
Abstract
Background
Surgical resection is usually recommended for the treatment of pulmonary sclerosing pneumocytoma (PSP). However, no comparative study has demonstrated that surgical resection leads to improved outcomes. We aimed to compare all-cause mortality between patients with PSP who underwent surgery or did not and those without PSP.
Methods
Participants aged ≥18 years who had pathologically diagnosed PSP between 2001 to 2018, at 3 hospitals were included. Randomly selected (up to 1:5) age-, sex-, and smoking status-matched controls without PSP who were randomly selected from those who underwent health checkups including chest CT were included. Mortality was compared using Kaplan–Meier estimates and Cox proportional hazards regression models. Literature review of studies reporting PSP was also conducted.
Results
This study included 107 patients with PSP (surgery:non-surgery, 80:27) and 520 matched controls. There were no cases of lymph node or distant metastasis, recurrence, or mortality from PSP. No significant difference in all-cause mortality risk was observed between the PSP surgery, PSP non-surgery, and non-PSP groups (log rank test P = 0.78) (PSP surgery vs. non-PSP: adjusted hazards ratio [aHR], 1.80; 95% confidence interval [CI], 0.22–14.6; PSP non-surgery vs. non-PSP: aHR, 0.77; 95% CI, 0.15–3.86; PSP surgery vs. PSP non-surgery: aHR, 2.35; 95% CI, 0.20–28.2). In the literature review, we identified 3469 patients with PSP from 355 studies. Only 1.33% of these patients reported metastasis, recurrence, or death.
Conclusions
All-cause mortality did not differ between patients with PSP and those without, irrespective of undergoing surgery. Our study and the literature review suggest that PSP has less impact on increased mortality risk.
Similar content being viewed by others


Background
Pulmonary sclerosing pneumocytoma (PSP) is a rare neoplasm that was first described by Liebow and Hubbell in 1956 as sclerosing hemangioma [1]. Sclerosing hemangioma was renamed PSP and categorized into “adenoma” by World Health Organization in 2015 [2]. Although PSP was previously considered a vascular neoplasm, it is currently understood as a tumor originating from the primitive respiratory epithelium [3]. PSP is predominant in middle-aged women with increased prevalence in Asians [4, 5]. PSP is mainly found incidentally. More than 70% of patients with PSP are asymptomatic. Symptoms of PSP include hemoptysis, chronic cough, and chest pain [6]. It is generally observed as a slow-growing well-circumscribed nodule with high-strength homogeneous enhancement on computed tomography (CT) [7].
Surgical resection is usually recommended for the treatment of PSP [6] considering that cases with lymph node metastasis [3, 8,9,10,11,12,13,14], distant or pleural metastasis [15,16,17], recurrence [18], malignant transformation [19] and death [20] have been reported. However, as most patients with PSP show a benign indolent course, not all patients with PSP undergo surgical resection clinically [21]. In fact, it has not been clarified whether surgical resection leads to better outcomes. No study has compared outcomes between patients with PSP who underwent surgery and those who did not. In addition, it has not been investigated whether those with PSP have a higher mortality risk than those without PSP. Therefore, we aimed to investigate the treatment outcomes and prognosis of patients with PSP, including those who underwent surgery and those who did not.
Methods
Study design and participants
Participants who were diagnosed with PSP pathologically confirmed at tertiary hospitals (Seoul National University Hospital, Seoul National University Bundang Hospital and Seoul National University Seoul Metropolitan Government Boramae Medical Center) between January 1, 2001, and December 31, 2018 (“PSP group”) were enrolled. Those who were under 18 years of age and who lacked mortality information were excluded. Participants in the PSP group were categorized into “PSP surgery group” and “PSP non-surgery group” based on the treatment undergone for PSP. Participants in the PSP group were matched with up to five age-, sex-, and smoking status-matched controls without PSP who were randomly selected from those who underwent health checkups including chest CT at a health screening center (Seoul National University Healthcare System Gangnam Center) between October 2004 and December 2013 (“non-PSP group”). In the control group, those who presented with nodules suspicious of PSP on chest CT and those who had undergone lung surgery were excluded.
Their medical records, operative procedures, histological examinations, and outpatient clinic follow-up data were reviewed retrospectively. In the PSP group, we investigated age, sex, body mass index (BMI), smoking status, comorbidity, first department visit, initial symptoms, and tumor size, location, and number. In addition, we analyzed initial diagnostic methods, surgery methods, whether the lymph node was enlarged on chest CT, and whether lymph nodes were dissected during surgery, as well as the presence of lymph node metastasis, distant metastasis, and recurrence. In the non-PSP group, we collected data on age, sex, BMI, smoking status, and comorbidity. The index date for statistics was defined as the date of the first biopsy or surgery performed in the PSP group and chest CT performed in the non-PSP group. Comorbidities were identified based on the International Classification of Diseases, 10th Revision codes registered before the index date. Comorbidities were classified as follows: hypertension (I10), diabetes mellitus (E10–E14), dyslipidemia (E78), respiratory diseases, cardiovascular diseases (I20–I25, I50, I110), chronic liver diseases (K703, except K7039, K717, K740–746, K761, P788), chronic kidney diseases (E10.2x, E11.2x, E13.2x, E14.2x, I12.0, I12.9, I13.x, N18, N19), and malignancy (C00–C97). Respiratory diseases were investigated in patients with pulmonary tuberculosis (A15, A16, A19, B909), nontuberculous mycobacterial pulmonary disease (A31, except A311), chronic obstructive pulmonary disease (J44), asthma (J45 and J46), bronchiectasis (J47, Q334), and interstitial lung disease (J70, J84).
The primary outcome was all-cause mortality. Mortality information, including that on the causes of death, was collected from the Korean National Statistical Office. This study was approved and the requirement for written informed consent was waived by the institutional review board of Seoul National University Hospital (IRB no. H-1607-038-774). The study was conducted in accordance with the tenets of the Declaration of Helsinki.
Statistical analysis
We compared the baseline characteristics between the PSP surgery group and PSP non-surgery groups using Student’s t-tests for continuous variables and chi-squared tests or Fisher’s exact tests for categorical variables. Paired t-tests and McNemar tests were used to compare the PSP group and the matched non-PSP group. Kaplan–Meier curves with log-rank tests and Cox proportional hazards regression adjusted by covariates were used to compare the all-cause mortality risk between the groups. A proportional hazards assumption was also tested using Schoenfeld residuals. The estimates of mortality risk were presented as adjusted hazard ratios (aHRs) and their 95% confidence intervals (CIs). Statistical significance was set at p < 0.05. All analyses were performed using Stata 14.2 (StataCorp., College Station, TX, USA) and SPSS version 26 (IBM, Armonk, NY, USA).
Literature review
We conducted a literature review of studies that reported patients with PSP. We identified studies on PSP using the terms “pulmonary sclerosing pneumocytoma,” “pulmonary sclerosing hemangioma,” “pneumocytoma of the lung,” and “sclerosing hemangioma of the lung” on PUBMED. Original articles, case reports, case series, and review articles that reported the total number of patients and the number of metastases, recurrence, or death were included in the review. After removing duplicate data, we counted the number of patients who reported with PSP, lymph node metastases, distant metastases, or recurrence and the global mortality rate of PSP since the first PSP case was reported in 1956 [1].
Results
Participants
The study flow diagram is shown in Fig. 1. A total of 107 patients with PSP were included. Most (91.6%) were women, and the mean age was 50.6 ± 12.5 years. Of these, 80 patients underwent surgery (PSP surgery group) and 27 patients were categorized into the PSP non-surgery group, and there were no significant differences in baseline characteristics (Table 1).

Study flow diagram
A total of 520 age-, sex-, and smoking status-matched controls were included. The baseline characteristics of the PSP and non-PSP groups are summarized in Supplementary Table S1. The PSP group had a higher mean BMI and higher rates of diabetes mellitus, cardiovascular diseases, chronic liver diseases, and malignancy.
Tumor characteristics of PSP group
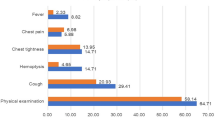
The tumor characteristics of patients in the PSP group are summarized in Table 2. The rate of not performing surgery was significantly higher when the patient first visited the pulmonology department than the thoracic surgery department. The majority (79.4%) of the patients had no symptoms and the remaining 20.6% had symptoms. Cough was the most common symptom at 9.3%, and hemoptysis occurred in 2.8%. Three out of 107 patients (2.8%) underwent surgery due to repeated symptoms that reduced their quality of life. All symptoms were hemoptysis, and the hemoptysis improved after surgery in all three patients. In particular, there was one person who had a blood-tinged sputum that repeats for about a month every year. Eventually, the operation was performed and the blood-tinged sputum improved. Less than a fifth had a tumor size > 3 cm. There were no significant differences in the presence of symptoms and tumor size between the PSP surgery group and PSP non-surgery groups. Most of them were single lesions, but four patients (3.7%) showed two lesions, and all of them underwent surgery. In the PSP surgery group, one-third of the patients were diagnosed by either percutaneous needle biopsy (n = 24) or bronchoscopic biopsy (n = 3), including two cases confirmed by endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA), before surgery. Lymph node enlargement was observed on chest CT in seven patients. In the PSP surgery group, lymph node dissection was performed in 47.5% of the patients. During diagnosis and follow-up over 87.4 ± 52.0 months, there were no cases of lymph node metastasis, distant metastasis, or recurrence.
All-cause mortality
Two (1.86%) deaths in the PSP surgery group (91.5 ± 55.5 months) and one (0.93%) death in the PSP non-surgery group (75.1 ± 38.1 months) were observed during a follow-up period of 87.4 ± 52.0 months. There were no cases of PSP-related deaths. There were 14 deaths in the non-PSP group. There was no significant difference in all-cause mortality risk between the PSP surgery group, PSP non-surgery group, and non-PSP group based on Kaplan–Meier estimates (log-rank test, P = 0.78). Multivariable Cox proportional hazards regression also showed that there were no differences in all-cause mortality risk between groups, even after adjustment for age, sex, BMI, smoking status, and comorbidities (PSP surgery group vs. non-PSP group: aHR, 1.80; 95% CI, 0.22–14.6; PSP non-surgery group vs. non-PSP group: aHR, 0.77; 95% CI, 0.15–3.86; PSP surgery group vs. PSP non-surgery group: aHR, 2.35; 95% CI, 0.20–28.2). An assumption of proportional hazards was not rejected (P > 0.99) (Fig. 2).

Comparisons of all-cause mortality risk between groups. PSP, pulmonary sclerosing pneumocytoma
Literature review
We reviewed all PSP cases, lymph node metastases, distant metastases, recurrence, and deaths published worldwide over 65 years since the first case of PSP reported in 1956 (Supplementary Table S2). We identified 355 studies that reported the total number of patients and the number of metastases, recurrence, or death. To date, 3469 patients with PSP have been reported. Among them, there were 38 cases with lymph node metastases, 6 distant and pleural metastases, 4 recurrences, and 1 death.
Discussion
The principal finding of the current study was that there were no differences in all-cause mortality risk between the PSP surgery group, PSP non-surgery group, and non-PSP group. To our knowledge, this is the first study to investigate the all-cause mortality risk of patients with PSP based on the treatment undergone compared with those without PSP. To date, the all-cause mortality risk of patients with PSP has not been reported, although mortality is the most important factor in treatment outcomes and prognosis in patients with tumors. In addition, no studies have compared outcomes based on undergoing surgical resection by the patients with PSP. Although surgical resection has been considered a treatment option [6, 14], the results of the present study questions the validity of surgical resection in all cases of PSP. The PSP surgery group did not show better survival than the PSP non-surgery group in our study. The two groups had similar baseline characteristics, including age, sex, smoking status, comorbidities, tumor size, and lymph node enlargement. Even the PSP non-surgery group showed a comparable all-cause mortality risk to age-, sex-, and smoking status-matched non-PSP control group.
The small impact of PSP on all-cause mortality might be explained by the benign nature of the tumor. There were no PSP-related deaths among the participants of our study. But one case of PSP-related death was identified through an extensive literature review [20]. It was the first case of death from respiratory and circulatory failure due to a large, multiple PSP tumor and lymph node and extrapulmonary metastases (liver, abdominal cavity, bone) compressing mediastinal tissue. In addition, we could identify only one serious PSP patient from the literature reviews, who had experienced respiratory arrest due to airway obstruction by endobronchial PSP, which improved after pneumonectomy [22].
The main reason for surgical resection of PSP is the suspicion of early-stage lung cancer. In 1986, Tanaka et al. reported the first case of PSP with lymph node metastasis [8]. In a relatively large series of published PSP cases, only 1 out of 100 and 3 out of 239 PSP patients showed lymph node metastases [3, 13]. These reports suggested that PSP may be potentially malignant. When we extensively searched all references regarding PSP, we identified a total of 38 cases of PSP with lymph node metastases [3, 8,9,10,11,12,13,14], 6 with distant and pleural metastases [15,16,17], 4 with recurrence [18], 1 with massive necrosis and vascular invasion [23] and 1 with death [20]. However, considering that 3469 PSP cases were reported in the past 65 years after the reporting of the first PSP case, only 1.33% of PSP cases can be regarded as malignant. Interestingly, there was only one death due to PSP in these patients presenting with metastasis or recurrence, suggesting that PSP does not have a significant impact on prognosis even if metastasis or recurrence occurs. Recently, a case of malignant transformation in both cuboidal surface cells and stromal round cells was confirmed for the first time, but it was reported as an outpatient follow-up state without recurrence or metastasis after surgery [19]. Rather, lung resection surgery might lead to significant complications, including prolonged air leak, bronchopleural fistula, pneumonia, acute respiratory failure, hemorrhage, atelectasis, pneumothorax, bronchospasm, pulmonary embolism, acute respiratory distress syndrome, and cardiovascular complications [24] affecting prognosis, although there were no deaths immediately after surgery in our study. Therefore, it could be helpful to identify the risk group requiring surgery among patients with PSP. Among the prior studies related to this, it was reported that PSP patients with spindle cells or male patients may be more prone to metastasis [13]. Another study reported that young male patients are prone to lymph node metastasis, and the tumor size is larger [25]. Moreover, resection has been performed to confirm the diagnosis in lesions that were otherwise not possible by endoscopic or percutaneous biopsy [26], to relieve local compression of adjacent structures [27, 28], or in the setting of mixed histology of PSP combined with another more aggressive tumor [29]. However, in the present study, we could not determine surgery candidates because there was no patient who presented with metastasis, recurrence, or death from PSP. Further studies related to the surgical indications are required.
The strengths of the current study are as follows. This is the first study to investigate the all-cause mortality risk of patients with PSP. A long-term follow-up duration (87.4 ± 52.0 months) is another advantage of our study. Comorbidities were included as confounders of mortality risk in the multivariate analysis. We also reviewed reports on PSP cases, lymph nodes, distant metastases, recurrence, and deaths published worldwide in 65 years since the first PSP case was reported.
Conclusions
In conclusion, PSP did not affect all-cause mortality, regardless of whether surgery was performed, compared to those without PSP. Our study and the literature review suggest that PSP has less impact on an increased mortality risk. Efforts should be made through further studies to identify subgroups that actually require surgery rather than performing surgical resection in all patients with PSP.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PSP:
-
Pulmonary sclerosing pneumocytoma
- CT:
-
Computed tomography
- BMI:
-
Body mass index
References
Liebow AA, Hubbell DS. Sclerosing hemangioma (histiocytoma, xanthoma) of the lung. Cancer. 1956;9(1):53–75.
Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB, Chirieac LR, Dacic S, Duhig E, Flieder DB, et al. The 2015 World Health Organization classification of lung tumors impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015;10(9):1243–60.
Devouassoux-Shisheboran M, Hayashi T, Linnoila RI, Koss MN, Travis WD. A clinicopathologic study of 100 cases of pulmonary sclerosing hemangioma with immunohistochemical studies: TTF-1 is expressed in both round and surface cells, suggesting an origin from primitive respiratory epithelium. Am J Surg Pathol. 2000;24(7):906–16.
Zhu J. Analysis of the clinical differentiation of pulmonary sclerosing pneumocytoma and lung cancer. J Thorac Dis. 2017;9(9):2974–81.
Yang CH, Lee LY. Pulmonary sclerosing pneumocytoma remains a diagnostic challenge using frozen sections: a clinicopathological analysis of 59 cases. Histopathology. 2018;72(3):500–8.
Lei Y, Yong D, Jun-Zhong R, Zhi Y, Zi-Tong W. Treatment of 28 patients with sclerosing hemangioma (SH) of the lung. J Cardiothorac Surg. 2012;7(1):34.
Shin SY, Kim MY, Oh SY, Lee HJ, Hong SA, Jang SJ, Kim SS. Pulmonary sclerosing pneumocytoma of the lung: CT characteristics in a large series of a tertiary referral center. Medicine (Baltimore). 2015;94(4):e498.
Tanaka I, Inoue M, Matsui Y, Oritsu S, Akiyama O, Takemura T, Fujiwara M, Kodama T, Shimosato Y. A case of pneumocytoma (so-called sclerosing hemangioma) with lymph node metastasis. Jpn J Clin Oncol. 1986;16(1):77–86.
Yano M, Yamakawa Y, Kiriyama M, Hara M, Murase T. Sclerosing hemangioma with metastases to multiple nodal stations. Ann Thorac Surg. 2002;73(3):981–3.
Miyagawa-Hayashino A, Tazelaar HD, Langel DJ, Colby TV. Pulmonary sclerosing hemangioma with lymph node metastases: report of 4 cases. Arch Pathol Lab Med. 2003;127(3):321–5.
Kim KH, Sul HJ, Kang DY. Sclerosing hemangioma with lymph node metastasis. Yonsei Med J. 2003;44(1):150–4.
Pokharel S, Dhillon SS, Ylagan L, George S, Yendamuri S. Sclerosing Pneumocytoma with lymph node metastasis. J Thorac Oncol. 2016;11(10):1802–4.
Gao Q, Zhou J, Zheng Y, Cui J, Teng X. Clinical and histopathological features of pulmonary sclerosing pneumocytoma with dense spindle stromal cells and lymph node metastasis. Histopathology. 2020;77(5):718–27.
Kocaman G, Yenigun MB, Ersoz CC, Sak SD, Enon S. Pulmonary sclerosing pneumocytoma with mediastinal lymph node metastasis: a case report. Gen Thorac Cardiovasc Surg. 2021;69(1):142–6.
Bae YS, Ro JY, Shim HS, Hong SW, Yoon SO. Pulmonary sclerosing haemangioma with metastatic spread to stomach. Histopathology. 2012;60(7):1162–4.
Kim MK, Jang SJ, Kim YH, Kim SW. Bone metastasis in pulmonary sclerosing hemangioma. Korean J Intern Med. 2015;30(6):928–30.
Suzuki H, Saitoh Y, Koh E, Hoshino H, Kase D, Kasei Y, Azuhata Y, Kishi H, Hiroshima K, Sekine Y. Pulmonary sclerosing hemangioma with pleural dissemination: report of a case. Surg Today. 2011;41(2):258–61.
Wei S, Tian J, Song X, Chen Y. Recurrence of pulmonary sclerosing hemangioma. Thorac Cardiovasc Surg. 2008;56(2):120–2.
Teng X, Teng XD. First report of pulmonary sclerosing pneomucytoma with malignant transformation in both cuboidal surface cells and stromal round cells: a case report. BMC Cancer. 2019;19(1):1–7.
Zhang W, Liu Y, Chai Y, Shi K, Chen J, Shi D, Wu X. Case report: rare pulmonary Sclerosing Pneumocytoma: large, multiple, metastatic, and fatal. Front Med (Lausanne). 2021;8:661032.
Khanna A, Alshabani K, Mukhopadhyay S, Lam L, Ghosh S. Sclerosing pneumocytoma: case report of a rare endobronchial presentation. Medicine (Baltimore). 2019;98(15):e15038.
Latif MJ, Rahman GF, Connery CP. Respiratory arrest caused by endobronchial sclerosing hemangioma of the left main bronchus. J Bronchology Interv Pulmonol. 2009;16(3):188–90.
Sakai T, Miyoshi T, Umemura S, Suzuki J, Nakasone S, Okada S, Tane K, Aokage K, Goto K, Motoi N, et al. Large pulmonary sclerosing pneumocytoma with massive necrosis and vascular invasion: a case report. Oxf Med Case Reports. 2019;2019(7):omz066.
Steéphan F, Boucheseiche S, Hollande J, Flahault A, Cheffi A, Bazelly B, Bonnet FJC. Pulmonary complications following lung resection: a comprehensive analysis of incidence and possible risk factors. Chest. 2000;118(5):1263–70.
Adachi Y, Tsuta K, Hirano R, Tanaka J, Minamino K, Shimo T, Ikehara S. Pulmonary sclerosing hemangioma with lymph node metastasis: a case report and literature review. Oncol Lett. 2014;7(4):997–1000.
Lovrenski A, Vasilijevic M, Panjkovic M, Tegeltija D, Vuckovic D, Baros I, Lovrenski J. Sclerosing Pneumocytoma: a ten-year experience at a Western Balkan University hospital. Medicina-Lithuania. 2019;55(2):27.
Ikeda M, Okada Y, Hagiwara K, Murata Y, Kanayama T, Hara A, Fujinaga T. A case of pulmonary sclerosing pneumocytoma in the hilar lesion. Gen Thorac Cardiovasc Surg. 2019;67(9):818–20.
Celik A, Akpek M, Calapkorur B, Ozdogru I. Giant sclerosing hemangioma of the lung causing compression to the heart. Turk Kardiyol Dern Ars. 2010;38(8):589.
Wang Z, Yang MQ, Huang WJ, Zhang D, Xu HT. Sclerosing pneumocytoma mixed with a typical carcinoid tumor: a case report and review of literature. Medicine (Baltimore). 2019;98(5):e14315.
Acknowledgments
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
S.K., H.K. C.L. and S.C were involved in the cohort selection and data analysis. S.K. and C.L. wrote the main manuscript. All authors reviewed the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved and the requirement for written informed consent was waived by the institutional review board of Seoul National University Hospital (IRB no. H-1607-038-774). The study was conducted in accordance with the tenets of the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Characteristics of patients with pulmonary sclerosing pneumocytoma and age-, sex-, and smoking status-matched controls. Table S2. Review of pulmonary sclerosing pneumocytoma cases with lymph node metastases, distant metastases, recurrence, and deaths published worldwide.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kim, S.J., Kang, HR., Lee, C.G. et al. Pulmonary sclerosing pneumocytoma and mortality risk. BMC Pulm Med 22, 404 (2022). https://doi.org/10.1186/s12890-022-02199-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-022-02199-1