
Abstract
Background
Usual clinical practice for arterial blood gas analysis (BGA) in conscious patients involves a one-time arterial puncture to be performed after a resting period of 20–30 min. The aim of this study was to evaluate the use of transcutaneous BGA for estimating this gold standard arterial BGA.
Methods
Spontaneously breathing Asian adults (healthy volunteers and respiratory patients) were enrolled (n = 295). Transcutaneous PO2 (PtcO2) and PCO2 (PtcCO2) were monitored using a transcutaneous monitor (TCM4, Radiometer Medical AsP, Denmark) with sensors placed on the chest, forearm, earlobe or forehead. Transcutaneous BGA at 1-min intervals was compared with arterial BGA at 30 min. Reasonable steps to find severe hypercapnia with PaCO2 > 50 mmHg were evaluated.
Results
Sensors on the chest and forearm were equally preferred and used because of small biases (n = 272). The average PCO2 bias was close to 0 mmHg at 4 min, and was almost constant (4–5 mmHg) with PtcCO2 being higher than PaCO2 at ≥8 min. The limit of agreement for PCO2 narrowed over time: ± 13.6 mmHg at 4 min, ± 7.5 mmHg at 12–13 min, and ± 6.3 mmHg at 30 min. The limit of agreement for PO2 also narrowed over time (± 23.1 mmHg at 30 min). Subgroup analyses showed that the PaCO2 and PaO2 levels, gender, and younger age significantly affected the biases. All hypercapnia subjects with PaCO2 > 50 mmHg (n = 13) showed PtcCO2 ≥ 50 mmHg for until 12 min.
Conclusions
Although PtcCO2 is useful, it cannot completely replace PaCO2 because PCO2 occasionally showed large bias. On the other hand, the prediction of PaO2 using PtcO2 was unrealistic in Asian adults. PtcCO2 ≥ 50 mmHg for until 12 min can be used as a screening tool for severe hypercapnia with PaCO2 > 50 mmHg.
Similar content being viewed by others

Background
The partial pressure of blood gases can be estimated through measurement of dissolved gases that diffuse to the skin surface [1, 2]. Measurement of transcutaneous PO2 (PtcO2) and PCO2 (PtcCO2) requires local heating of the skin, which dilates vessels and increases arterial blood supply to the skin capillary bed under the sensor, resulting in accelerated gas diffusion [3, 4]. In clinical practice, this method is widely used to assess pulmonary gas exchange function in infants and children, and in adults with acute or chronic respiratory failure [5,6,7]. It may also be applied to monitoring the condition of patients on mechanical ventilation and managing limb ischemia [8,9,10].
Although previous studies have investigated the relationship between PtcCO2 and PaCO2 over time, the time courses of transcutaneous data for the estimation of arterial blood gas analysis (BGA) are not well characterized [11,12,13]. Various factors may influence the time course of agreement including the response speed of the electromechanical gas measuring system, the speed of skin heating, and the time to equilibration of gases [3, 13,14,15]. This information would allow physicians to choose a convenient (early) time-point for transcutaneous BGA for the estimation of arterial BGA and an optimal time-point for increased accuracy.
A previous study suggested that the correlation between arterial BGA and transcutaneous BGA data via sensors on the chest is stronger than that observed via sensors on the arm; however, this report involved only anesthetized adult patients [16]. The most commonly recommended sensor location, according to the guidelines established by the American Association for Respiratory Care, is the upper chest followed by the lateral side of the abdomen, chest, buttock, inside of the upper thigh, forearm, the zygomatic bone, the ear lobe, cheek, or the forehead in neonates and small pediatric patients [9]. In the beginning, we compared data obtained from sensors placed on the chest, forearm, earlobe, and forehead in spontaneously breathing adults. In the early stage of the study, we decided to use only a chest or forearm sensor (data are shown later).
Arterial blood samples are drawn with the patient being in a steady state [17]. The usual clinical practice for arterial BGA in fully conscious patients involves a single arterial puncture performed after a waiting period of 20–30 min [17, 18]. The procedure of arterial puncture may cause pain and hyperventilation, thereby altering subsequent arterial BGA data due to respiratory alkalosis [17]. In mechanically ventilated patients, the stability after a change in FIO2 is reached between 10 and 30 min depending on the physiological and pathophysiological conditions of the patient [19]. Therefore, in the present study, the arterial BGA data with one-time arterial puncture after a waiting (resting) period of 30 min in the supine position was defined as the gold standard blood gas data.
We evaluated the transcutaneous BGA data at 1-min intervals comparing the final goal of arterial BGA at 30 min. This novel approach will answer the following questions: “From which time point are the transcutaneous BGA data meaningful?” and “How accurately are the current transcutaneous BGA data predicting arterial BGA?” In addition, the results of the subgroup analyses which may help to understand transcutaneous BGA, are shown. Finally, we discuss the most important subgroup (i.e., severe hypercapnia with PaCO2 > 50 mmHg) and recommend a reasonable time-saving step for the accurate diagnosis of these patients.
Methods
Subjects and study procedures
The study was approved by the Ethics Committee of the International University of Health and Welfare (IUHW, approval number 13-B-109). All subjects provided written consent prior to participating in this study. All subjects were adults, aged ≥20 years. Both healthy volunteers and patients who visited the Department of Respiratory Medicine, IUHW Shioya Hospital were invited to participate in the study. Measurements were performed in the supine position at room temperature (24–25 °C). Transcutaneous BGA data from 1 to 30 min and arterial BGA data at 30 min were obtained, and compared through Bland–Altman analysis [20]. Monitoring of percutaneous oxygen saturation (SpO2) with a pulse oximeter (PULSOX-C; KONICA MINOLTA, Osaka, Japan) was performed to confirm that SpO2 data from each subject were constant during the study (from sensor fixation to arterial blood sampling).
Transcutaneous BGA
PtcO2 and PtcCO2 were measured with a transcutaneous gas monitoring system (TCM4 with tcSensor 84 for neonatal, pediatric and adult patients; Radiometer Medical AsP, Copenhagen, Denmark), using the principles of the Clark and Severinghaus electrodes [21]. Calibration was achieved within 5–6 min. Following membrane change, the calibration required approximately 10 min. The temperature of the skin probe was set at 44 °C, as previously recommended [3, 8, 9]. Measurements were performed in the supine position with the skin probe position on (i) the upper chest wall (left or right second intercostal space in the midclavicular line), (ii) the inside of the forearm (upper third of the inner surface of the left or the right forearm), (iii) the earlobe, or (iv) the forehead. The sensor location was randomized and the duration of measurements was ≥30 min. Prior to sensor fixation, the skin and electrode were thoroughly cleaned, and an adhesive ring with two drops of contact gel was applied, according to the instructions provided by the manufacturer. Chest hair was avoided, and depilation from the thoracic skin was not necessary. After sensor fixation, PtcO2 and PtcCO2 were recorded at 1-min intervals. Prior to sensor fixation, the sensor detected the atmospheric PO2 and PCO2. The electromechanical response of the TCM4 device, as shown by breathing on the sensor measuring atmospheric PO2 and PCO2, elicited a decrease in PO2 within 5 s and an increase in PCO2 within 15 s.
Arterial BGA
Arterial BGA was performed at 30 min after sensor fixation in the supine position. Femoral arterial blood (0.5–1.0 ml) was drawn with a 22-gauge needle attached to a heparinized syringe. Samples were immediately analyzed with a blood gas analyzer (Rapidlab 1265; Siemens Healthcare Diagnostics, Sudbury, United Kingdom).
Subgroup analysis
The effects of gender, age, PaCO2 level and PaO2 level on the agreement data were evaluated. The transcutaneous data obtained via the sensors on the chest or forearm were used. The subjects with a PaCO2 level within the normal range (35–45 mmHg) were compared with those having different levels of hypocapnia or hypercapnia [17]. The subjects with a PaO2 level with the normal range (80–100 mmHg) were compared with those having hypoxemia or hyperoxemia [17].
Data analysis
Data are expressed as means ± standard deviation (SD), unless otherwise indicated. Concordance of arterial (at 30 min) and transcutaneous (between 1 and 30 min) blood gas data were investigated by Bland–Altman analysis. Therefore, 30 Bland–Altman analyses were performed. Analysis of variance with Tukey’s correction or unpaired t-test (two-tailed) was used for the comparison at 30 min. The Excel Statistics software, 2010 version (Social Survey Research Information Co., Ltd., Tokyo, Japan) was used. P < 0.05 denoted a statistically significant difference. Data were accumulated from the usual clinical practice at IUHW Shioya Hospital. When the number of subjects using chest or forearm sensor was 163 (males: 107, females: 56), PtcCO2 at 30 min was markedly larger than PaCO2 at 30 min (P = 3.8 × 10− 42). In the subgroup analysis, the absolute values of PO2 bias were larger in males than in females with P = 0.050. We calculated the necessary sample size to evaluate this interesting effect of gender. The expected effect size was 4.0 mmHg (SD: 12.1 mmHg); therefore, the standardized effect size was 0.33 [22]. It was considered that approximately 100 samples per group were necessary for an 80% power to detect significance at the 10% level (two-sided) in a t-test. The number of subjects using a chest or forearm sensor increased to 272 (males: 168, females: 104). The P-value decreased to < 0.01 and the effect of gender was confirmed (data are shown later).
Results
The tolerance of local heating for electrode attachment was good. There were no signs of skin irritation or erythema at the end of the monitoring.
Study population
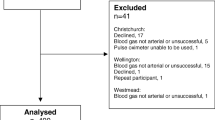
A total of 295 spontaneously breathing Asian adults (184 males, 111 females; mean age: 73.6 ± 14.5 years), comprising 10 healthy volunteers and 285 patients with various lung diseases, were enrolled from August 2015 to August 2019. The breakdown of lung diseases is shown in Supplementary Table S1 (Additional file 1). Forty-nine subjects received oxygen therapy. These subjects were studied while receiving supplemental O2. Initially, four sensor positions were randomly used. However, shortly after the study was initiated, the use of the forehead as a sensor location was discontinued because of prominently large biases (Fig. 1). The use of the earlobe as sensor location was also discontinued because of large biases (data shown later in this article). Age, gender, body mass index and diagnosed diseases were almost equally distributed among the four groups (one group per probe; Additional file 1, Supplementary Table S1). Monitored SpO2 was stable and constant (i.e., ≤ 2% change during the 30 min observation period in any subject).

Process of data collection via the chest or forearm sensors
Agreement at 30 min
The concordances between transcutaneous BGA and arterial BGA data at 30 min are shown in Fig. 2. Transcutaneous data obtained via the chest or forearm sensors were used (n = 272). The bias of PCO2 was 4.7 mmHg, with PtcCO2 being higher than PaCO2, and the 95% limits of agreement were ± 6.3 mmHg (Fig. 2a). The bias of PO2 was 12.2 mmHg, with PaO2 being higher than PtcO2, and the 95% limits of agreement were ± 23.1 mmHg (Fig. 2b).

Blood gas data at 30 min (transcutaneous data were obtained via the chest or forearm sensors, n = 272). a Concordance between PaCO2 and PtcCO2 data at 30 min. The bias of PCO2 was 4.7 mmHg, with PtcCO2 being higher than PaCO2 and 95% limits of agreement of ±6.3 mmHg. b Concordance between PaO2 and PtcO2 data at 30 min. The bias of PO2 was 12.2 mmHg, with PaO2 being higher than PtcO2 and 95% limits of agreement of ±23.1 mmHg
Time courses of agreement
The time courses of the two indices used in the Bland–Altman analysis (the bias and the 95% limits of agreement) are shown in Fig. 3. This was a series of 30 Bland–Altman analyses in which we compared 1–30 min transcutaneous data with min-30 arterial BGA data. Transcutaneous data obtained via the chest or forearm sensors were used (n = 272). The bias of PCO2 was 0.2 mmHg at 4 min (Fig. 3a), and the 95% limits of agreement (± 1.96SD) were ± 13.6 mmHg (Fig. 3b). This 1.96SD for PCO2 was initially reduced; however, it was similar to that obtained between 12 and 30 min (6.3–7.5 mmHg). At 8 min or later, the bias was 4.1–4.8 mmHg, with PtcCO2 being higher than PaCO2. In contrast, the absolute value of bias of PO2 was lowest (almost 0 mmHg) at 1–2 min (Fig. 3c), and the 1.96SD was reduced over time, with the closest agreement observed at 30 min (± 23.1 mmHg) (Fig. 3d).

Time courses of Bland-Altman analysis indices: the bias and 95% limits of agreement (transcutaneous data were obtained via the chest or forearm sensors, n = 272). Average data from 272 subjects are shown. a Bias and b 1.96SD on PCO2; c bias and d 1.96SD on PO2. The bias on PCO2 was 0.2 mmHg at 4 min (a), and subsequently increased to a plateau of 4.1–4.8 mmHg, which was almost stable between 8 and 30 min. 1.96SD on PCO2 declined over time, with the minimum (6.3 mmHg) observed at 30 min; however, it remained almost constant (6.3–7.5 mmHg) between 12 and 30 min, (b). The bias on PO2 initially decreased, passed the nadir at 5–6 min, and plateaued between 16 and 30 min (c). 1.96SD on PO2 decreased over time, with the minimum (23.1 mmHg) observed at 30 min (d)
Differences in agreement among four sensor locations
The time courses of the agreement data were compared among the four sensor locations (Additional file 2, Supplementary Fig. S1). At 30 min, the absolute values of bias obtained via the forearm and chest sensors were equivalent, and significantly lower than those obtained via the earlobe or forehead sensors for both PCO2 and PO2 (Fig. 4). At 30 min, the absolute values of PO2 bias obtained via the earlobe sensor were significantly lower than those obtained via the forehead sensor. There was no significant difference in arterial BGA data or pulse oximeter data among the four different sensor location groups (Additional file 1, Supplementary Table S2). On the other hand, PtcO2 data obtained via the earlobe or forehead sensor at 30 min were significantly different from those obtained via the forearm or chest sensor at 30 min.

Comparison of bias at 30 min among four sensor locations. The absolute values of bias obtained via forearm (n = 143) and chest (n = 129) sensors were equivalent, and were significantly lower than those obtained via the earlobe (n = 17) or forehead (n = 6) sensors for both PCO2 and PO2. The absolute values of PO2 bias obtained via the earlobe sensor were significantly lower than those obtained via the forehead. ANOVA with Tukey’s pot-hoc test, *: P < 0.05, **: P < 0.01, Bars: SEM
Subgroup analyses
Effects of gender and age
The effects of gender on the time courses were examined: male (n = 168), female (n = 104, Additional file 2, Supplementary Fig. S2). At 30 min, the absolute values of PO2 bias in males were significantly larger than those recorded in females (P < 0.01; Fig. 5a). The effects of age on the time courses were examined in the following four groups: 20–39 years (n = 11), 40–59 years (n = 12), 60–79 years (n = 138), and ≥ 80 years (n = 111) (Additional file 2, Supplementary Fig. S3). At 30 min, the PCO2 biases in young adults (20–39 years old) were significantly lower than those observed in the 40–59 year-old group and ≥ 80 year-old group (both P < 0.05; Fig. 5b).

Subgroup analyses on gender and age at 30 min. Transcutaneous data obtained via the chest or forearm sensors were used (n = 272). Bars: SEM, *: P < 0.05, **: P < 0.01. a Comparison of biases between males (n = 168) and females (n = 104). Gender had no significant effects on PCO2 bias. However, the absolute values of male PO2 bias observed were significantly larger than those of female PO2 bias (Unpaired t-test). b Comparison of biases among 4 age groups: 20–39 years (n = 11), 40–59 years (n = 12), 60–79 years (n = 138), and ≥ 80 years (n = 111). PCO2 biases in young adults (20–39 years) were significantly lower than in the 2 groups of 40–59 years and ≥ 80 years. However, there were no significant differences in PO2 bias among the four groups (ANOVA with Tukey’s pot-hoc test)
Effects of PaCO2 and PaO2 levels
The effects of hypocapnia on the time courses were examined in the following two levels of PaCO2: PaCO2 < 31 mmHg group (severe hypocapnia, n = 7) and 31 ≤ PaCO2 < 35 mmHg group (mild hypocapnia, n = 24; Additional file 2, Supplementary Fig. S4). At 30 min, the absolute values of bias in the severe hypocapnia group were higher than those noted in the normal PaCO2 group (n = 202) for both PCO2 (P < 0.01) and PO2 (P < 0.05; Fig. 6a). This effect of hypocapnia on the PCO2 bias was dependent on severity. The effects of hypercapnia on the time courses were examined in the following two levels of PaCO2: 45 < PaCO2 ≤ 50 mmHg group (mild hypercapnia, n = 26) and > 50 mmHg group (severe hypercapnia, n = 13; Additional file 2, Supplementary Fig. S5). At 30 min, the PCO2 bias in the mild hypercapnia group was significantly lower than that observed in the normal PaCO2 group (P < 0.01; Fig. 6b). The effects of the PaO2 level on the time courses were similarly examined (Additional file 2, Supplementary Fig. S6). At 30 min, the absolute values of bias in the hypoxemia group (n = 158) were lower than those measured in the normal PaO2 group (n = 102) for both PCO2 (P < 0.05) and PO2 (P < 0.01; Fig. 6c). At 30 min, the absolute values of PO2 bias in the hyperoxemia group (n = 12) were larger than those recorded in the normal PaO2 group (P < 0.05; Fig. 6c).

Subgroup analyses on PaCO2 level and PaO2 level at 30 min. Transcutaneous data obtained via the chest or forearm sensors were used (n = 272). Bars: SEM, *: P < 0.05, **: P < 0.01, ANOVA with Tukey’s pot-hoc test. a Comparison of biases among severe hypocapnia (PaCO2 < 31 mmHg, n = 7), mild hypocapnia (31 mmHg ≤ PaCO2 < 35 mmHg, n = 24), and normal range (35 mmHg ≤ PaCO2 ≤ 45 mmHg, n = 202). The absolute values of bias observed in the severe hypocapnia group were significantly larger than those observed in the normal range group for both PCO2 and PO2. This effect of hypocapnia seemed to be intensity-dependent. b Comparison of biases among normal range (35 mmHg ≤ PaCO2 ≤ 45 mmHg, n = 202), mild hypercapnia (45 mmHg < PaCO2 ≤ 50 mmHg, n = 26), and severe hypercapnia (50 mmHg < PaCO2, n = 13). PCO2 biases in mild hypercapnia were significantly smaller than in normal range group. c Comparison of biases among hypoxemia (PaO2 < 80 mmHg, n = 158), normal range (80 mmHg ≤ PaO2 ≤ 100 mmHg, n = 102), and hyperoxemia (100 mmHg < PaO2, n = 12). The absolute values of bias observed in the hypoxemia group were significantly smaller than those observed in the normal range group for both PCO2 and PO2. The absolute values of PO2 bias observed in the hyperoxemia group were significantly larger than those observed in the normal range group. These effects on PO2 biases seemed to be PaO2 level-dependent
Precise observation of subjects with hypercapnia PaCO2 > 50 mmHg
Data and profiles of subjects with hypercapnia (PaCO2 > 50 mmHg, n = 13) are shown in Table 1. Most of these subjects (85%) were receiving O2 therapy. At 4 min, PtcCO2 ≥ 50 mmHg was observed in 69% of these subjects. This ratio increased over time; at 12 min, all these subjects showed PtcCO2 ≥ 50 mmHg. At 13 min, all these subjects showed PtcCO2 ≥ 51 mmHg. Subjects with severe hypercapnia appeared to have more diseases (e.g., circulatory failure) than those with mild hypercapnia.
Discussion
By comparing the agreement between minutely obtained transcutaneous BGA data and the final answer data of arterial BGA at 30 min, we obtained the following findings. Firstly, the sensors placed on the chest and forearm are equally preferred. Secondly, the method to predict PaCO2 at 30 min is to initially measure PtcCO2 at 4 min without bias, and observe PtcCO2 at 8 min or later considering a bias of 4–5 mmHg. Thirdly, although PtcCO2 is useful, it cannot completely replace the actual levels of PaCO2 due to occasional large PCO2 bias. Fourthly, the subgroup analyses showed that gender, younger age, PaCO2 levels, and PaO2 levels affected PO2 and/or PCO2 biases. Fifthly, a reasonable step to reach accurate diagnosis of PaCO2 > 50 mmHg using transcutaneous BGA data was recommended. Finally, we showed that the prediction of PaO2 by PtcO2 was unrealistic in Asian adults.
Previously, it was reported that the 1.96SD between venous PCO2 and PaCO2 was 15.0 mmHg [23]. Venous PCO2 is occasionally used as a surrogate with a bias of 5 mmHg. Our approach enabled to answer the question of “From which time point are the PtcCO2 data meaningful?” The answer is “From 4 min.”, because the limits of agreement between PaCO2 and PtcCO2 at 4 min or later were ± 13.6 mmHg or narrower. Of note, they were narrower than the limit of agreement (± 15.0 mmHg) between PaCO2 and venous PCO2. By waiting longer, we can obtain more accurate PtcCO2 data for the estimation of PaCO2. Several studies have indicated that PtcCO2 is more accurate than end-tidal PCO2 as a surrogate measure of PaCO2 [24,25,26,27,28]. While 1.96SD data between end-tidal PCO2 and PaCO2 ranged from 6.9 to 14.4 mmHg, 1.96SD data between PtcCO2 and PaCO2 ranged from 4.6 to 10.4 mmHg. The PtcCO2 data at 12–13 min or later were within the acceptable clinical range of agreement for PtcCO2 (± 7.5 mmHg) recommended in the guideline of the American Association for Respiratory Care [9].
As a whole, the prediction of PaCO2 is possible. It involves initial measurement of PtcCO2 at 4 min without bias, and observation of PtcCO2 at 8 min or later considering a bias of 4–5 mmHg. In a steady state, PtcCO2 is higher than PaCO2 because the former is an epidermal parameter which does not exclusively reflect arterial blood, and CO2 is produced by living epidermal cells [7, 29, 30].
The 1.96SD between PtcO2 and PaO2 displayed a continual decline without an obvious plateau at 30 min. Even the minimal limit of agreement of ±24.0 mmHg at 30 min is not negligible in clinical practice. Therefore, PtcO2 is not an appropriate substitute for PaO2. Kesten et al. reported that the 90% response speed of PtcCO2 in this system was approximately three times faster than that of PtcO2 [14]. The Krogh’s constants of diffusion for O2 and CO2 in water and aqueous tissues may be important to understand the difference between these gases [15]. In water and aqueous tissues, the Krogh’s constant of diffusion for CO2 has been reported to be 20–25 times higher than that for O2.
A change in the baseline level with time is termed “drift” [31]. The calibration was performed prior to measuring each subject according to the protocol provided by the manufacturer. The duration of the measurement was only 30–40 min per subject; therefore, the “drift” effect was considered negligible.
A few previous studies have investigated the relationship between PtcCO2 and PaCO2 over time [11,12,13]. Fuke et al. compared PaCO2 via an arterial catheter and PtcCO2 over time (n = 6), yielding evaluations of individual agreements [11]. Excellent agreement over time was shown in three subjects. Both Cuvelier et al. [12] and Storre et al. [13] compared PaCO2 via an arterial catheter and PtcCO2 over time (n = 12 and n = 10, respectively), demonstrating parallel changes without any description of concordance over time. The present noninvasive study without arterial catheterization is in line with the actual clinical practice for spontaneously breathing patients, and provides data from a larger sample of subjects compared with previous studies [11,12,13]. The subgroup analyses revealed that gender and younger age affected the biases. Further investigation is necessary to confirm this observation. The absolute values of biases (for both PCO2 and PO2) were larger in the PaCO2 < 31 mmHg group than in the normal group. Arterial vasoconstriction by hyperventilation may be involved in this phenomenon [23]. If PaCO2 is low, the PCO2 bias may increase and underestimation of hyperventilation might occur. However, Bendjelid et al. reported that the PaCO2 level did not affect the PCO2 bias (n = 55, Caucasians 85%) [32]. The absolute values of biases (for both PCO2 and PO2) were smaller in the hypoxemia group than in the normal group. Hypoxic vasodilation may be involved in this phenomenon [33].
Another limitation of the study is that arterial BGA was performed only at 30 min. However, it is worth performing Bland–Altman analysis for the comparison of the single time point arterial BGA data with the minutely obtained transcutaneous data. All gas data were collected during a short period (30–40 min) in the steady state, which was validated by observations that SpO2 data were almost constant in each subject from the sensor fixation to the arterial blood sampling procedure. The effect of changing body position (e.g., from sitting to supine position) on PaCO2 has been reported to be smaller than that exerted on PaO2 [34, 35]. Bland and Altman compared data from two different peak flow meters which cannot be performed simultaneously [20].
Correct diagnosis of severe hypercapnia with PaCO2 > 50 mmHg is important to avoid CO2 narcosis. This technology of TCM4 with a Severinghaus electrode is useful in identifying subjects with PaCO2 > 50 mmHg. By performing arterial BGA after detecting PtcCO2 ≥ 50 mmHg during an observation for 12 min, PaCO2 > 50 mmHg can be accurately measured (without exceptions at least in our 13 subjects). We recommend this reasonable step for the efficient use of PtcCO2 data.
Conclusions
We compared the agreement between minutely obtained transcutaneous BGA data and the final answer data of arterial BGA at 30 min. The use of sensors on the chest and forearm is equally recommended. Although PtcCO2 is useful and can be used as a screening tool for severe hypercapnia, it cannot completely replace PaCO2. On the other hand, the prediction of PaO2 by PtcO2 was unrealistic in Asian adults. Consideration of gender, age, PaCO2 levels, and PaO2 levels may assist in improving the accuracy of estimation. Further investigations are needed to clarify the mechanisms of these factors that influence the biases. This approach may be of potential use to better understand transcutaneous BGA.
Availability of data and materials
The datasets used in this study are available from the corresponding author upon reasonable request.
Abbreviations
- AARC:
-
American Association for Respiratory Care
- ACO:
-
Asthma-chronic obstructive pulmonary disease overlap
- ANOVA:
-
Analysis of variance
- BGA:
-
Blood gas analysis
- COPD:
-
Chronic obstructive pulmonary disease
- IUHW:
-
International University of Health and Welfare
- PtcCO2 :
-
Transcutaneous PCO2
- PtcO2 :
-
Transcutaneous PO2
- SD:
-
Standard deviation
- SpO2 :
-
Percutaneous oxygen saturation
References
Huch R, Huch A, Albani M, Gabriel M, Schulte FJ, Wolf H, et al. Transcutaneous PO2 monitoring in routine management of infants and children with cardiorespiratory problems. Pediatrics. 1976;57(5):681–90.
Huch A, Seiler D, Meinzer K, Huch R, Galster H, Lübbers DW. Transcutaneous PCO2 measurement with a miniaturised electrode. Lancet. 1977;1(8019):982–3.
Lucey JF. Clinical uses of transcutaneous oxygen monitoring. Adv Pediatr. 1981;28:27–56.
Wimberley PD, Pedersen KG, Thode J, Fogh-Andersen N, Sørensen AM, Siggaard-Andersen O. Transcutaneous and capillary pCO2 and pO2 measurements in healthy adults. Clin Chem. 1983;29(8):1471–3.
Rüdiger M, Töpfer K, Hammer H, Schmalisch G, Wauer RR. A survey of transcutaneous blood gas monitoring among European neonatal intensive care units. BMC Pediatr. 2005;5:30.
Delerme S, Montout V, Goulet H, Arhan A, Le Saché F, Devilliers C, et al. Concordance between transcutaneous and arterial measurements of carbon dioxide in an ED. Am J Emerg Med. 2012;30(9):1872–6.
Stieglitz S, Matthes S, Priegnitz C, Hagmeyer L, Randerath W. Comparison of transcutaneous and capillary measurement of PCO2 in hypercapnic subjects. Respir Care. 2016;61(1):98–105.
Nishiyama T, Nakamura S, Yamashita K. Effects of the electrode temperature of a new monitor, TCM4, on the measurement of transcutaneous oxygen and carbon dioxide tension. J Anesth. 2006;20(4):331–4.
Restrepo RD, Hirst KR, Wittnebel L, Wettstein R. AARC clinical practice guideline: transcutaneous monitoring of carbon dioxide and oxygen: 2012. Respir Care. 2012;57(11):1955–62.
Ruangsetakit C, Chinsakchai K, Mahawongkajit P, Wongwanit C, Mutirangura P. Transcutaneous oxygen tension: a useful predictor of ulcer healing in critical limb ischaemia. J Wound Care. 2010;19(5):202–6.
Fuke S, Miyamoto K, Ohira H, Ohira M, Odajima N, Nishimura M. Evaluation of transcutaneous CO2 responses following acute changes in PaCO2 in healthy subjects. Respirology. 2009;14(3):436–42.
Cuvelier A, Grigoriu B, Morano LC, Muir JF. Limitation of transcutaneous carbon dioxide measurements for assessing long-term mechanical ventilation. Chest. 2005;127(5):1744–8.
Storre JH, Steurer B, Kabitz HJ, Dreher M, Windisch W. Transcutaneous PCO2 monitoring during initiation of noninvasive ventilation. Chest. 2007;132(6):1810–6.
Kesten S, Chapman KR, Rebuck AS. Response characteristics of a dual transcutaneous oxygen/carbon dioxide monitoring system. Chest. 1991;99(5):1211–5.
Dejours P. Oxygen and carbon dioxide exchanges by diffusion. In: Principles of comparative respiratory physiology. 2nd ed. Amsterdam: Elsevier/North-Holland Biomedical Press; 1981. p. 63–74.
Nishiyama T, Nakamura S, Yamashita K. Comparison of the transcutaneous oxygen and carbon dioxide tension in different electrode locations during general anaesthesia. Eur J Anaesthesiol. 2006;23(12):1049–54.
Malley WJ. Arterial blood gases. In: Clinical blood gases: Assessment and Intervention. 2nd ed. St. Louis: Elsevier Saunders; 2005. p. 3–34.
American Association for Respiratory Care. AARC clinical practice guideline. Sampling for arterial blood gas analysis. Respir Care. 1992;37(8):913–7.
Sasse SA, Jaffe MB, Chen PA, Voelker KG, Mahutte CK. Arterial oxygenation time after an FIO2 increase in mechanically ventilated patients. Am J Respir Crit Care Med. 1995;152(1):148–52.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307–10.
Malley WJ. Blood gas electrodes and quality assurance. In: Clinical blood gases: Assessment and Intervention. 2nd ed. St. Louis: Elsevier Saunders; 2005. p. 82–113.
Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB. Designing clinical research. 4th ed. Philadelphia: Lippincott Williams & Wilkins, a Wolters Kluwer business; 2013.
Umeda A, Kawasaki K, Abe T, Watanabe M, Ishizaka A, Okada Y. Hyperventilation and finger exercise increase venous-arterial PCO2 and pH differences. Am J Emerg Med. 2008;26(9):975–80.
Aliwalas LL, Noble L, Nesbitt K, Fallah S, Shah V, Shah PS. Agreement of carbon dioxide levels measured by arterial, transcutaneous and end tidal methods in preterm infants < or = 28 weeks gestation. J Perinatol. 2005;25(1):26–9.
Tobias JD, Meyer DJ. Noninvasive monitoring of carbon dioxide during respiratory failure in toddlers and infants: end-tidal versus transcutaneous carbon dioxide. Anesth Analg. 1997;85(1):55–8.
Oshibuchi M, Cho S, Hara T, Tomiyasu S, Makita T, Sumikawa K. A comparative evaluation of transcutaneous and end-tidal measurements of CO2 in thoracic anesthesia. Anesth Analg. 2003;97(3):776–9.
Tingay DG, Stewart MJ, Morley CJ. Monitoring of end tidal carbon dioxide and transcutaneous carbon dioxide during neonatal transport. Arch Dis Child Fetal Neonatal Ed. 2005;90(6):F523–6.
Hirabayashi M, Fujiwara C, Ohtani N, Kagawa S, Kamide M. Transcutaneous PCO2 monitors are more accurate than end-tidal PCO2 monitors. J Anesth. 2009;23(2):198–202.
Severinghaus JW, Bradley AF, Stafford MJ. Transcutaneous PCO2 electrode design with internal silver heat path. Birth Defects Orig Artic Ser. 1979;15(4):265–70.
Severinghaus JW, Stafford M, Thunstrom AM. Estimation of skin metabolism and blood flow with tcPO2 and tcPO2 electrodes by cuff occlusion of the circulation. Acta Anaesthesiol Scand Suppl. 1978;68:9–15.
Malley WJ. Noninvasive blood gas monitoring. In: Clinical blood gases: Assessment and Intervention. 2nd ed. St. Louis: Elsevier Saunders; 2005. p. 387–418.
Bendjelid K, Schütz N, Stotz M, Gerard I, Suter PM, Romand JA. Transcutaneous PCO2 monitoring in critically ill adults: clinical evaluation of a new sensor. Crit Care Med. 2005;33(10):2203–6.
Kulandavelu S, Balkan W, Hare JM. Regulation of oxygen delivery to the body via hypoxic vasodilation. Proc Natl Acad Sci U S A. 2015;112(20):6254–5.
Sandoval J, Alvarado P, Martínez-Guerra ML, Gómez A, Palomar A, Meza S, et al. Effect of body position changes on pulmonary gas exchange in Eisenmenger's syndrome. Am J Respir Crit Care Med. 1999;159(4 Pt 1):1070–3.
Hardie JA, Mørkve O, Ellingsen I. Effect of body position on arterial oxygen tension in the elderly. Respiration. 2002;69(2):123–8.
Acknowledgements
We thank all the participants of this study. We especially thank Ms. Rena Ishizaki for assisting with the data reduction work.
Funding
This work was partly supported by IUHW Shioya Hospital.
Author information
Authors and Affiliations
Contributions
AU: conceived the idea, involved in patient management, data collection and statistical analysis, drafted and revised the manuscript for intellectual content. MI: involved in patient management and data collection, revised the manuscript for intellectual content. MT: involved in data collection, revised the manuscript. TY, TW, YI, TM and SK revised the manuscript for intellectual content. YO: involved in statistical analysis, revised the manuscript for intellectual content. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The project was approved by the Ethics Committee of the International University of Health and Welfare (IUHW, approval number 13-B-109). All subjects provided written consent before participating in this study.
Consent for publication
Not applicable.
Competing interests
The authors have no potential conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
AU presented part of the data at the 56th annual meeting of Japanese Respiratory Society (Apr 8, 2016. Kyoto), and at the 114th annual meeting of Japanese Society of Internal Medicine (Apr 15, 2017. Tokyo).
Supplementary information
Additional file 1: Supplementary Table S1.
Comparison of subjects among the four groups of different sensor locations. Supplementary Table S2. Comparison of blood gas data among the four groups of different sensor locations.
Additional file 2: Supplementary Fig. S1.
Comparison of the time course data among the four locations of sensors. Average data are shown. Blue line: forearm (n = 143), red line: chest (n = 129), green line: earlobe (n = 17), and purple line: forehead (n = 6). Trajectories of (a) bias and (b) 1.96SD on PCO2. Trajectories of (c) bias and (d) 1.96SD on PO2. (a): Compared with the forearm or chest sensors, the earlobe or forehead sensors yielded larger bias for PCO2 at 4 min or later. (b): 1.96SD on PCO2 was similar among the four locations. (c): The forearm and chest sensors showed almost the same time course of bias for PO2. The earlobe sensor yielded larger absolute values of bias, whereas the forehead sensor yielded much larger absolute values of bias. (d): 1.96SD of the forehead sensor was larger than that of the forearm or chest sensors. Supplementary Fig. S2. Comparison of the time course data (males vs. females, n = 272). Transcutaneous data obtained via the chest or forearm sensors were used. Average data are shown. Blue line: males (n = 168), red line: females (n = 104). Trajectories of (a) bias and (b) 1.96SD on PCO2. Trajectories of (c) bias and (d) 1.96SD on PO2. PCO2 bias was similar between the two groups (a). The 1.96SD of females on PCO2 was slightly lower than male (b). The absolute values of female PO2 bias was lower than that of males (c). 1.96SD on PO2 was not affected by gender (d). Supplementary Fig. S3. Comparison of the time course data (among four age groups, n = 272). Transcutaneous data obtained via the chest or forearm sensors were used. Average data are shown. Blue line: 20–39 years (n = 11), red line: 40–59 years (n = 12), green line: 60–79 years (n = 138), purple line: ≥ 80 (n = 111). Trajectories of (a) bias and (b) 1.96SD on PCO2. Trajectories of (c) bias and (d) 1.96SD on PO2. Crossing the 0 line at approximately 5 min (later than in the other three groups), PCO2 biases in young adults (20–39 years) was slightly lower than those of the other three groups (a). The 1.96SD of young adults (20–39 years) on PCO2 was slightly higher than that of the other three groups at 21 min or later (b). The absolute values of PO2 bias in 40–59 years group seemed a little larger than those of the other three groups at 13 min or later. (c). The 1.96SD of young adults (20–39 years) on PO2 was slightly higher than that of the other three groups at 11 min or later (d). Supplementary Fig. S4. Comparison of the time course data to evaluate effects of hypocapnia. Transcutaneous data obtained via the chest or forearm sensors were used. Average data are shown. Blue line: severe hypocapnia (PaCO2 < 31 mmHg, n = 7), red line: mild hypocapnia (31 mmHg ≤ PaCO2 < 35 mmHg, n = 24), green line: normal range (35 mmHg ≤ PaCO2 ≤ 45 mmHg, n = 202). Trajectories of (a) bias and (b) 1.96SD on PCO2. Trajectories of (c) bias and (d) 1.96SD on PO2. Crossing the 0 line at 2–3 min (earlier than in the other two groups), PCO2 biases in severe hypocapnia group was larger than those of the other two groups (a). This effect of hypocapnia seemed to be severity-dependent at 9 min or later. The 1.96SD of severe hypocapnia group was higher than that of the other two groups (b, d). The absolute values of PO2 bias in severe hypocapnia group were larger than those of the other two groups at 6 min or later. (c). Supplementary Fig. S5. Comparison of the time course data to evaluate effects of hypercapnia. Transcutaneous data obtained via the chest or forearm sensors were used. Average data are shown. Blue line: normal range (35 mmHg ≤ PaCO2 ≤ 45 mmHg, n = 202), red line: mild hypercapnia (45 mmHg < PaCO2 ≤ 50 mmHg, n = 26), green line: severe hypercapnia (50 mmHg < PaCO2, n = 13). Trajectories of (a) bias and (b) 1.96SD on PCO2. Trajectories of (c) bias and (d) 1.96SD on PO2. Crossing the 0 line at about 6 min (later than normal range group), PCO2 biases in mild hypocapnia group were smaller than those of normal range group (a). This delay of crossing the 0 line seemed to be severity-dependent. The 1.96SD of severe hypercapnia group on PCO2 was higher than that of the other two groups (b). The absolute values of PO2 bias in mild hypercapnia group were smaller than those of normal range group at 2 min or later (c). 1.96SD on PO2 seemed to be about the same among the three groups (d). Supplementary Fig. S6. Comparison of the time course data to evaluate effects of PaO2 levels. Transcutaneous data obtained via the chest or forearm sensors were used. Average data are shown. Blue line: hypoxemia (PaO2 < 80 mmHg, n = 158), red line: normal range (80 mmHg ≤ PaO2 ≤ 100 mmHg, n = 102), green line: hyperoxemia (100 mmHg < PaO2, n = 12). Trajectories of (a) bias and (b) 1.96SD on PCO2. Trajectories of (c) bias and (d) 1.96SD on PO2. PCO2 biases in hypoxemia group were smaller than those of the other two groups (a). The 1.96SD on PCO2 seemed to be about the same among the three groups (b). The absolute values of PO2 bias in hypoxemia group were smaller than those of normal range group (c). The absolute values of PO2 bias in hyperoxemia group were larger than those of normal range group (c). The 1.96SD of hyperoxemia group on PO2 was higher than that of the other two groups (d).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Umeda, A., Ishizaka, M., Tasaki, M. et al. Evaluation of time courses of agreement between minutely obtained transcutaneous blood gas data and the gold standard arterial data from spontaneously breathing Asian adults, and various subgroup analyses. BMC Pulm Med 20, 151 (2020). https://doi.org/10.1186/s12890-020-01184-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-020-01184-w