
Abstract
Background
Lack of physical activity (PA), poor dietary habits, or other unhealthy lifestyle behaviors are potential modifiable risk factors for hypertension. It has been sufficiently demonstrated in previous studies that physical activity or healthy dietary patterns can reduce the risk of hypertension. However, no research focused on the joint effects of PA and healthy dietary patterns on hypertension in a representative sample of adults.
Methods
We used data collected from the 2007–2018 National Health and Nutrition Examination Survey. Healthy dietary patterns were assessed with the Healthy Eating Index 2015 (HEI-2015), and PA was measured using the metabolic equivalent minutes per week reported in questionnaires. We created four lifestyle categories based on the HEI-2015 and PA: (1) unhealthy diet and physically inactive (less than recommended PA), (2) healthy diet but physically inactive, (3) unhealthy diet but physically active (recommended PA), (4) healthy diet and physically active. Logistic regression was used to evaluate the association between joint PA and HEI-2015 and hypertension.
Results
A total of 24,453 participants were enrolled in the study. Compared with unhealthy diet and physically inactive individuals, only healthy diet and physically active participants (adjusted odds ratio [AOR]: 0.77, 95% CI 0.65–0.9) were negatively associated with hypertension, while healthy diet but physically inactive participants (AOR: 0.89, 95% CI 0.76–1.03) and unhealthy diet but physically active participants (AOR: 0.9, 95% CI 0.76–1.06) were not associated with hypertension.
Conclusion
In a representative sample of US adults, our findings suggest that individuals with recommended PA and healthy dietary patterns have a lower risk of hypertension than those with an unhealthy diet or less than recommended PA. Healthy eating habits and regular PA are potential preventive precautions against hypertension.
Similar content being viewed by others


Introduction
Hypertension is a global health problem with a leading cause of cardiovascular disease and premature death, which affects about 1 billion adults worldwide [1]. By 2030, 41% of US adults are expected to be diagnosed with hypertension [2]. Hypertension may be caused by a complex combination of risk factors such as a high-sodium and low-potassium diet, sedentariness, smoking, alcoholism, and genetic factors [3, 4]. As hypertension is a chronically progressive disease, some risk factors can be controlled to prevent its development and progression [5].
Previous studies have reported a strong association between diet quality and PA on hypertension [6,7,8]. Chronic lack of physical activity (PA) is one of the risk factors for hypertension [9]. Moderate PA may contribute to lower blood pressure and improve cardiovascular health [10, 11]. PA is beneficial in enhancing heart function, inhibiting insulin resistance and inflammation in the body, promoting vasodilation, and lowering blood resistance [12, 13]. Additionally, the reduction in weight, anxiety, and depression that comes with PA can also be helpful to reduce blood pressure [14, 15]. Also, diet is strongly associated with hypertension, and a large number of studies have emphasized the importance of specific dietary patterns (e.g., the DASH diet [Dietary Approaches to Hypertension Control] and the Mediterranean diet) in controlling hypertensio n[16,17,18]. Healthy Eating Index 2015(HEI-2015) was developedbased on the Dietary Guidelines for Americans to assess dietary quality. HEI-2015 measures multiple aspects of diet, which provides a comprehensive assessment that can help people to form a healthy habit [19]. It has been proven that strict adherence to HEI-2015 helps aid blood pressure control in hypertensive patients [20].
Previous studies have provided sufficient evidence for the individual impact of PA or healthy dietary patterns in reducing the risk of hypertension. However, there has been no research on the joint effects of PA and healthy dietary patterns on hypertension in a representative sample of adults. To compensate for these limitations, our study used National Health and Nutrition Examination Survey (NHANES) data to explore the association between Joint PA and HEI-2015 and hypertension.
Materials and methods
Study population
NHANES uses a complex, multi-stage probability sampling design to select the representative, noninstitutionalized population in the US (https://www.cdc.gov/nchs/nhanes/index.htm). All participants provided written informed consent. The survey protocol was approved by the Research Ethics Review Board of the National Center for Health Statistics and the Centers for Disease Control and Prevention [21].
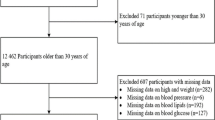
34,770 participants were aged 20 years or more. In the current study, we excluded individuals who missed valid 24-h dietary recall (n = 7,919); history of hypertension (n = 1); data about PA (n = 55). participants who had extreme total energy intakes of < 500 or > 5000 kcal/day for women, and < 500 or > 8000 kcal/day for men (n = 2,111) [22], and pregnant women (n = 231). 24,453 participants were included in the main analysis. After removing 4,979 participants with missing covariates, 19,474 participants were included in the sensitivity study (Fig. 1).

Flow diagram of inclusion criteria and exclusion criteria. Abbreviations NHANES, National Health and Nutrition Examination Survey
Hypertension
A standardized blood pressure measurement protocol recommended by the American Heart Association was used between 2007 and 2018. Trained clinicians measured blood pressure using a mercury sphygmomanometer and an appropriately sized blood pressure cuff. Blood pressure was measured after 5 min of sitting still and three blood pressure readings were taken at 30-s intervals. The average of the three measurements was used to define systolic and diastolic levels. Quality control measures included quarterly recertification and retraining of clinicians as needed and annual retraining of all clinicians. Hypertension was defined as systolic blood pressure ≥ 140 mm Hg or diastolic blood pressure ≥ 90 mmHg, self-reported history of hypertension, or use of antihypertensive medications [23, 24].
Healthy eating index 2015
Dietary intake data were obtained from two 24-h recall interviews with NHANES, conducted by a professional dietary interviewer. The first interview was conducted face-to-face, and the second interview was conducted by telephone after 3–10 days, where participants were asked to recall the types and amounts of food and beverages consumed in the past 24 h, and dietary intake was estimated using the average of the two 24-h recall data [25]. Energy and nutrient intakes for all foods were calculated using the Food and Nutrition Database for Dietary Studies [22]. NHANES Individual Food Data and Food Pattern Equivalence Database dietary data were used to construct intakes for food components for the HEI-2015.
The HEI-2015 is a tool used to assess the quality of an individual's diet. The United States Department of Agriculture Food Patterns Equivalency Database is used to convert dietary data into standardized quantities of food groups for the calculation of the HEI-2015. The HEI-2015 calculation is not based on absolute amounts of ingredients but on energy density per 1,000 kcal. It consists of 13 components, nine adequate components, including total fruits, whole fruits, total vegetables, vegetables and legumes, total protein foods, seafood and plant proteins (0–5 points each), whole grains, dairy products, and fatty acids (0–10 points each), with higher intakes scoring higher, and four moderating components, including sodium, refined grains, added sugars, and saturated fats (0–10 points each), with lower intakes, the higher the score [26]. The HEI-2015 was calculated using SAS codes [27], and higher scores indicate better overall dietary quality. This implies better compliance with DGA recommendations [26]. Participants with a two-day average score at or above the 60th percentile on the HEI were considered individuals with healthy diets (adhering to dietary guidelines or consuming healthy foods); otherwise, they were considered individuals with unhealthy diets [28].
Physical activity
Information on PA was collected using a global PA questionnaire based on that created by the World Health Organization [29]. Participants were asked to report their PA behaviors in the last 30 days. Levels of three PA types were examined: strenuous work activity/recreational activity, moderate work activity/recreational activity, and walking/cycling activity. The number of days per week they engaged in each type of PA in a typical week was reported. and the amount of time (in minutes) spent on that type of activity during the day. The frequency and duration of these activities were used to calculate weekly metabolic equivalents (Met) estimations. NHANES provides a Met corresponding to each activity category to determine activity intensity [30].
First, Met/week was calculated by multiplying the total number of minutes per week for each activity by the NHANES-recommended MET value [31], as well as the total sum of all activities was calculated by summing over all activity categories. Secondly, respondents were categorized according to compliance with US PA guidelines (moderate intensity PA in adults should be performed for 150 min per week [equivalent to 600 Met minutes/week]). Participants were classified as physically inactive individuals (600 < Met minutes/week, less than PA recommended) and physically active individuals (≥ 600 Met minutes/week, PA recommended) [32].
Lifestyle category
According to previous studies [33, 34], we created four lifestyle categories based on the HEI-2015 and PA: (1) unhealthy diet and physically inactive, (2) healthy diet but physically inactive, (3) unhealthy diet but physically active, (4) healthy diet and physically active.
Covariates
Covariates included in this study include gender ( male or female), age, race/ethnicity (Non-Hispanic White, Non-Hispanic Black, Mexican American or Other Race), education levels (below high school, high school or college/above), poverty, marital (widowed or divorced or separated, never married, married or living with a partner), alcohol drinker (never, former or now), smoking status (current smoker, former smoker or never smoked), diabetes, hyperlipidemia, body mass index (BMI, calculated as weight in kilograms divided by height in meters squared), total cholesterol, high-density lipoprotein cholesterol (HDL-C).
Statistical analysis
Data in this study were weighted using dietary interview sample weights provided by NHANES to account for the complexity of the NHANES database survey design [35]. All statistical analyses were performed using SAS 9.4 (version 9.4, SAS Institute) and R Studio software (4.2.1), and a two-sided P < 0.05 was considered statistically significant.
Continuous variables were described as mean and Confidence interval (95%CI), and categorical variables were expressed as proportions (%). Variance and chi-squared tests were used to analyze differences between groups [36]. To assess whether PA and HEI-2015 could modify the risk of hypertension, we calculated interactions on multiplicative and additive scales. Considering the exclusion of 4,979 participants with missing covariates, we used multiple interpolations for further analysis of 24,453 participants. Multiple interpolations were performed using Surveyimpute and MIANALYZE methods.
The association between PA and HEI-2015 and hypertension was assessed using multivariable logistic regression analyses, and the regression models were well-fitted (Supplementary Table 1) Results were expressed as odds ratio (OR) and 95% confidence interval (95% CI). Model 1 was adjusted for age, gender, and race. Model 2 was adjusted for model 1 plus education levels, poverty, marital, alcohol drinker (never, former, or now), and smoking status. And model 3 was further adjusted for model 2 plus diabetes, hyperlipidemia, BMI, total cholesterol, and HDL-C. We investigated the nonlinear association between PA and HEI-2015 and hypertension by including restricted cubic spline curves with nodes at the 10th, 50th, and 90th quartiles in the fully adjusted model. In addition, we used the data after excluding the missing values (n = 4979) and repeated the analysis to assess the robustness of our results.
Results
A total of 24,453 participants were enrolled in the main analysis, including 8570 hypertension. The weighted HEI-2015 was 54.2, and the PA level was 3762.36 Met-minutes/week. The mean age was 47.73 years, of which 49.17% were female. According to the lifestyle categories, age, poverty, gender, race/ethnicity, education levels, smoking status, alcohol drinker, marital, hyperlipidemia, diabetes, BMI, and HDL-C have significant differences between groups (P < 0.05) (Table 1).
Association between PA or HEI-2015 and hypertension
We first assessed the single effect of HEI-2015 or PA on hypertension (Table 2). In unadjusted for covariates (model 1), participants with healthy diet were negatively associated with hypertension compared to individuals with unhealthy diet (OR: 0.72, 95% CI 0.65–0.80), and this association remained even after adjusting for age, gender, race, and education levels, poverty, marital, smoking status, alcohol consumption, diabetes, BMI, fast total cholesterol, and HDL-C (model 3) (OR: 0.86, 95% CI 0.77–0.96). Similarly, there was a negative association between PA and hypertension. Physically active participants had a lower risk of developing hypertension compared to physically inactive individuals (OR: 0.88, 95% CI 0.78–0.99 in model 3).
Joint association between PA and HEI-2015 and hypertension
According to the PA and HEI-2015, we have divided the lifestyle categories into four groups (unhealthy diet and physically inactive, healthy diet but physically inactive, unhealthy diet but physically active, and healthy diet and physically active) and assessed the association of lifestyle categories with hypertension. Interestingly, after adjusting for age, gender, race, education levels, poverty, marital, smoking status, alcohol consumption, diabetes, BMI, fast total cholesterol, and HDL-C, compared to the unhealthy diet and physically inactive participants, only healthy diet and physically active individuals were negatively associated with hypertension (OR: 0.77, 95% CI 0.65–0.9), whereas no association with hypertension were observed for healthy diet but physically inactive individuals (OR: 0.89, 95% CI 0.76–1.03) and unhealthy diet but physically active individuals (OR: 0.9, 95% CI 0.76–1.06).
Although the additive interaction between PA and HEI-2015 was not statistically significant (RERI = − 0.052,95%CI − 2.149 ~ 2.044; AP = − 0.078,95%CI − 3.333 ~ 3.177; S = 1.189, 95%CI 0.435 -3.837) (Supplementary Table 2). However, we did RCS analyses with PA (physically inactive or physically active) and HEI-2015 (healthy diet or unhealthy diet) respectively. It was found that HEI-2015 showed an inverse dose relationship with hypertension in the physically active group and PA also showed an inverse dose relationship with hypertension in the healthy diet group (Fig. 2).

Adjusted spline curves analyze for the association of HEI-2015 (A) or PA (B) with Hypertension Among US Adults with Hypertension. Solid lines were odds ratios with 95% CI in shaded areas. Knot locations were the 10th, 50th, and 90th tertiles of PA. All models were adjusted for age, gender, race, education levels, poverty, marital, smoking status, alcohol consumption, diabetes, BMI, fast total cholesterol, and HDL-C. Abbreviations: BMI, body mass index, HDL-C, high-density lipoprotein cholesterol, HEI, Healthy Eating Index; PA, physical activity
Subgroup analyses and sensitivity analyses
The main analysis of the lifestyle-hypertension association based on demographic subgroups showed similar ORs within each group after adjusting for covariates (Supplementary Table 3). Results indicated heterogeneity in the joint association between lifestyle and hypertension between Races/ethnicity. There was a statistically significant difference in the joint association between lifestyle and hypertension among non-Hispanic whites (0.56,95% CI 0.46–0.68) and Mexican-Americans (0.66, 95% CI 0.48–0.91) who were healthy diet but physically active compared to unhealthy eaters and physically inactive individuals.
To assess potential bias from missing values, we used the data after excluding the missing values (n = 4979) and repeated the analysis. The analysis was consistent with the results of the main analysis. After adjusting for all of the covariates, compared with the unhealthy diet and physically inactive individuals, the OR for hypertension was 0.75(95% CI, 0.63–0.89) for the healthy diet and physically active participants (Supplementary Table 4).
Discussion
In this study, we evaluated the joint effect of PA with healthy dietary patterns on hypertension by using the NHANES database. Interestingly, the results showed that the risk of hypertension was lower among participants who followed a healthy dietary pattern and had recommended PA. Our findings provide new evidence for the association between joint healthy dietary patterns and recommended PA and a lower risk of hypertension than those with an unhealthy diet or less than recommended PA. Furthermore, our findings emphasize the combined effect of PA and HE-2105 on hypertension, and that the benefits to reduce the risk of hypertension cannot be achieved by failing to fulfill either of the above two.
PA is known as a modifiable lifestyle change associated with a variety of health outcomes. In a 12-week aerobic exercise trial, it was found that The mean decrease in systolic blood pressure by aerobic exercise was 7.1 mmHg, and the mean decrease in diastolic blood pressure was 5.1 mmHg [37]. However, most studies have focused on the benefits of recreational PA, and little research has been conducted on non-recreational PA. The NHANES assesses participants' PA intensity by collecting information on their work, transport, and recreational activities, which is more consistent with lifestyle [38]. Our study provides additional evidence that PA intensity is strongly associated with hypertension. PA can affect blood pressure through several mechanisms. Studies have shown that PA promotes cardiovascular health, reduces body weight, and improves peripheral arterial resistance [13]. which may explain the association between PA and the prevalence of hypertension [6]. In addition, physical activity may reduce stress-related psychological disorders such as anxiety and depression, further helping to control blood pressure and reduce the incidence of hypertension [14].
A large number of studies conducted in the last decades have emphasized the importance of diet in the risk of hypertension [16,17,18, 39]. High sodium intake may contribute to the development of hypertension, while sodium excretion, a surrogate marker of sodium intake, is also highly correlated with blood pressure levels in hypertensive patients [40]. An increase in dietary sodium content leads to an accumulation in sodium retention, which raises the venous tone and central blood volume, thus contributing to the development of hypertension [41]. A plant-based diet consists of high fiber, antioxidants, high potassium, and low saturated fat and sodium [42, 43]. A plant-based diet prevents hypertension and has beneficial effects on blood viscosity, vasodilatation, and reduction of insulin resistance [44]. In addition, with its antioxidant and anti-inflammatory properties and valuable fiber content, it can alter colonies and strains of intestinal flora and improve blood pressure by affecting the renin-angiotensin system and pressure receptors [45]. According to Lea Borgi, long-term fruit use may reduce the risk of developing hypertension [46]. A study conducted in Bangladesh found that higher fruit and vegetable intake was associated with lower annual pulse pressure and systolic blood pressure, while higher meat intake was associated with higher pulse pressure [47].
However, there is a growing emphasis in dietary studies on evaluating overall dietary patterns instead of isolated nutrients or food groups. This approach recognizes that dietary components are interconnected and consumed together[48]. By evaluating dietary patterns, one can overcome the complexity of assessing individual foods or nutrients and their interactions, thus gaining a comprehensive understanding of how overall dietary quality relates to hypertension [49, 50]. Numerous studies have conclusively shown that adopting a healthy diet is strongly correlated with reduced incidence of hypertension and lower mortality rates attributed to hypertension [5, 51, 52]. The HEI-2015 was proposed as a composite measure of dietary quality by the Dietary Guidelines for Americans (DGA), based on evidence-based recommendations from the U.S. Departments of Agriculture (USDA) and Health and Human Services (HHS). The HEI 2015 criteria have been shown to be a reliable and accurate measure of nutritional quality for Americans [48], and related studies have also demonstrated that stricter adherence can bring a preventive effect on the development of hypertension [20].
Although recommended PA and healthy diet quality are both independently associated with a reduced risk of hypertension, few studies have examined the combined effects of these lifestyle factors. Interestingly, our study found that the healthy diet and physically active participants alone were negatively associated with hypertension. Previous research has also shown that a DASH diet and exercise significantly reduces daytime ambulatory SBP compared with a DASH diet alone in a hypertensive population [53]. This is consistent with the results of this study. It is important to note that dietary patterns and PA have a strong influence on health and disease risk. Although high levels of PA may help to mitigate the negative effects of certain poor dietary habits, unhealthy eating habits may still increase the risk of developing hypertension in the long run [6, 54]. Therefore, a combination of healthy eating habits and adequate PA is the key to preventing hypertension.
The strengths of this study included a nationally representative design, information on three PA types (strenuous work activity/recreational activity, moderate work activity/recreational activity, and walking/cycling activity), and comprehensive as well as detailed dietary information. Despite this, there are limitations to our study. First, our cross-sectional study design made it difficult to determine causal associations between HEI and PA and hypertension. In the future, prospective observational and intervention studies are needed to explore how PA and dietary patterns prevent hypertension. Second, In NHANES, interviews and questionnaires were used to collect data, and data on diet, bowel, and PA were based on self-reported measurements. This may lead to inaccurate information and recall bias. In addition, PA collected by NHANES is the participant's subjective conscious report of PA, so unconscious PA may be ignored.
Conclusion
Our study shows that recommended PA combined and healthy dietary patterns were negatively associated with the risk of hypertension in a representative sample of U.S. adults. This implies that the combination of recommended physical activity with healthy dietary patterns to prevent hypertension is a practical approach. Therefore, our findings help to identify specific lifestyles that are effective in the prevention of hypertension and provide a useful reference for policymakers to initiate relevant prevention programs and promote them to the public.
Availability of data and materials
All data used in this study is available in NHANES database. NHANES—National Health and Nutrition Examination Survey Homepage (cdc.gov).
References
Schwingshackl L, Chaimani A, Schwedhelm C, Toledo E, Pünsch M, Hoffmann G, Boeing H. Comparative effects of different dietary approaches on blood pressure in hypertensive and pre-hypertensive patients: A systematic review and network meta-analysis. Crit Rev Food Sci Nutr. 2019;59:2674–87.
Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics–2014 update: a report from the American Heart Association. Circulation. 2014;129:e28–292.
Ramezankhani A, Hosseini-Esfahani F, Mirmiran P, Azizi F, Hadaegh F. The association of priori and posteriori dietary patterns with the risk of incident hypertension: Tehran Lipid and Glucose Study. J Transl Med. 2021;19:44.
Gelaw YA, Koye DN, Alene KA, Ahmed KY, Assefa Y, Erku DA, Tegegn HG, Tesema AG, Zeleke BM, Melaku YA. Socio-demographic correlates of unhealthy lifestyle in Ethiopia: a secondary analysis of a national survey. BMC Public Health. 2023;23:1528.
Motamedi A, Ekramzadeh M, Bahramali E, Farjam M, Homayounfar R. Diet quality in relation to the risk of hypertension among Iranian adults: cross-sectional analysis of Fasa PERSIAN cohort study. Nutr J. 2021;20:57.
US Preventive Services Task Force, Krist AH, Davidson KW, et al. Behavioral counseling interventions to promote a healthy diet and physical activity for cardiovascular disease prevention in adults with cardiovascular risk factors: US Preventive Services Task Force Recommendation Statement. JAMA. 2020;324:2069–75.
Camões M, Oliveira A, Pereira M, Severo M, Lopes C. Role of physical activity and diet in incidence of hypertension: a population-based study in Portuguese adults. Eur J Clin Nutr. 2010;64:1441–9.
Badr HE, Rao S, Manee F. Gender differences in quality of life, physical activity, and risk of hypertension among sedentary occupation workers. Qual Life Res. 2021;30:1365–77.
Diaz KM, Shimbo D. Physical activity and the prevention of hypertension. Curr Hypertens Rep. 2013;15:659–68.
Valenzuela PL, Ruilope LM, Santos-Lozano A, Wilhelm M, Kränkel N, Fiuza-Luces C, Lucia A. Exercise benefits in cardiovascular diseases: from mechanisms to clinical implementation. Eur Heart J. 2023;44:1874–89.
Arija V, Villalobos F, Pedret R, Vinuesa A, Jovani D, Pascual G, Basora J. Physical activity, cardiovascular health, quality of life and blood pressure control in hypertensive subjects: randomized clinical trial. Health Qual Life Outcomes. 2018;16:184.
Ml P, Ra M, Dp K, Sg N, B E, H T, Am L,. Different exercise training modalities produce similar endothelial function improvements in individuals with prehypertension or hypertension: a randomized clinical trial Exercise, endothelium and blood pressure. Sci Rep. 2020. https://doi.org/10.1038/s41598-020-64365-x.
Nyberg M, Gliemann L, Hellsten Y. Vascular function in health, hypertension, and diabetes: effect of physical activity on skeletal muscle microcirculation. Scand J Med Sci Sports. 2015;25(Suppl 4):60–73.
A D-Z, B B-F, P H-G, Ma G-G, A C-P, J R-R, S G-P, S B-F (2023) A Cross-Sectional Study on the Associations between Depression and Anxiety, Medication Use for These Diseases and Physical Activity Level in Spanish People with Hypertension. International journal of environmental research and public health. https://doi.org/10.3390/ijerph20031803
Hall ME, Cohen JB, Ard JD, et al. Weight-Loss strategies for prevention and treatment of hypertension: a scientific statement from the American Heart Association. Hypertension. 2021;78:e38–50.
Mohammadifard N, Talaei M, Sadeghi M, Oveisegharan S, Golshahi J, Esmaillzadeh A, Sarrafzadegan N. Dietary patterns and mortality from cardiovascular disease: Isfahan Cohort Study. Eur J Clin Nutr. 2017;71:252–8.
Shim J-S, Jung SJ, Kim HC. Self-reported diet management, dietary quality, and blood pressure control in Korean adults with hypertension. Clin Hypertens. 2019;25:24.
Zaribaf F, Mohammadifard N, Sarrafzadegan N, Karimi G, Gholampour A, Azadbakht L. Dietary patterns in relation to lipid profiles among Iranian adults. J Cardiovasc Thorac Res. 2019;11:19–27.
Panizza CE, Shvetsov YB, Harmon BE, Wilkens LR, Le Marchand L, Haiman C, Reedy J, Boushey CJ. Testing the Predictive Validity of the Healthy Eating Index-2015 in the Multiethnic Cohort: Is the Score Associated with a Reduced Risk of All-Cause and Cause-Specific Mortality? Nutrients. 2018;10:452.
Pasdar Y, Hamzeh B, Moradi S, Mohammadi E, Cheshmeh S, Darbandi M, Faramani RS, Najafi F. Healthy eating index 2015 and major dietary patterns in relation to incident hypertension; a prospective cohort study. BMC Public Health. 2022;22:734.
Johnson CL, Paulose-Ram R, Ogden CL, Carroll MD, Kruszon-Moran D, Dohrmann SM, Curtin LR. National health and nutrition examination survey: analytic guidelines, 1999–2010. Vital Health Stat. 2013;2:1–24.
Liu Q, Kang Y, Yan J. Association between overall dietary quality and constipation in American adults: a cross-sectional study. BMC Public Health. 2022;22:1971.
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2018;138:e426–83.
Zeng X, Zeng Q, Zhou L, Zhu H, Luo J. Prevalence of chronic kidney disease among US adults with hypertension, 1999 to 2018. Hypertension. 2023;80:2149–58.
Gress TW, Mansoor K, Rayyan YM, Khthir RA, Tayyem RF, Tzamaloukas AH, Abraham NG, Shapiro JI, Khitan ZJ. Relationship between dietary sodium and sugar intake: A cross-sectional study of the National Health and Nutrition Examination Survey 2001–2016. J Clin Hypertens (Greenwich). 2020;22:1694–702.
Krebs-Smith SM, Pannucci TE, Subar AF, Kirkpatrick SI, Lerman JL, Tooze JA, Wilson MM, Reedy J. Update of the Healthy Eating Index: HEI-2015. J Acad Nutr Diet. 2018;118:1591–602.
Healthy Eating Index SAS Code | EGRP/DCCPS/NCI/NIH. https://epi.grants.cancer.gov/hei/sas-code.html. Accessed 18 Oct 2023
Ford ES, Bergmann MM, Boeing H, Li C, Capewell S. Healthy lifestyle behaviors and all-cause mortality among adults in the United States. Prev Med. 2012;55:23–7.
Bull FC, Maslin TS, Armstrong T. Global physical activity questionnaire (GPAQ): nine country reliability and validity study. J Phys Act Health. 2009;6:790–804.
PAQ_E. https://wwwn.cdc.gov/Nchs/Nhanes/2007-2008/PAQ_E.htm. Accessed 18 Oct 2023
Wilson PB. Associations between physical activity and constipation in adult Americans: Results from the National Health and Nutrition Examination Survey. Neurogastroenterol Motil. 2020;32: e13789.
Piercy KL, Troiano RP. Physical activity guidelines for Americans from the US Department of Health and Human Services. Circ Cardiovasc Qual Outcomes. 2018;11: e005263.
Liang J, Huang S, Jiang N, et al. Association between joint physical activity and dietary quality and lower risk of depression symptoms in US Adults: Cross-sectional NHANES Study. JMIR Public Health Surveill. 2023;9: e45776.
Loprinzi PD, Smit E, Mahoney S. Physical activity and dietary behavior in US adults and their combined influence on health. Mayo Clin Proc. 2014;89:190–8.
NHANES Tutorials - Weighting Module. https://wwwn.cdc.gov/nchs/nhanes/tutorials/weighting.aspx. Accessed 18 Oct 2023
NHANES Tutorials - Variance Estimation Module. https://wwwn.cdc.gov/nchs/nhanes/tutorials/VarianceEstimation.aspx. Accessed 18 Oct 2023
Lopes S, Mesquita-Bastos J, Garcia C, et al. Effect of Exercise Training on Ambulatory Blood Pressure Among Patients With Resistant Hypertension: A Randomized Clinical Trial. JAMA Cardiol. 2021;6:1317–23.
Bazargan-Hejazi S, Arroyo JS, Hsia S, Brojeni NR, Pan D. A Racial Comparison of Differences between Self-Reported and Objectively Measured Physical Activity among US Adults with Diabetes. Ethn Dis. 2017;27:403–10.
Khodarahmi M, Asghari-Jafarabadi M, Abbasalizad Farhangi M. A structural equation modeling approach for the association of a healthy eating index with metabolic syndrome and cardio-metabolic risk factors among obese individuals. PLoS ONE. 2019;14:e0219193.
Mente A, O’Donnell MJ, Rangarajan S, et al. Association of urinary sodium and potassium excretion with blood pressure. N Engl J Med. 2014;371:601–11.
He FJ, Tan M, Ma Y, MacGregor GA. Salt Reduction to Prevent Hypertension and Cardiovascular Disease: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75:632–47.
Alexander S, Ostfeld RJ, Allen K, Williams KA. A plant-based diet and hypertension. J Geriatr Cardiol. 2017;14:327–30.
Joshi S, Ettinger L, Liebman SE. Plant-Based Diets and Hypertension. Am J Lifestyle Med. 2020;14:397–405.
Lee KW, Loh HC, Ching SM, Devaraj NK, Hoo FK. Effects of Vegetarian Diets on Blood Pressure Lowering: A Systematic Review with Meta-Analysis and Trial Sequential Analysis. Nutrients. 2020;12:1604.
Marques FZ, Nelson E, Chu P-Y, et al. High-Fiber Diet and Acetate Supplementation Change the Gut Microbiota and Prevent the Development of Hypertension and Heart Failure in Hypertensive Mice. Circulation. 2017;135:964–77.
Borgi L, Muraki I, Satija A, Willett WC, Rimm EB, Forman JP. Fruit and Vegetable Consumption and the Incidence of Hypertension in Three Prospective Cohort Studies. Hypertension. 2016;67:288–93.
Jiang J, Liu M, Parvez F, et al. Association of major dietary patterns and blood pressure longitudinal change in Bangladesh. J Hypertens. 2015;33:1193–200.
Morze J, Danielewicz A, Hoffmann G, Schwingshackl L. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: A Second Update of a Systematic Review and Meta-Analysis of Cohort Studies. J Acad Nutr Diet. 2020;120:1998-2031.e15.
Schwingshackl L, Schwedhelm C, Hoffmann G, Knüppel S, Iqbal K, Andriolo V, Bechthold A, Schlesinger S, Boeing H. Food Groups and Risk of Hypertension: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv Nutr. 2017;8:793–803.
Turner-McGrievy GM, Wilson MJ, Carswell J, et al. A 12-Week Randomized Intervention Comparing the Healthy US, Mediterranean, and Vegetarian Dietary Patterns of the US Dietary Guidelines for Changes in Body Weight, Hemoglobin A1c, Blood Pressure, and Dietary Quality among African American Adults. J Nutr. 2023;153:579–87.
Li S, Zhu Y, Chavarro JE, et al. Healthful Dietary Patterns and the Risk of Hypertension Among Women With a History of Gestational Diabetes Mellitus: A Prospective Cohort Study. Hypertension. 2016;67:1157–65.
Zhang Y, Li D, Zhang H. Associations of the Healthy Eating Index-2010 with risk of all-cause and heart disease mortality among adults with hypertension: Results from the National Health and Nutrition Examination Survey 2007–2014. Front Nutr. 2023;10:1077896.
Lee CJ, Kim JY, Shim E, Hong SH, Lee M, Jeon JY, Park S. The Effects of Diet Alone or in Combination with Exercise in Patients with Prehypertension and Hypertension: a Randomized Controlled Trial. Korean Circ J. 2018;48:637–51.
Di Raimondo D, Buscemi S, Musiari G, Rizzo G, Pirera E, Corleo D, Pinto A, Tuttolomondo A. Ketogenic Diet, Physical Activity, and Hypertension-A Narrative Review. Nutrients. 2021;13:2567.
Acknowledgements
We express our gratitude to the National Center for Health Statistics at the CDC for their responsibilities in designing, collecting, and administering the NHANES data and for making it accessible to the public.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
The authors’ responsibilities were as follows—Mr. Yanzhou Zhu had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: Yanzhou Zhu; Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: Yanzhou Zhu; Critical revision of the manuscript for important intellectual content: Zhigang Wang.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the NCHS Institutional Review Board. Written informed consent was obtained from all subjects/patients.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhu, Y., Wang, Z. Association between joint physical activity and healthy dietary patterns and hypertension in US adults: cross-sectional NHANES study. BMC Public Health 24, 855 (2024). https://doi.org/10.1186/s12889-024-18346-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18346-8