
Abstract
Background
Flight attendants face various risk factors in their working environments, particularly occupational exposure to cosmic radiation. This study aimed to assess cancer risk among air transportation industry workers, including flight attendants, in Korea by constructing a cohort using national health registry-based data and analyzing cancer incidence risk.
Methods
We used the Korea National Health Insurance Service database from 2002 to 2021 to construct a cohort of 37,011 workers in the air transportation industry. Cancer incidence was defined using the tenth version of the International Classification of Diseases. We calculated the age- and sex-specific standardized incidence ratios (SIRs) and 95% confidence intervals (CIs) by applying the cancer incidence rate of the general population between 2002 and 2019.
Results
Approximately 5% of the cohort developed cancer. Overall, the cancer incidence in the cohort was similar to or lower than that of the general population, with the SIRs for all cancers being lower. However, significantly higher SIRs were observed for nasopharyngeal cancer (SIR, 3.21; 95% CI, 1.71–5.48) and non-Hodgkin lymphoma (SIR, 1.57; 95% CI, 1.02–2.32) in male workers and breast and genital cancer (SIR, 1.51; 95% CI, 1.34–1.70) and thyroid cancer (SIR, 1.25; 95% CI, 1.05–1.47) in female workers.
Conclusions
The lower overall cancer incidence among air transportation industry workers observed in this study could indicate the “healthy worker effect”; however, the incidences of certain cancers were higher than those in the general population. Given that these workers are exposed to multiple occupational and lifestyle-related risk factors, including cosmic radiation, further studies are necessary to determine radiation-induced cancer risk while considering potential confounding factors.
Similar content being viewed by others

Background
Flight attendants encounter various physical, biological, chemical, and psychosocial stressors while performing their in-flight duties. Among these, cosmic radiation is regarded as an important physical factor. Cosmic radiation is a natural form of ionizing radiation from outer space and includes particles released from the sun during solar flares [1]. It is characterized by an increasing dose rate variation with rising flight altitude, expanding latitude (both pole and equator), and decreasing solar activity [2]. Flight attendants experience prolonged exposure to cosmic radiation during their careers while performing their professional tasks at high altitudes [3]. Acknowledging these occupational characteristics, the International Commission on Radiological Protection recommends that cosmic radiation exposure during flights be defined as occupational exposure [4].
Besides cosmic radiation, various other factors also contribute to increased work fatigue among flight attendants. Increased night shift work and prolonged working hours driven by the increasing demand for aviation are significant and prevalent organizational risk factors that contribute to this problem [5]. Other contributing factors include variation in atmospheric pressure and humidity with altitude, ergonomic constraints, and noise and pressure variations in the aircraft cabin. Additionally, workers are exposed to air quality issues due to the presence of cleaning chemicals and abnormal concentrations of gases such as ozone and carbon dioxide [6, 7]. The presence of a large number of passengers also increases the risk of exposure to infectious diseases [8].
Studies investigating the health effects of flight attendants have primarily been conducted in Northern Europe and the United States [9,10,11,12]. The most extensive investigation was a mortality study involving 93,771 flight attendants from nine European countries and the United States. This study revealed that the overall cancer mortality rate among male pilots and both male and female cabin crew members tended to be lower than that in the general population. However, the individual sites of cancer outcomes revealed significant increases in mortality rates for melanoma, other skin cancers, and non-Hodgkin lymphoma (NHL) among male workers compared with the general population [13]. Moreover, previous studies have indicated that female flight attendants exhibit a higher incidence of breast cancer than the general population [14,15,16], and another study has also suggested a potential association with the cumulative cosmic radiation dose [17].
However, the epidemiological findings of these studies, including on possible associations with cosmic radiation exposure, have been inconclusive [18,19,20]. This study aimed to assess cancer incidence among workers in the air transportation industry in Korea, including flight attendants, and compare it with that in the general population.
Materials and methods
Databases
We used the Korea National Health Insurance Service (K-NHIS) database, which is based on the insurance data of 97% of the Korean population [21]. The K-NHIS, a nonprofit organization, manages subscriber information and insurance premium collection and offers various health databases accessible through the National Health Insurance Sharing Service (NHISS) to support healthcare research. Among the database options provided by the NHISS, a customized database (DB) covering 2002–2021 allows researchers to tailor data according to the study population and design. Additionally, the sample cohort DB for calculating the general population incidence encompasses information derived from a 2% sample of the total national health insurance beneficiaries, comprising 1,000,000 individuals from 2002 to 2019. It consists of a stratified sample based on variables such as sex, age, subscriber classification, insurance premium, and regions, representing the entire Korean population [22]. Consequently, we used the DB to define the study population, focusing on workers in the air transportation industry, and the sample cohort DB to calculate the cancer incidence rate in the general population. The databases were organized into detailed subcategories, including the qualification table (QT), payment specification (20T), and diagnosis statements based on the International Classification of Diseases, 10th version (ICD-10) (40T). Each data table is identified by the letters QT, 20T, and 40T, using a specific number-table delimiter, where “T” signifies “Table.” The QT contains demographic characteristics such as sex, birth year, death date, subscriber classification, and socioeconomic variables such as income rank derived from insurance premiums. Moreover, the 20T and 40T tables provide details on treatment dates, medical care institutions, and diagnostic information for all treatments received during hospital visits, covering the principal and additional diagnoses.
Study population
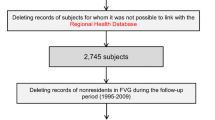
The cohort comprises workers employed in the air transportation industry at least once between 2002 and 2021. This group is defined as eligible employee subscribers identified using the QT with workplace industry codes related to the air transportation industry. After applying these two criteria, 37,687 workers were identified as the study population. After excluding those diagnosed with cancer before commencing employment (n = 676), the final cohort comprised of 37,011 workers. Subsequently, those who entered the industry after 2019, a period for which information on the sample cohort DB is not available, were excluded (n = 2,906), resulting in a pool of 34,105 workers for the analysis of the standardized incidence ratio (SIR) between 2002 and 2019 (Fig. 1)

Flowchart of selection of study population
Follow-up on cancer incidence
Cancer incidence was determined using disease information from the 40T in the K-NHIS and categorized into 61 cancer types according to the Cancer Incidence in Five Continents criteria of the International Agency for Research on Cancer (IARC), based on ICD-10 codes. The date of cancer incidence was defined as the earliest date of treatment for the corresponding cancer type, with priority given to the diagnosis of the first cancer in cases of multiple cancers. The follow-up period was set from 2002 to 2019, aligned with the termination of the sample cohort DB used to calculate the incidence rate in the general population. Hence, cohort entry was set as the later date of January 1, 2002, or January 1 of the year of first employment. The exit of the cohort was set to the date of cancer diagnosis, the date of death, or December 31, 2019, whichever occurred earlier.
Statistical analyses
We compared cancer incidence between air transportation workers and the general population by calculating age- (5-year interval) and sex-specific SIRs and 95% confidence intervals (CIs). The cancer incidence rate in the general population was obtained from the sample cohort DB in the K-NHIS from 2002 to 2019. SIRs were computed for all cancers and 61 cancer sites. However, owing to limitations in the sample cohort DB, which only provides the first digit of the ICD code for certain statutory infectious and sensitive diseases, the SIR was calculated by aggregating these diseases. For clarity, these categories have been labeled as “female breast and genital cancers” and “male genital cancers”. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Ethics approval
The data used in this study were anonymized prior to their release to the authors of the National Health Insurance Service. This study was approved by the Institutional Review Board (IRB) of the Korea Institute of Radiological and Medical Sciences (IRB file no. KIRAMS 2023-01-002).
Results
The demographic characteristics of air transportation industry workers between 2002 and 2021 are presented in Table 1.
A total of 37,011 workers were included in this study, including 23,400 (63.3%) male and 13,611 (36.7%) female. Most workers were born after 1980, and a significant portion commenced work after 2015, resulting in a short tenure, typically < 5 years. The mean age (± standard deviation) at the time of starting work from 2003 to 2021 was 32.6 ± 10.2 years, with female workers (28.0 ± 6.8 years) starting at a relatively younger age than male workers (35.6 ± 10.9 years).
Between 2002 and 2021, cancers were identified in 1,946 workers, accounting for approximately 5% of the total cohort (Table 2). There was no apparent difference in the incidence of cancer between the sexes (5.2% in male workers and 5.3% in female workers). The most prevalent cancers among male workers were prostate cancer (16.9%), followed by liver (13.4%) and lung (11.3%) cancers. Thyroid cancer was the most prevalent (24.3%) among female workers, followed by ovarian cancer (23.4%), and breast cancer (14.5%).
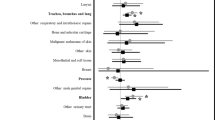
The SIR analysis involving 34,105 workers observed 292,945 person-years, with a mean of 8.6 years, and male workers (9.1 years) were observed for a longer period than female workers (7.7 years). The SIRs and 95% CIs for all cancers and 61 cancer sites calculated by applying the incidence rate of the general population between 2002 and 2019 are presented in Table 3.
When examining all cancers (C00–96), male workers exhibited an SIR of 0.90 (95% CI, 0.85–0.96), indicating a lower-than-expected incidence, whereas female workers demonstrated a high SIR of 1.20 (95% CI, 1.10–1.31).
In male workers, significantly higher incidence rates were noted for nasopharyngeal cancer (SIR, 3.21; 95% CI, 1.71–5.48) and NHL (SIR, 1.57; 95% CI, 1.02–2.32) compared to those in the general population. No significant differences were observed for male genital cancer, including prostate cancer, which was the most prevalent type. In female workers, we observed significantly higher incidence rates of breast and genital cancer (SIR, 1.51; 95% CI, 1.34–1.70) as well as thyroid cancer (SIR, 1.25; 95% CI, 1.05–1.47).
The SIR was calculated by categorizing the significantly observed cancer sites in the SIR results according to birth year, year of starting work, and working duration. However, no notable trends were identified based on the stratification factors (Table 4).
Discussion
In this study, we investigated the incidence of cancer in the air transportation industry by establishing a cohort using a health insurance database and comparing it with that in the general population. We observed that cancer developed in approximately 5% of workers from 2002 to 2021. Furthermore, our analysis revealed significantly lower incidence rates of all cancers combined, liver cancer, and lung cancer among male workers.
These findings align with those of previous studies on cancer incidence and mortality. In studies on Canadian pilots and UK flight crew members, the SIRs for all cancers combined and lung cancer were significantly lower compared to those in the general population, with the SIRs varying between 0.2 and 0.8 [23, 24]. Similarly, a study on air transportation industry workers in Korea showed a significantly low overall SIR for cancer (SIR = 0.57) [25]. These findings can be interpreted as indicative of a phenomenon often observed in occupational epidemiology, wherein the incidence or mortality of diseases decreases among workers due to the “healthy worker effect” [26]. In particular, flight attendants, whose primary duties include ensuring passenger safety during emergencies, prioritize both their physical and mental well-being more rigorously than many other professionals. Moreover, airlines deal with the challenging work environments inherent in the profession, such as altitude and air pressure variations and time-zone crossing, by implementing stringent physical examination standards for employees. Hence, the implementation of such management strategies may mitigate the underlying risk factors for cancer.
However, in contrast to this trend, significant increases in SIRs were observed for nasopharyngeal cancer and NHL in male workers. These findings are also consistent with those of previous epidemiological studies on flight attendants. In a study on participants from Nordic countries, including Finland, Iceland, Norway, and Sweden, the SIR for pharyngeal cancer among male cabin crew staff was significantly higher, at 3.12, than that in the general population [27]. For nasopharyngeal cancer, smoking and alcohol consumption are recognized as primary risk factors, underscoring their significant influence [28]. Similarly, the SIR for NHL among male U.S. air force aviator pilots and backseat aircrew was recently reported as 1.13 and was higher than the rate in the general population [29]; the study also reported a standardized mortality ratio (SMR) of 1.32. Although these findings were statistically significant, the study noted that the magnitudes of the SIR and SMR were considered ‘small’ from an epidemiological perspective, indicating that their impact may be limited. In another study, elevated SMRs for NHL were noted among male pilots and cabin crew, and the mortality rate among male cabin crew in a German study was up to four times higher than that among males in the general population [11, 13, 30, 31]. Both nasopharyngeal cancer and NHL are strongly associated with the human immunodeficiency virus (HIV), with HIV-infected patients being at higher risk, making it crucial to consider this factor as well [32, 33].
The elevated incidence of all cancers combined among female workers seems to be driven by the heightened SIR for breast and genital cancer and thyroid cancer, which constitute a significant proportion of all cases. These results are likely to be primarily attributable to a surveillance bias resulting from screening. A study investigating the association between thyroid cancer incidence and thyroid screening rates among radiation workers in Korea revealed a concurrent increase in the incidence ratio with the risk of screening. This finding offers robust epidemiological evidence that the increased rate of thyroid screening is associated with concerns about radiation exposure, consequently leading to an increase in the incidence rate [34]. In Korea’s national health checkup system, local subscribers and office workers among employee subscribers must undergo a health examination every 2 years, whereas non-office workers, including flight attendants, must undergo an annual examination. Furthermore, it is recommended that women aged ≥ 40 years should undergo screening for breast cancer and those aged > 20 years should undergo cervical cancer screening every 2 years as part of a national cancer screening project [35]. Additionally, non-office workers undergo annual employee health check-ups, making these screenings more accessible. Consequently, this screening cycle was anticipated to affect incidence. However, additional relevant interpretations for breast cancer are also available. Previous studies have reported an elevated risk of breast cancer among flight attendants [10, 14, 15, 27], and a pooled meta-analysis corroborated this increased risk [36]. As flight attendants frequently travel across multiple time zones, they are at a higher risk of circadian rhythm disruption. In 2007, the IARC monograph working group classified shift work involving circadian rhythm disruptions as a Group 2 A carcinogen, possibly carcinogenic to humans [37]. While the definitive association between night-shift work and breast cancer remains ambiguous, it is suggested that the reduction in melatonin secretion, a sleep hormone due to nocturnal work, may potentially facilitate the proliferation of breast cancer cells and lead to compromised immunity, as established in an existing study [38]. In a study investigating the association between breast cancer incidence and exposure to cosmic radiation among female flight attendants, a notable dose-response relationship was found in women with a high parity of three or more who might be exposed to a sleep-deficient environment at home, being more sensitive to the effects of circadian rhythm disruption [17].
This study is significant because it is one of the few studies exploring the health effects faced by flight attendants in regions beyond Nordic Europe and the United States, where previous research was predominantly concentrated. Furthermore, it is comprehensive because it utilizes an extensive database from K-NHIS, which encompasses more than 97% of Korea’s total population [39]. Using this large national database, a detailed analysis was performed on all 61 cancer types rather than focusing on a few selected cancers.
However, our study was constrained by limitations inherent to the data sources, as we obtained information on diseases from insurance data. Considering that the primary purpose of the data was insurance premium claims, their suitability for determining disease incidence may be suboptimal [40]. Nonetheless, a study that assessed the accuracy of ICD-10 codes in relevant Korean claims data reported that diagnostic accuracy was ensured solely by using ICD-10 codes [41, 42]. Furthermore, the counts of observed cases for certain rare cancers may require careful interpretation of the corresponding results.
Our study provides valuable findings for the limited literature on the health effects experienced by flight attendants. Studies on radiation workers sharing parallel characteristics of occupational radiation exposure have been consistently conducted, leading to a robust accumulation of epidemiological evidence. However, only a handful of these studies focused on flight attendants, particularly those assessing their exposure to cosmic radiation. Although we used job codes assigned based on the nature of the workplace, we faced the challenge of classifying flight attendants precisely; therefore, we conducted this study focusing on flight attendants to the greatest extent possible. In future studies, it will be crucial to define study populations more accurately and conduct high-quality analyses that consider individual radiation doses among flight attendants. Studies comparing incidences among workers having exposure to similar occupational and lifestyle-related factors will also be informative.
In Korea, with the revision of the legislation supporting the investigation of the health effects of flight attendants in 2023, we anticipate that the collection of dose registries will be facilitated. In addition to gathering the dose registry, we will be able to gather data on confounding factors, such as smoking, alcohol consumption, and shift work, which are key risk factors for cancer, by linking them to various Korean national health data sources. With access to these sources, we anticipate being able to perform a stronger assessment of health effects for flight attendants.
Conclusions
This study investigated the incidence of cancer in the air transportation industry by employing a cohort established from health insurance databases and comparing it with the general population. Our findings revealed a healthy worker effect in the overall cancer risk of the cohort; however, several types of cancer exhibited higher incidence rates. To better understand the association with cosmic radiation, further investigation through dose-response assessments using radiation doses among flight attendants is imperative. Moreover, given that flight attendants are exposed to multiple risk factors during their flights, it is necessary to determine radiation-induced cancer risk while considering potential confounders and their effect modifications.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- DB:
-
Database
- IARC:
-
International Agency for Research on Cancer
- K-NHIS:
-
Korea National Health Insurance Service
- NHL:
-
Non-Hodgkin lymphoma
- QT:
-
Quantification table
- SIR:
-
Standardized incidence ratio
- SMR:
-
Standardized mortality ratio
References
Aw JJ. Cosmic radiation and commercial air travel. J Travel Med. 2003;10:19–28.
Ahn H-B, Kwak J, Hwang J. Comparative analysis of cosmic radiation exposure dose due to the Russian detour route. J Astron Space Sci. 2023;40:59–66.
Toprani SM, Scheibler C, Mordukhovich I, McNeely E, Nagel ZD. Cosmic ionizing radiation: a DNA damaging agent that may underly excess cancer in flight crews. Int J Mol Sci. 2024;25:7670.
ICoR P. Recommendations of the international commission on radiological protection. Ann ICRP. 1990;21:1–201.
Marqueze EC, de Sá E, Benevides EA, Russo AC, Fürst MSG, Roscani RC, Guimarães PCV, et al. Organizational risk factors for aircrew health: a systematic review of observational studies. Int J Environ Res Public Health. 2023;20:3401.
Kim Y-H, Kim J-S, Song B-H. Fatigue analysis according to flight conditions of airline crew members. J Korean Soc Aviat Aeronaut. 2023;31:126–32.
Posch M, Schranz A, Lener M, Senn W, Äng BO, Burtscher M, et al. Prevalence and potential risk factors of flight-related neck, shoulder and low back pain among helicopter pilots and crewmembers: a questionnaire-based study. BMC Musculoskelet Disord. 2019;20:44.
Vata A, Miftode L, Obreja M, Miftode R, Vata LG. Infectious diseases and the air travel – a new Pandora’s box? Ro J Infect Dis. 2020;23:6–13.
Langner I, Blettner M, Gundestrup M, Storm H, Aspholm R, Auvinen A, et al. Cosmic radiation and cancer mortality among airline pilots: results from a European cohort study (ESCAPE). Radiat Environ Biophys. 2004;42:247–56.
Reynolds P, Cone J, Layefsky M, Goldberg DE, Hurley S. Cancer incidence in California flight attendants (United States). Cancer Causes Control. 2002;13:317–24.
Zeeb H, Blettner M, Langner I, Hammer GP, Ballard TJ, Santaquilani M, et al. Mortality from cancer and other causes among airline cabin attendants in Europe: a collaborative cohort study in eight countries. Am J Epidemiol. 2003;158:35–46.
Pinkerton LE, Hein MJ, Anderson JL, Christianson A, Little MP, Sigurdson AJ, et al. Melanoma, thyroid cancer, and gynecologic cancers in a cohort of female flight attendants. Am J Ind Med. 2018;61:572–81.
Hammer GP, Auvinen A, De Stavola BL, Grajewski B, Gundestrup M, Haldorsen T, et al. Mortality from cancer and other causes in commercial airline crews: a joint analysis of cohorts from 10 countries. Occup Environ Med. 2014;71:313–22.
Pukkala E, Auvinen A, Wahlberg G. Incidence of cancer among Finnish airline cabin attendants, 1967-92. BMJ. 1995;311:649–52.
Schubauer-Berigan MK, Anderson JL, Hein MJ, Little MP, Sigurdson AJ, Pinkerton LE. Breast cancer incidence in a cohort of U.S. flight attendants. Am J Ind Med. 2015;58:252–66.
McNeely E, Mordukhovich I, Staffa S, Tideman S, Gale S, Coull B. Cancer prevalence among flight attendants compared to the general population. Environ Health. 2018;17:49.
Pinkerton LE, Hein MJ, Anderson JL, Little MP, Sigurdson AJ, Schubauer-Berigan MK. Breast cancer incidence among female flight attendants: exposure-response analyses. Scand J Work Environ Health. 2016;42:538–46.
Scheibler C, Toprani SM, Mordukhovich I, Schaefer M, Staffa S, Nagel ZD, et al. Cancer risks from cosmic radiation exposure in flight: a review. Front Public Health. 2022;10:947068.
Russo AC, Marqueze EC, Furst MSG, de Sá E, Benevides EA, Roscani RC, Salim CA, et al. Aircrew health: a systematic review of physical agents as occupational risk factors. Int J Environ Res Public Health. 2023;20:5849.
Boice JDJ, Blettner M, Auvinen A. Epidemiologic studies of pilots and aircrew. Health Phys. 2000;79:576–84.
Kim MK, Han K, Lee SH. Current trends of big data research using the Korean National Health Information Database. Diabetes Metab J. 2022;46:552–63.
Lee J, Lee JS, Park S-H, Shin SA, Kim KW. Cohort profile: the National Health Insurance Service–National Sample Cohort (NHIS-NSC), South Korea. Int J Epidemiol. 2016;46:e15.
Band PR, Le ND, Fang R, Deschamps M, Coldman AJ, Gallagher RP, et al. Cohort study of Air Canada pilots: mortality, cancer incidence, and leukemia risk. Am J Epidemiol. 1996;143:137–43.
dos Santos Silva I, De Stavola B, Pizzi C, Evans AD, Evans SA. Cancer incidence in professional flight crew and air traffic control officers: disentangling the effect of occupational versus lifestyle exposures. Int J Cancer. 2013;132:374–84.
Lee W, Kang M-Y, Yoon J-H. Cancer incidence among air transportation industry workers using the National cohort study of Korea. Int J Environ Res Public Health. 2019;16:2906.
Chowdhury R, Shah D, Payal AR. Healthy worker effect phenomenon: revisited with emphasis on statistical methods - a review. Indian J Occup Environ Med. 2017;21:2–8.
Pukkala E, Helminen M, Haldorsen T, Hammar N, Kojo K, Linnersjö A, et al. Cancer incidence among nordic airline cabin crew. Int J Cancer. 2012;131:2886–97.
Dreyer L, Winther JF, Andersen A, Pukkala E. Avoidable cancers in the nordic countries. Alcohol consumption. APMIS Suppl. 1997;76:48–67.
Webber BJ, Tacke CD, Wolff GG, Rutherford AE, Erwin WJ, Escobar JD, et al. Cancer incidence and mortality among fighter aviators in the United States Air Force. J Occup Environ Med. 2022;64:71–8.
Pinkerton LE, Waters MA, Hein MJ, Zivkovich Z, Schubauer-Berigan MK, Grajewski B. Cause-specific mortality among a cohort of U.S. flight attendants. Am J Ind Med. 2012;55:25–36.
Zeeb H, Hammer GP, Langner I, Schafft T, Bennack S, Blettner M. Cancer mortality among German aircrew: second follow-up. Radiat Environ Biophys. 2010;49:187–94.
Berhan A, Bayleyegn B, Getaneh Z. HIV/AIDS associated lymphoma: review. Blood Lymphat Cancer. 2022;12:31–45.
Chen C-H, Chung C-Y, Wang L-H, Lin C, Lin H-L, Lin H-C. Risk of cancer among HIV-infected patients from a population-based nested case–control study: implications for cancer prevention. BMC Cancer. 2015;15:133.
Seo S, Park S, Lee DN, Cha ES, Park S, Jin YW. Increased incidence of thyroid cancer in occupational radiation epidemiology: attribution to screening among radiation workers. Radiat Res. 2021;195:397–400.
Suh M, Song S, Cho HN, Park B, Jun JK, Choi E, et al. Trends in participation rates for the national cancer screening program in Korea, 2002–2012. Cancer Res Treat. 2017;49:798–806.
Liu T, Zhang C, Liu C. The incidence of breast cancer among female flight attendants: an updated meta-analysis. J Travel Med. 2016;23:taw055.
IARC Working Group on the Evaluation of. Carcinogenic risks to humans. Painting, firefighting, and shiftwork. IARC Monogr Eval Carcinog Risks Hum. 2010;98:9–764.
Gehlert S, Clanton M. Shift work and breast cancer. Int J Environ Res Public Health. 2020;17:9544.
Kim HK, Song SO, Noh J, Jeong I-K, Lee B-W. Data configuration and publication trends for the Korean national health insurance and health insurance review & assessment database. Diabetes Metab J. 2020;44:671-8.
Seong SC, Kim Y-Y, Khang Y-H, Park JH, Kang H-J, Lee H, et al. Data resource profile: the national health information database of the national health insurance service in South Korea. Int J Epidemiol. 2016;46:799–800.
Kimm H, Yun JE, Lee S-H, Jang Y, Jee SH. Validity of the diagnosis of acute myocardial infarction in Korean national medical health insurance claims data: the Korean heart study (1). Korean Circ J. 2012;42:10–5.
Hwang Y-J, Park SM, Ahn S, Lee J-C, Park YS, Kim N. Accuracy of an administrative database for pancreatic cancer by international classification of disease 10(th) codes: a retrospective large-cohort study. World J Gastroenterol. 2019;25:5619–29.
Acknowledgements
Not applicable.
Funding
This study was supported by the Korea Institute of Radiological and Medical Sciences and funded by the Nuclear Safety and Security Commission of the Republic of Korea (Grant No: 50092).
Author information
Authors and Affiliations
Contributions
Conception and design: SS, SP; Formal analysis: SP; Investigation: SP, GBL, DL, KH, EC, and SS; Methodology: SS, SP; Supervision: SS; Writing-Origin draft: SP; Writing-review and editing: SP, GBL, DL, KH, EC, MC, and SS; Funding acquisition: S.S. All other authors read and commented on the drafts of the paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board (IRB) of the Korea Institute of Radiological and Medical Sciences (IRB file no. KIRAMS 2023-01-002) with a waiver for obtaining informed consent according to national regulations (Act on the protection action guidelines against radiation in the natural environment Article 18 − 3).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Park, S., Lee, G.B., Lee, D. et al. Cancer risk among air transportation industry workers in Korea: a national health registry-based study. BMC Public Health 24, 2435 (2024). https://doi.org/10.1186/s12889-024-19904-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19904-w