of variation for PaCO2. *P < 0.05, **P < 0.01, ***P < 0.001
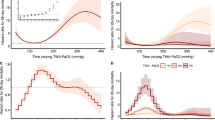
The results of the subgroup analyses of the association between time-varying PaCO2 and CV-PaCO2 with 28-day mortality are shown in Fig. 3. The association seemed to be stronger in patients exhibiting pulmonary ARDS, presenting a low ventilatory ratio (VR < 2), and receiving lung-protective ventilation (tidal volume ≤ 8 mL/kg PBW and dynamic driving pressure ≤ 15 cmH2O), and no interaction was detected.

Subgroup analyses of the association between A: time-varying PaCO2. B: the coefficient of variation for PaCO2 with 28-day mortality
Cumulative effect of PaCO2 on 28-day mortality in ARDS patients
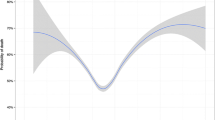
After adjustment for confounders as mentioned above, a higher proportion of normocapnia among all arterial blood gas analyses (HR 0.72 per 10% increase, 95% CI 0.58–0.89, p = 0.002) during the first five days since invasive mechanical ventilation was independently associated with a decreased hazard of death on Day 28 (Table S4). Consistently, the cumulative proportion of exposure to abnormal PaCO2 showed a decreased relationship with 28-day survival (Fig. S1). Similarly, exposure to PaCO2 dysregulation was generally associated with reduced hospital and ICU survival rates as well as shorter VFDs by Day 28 (Fig. S1).
Discussion
These data highlighted the importance of CO2 management in mechanically ventilated ARDS patients. Time-varying PaCO2, measured by daily PaCO2 and the coefficient of variation for PaCO2 during the early phase of mechanical ventilation, independently influenced the clinical outcomes. Additionally, we observed a cumulative effect of PaCO2 derangement over time: every additional exposure to abnormal PaCO2 was associated with an increased risk of death. Therefore, limiting exposure to hypocapnia and hypercapnia in ARDS patients could improve outcomes.
The association between PaCO2 and clinical outcomes has solid biological plausibility. PaCO2 can be significantly influenced by disease severity and clinical management and has profound pathophysiological effects. PaCO2 may increase due to alveolar hypoventilation, resulting from increased dead space and massive shunt fraction or low tidal volume ventilation. Either the increased dead space [17] responsible for hypercapnia, or the hemodynamic instability rendered by hypercapnia [18, 19] is associated with poor outcomes. An important tactic to compensate for gas exchange is to increase cardiac output and subsequently altered lung perfusion [20]. The PaCO2 derangement in the non-survivors may due to hemodynamic impairment. Although studies have found that hypercapnia can alleviate the inflammatory response [21], it may simultaneously inhibit innate immunity and suppress the clearance of pathogens [22, 23].
On the other hand, hypocapnia may occur when high respiratory drive and strong inspiratory efforts or unnecessary high tidal volume ventilation lead to alveolar hyperventilation with a dangerous increase of mechanical power. The high-stretch ventilation caused by patient self-induced lung injury [24] and ventilator-induced lung injury [25] may exacerbate the detrimental effects of hypocapnia. Preclinical studies have revealed that hypocapnia can inhibit the secretion of alveolar surfactant [26] and impair the hypoxic contraction of pulmonary vessels, consequently reducing lung compliance and aggravating the ventilation-perfusion mismatch [27]. To date, there is considerable variability in CO2 management.
Our findings that PaCO2 derangement is associated with an increased mortality rate are consistent with several prior studies [5, 6, 28], although the protocols are diverse. The main difference between the present study and prior studies is the assessment period of PaCO2. Published studies regarding the association between PaCO2 and outcomes are mainly limited to cross-sectional analyses of single-time point data. However, a single measurement of PaCO2 cannot precisely describe the overall PaCO2 during the whole disease course and, therefore, may not necessarily significantly affect mortality. In fact, our study has shown that PaCO2 varies during the early phase of illness. PaCO2 reflects the balance between carbon dioxide production and elimination, and there is no doubt that derangement in PaCO2 may pose high risks for unfavorable outcomes [29]. Our study can be considered a complement and refinement of the previous results by investigating the cumulative effect of abnormal PaCO2 on 28-day mortality.
The importance of dynamic variations in respiratory parameters has been exemplified by longitudinal comparisons of ventilatory ratio and mechanical power in COVID-19 ARDS patients [30, 31]. However, limited data are available regarding the effect of time-varying PaCO2. We focused on longitudinal PaCO2, and the results were generally consistent with prior studies concerning dynamic PaCO2. Tiruvoipati and his colleagues [32] found that in patients with sepsis who received mechanical ventilation, CV-PaCO2 showed a persistent association with an increased odds ratio for mortality, likely reflecting physiological instability. Similarly, an early rapid change in PaCO2 after ECMO in patients with respiratory failure was correlated with an increased risk of neurological complications [33]. Regrettably, none of the above studies investigated the effects of daily PaCO2 in ARDS patients and failed to represent the frequency and persistence of abnormal carbon dioxide exposure. By accounting for baseline confounders and time-dependent PaCO2, we have confirmed the importance of repeated PaCO2 measurements across the entire course or at least during the early phase of mechanical ventilation in ARDS patients.
Our study has certain implications for the clinical practice of critically ill patients. Clinicians should pay close attention to PaCO2 from the start of mechanical ventilation in ARDS patients. Efforts should be made to prevent dramatic changes in PaCO2 and limit exposure to potentially harmful hypocapnia and hypercapnia. In addition to limiting the tidal volume and driving pressure, it is also crucial to ensure adequate alveolar ventilation to facilitate the stabilization of carbon dioxide removal, as indicated by the results of the subgroup analysis performed in the subpopulation that received lung protective ventilation. Rescue therapies such as extracorporeal carbon dioxide removal and ECMO should be initialized when severe hypercapnia persists despite optimal medical management [34, 35]. Moreover, numerous studies have illustrated the association between PaCO2 and clinical outcomes in a large population of non-ARDS patients receiving mechanical ventilation [36, 37]. We speculate that the time-varying PaCO2 may affect the prognosis in non-ARDS patients equally.
To our knowledge, this study is the first to evaluate the effects of time-varying PaCO2 and CV-PaCO2 in ARDS patients and highlight the importance of the cumulative effect of normocapnia. There are several limitations we should acknowledge. First, patients were retrospectively enrolled from a single center which may impede the generalization of the results. Of concern, our cohort is comparable with a national cross-sectional survey of ARDS patients with regard to baseline characteristics [1]. Even though we excluded 92 patients who received ECMO, several studies have found that in patients receiving ECMO, PaCO2 derangements, as well as large relative changes in PaCO2, were associated with poor prognosis, supporting our results [32, 38]. Second, this observational study could not lead to causal inferences for any associations. Third, the frequency of PaCO2 measurements differs among patients, depending on the severity of the disease. It was perhaps impossible to accurately estimate the cumulative time that patients were exposed to abnormal PaCO2. Calculating the ratio of the number of normocapnic cases to the total number of tests may be a reasonable method to quantify the cumulative effect. Fourth, due to the limited number of enrolled patients and insufficient data on PaCO2 measurements, we only included the first five days of mechanical ventilation. We may have overlooked the impact of time-varying PaCO2 on clinical outcomes in the subsequent course of the illness. Nevertheless, epidemiological studies have found that the median duration of ventilation for ARDS patients was 6 to 8 days [1, 2]. Thus, the analysis of longitudinal PaCO2 for five days still makes sense. Finally, since PaCO2 variation over time could not comprehensively describe the complexity of ARDS severity and evolution, in addition that modifications of ventilatory parameters may make a difference in prognosis, there remains a paucity of prospective data and evidence to interpret the effect of those time-varying variables.
Conclusion
In conclusion, PaCO2 should be carefully monitored in ARDS patients, especially during the early course of mechanical ventilation. Substantial variations in PaCO2 and cumulative exposure to PaCO2 derangements were found in this study to be independently associated with an increase in 28-day mortality. Prospective studies may further clarify the effects of PaCO2 and optimize the early management of CO2.
Availability of data and materials
The dataset used during the current study are available from the corresponding author on reasonable request.
Abbreviations
- APACHE II:
-
Acute Physiology and Chronic Health Evaluation II
- ICU:
-
intensive care unit
- FiO2 :
-
fraction of inspired oxygen
- PaO2 :
-
Partial arterial oxygen pressure
- PaCO2 :
-
partial arterial carbon dioxide pressure
- PEEP:
-
positive end-expiratory pressure
- CV:
-
coefficient of variation
- PBW:
-
predicted body weight
- ICU:
-
intensive care unit
- LOS:
-
length of stay
- VFD:
-
ventilator-free day
References
Liu L, Yang Y, Gao Z, Li M, Mu X, Ma X, et al. Practice of diagnosis and management of acute respiratory distress syndrome in mainland China: a cross-sectional study. J Thorac Dis. 2018;10(9):5394–404.
Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of Care, and mortality for patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 countries. JAMA. 2016;315(8):788–800.
Huang X, Zhang R, Fan G, Wu D, Lu H, Wang D, et al. Incidence and outcomes of acute respiratory distress syndrome in intensive care units of mainland China: a multicentre prospective longitudinal study. Crit Care. 2020;24(1):515.
Radermacher P, Maggiore SM, Mercat A. Fifty years of Research in ARDS. Gas Exchange in Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017;196(8):964–84.
Madotto F, Rezoagli E, McNicholas BA, Pham T, Slutsky AS, Bellani G, et al. Patterns and impact of arterial CO(2) management in patients with Acute Respiratory Distress Syndrome: insights from the LUNG SAFE study. Chest. 2020;158(5):1967–82.
Nin N, Muriel A, Peñuelas O, Brochard L, Lorente JA, Ferguson ND, et al. Severe hypercapnia and outcome of mechanically ventilated patients with moderate or severe acute respiratory distress syndrome. Intensive Care Med. 2017;43(2):200–8.
Iqbal N, Irfan M, Zubairi ABS, Awan S, Khan JA. Association of hypercapnia on admission with increased length of hospital stay and severity in patients admitted with community-acquired pneumonia: a prospective observational study from Pakistan. BMJ Open. 2017;7(6):e013924.
Zhang Z, Reinikainen J, Adeleke KA, Pieterse ME, Groothuis-Oudshoorn CGM. Time-varying covariates and coefficients in Cox regression models. Ann Transl Med. 2018;6(7):121.
Bos LDJ, Sjoding M, Sinha P, Bhavani SV, Lyons PG, Bewley AF, et al. Longitudinal respiratory subphenotypes in patients with COVID-19-related acute respiratory distress syndrome: results from three observational cohorts. Lancet Respir Med. 2021;9(12):1377–86.
Urner M, Jüni P, Hansen B, Wettstein MS, Ferguson ND, Fan E. Time-varying intensity of mechanical ventilation and mortality in patients with acute respiratory failure: a registry-based, prospective cohort study. Lancet Respir Med. 2020;8(9):905–13.
Libório AB, Barbosa ML, Sá VB, Leite TT. Impact of loop diuretics on critically ill patients with a positive fluid balance. Anaesthesia. 2020;75(Suppl 1):e134–e42.
Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307(23):2526–33.
Combes A, Schmidt M, Hodgson CL, Fan E, Ferguson ND, Fraser JF, et al. Extracorporeal life support for adults with acute respiratory distress syndrome. Intensive Care Med. 2020;46(12):2464–76.
Tusman G, Bohm SH, Suarez-Sipmann F, Scandurra A, Hedenstierna G. Lung recruitment and positive end-expiratory pressure have different effects on CO2 elimination in healthy and sick lungs. Anesth Analg. 2010;111(4):968–77.
Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372(8):747–55.
Costa ELV, Slutsky AS, Brochard LJ, Brower R, Serpa-Neto A, Cavalcanti AB, et al. Ventilatory variables and mechanical power in patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2021;204(3):303–11.
Morales-Quinteros L, Schultz MJ, Bringué J, Calfee CS, Camprubí M, Cremer OL, et al. Estimated dead space fraction and the ventilatory ratio are associated with mortality in early ARDS. Ann Intensive Care. 2019;9(1):128.
Repessé X, Vieillard-Baron A. Hypercapnia during acute respiratory distress syndrome: the tree that hides the forest! J Thorac Dis. 2017;9(6):1420–5.
Barnes T, Zochios V, Parhar K. Re-examining Permissive Hypercapnia in ARDS: a narrative review. Chest. 2018;154(1):185–95.
Wagner PD. The physiological basis of pulmonary gas exchange: implications for clinical interpretation of arterial blood gases. Eur Respir J. 2015;45(1):227–43.
Marongiu I, Spinelli E, Scotti E, Mazzucco A, Wang YM, Manesso L, et al. Addition of 5% CO(2) to Inspiratory Gas prevents Lung Injury in an experimental model of Pulmonary Artery Ligation. Am J Respir Crit Care Med. 2021;204(8):933–42.
Casalino-Matsuda SM, Wang N, Ruhoff PT, Matsuda H, Nlend MC, Nair A, et al. Hypercapnia alters expression of Immune Response, Nucleosome Assembly and lipid metabolism genes in differentiated human bronchial epithelial cells. Sci Rep. 2018;8(1):13508.
Casalino-Matsuda SM, Chen F, Gonzalez-Gonzalez FJ, Nair A. Hypercapnia suppresses macrophage antiviral activity and increases mortality of Influenza a infection via Akt1. J Immunol. 2020;205(2):489–501.
Vaporidi K, Akoumianaki E, Telias I, Goligher EC, Brochard L, Georgopoulos D. Respiratory drive in critically ill patients. Pathophysiology and clinical implications. Am J Respir Crit Care Med. 2020;201(1):20–32.
Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013;369(22):2126–36.
Kiefmann M, Tank S, Tritt MO, Keller P, Heckel K, Schulte-Uentrop L, et al. Dead space ventilation promotes alveolar hypocapnia reducing surfactant secretion by altering mitochondrial function. Thorax. 2019;74(3):219–28.
Curley G, Kavanagh BP, Laffey JG. Hypocapnia and the injured brain: more harm than benefit. Crit Care Med. 2010;38(5):1348–59.
Tiruvoipati R, Pilcher D, Buscher H, Botha J, Bailey M. Effects of Hypercapnia and Hypercapnic Acidosis on Hospital Mortality in mechanically ventilated patients. Crit Care Med. 2017;45(7):e649–e56.
Marhong J, Fan E. Carbon dioxide in the critically ill: too much or too little of a good thing? Respir Care. 2014;59(10):1597–605.
Beloncle F, Studer A, Seegers V, Richard JC, Desprez C, Fage N, et al. Longitudinal changes in compliance, oxygenation and ventilatory ratio in COVID-19 versus non-COVID-19 pulmonary acute respiratory distress syndrome. Crit Care. 2021;25(1):248.
Kaku N, Nakagama Y, Shirano M, Shinomiya S, Shimazu K, Yamazaki K, et al. Longitudinal ventilatory ratio monitoring for COVID-19: its potential in predicting severity and assessing treatment response. Crit Care. 2021;25(1):366.
Cavayas YA, Munshi L, Del Sorbo L, Fan E. The early change in Pa(CO(2)) after extracorporeal membrane oxygenation initiation is Associated with neurological complications. Am J Respir Crit Care Med. 2020;201(12):1525–35.
Tiruvoipati R, Serpa Neto A, Young M, Marhoon N, Wilson J, Gupta S, et al. An exploratory analysis of the Association between Hypercapnia and Hospital Mortality in critically ill patients with Sepsis. Ann Am Thorac Soc. 2022;19(2):245–54.
Combes A, Fanelli V, Pham T, Ranieri VM. Feasibility and safety of extracorporeal CO(2) removal to enhance protective ventilation in acute respiratory distress syndrome: the SUPERNOVA study. Intensive Care Med. 2019;45(5):592–600.
Tonna JE, Abrams D, Brodie D, Greenwood JC, Rubio Mateo-Sidron JA, Usman A, et al. Management of adult patients supported with venovenous extracorporeal membrane oxygenation (VV ECMO): Guideline from the extracorporeal life support Organization (ELSO). ASAIO J. 2021;67(6):601–10.
Fuller BM, Mohr NM, Drewry AM, Ferguson IT, Trzeciak S, Kollef MH, et al. Partial pressure of arterial carbon dioxide and survival to hospital discharge among patients requiring acute mechanical ventilation: a cohort study. J Crit Care. 2017;41:29–35.
Yokoyama S, Hifumi T, Okazaki T, Noma T, Kawakita K, Tamiya T, et al. Association of abnormal carbon dioxide levels with poor neurological outcomes in aneurysmal subarachnoid hemorrhage: a retrospective observational study. J Intensive Care. 2018;6:83.
Diehl A, Burrell AJC, Udy AA, Alexander PMA, Rycus PT, Barbaro RP, et al. Association between arterial Carbon Dioxide Tension and clinical outcomes in venoarterial extracorporeal membrane oxygenation. Crit Care Med. 2020;48(7):977–84.
Acknowledgements
We thank the Intensive Care Unit of Zhongda Hospital, School of Medicine, Southeast University (Nanjing, China) for their helpful support.
Funding
This work was supported by the Clinical Science and Technology Specific Projects of Jiangsu Province (BE2020786), National Science and Technology Major Project (2022YFC2504400), the National Natural Science Foundation of China (81870066, 82270083), the Second Level Talents of the “333 High Level Talents Training Project” in the sixth phase in Jiangsu (LGY2022025), and Jiangsu Provincial Geriatric Health Research Project (LD2021010).
Author information
Authors and Affiliations
Contributions
RZ carried out the design and drafted the manuscript, RZ, RT and ZL participated in the collection and assembly of data. HC, YY and HQ participated in the manuscript revision. LL finally approved this research and manuscript. All authors read and approved the final version before submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Research Ethics Commission of Zhongda Hospital, School of Medicine, Southeast University approved by the study, and waived the informed consent. All methods were carried out in accordance with declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, R., Chen, H., Teng, R. et al. Association between the time-varying arterial carbon dioxide pressure and 28-day mortality in mechanically ventilated patients with acute respiratory distress syndrome. BMC Pulm Med 23, 129 (2023). https://doi.org/10.1186/s12890-023-02431-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-023-02431-6