
Abstract
Background
Positive psychology interventions are known to have an impact on mental health as well as on a number of beneficial characteristics like optimism, gratitude and self-efficacy. The Positive Emotions Training (PoET) is one of the first holistic training programs covering eleven positive psychology constructs. The goal of this study was to test PoET’s feasibility in the general population and to assess possible effects on positive and negative mental health factors. Additionally, possible effects on optimism, gratitude, happiness, resilience, and self-efficacy were examined.
Methods
The sample (n = 101) was not randomized. Participants were allocated to PoET (n = 55) or control group (n = 46) that did not receive treatment initially. The PoET group completed two training sessions (3.5 h each) that were conducted in an online format with groups of about 30 people. All participants completed positive and negative mental health measures at the beginning of the first training session and at the beginning of the second one as well as 30 days after the second session. Two-factorial repeated measures ANOVAs were conducted to test for possible effects of PoET on mental health.
Results
The results showed that the contents were comprehensible and that the conduction of the training was feasible overall. In addition, a significant decrease of depression and anxiety symptoms as well as a significant increase of optimism were found in the PoET group. No significant changes were found in the control group.
Conclusions
Results indicate that PoET is an applicable intervention for improving mental health in the general population.
Trial registration
Retrospectively registered at ClinicalTrials.gov on 21/02/2023 (Identifier/Trial registration number: NCT05737251).
Similar content being viewed by others
Background
Mental disorders affect millions of people worldwide, causing suffering and various negative consequences. According to the World Health Organization (WHO), the lifetime prevalence ranges from 18.1 to 36.1% [1]. Studies indicate reduced life expectancy by nearly 18 years for individuals with mental disorders [2,3,4]. Also, Disability Adjusted Life Years (DALYs) [5] related to mental disorders have significantly increased since 2005, with depressive and anxiety disorders ranking among the top causes [6]. Global public healthcare costs associated with mental disorders are substantial [7, 8]. For example, in the US anxiety disorders alone account for one-third of total expenditures on mental disorders [9, 10]. Depressive disorders in the UK result in £9 billion in costs, 100 million lost working days, and 2,615 deaths [11], while, for example, Germany spends approximately €27 billion on mental disorder treatment and compensation, representing 11.3% of medical spending [12]. In addition, mental disorders negatively impact education, employment, and overall quality of life [13]. These findings indicate that mental disorders have severe negative consequences for individuals and society.
Several studies highlight the psychological burden of the COVID-19 pandemic and related restrictions [14,15,16], including a negative impact on mental health in the general population [17,18,19]. Unlike other mental disorders that returned to pre-pandemic levels, depression and mood disorders remained alarmingly high [20]. Germany, specifically, faces overcrowded psychotherapy practices, with an average waiting time of 19.9 weeks for treatment initiation [21, 22]. Consequently, patients may not seek therapy at all due to long waiting periods [23, 24]. Access to alternative psychological support, such as primary and secondary prevention, is limited in the German healthcare system [25]. Considering the high prevalence of mental illness and the pandemic’s impact, it is crucial to provide more accessible psychological help, particularly through low-threshold interventions that compensate the long waits and accessibility challenges. Hence, our research team developed a low-threshold program to enhance mental health in a broad population. By combining clinical and positive psychological approaches, a new form of low-threshold intervention might be created.
For a long time, psychology focused on curing existing psychopathologies. Positive psychology has shifted the focus from dealing only with the negative aspects of life to further improving positive qualities [26]. In this context, the consideration of positive emotions plays a relevant role. The broaden-and-build theory points out that positive emotions can expand the repertoire of thought and action and build up lasting personal resources [27, 28]. Following these considerations, it seems to be useful to promote the experience of positive emotions to build up such resources. In the past decades, positive psychology interventions [29] based on the principles of positive psychology were developed to promote positive emotions, behavior, or cognitions [30]. Meta-analyses support the efficacy of positive psychology interventions for improving mental health and well-being [30,31,32,33].
However, most studies so far have examined individual exercises, but rarely entire holistic training programs. Mostly, such training programs were designed for specific target groups. The first training program of this kind was developed to increase happiness and life satisfaction in college students. It extended over six weeks and was able to significantly increase happiness of the participants [34]. Positive psychology training programs have also successfully been conducted with patients with various physical symptoms or diseases: Positive effects on pain perception and depressive symptoms as well as an increase of positive affect were found [35,36,37]. Furthermore, it was explored how positive psychology interventions can be used as a psychotherapy program: Positive psychotherapy was able to reduce mild to moderate depression [38]. A similar approach was chosen in a study by Chaves and colleagues in patients with major depression or dysthymia whose clinical symptoms and well-being were shown to improve [39].
Overall, the literature supports the effectiveness of positive psychology training programs. However, as described above, research so far has focused on testing the effectiveness of such trainings in specific target groups or individual exercises, but not as a holistic training program in the general population. To contribute to closing this research gap, we developed the Positive Emotions Training (PoET) which refers to the promotion of several positive psychology constructs and the improvement of mental health. The development of PoET was based on existing literature on positive psychology treatments as well as long-term discussions among the research group about how to promote respective constructs. For the training, an online format was chosen so that it could be conducted in larger groups despite the prevailing COVID-19 pandemic.
We decided to test PoET as an intervention and the methodical approach in a feasibility study. The main goal of this study was to evaluate the practicability of PoET and examine whether it might be an effective intervention to promote mental health. First, we hypothesized that participants receiving PoET would show a significant increase in positive mental health factors one month after the second training day (Hypothesis 1). Second, we expected to find a significant decrease in depression, anxiety, and stress symptoms one month after the second training day (Hypothesis 2). Third, we hypothesized participants in the control group not to show any significant changes in this regard (Hypothesis 3). In addition, we examined whether there might be a significant increase in optimism, gratitude, happiness, resilience, and self-efficacy for participants of PoET in comparison to the control group.
Methods
Recruitment
To advertise the PoET, a flyer was distributed on social media and two articles were published in newspapers. Those interested could contact an email address to receive further information about the training and to apply. Participants for the control group were also recruited via social media. As PoET is a low-threshold intervention, there were no exclusion criteria for participation and no screening for mental illness before the start. Any person older than 18 years could participate. Psychology students could get VPN hours as compensation. Overall, nearly 600 people were interested in participating. Because the number of psychologists to conduct training sessions was limited, not everyone got the possibility to participate. Places in the intervention study were not randomly allocated, but according to the principle “first-come, first-served”. Participants of the control group did not receive any treatment initially, but were offered to participate in one of the next PoETs.
Participants
A total of N = 174 participants completed the registration process and baseline steps of the study and were finally offered to participate. Out of those, n = 100 were allocated to the PoET intervention group and n = 74 were allocated to the control group.
PoET
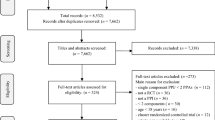
Since we were interested in the specific outcome effects of the training, only participants who took part at both training days and completed all data sets were considered in the analyses. N = 100 subjects took part in the first training session, of which n = 92 completed the first questionnaire. Up to the second session, there was a drop-out of n = 25 (27.17%). N = 1 (1.09%) did not fill out the last questionnaire. After another n = 11 (11.96%) data sets were removed because of missing values, n = 55 (59.78%) data sets were used for calculations. Participants in the PoET group were between 22 and 76 years old (M = 45.98, SD = 15.97) and n = 49 (89%) of the group were female. 12 participants were college students (22%), while n = 35 (64%) were employed and n = 8 (15%) were retired or classified themselves as homemakers. N = 39 participants were in stable relationships or married (71%).
Control
The final sample consisted of n = 46 persons because participants who did not complete the questionnaires at all three assessment points (n = 28, 37.84%) were excluded. Participants were between 19 and 68 years old (M = 35.13, SD = 15.37) and n = 35 (76%) of the group were female. N = 17 participants were college students (37%), n = 24 were employed (52%) and n = 5 (11%) were retired, in an apprenticeship or considered themselves homemakers. N = 28 participants were in stable partnerships or married (61%).
The two groups differed significantly in their age (t(99) = 3.459, p < .001).
Development and description of PoET
For the development of PoET, a systematic literature analysis was first carried out within the context of the project “On the Role of Positive Emotions in the Promotion of Mental Health - An Experimental Study” to collect various positive psychology constructs and exercises for the promotion of positive emotion experience. Over a period of three years, these results were discussed in context of the Annual Congress for Psychotherapy in Bochum and a list of about 20 important positive psychological constructs was developed. A further literature analysis of the existing possibilities for promoting these constructs was conducted. Based on their potential regarding feasibility and effects on mental health, eleven constructs were selected by the team and included in the training. Exercises from already existing literature were compiled and own exercises were developed afterwards. After that, the exercises and formal aspects of the training were tested in a pilot phase in January 2022. In the context of this pilot phase, an exemplary training session was conducted with a group of volunteers and feedback was collected as well as integrated into the general PoET concept.
The PoET conducted in spring 2022 consisted of two training days of 3.5 h each, one week apart. The training was carried out online via Zoom in groups of about 30 to 35 people and was led by two psychologists who were also part of the research team. A total of eleven lessons on positive psychology constructs were conducted: happiness, hope, optimism, humor, self-efficacy, gratitude, flow, meaningfulness, forgiveness, spirituality, and resilience. At the beginning of each lesson, the participants received a short theoretical input on the respective positive psychology construct. After that, exercises were carried out either in the large group, in groups of three to six people in breakout rooms or alone. Afterwards, there was a short discussion on how the participants experienced each respective exercise. Finally, participants were given at-home-exercises. In addition, the participants received a booklet with descriptions of the exercises and space for notes. During the training days, a PowerPoint presentation was used as visual support. Between the two training days, there was a so-called 7-day challenge which should motivate the participants to complete the exercises at home. Table 1 lists the positive psychology constructs and the respective exercises.
Measures
At all three assessment points, participants in the PoET and control group completed a battery of questionnaires. Socio-demographic data, questions about the experience of flow, current mood and stress, and exercise practice at home (in the PoET group) were assessed. In addition, the battery contained the German versions of ten validated questionnaires. The following seven questionnaires were relevant for this study.
DASS-21
The Depression Anxiety Stress Scale [40] was used to assess the negative emotional states of depression, anxiety, and stress. The questionnaire consists of 21 items. On a scale from 0 (“did not apply to me at all”) to 3 (“applied to me very much or most of the time”), participants could indicate their agreement with the items. The sum scores of the three subscales were used for calculations. Higher scores indicate worse mental health. A good internal consistency could be demonstrated for the three subscales depression (α = 0.89), anxiety (α = 0.75) and stress (α = 0.87).
PMH
The Positive Mental Health Scale [41] assesses emotional and psychological aspects of wellbeing across nine items. On a scale from 0 (“I do not agree “) to 3 (“I agree”), participants indicate their agreement with the items. Sum scores were formed for the calculations with higher scores indicating greater positive mental health. For the current sample an internal consistency of α = 0.91 was found.
LOT-r
The Life Orientation Test-revised [42] assesses the dispositional optimism. This questionnaire consists of 10 items. Of them, six capture dispositional optimism, while four items are filler items. On a scale from 0 (“strongly disagree”) to 4 (“strongly agree”), agreement with the items could be indicated. Higher values represent a higher level of dispositional optimism. The sum score was used for the calculation after three negatively formulated items have been inverted. In this sample, we found an internal consistency of α = 0.77.
GQ-5
The Gratitude Questionnaire [43] measures gratitude across five items. On a scale from 1 (“strongly disagree”) to 7 (“strongly agree”) agreement with the statements can be indicated. A scale mean was used for the calculation with higher scores indicating a more pronounced sense of gratitude. A Cronbach’s alpha of α = 0.82 could be found in the current sample.
SWLS
The Satisfaction with Life Scale [44] assesses global subjective happiness across five items. Participants were asked to rate their agreement with the items on a scale from 1 (“strongly disagree”) to 7 (“strongly agree”). The sum score was used for analysis with higher values indicating a happier person. For the current sample an internal consistency of α = 0.90 could be proven.
NGSE
The New General Self-Efficacy Scale [45] is an 8-item scale used to assess how much the participants believe in their ability to perform across a variety of situations. On a scale from 1 (“strongly disagree”) to 5 (“strongly agree”), agreement with the items can be indicated. Mean values were used for the calculation with higher scores representing higher self-efficacy. A Cronbach’s alpha of α = 0.89 could be found in this sample.
BRS
The Brief Resilience Scale [46] measures the participants’ ability to recover from stress despite significant adversity across six items. On a scale from 1 (“strongly disagree”) to 5 (“strongly agree”) participants could indicate their agreement with the items. The scale mean was used for the calculations with higher scores representing a higher resilience. For the current sample an internal consistency of α = 0.85 could be demonstrated.
Procedure
PoET
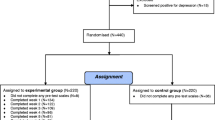
Figure 1 shows the chronological order of PoET. To register for the training, all participants of the PoET group had to give their written consent. One day before the training, participants received the link to join the online meeting as well as the exercise booklet. The first training day started with all participants filling in the first questionnaire (T1). Afterwards, the participants were officially welcomed, and everyone had the opportunity to introduce themselves briefly. The rules for the training were explained and there was a short introduction to the topic of emotions which was followed by the lessons on happiness, hope, optimism, humor, self-efficacy, and gratitude. Thereafter, the 7-day challenge was explained, and the participants got a short preview on the contents of the second training day. Finally, participants’ mood and stress were assessed via two short items (on a 5-point Likert scale). The second day of training began with the completion of the second questionnaire (T2). Afterwards, participants were asked about their experiences during the 7-day challenge and the lessons on flow, meaningfulness, spirituality, forgiveness, and resilience were conducted. Then participants assessed their mood and stress in a short questionnaire. Finally, participants were asked which exercises they would integrate into their everyday life. Thirty days later, participants received an email with a link to the last questionnaire (T3).

Chronological order of PoET procedure
Control
Participants of the control group only filled out the questionnaires at three assessment points. This happened in the same intervals as in the PoET group. They received the link to the questionnaires via email.
This study was approved by the Local Ethics Committee for Psychological Studies of Ruhr-University Bochum. All methods were performed in accordance with the relevant guidelines and regulations.
Data analysis
The statistics program R Studio (version 2022.02.3) [47] was used for calculations. A two-factorial analysis of variance (ANOVA) with repeated measures was conducted to investigate changes in positive mental health factors (measured via PMH) in the PoET and the control group over the three assessment points. The two groups served as between-subject factor and the three assessment points as within-subject factor (2 × 3 mixed design). In the same procedure, possible differences in negative mental health, measured via DASS-21, were analyzed. The two-factorial analysis of variance with repeated measures was conducted for all three subscales depression, anxiety and stress. Bonferroni-adjusted pairwise comparisons between assessments and groups (time*group interactions) were performed. To test the prerequisites for the analyses, the Mauchly test for sphericity and the Shapiro-Wilk test for normal distribution were carried out. All prerequisites were met. The sample size was determined by power calculations which indicated that a sample of 61 would be sufficient for p < .05 with a power of 0.8 and an effect size of \(\eta_p^2\) = 0.14.
In addition, we examined whether the individual constructs that were treated as lessons during the training had changed in the PoET group in comparison to the control group by conducting another two-factor analysis of variance with repeated measures. The two groups served as between-subject factor and the three assessment points as within-subject factor (2 × 3 mixed design).
The level of significance was set as p < .05 for all calculations. \(\eta_p^2\) was calculated as effect size. According to Cohen [48], a \(\eta_p^2\) of 0.01 can be considered small, 0.06 medium, and 0.14 a large effect. Missing data was not imputed. Data sets with missing data were excluded from the statistical analyses.
Results
Results at baseline
At T1, the two groups significantly differed from each other in their PMH scores (p = .032) with higher scores in the control group. For DASS-21 subscales, no significant differences were found between PoET and control group at baseline (all p values > 0.08). The complete baseline results can be found in Table 2.
Effects of PoET on PMH scores
Descriptively, there was a higher increase in the PoET group PMH sum scores from T1 to T2 and T1 to T3 compared to the control group. While the PMH scores of the control group were significantly higher at T1, the PoET PMH scores approached the control at T2 and T3. The repeated measures ANOVA also showed a significant time*group effect (F(1.79, 177.34) = 3.385, p = .041; \(\eta_p^2\) = 0.033) for T1. Despite the descriptive differences in the PoET group from T1 to T2 and T1 to T3, the Bonferroni-adjusted pairwise comparisons showed no significance for those differences (all adjusted p values > 0.193). There were no significant results for the control group either. All mean differences are presented in Table 3.
Effects of PoET on DASS-21 scores
The repeated measures ANOVA showed significant time*group effects for the subscales DASS-D (F(1.87, 185.11) = 4.031, p = .011; \(\eta_p^2\) = 0.046) and DASS-A (F(2, 198) = 5.233, p = .006; \(\eta_p^2\) = 0.050). Bonferroni-adjusted pairwise comparisons showed that the PoET group DASS-D scores differed significantly from T1 to T2 (Mdiff = -2.36, adj. p = .002, d = 0.62) and from T1 to T3 (Mdiff = -2.56, adj. p < .001, d = 0.66). There were no significant differences between the assessment points in the control group (all adj. p > .507). It was the same for the DASS-A scores: The PoET group scores differed significantly from T1 to T2 (Mdiff = -1.84, adj. p = .001, d = 0.65) and from T1 to T3 (Mdiff = -2.05, adj. p < .001, d = 0.73). There were no significant differences between the assessment points in the control group (all adj. p > .624).
For the DASS-S there was a significant time effect (F(1.84, 182.48) = 19.504, p < .001; \(\eta_p^2\) = 0.165). The DASS-S scores of the whole sample (independent from group affiliation) differed significantly from T1 to T2 (adj. p > .001) and from T1 to T3 (adj. p > .001). There were no significant time*group interactions. A graphic presentation of those findings can be found in Fig. 2.

Changes in different measures for all assessment points and groups. Note. The blue lines depict significant changes in the PoET group. Significant differences between the groups at one specific assessment point are presented in black. PMH = Positive Mental Health Scale, DASS-21 = Depression-Anxiety-Stress Scale, DASS-D = Subscale “depression”, DASS-A = Subscale “anxiety”, DASS-S = Subscale “stress”, LOT-r = Life Orientation Test revised, GQ-5 = Gratitude Questionnaire, BRS = Brief Resilience Scale, SWLS = Satisfaction with Life Scale, NGSE = New General Self-Efficacy Scale. *p < .05, **p < .01, ***p < .001
Effects of PoET on discussed positive psychology constructs
Optimism
The two-factor analysis showed a significant time*group effect (F(2, 198) = 8.742, p < .001; \(\eta_p^2\) = 0.081) for the PoET group from T1 to T3 (adj. p < .001). There was also a significant difference between both groups at T3 (adj. p = .021) with higher scores in the PoET group.
Gratitude
With respect to the graphic presentation of descriptive statistics, there was a high increase of mean gratitude scores in the PoET group from T1 to T2 and T1 to T3. Results of the conducted repeated measures ANOVA showed a significant time*group effect (F(1.78, 176.23) = 3.913, p = .026; \(\eta_p^2\) = 0.038) which did not withstand the Bonferroni correction in any direction (adj. p > .091).
Resilience
Descriptive measures showed an increase of mean resilience scores in the PoET group from T1 to T2 and from T2 to T3. In the control group there was a slight decrease of mean resilience scores from T2 to T3. The repeated measures ANOVA showed no significant effects in neither of the two groups nor three assessments (all p values > 0.088).
Happiness
While the happiness sum scores in the control group graphically were relatively stable, there was a visible increase in the PoET group from T1 to T2. The repeated measures ANOVA showed a significant time*group effect (F(1.8, 178.45) = 3.560, p = .035; \(\eta_p^2\) = 0.035) which did not withstand the Bonferroni correction (adj. p > .343).
Self-efficacy
The repeated measures ANOVA showed a significant time*group effect (F(2, 198) = 10.754, p < .001; \(\eta_p^2\) = 0.098). The PoET and control group differed significantly at baseline (adj. p = .003) with M = 29.56, SD = 4.98 for the PoET group and M = 32.33, SD = 4.24 for the control group. Despite descriptive differences between the three assessments, the Bonferroni-adjusted pairwise comparisons showed no significance for those differences (all adjusted p values > 0.305).
A graphic presentation of the descriptive data for all relevant measures can be found in Fig. 2. All mean and sum scores of the different measures in this last part of the results are presented in Table 4.
Discussion
The main goal of this study was to evaluate the practicability of PoET and to examine whether PoET might be effective to promote mental health in the general population. We hypothesized an increase in positive mental health factors (Hypothesis 1) and a decrease in depression, anxiety, and stress symptoms (Hypothesis 2) in PoET participants one month after the second training day. For the control group, we hypothesized that there would be no changes in these scores (Hypothesis 3).
Regarding the effectiveness of PoET, our results were mixed but definitely promising. Due to the fact that the groups were not randomly allocated, these findings should be handled with care.
According to the first hypothesis, there was a descriptive increase in positive mental health factors assessed with the PMH in the PoET group, but the differences were not significant in the statistical analyses so that the hypothesis could not be confirmed with the present data. These results are in contrast to previous research: While we found no significant changes in PMH scores of the PoET group, other studies showed positive effects of positive psychology interventions on (psychological) well-being [30,31,32,33]. When looking at descriptive values of the PMH, after a significant difference between the groups at T1 (with higher scores in the control), the PoET group scores increased so far that there no longer were significant differences at T2 and T3. These findings indicate that the training was effective in improving the PoET group’s positive mental health, however, this can only be described as a trend due to the lack of significance.
In this regard, it is important to refer to possible reasons for the absence of significance: One of them could be the differences of the PoET and control group. Since the groups were not randomly assigned, they differed significantly in age (p < .001) and in PMH scores at T1 (p = .041). Previous research has been able to find correlations between age and mental health [1, 49, 50]. Therefore, it would be necessary to examine PoET and its effects on positive mental health factors in a randomized-controlled trial to avoid significant group differences and allow analyses without confounding variables. Another contributing factor might be that this study did not record which exercises the participants continued to do at home. Thus, we were not able to backtrace the effectiveness of specific exercises. It is possible that some of the participants did not exercise at all within the 7-day challenge and after the training and that the boosting effect on their mental health was therefore not achieved. To ensure the training’s full potential, it would be helpful to assess the frequency and duration of exercising at home. Nevertheless, the results regarding the increase of PMH scores in the PoET group show that PoET as a low-threshold intervention was able to settle the significant differences between the two groups.
The second hypothesis could be partially confirmed with significant decreases of depression and anxiety symptoms assessed with the DASS-21 from T1 to T3. According to Cohen [48], the found effect sizes represent a medium effect. For stress symptoms, no significant effect was found but there was a descriptive decrease pointing in the same direction. The findings regarding Hypothesis 2 fit partially into the picture of previous research: Several meta-analyses could show significant effects of positive psychology interventions on depressive symptoms [30,31,32,33]. Like in our study, some of those meta-analyses also found small to moderate effects on anxiety symptoms. In contrast to our results, they also found significant effects on stress symptoms [32, 33]. Since stress measurements in this study showed an overall decrease in the PoET group among all three assessments, a long-term follow-up (e.g., three months) would have revealed possible significant long-term changes.
Overall, these results indicate that PoET is effective to reduce symptoms of depression and anxiety in the general population. It is still to explore, whether an adjusted version of PoET might have similar effects in a clinical population. In the future, based on these promising results, PoET should be further examined and evaluated in a randomized controlled trial.
According to the third hypothesis, there were no significant changes in the control group in neither of these measures, which suggests that the improvements in the PoET group can be attributed to the training itself and not to other possible environmental factors.
In addition to the three hypotheses, we also examined possible increases in other relevant dimensions in the PoET group in comparison to the control. These were optimism, gratitude, resilience, happiness, and self-efficacy. Solid significant changes could only be found in optimism with a medium effect size [48]. Increases in optimism in the PoET group were so high that their scores significantly exceeded the control group at T3. One possible reason for this effect might be the usage of the highly evaluated best possible self-method that is proven to be effective in many studies [51,52,53] and meta-analyses [54, 55]. Therefore, our findings match those of previous literature. Optimism is known to correlate with well-being under adverse circumstances [56], positive physical health measures [57] and less psychopathology [58, 59]. Hence, our results for optimism can be seen as particularly valuable.
For the other constructs (gratitude, resilience, happiness, and self-efficacy), no significant effects were found, but all of them increased descriptively, indicating that there were slight improvements. Since other studies have shown that positive psychology interventions are able to enhance these constructs [60,61,62,63], it can be assumed that the lack of significance is based on methodical issues. One of them might be that not all of the used exercises were as effective as the ones in the studies mentioned above. For self-efficacy, for example, due to the short time dimension of PoET, the exercise addressed self-efficacy more on a surface level, similar to self-confidence. Maybe this kind of exercise was not profound enough to change NGSE-scores. For happiness, one factor could be the used questionnaire, as the SWLS explicitly assesses life satisfaction and not happiness [44]. An alternative questionnaire that could be used in future studies is the Positive and Negative Affect Schedule (PANAS, [64]) whose measurements are probably closer to happiness than those of the SWLS. Another more general contributing factor could lay in the problem of group allocation, which was neither randomized nor matched, therefore resulting in group differences and difficulties regarding their comparability. However, it can be noted that there were some descriptive changes in the positive psychology constructs warranting further examination in a randomized controlled trial.
Besides these promising results, the main goal of this study was to test PoET’s feasibility regarding the general concept and the training circumstances. Implementing PoET as a two-session online training was experienced to be feasible by the research team as well as participants. Beforehand, we had considered whether to conduct the training within one session, two sessions or more. Although past positive psychology intervention studies often used five or more training sessions [34, 36, 39], we decided to keep our training concept as short as possible to minimize dropout rates and to facilitate the participation. Overall, participants reported that two sessions (3.5 h each) were perceived as the optimal solution because they were able to keep up their concentration during the sessions and integrate them into their daily life more easily than attending more sessions. Despite primary worries regarding the online format, conducting the training via Zoom had more advantages than disadvantages: The participation was possible from everywhere in Germany, difficulties regarding the arrival time and costs could be avoided, and the training could be conducted in large groups of about 30 people despite the ongoing COVID-19 pandemic. However, some participants experienced slight complications while logging in or retrieving the online questionnaire via Zoom. Those complications did not affect the training in general but were time consuming. In the future, it would be helpful to send detailed instructions on how to use Zoom before the beginning of the online session. Although the group size of approximately 30–35 persons was relatively large, it was perceived as fitting for this kind of training by participants as well as the research team. There was enough time for everyone to ask questions or share their experiences in the large group as well as possibilities to have more intimate conversations in breakout rooms in smaller groups.
Limitations and future research
When interpreting the results, the following limitations must be considered. There were differences between both groups, that affected their comparability: At T1, the control group scored descriptively lower on the subscales of the DASS-21 and significantly higher (p = .032) on the PMH than the PoET group. In addition, the two groups differed significantly in their mean age (p < .001). This is critical as previous research has been able to find correlations between age and mental health [1, 49, 50]. Regarding the sample, it is also critical that there was no randomization, but rather a separate search for participants for the two groups, and that a large proportion of participants was female (PoET: 89%, control: 76%). High dropout rates of 45% in the PoET group and 37.84% in the control should also be considered. This can largely be attributed to errors in filling out the questionnaires or not being present at both training days. Finally, a limitation regarding the process of the questionnaires should be addressed: As no questionnaires were filled out after the end of the second training day, no statement can be made on how the training affected the mental health of the participants directly after completion. Thus, it could only be concluded that the training led to improvements in mental health at the beginning of the second training day and one month after the second training day.
Since the interest in participating in our study was tremendously high (nearly 600 people contacted us), future studies should address the urgent need for low-threshold interventions. Due to its simple structure, our PoET has the potential to build a foundation for a large-scale implementation. Future research is needed to test the effects of PoET on mental health in a randomized controlled trial. This would lead to more comparable groups when assessing the impact of the training on various positive psychological variables. As this research showed that PoET could significantly reduce depression and anxiety scores on the DASS-21 in the general population, it would also be interesting to investigate whether implementing the training can also improve depressive or anxiety symptoms in people with a diagnosed mental illness. Another interesting approach would be a comparison between an online and offline form of PoET to assess possible differences in the effectiveness.
Conclusion
The main goal of the present study was to test the feasibility of a low-threshold intervention promoting positive emotions. The results showed that PoET in its recent form could be successfully conducted in the general population. In addition, significant effects on depression, anxiety, and optimism were found. Overall, PoET appears to have the potential to contribute to psychotherapeutic interventions. After further and clinical validation, PoET as a low-threshold treatment could be used in the area of prevention as well as during the long waiting periods before the beginning of therapy.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on request.
Abbreviations
- BRS:
-
Brief Resilience Scale
- DASS-21:
-
Depression Anxiety Stress Scale
- GQ-5:
-
Gratitude Questionnaire Five Items Form
- LOT-r:
-
Life Orientation Test (revised)
- NGSE:
-
New General Self-Efficacy Scale
- PMH:
-
Positive Mental Health Scale
- PoET:
-
Positive Emotions Training
- SWLS:
-
Satisfaction with Life Scale
- T1 – T3:
-
Assessment 1–3
References
Kessler RC, Angermeyer M, Anthony JC, de Graaf RO, Demyttenaere K, Gasquet I, et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the world health organization’s world mental health survey initiative. World Psychiatry. 2007;6(3):168–76.
Chang C-K, Hayes RD, Perera G, Broadbent MTM, Fernandes AC, Lee WE, et al. Life expectancy at birth for people with serious mental illness and other major disorders from a secondary mental health care case register in London. PLoS ONE. 2011;6(5): e19590.
Hjorthøj C, Stürup AE, McGrath JJ, Nordentoft M. Years of potential life lost and life expectancy in schizophrenia: a systematic review and meta-analysis. Lancet Psychiatry. 2017;4(4):295–301.
Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiat. 2015;72(4):334–41.
Murray CJ. Quantifying the burden of disease: the technical basis for disability-adjusted life years. Bull World Health Organ. 1994;72(3):429–45.
Kassebaum NJ, Arora M, Barber RM, Bhutta ZA, Brown J, Carter A, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the global burden of Disease Study 2015. Lancet. 2016;388(10053):1603–58.
Christensen MK, Lim CCW, Saha S, Plana-Ripoll O, Cannon D, Presley F, et al. The cost of mental disorders: a systematic review. Epidemiology and Psychiatric Sciences. Cambridge University Press; 2020;29:e161, 1–8. https://doi.org/10.1017/S204579602000075X.
Arias D, Saxena S, Verguet S. Quantifying the global burden of mental disorders and their economic value. EClinicalMedicine. 2022;54: 101675. https://doi.org/10.1016/j.eclinm.2022.101675.
DuPont RL, Rice DP, Miller LS, Shiraki SS, Rowland CR, Harwood HJ. Economic costs of anxiety disorders. Anxiety. 1996;2(4):167–72.
Rice DP, Miller LS. Health economics and cost implications of anxiety and other mental disorders in the United States. Br J Psychiatry. 1998;173(S34):4–9.
Thomas CM, Morris S. Cost of depression among adults in England in 2000. Br J Psychiatry. 2003;183(6):514–9.
Nöthen M, Böhm K, editors. Krankheitskosten. Berlin: Robert-Koch-Inst; 2009. (Gesundheitsberichterstattung des Bundes; vol 48). Available from: URL: http://www.rki.de/cln_151/nn_204544/DE/Content/GBE/Gesundheitsberichterstattung/GBEDownloadsT/.html.
Doran CM, Kinchin I. A review of the economic impact of mental illness. Aust Health Rev. 2019;43(1):43–8.
Burhamah W, AlKhayyat A, Oroszlányová M, AlKenane A, Almansouri A, Behbehani M, et al. The psychological burden of the COVID-19 pandemic and associated lockdown measures: experience from 4000 participants. J Affect Disord. 2020;277:977–85.
Cooke JE, Eirich R, Racine N, Madigan S. Prevalence of posttraumatic and general psychological stress during COVID-19: a rapid review and meta-analysis. Psychiatry Res. 2020;292: 113347.
Le K, Nguyen M. The psychological burden of the COVID-19 pandemic severity. Econ Hum Biol. 2021;41: 100979.
Dragioti E, Li H, Tsitsas G, Lee KH, Choi J, Kim J, et al. A large-scale meta-analytic atlas of mental health problems prevalence during the COVID-19 early pandemic. J Med Virol. 2022;94(5):1935–49.
Killgore WDS, Cloonan SA, Taylor EC, Dailey NS. Mental Health during the first weeks of the COVID-19 pandemic in the United States. Front Psychiatry. 2021;12: 561898.
Wu T, Jia X, Shi H, Niu J, Yin X, Xie J, et al. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. 2021;281:91–8.
Robinson E, Sutin AR, Daly M, Jones A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J Affect Disord. 2022;296:567–76.
Bundespsychotherapeutenkammer. BPtK-Studie zu Wartezeiten in der ambulanten psychotherapeutischen Versorgung; 2011. Available from: URL: https://www.bptk.de/wp-content/uploads/2019/01/20110622_BPtK-Studie_Langfassung_Wartezeiten-in-der-Psychotherapie.pdf.
Bundespsychotherapeutenkammer. Ein Jahr nach der Reform der Psychotherapie-Richtlinie – Wartezeiten 2018; 2018. Available from: URL: https://www.bptk.de/wp-content/uploads/2019/01/20180411_bptk_studie_wartezeiten_2018.pdf.
Folkins C, Hersch P, Dahlen D. Waiting time and no-show rate in a community mental health center. Am J Community Psychol. 1980;8(1):121–3.
Grunebaum M, Luber P, Callahan M, Leon AC, Olfson M, Portera L. Predictors of missed appointments for psychiatric consultations in a primary care clinic. Psychiatr Serv. 1996;47(8):848–52.
Brieger P. Psychiatrische Versorgung in Deutschland – ein Überblick. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2019;62(2):121–7.
Seligman ME, Csikszentmihalyi M. Positive psychology. an introduction. Am Psychol. 2000;55(1):5–14.
Fredrickson BL. The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am Psychol. 2001;56(3):218–26.
Fredrickson BL. What good are positive emotions? Rev Gen Psychol. 1998;2(3):300–19.
Schueller SM, Parks AC. The Science of Self-Help. Eur Psychol. 2014;19(2):145–55.
Sin NL, Lyubomirsky S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J Clin Psychol. 2009;65(5):467–87.
Bolier L, Haverman M, Westerhof GJ, Riper H, Smit F, Bohlmeijer E. Positive psychology interventions: a meta-analysis of randomized controlled studies. BMC Public Health. 2013;13: 119.
Carr A, Cullen K, Keeney C, Canning C, Mooney O, Chinseallaigh E, et al. Effectiveness of positive psychology interventions: a systematic review and meta-analysis. J Posit Psychol. 2021;16(6):749–69.
Hendriks T, Schotanus-Dijkstra M, Hassankhan A, de Jong J. The efficacy of multi-component positive psychology interventions: a systematic review and meta-analysis of randomized controlled trials. J Happiness Stud. 2020;21(1):357–90.
Fordyce MW. Development of a program to increase personal happiness. J Couns Psychol. 1977;24(6):511–21.
Müller R, Gertz KJ, Molton IR, Terrill AL, Bombardier CH, Ehde DM, et al. Effects of a tailored positive psychology intervention on well-being and pain in individuals with chronic pain and a physical disability: a feasibility trial. Clin J Pain. 2016;32(1):32–44.
Nikrahan GR, Suarez L, Asgari K, Beach SR, Celano CM, Kalantari M, et al. Positive psychology interventions for patients with heart disease: a preliminary randomized trial. Psychosomatics. 2016;57(4):348–58.
Peters ML, Smeets E, Feijge M, van Breukelen G, Andersson G, Buhrman M, et al. Happy despite Pain: a randomized controlled trial of an 8-Week internet-delivered positive psychology intervention for Enhancing Well-being in patients with chronic pain. Clin J Pain. 2017;33(11):962–75.
Seligman MEP, Rashid T, Parks AC. Positive psychotherapy. Am Psychol. 2006;61(8):774–88.
Chaves C, Lopez-Gomez I, Hervas G, Vazquez C. A comparative study on the efficacy of a positive psychology intervention and a cognitive behavioral therapy for clinical depression. Cogn Ther Res. 2017;41(3):417–33.
Nilges P, Essau C. Die depressions-angst-stress-skalen. Schmerz. 2015;29:649–57.
Lukat J, Margraf J, Lutz R, van der Veld WM, Becker ES. Psychometric properties of the positive Mental Health Scale (PMH-scale). BMC Psychol. 2016;4:8.
Glaesmer H, Hoyer J, Klotsche J, Herzberg PY. Die deutsche Version des life-orientation-tests (LOT-R) zum dispositionellen optimismus und pessimismus. Z für Gesundheitspsychologie. 2008;16(1):26–31.
Hudecek MFC, Blabst N, Morgan B, Lermer E. Eindimensionale Skala zur Messung von Dankbarkeit (GQ-5-G). Zusammenstellung sozialwissenschaftlicher Items und Skalen (ZIS); 2021. https://doi.org/10.6102/zis300.
Glaesmer H, Grande G, Braehler E, Roth M. The german version of the satisfaction with Life Scale (SWLS). Eur J Psychol Assess. 2011;27(2):127–32.
Chen G, Gully SM, Eden D. Validation of a new general self-efficacy scale. Organizational Res Methods. 2001;4(1):62–83.
Chmitorz A, Wenzel M, Stieglitz R-D, Kunzler A, Bagusat C, Helmreich I, et al. Population-based validation of a german version of the brief resilience scale. PLoS ONE. 2018;13(2): e0192761.
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing. 2021. https://www.R-project.org/.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Erlbaum; 1988.
Aldwin CM, Spiro A, Levenson MR, Bossé R. Longitudinal findings from the normative aging study: 1. Does mental health change with age? Psychol Aging. 1989;4(3):295–306.
Lehtinen V, Sohlman B, Kovess-Masfety V. Level of positive mental health in the European Union: results from the Eurobarometer 2002 survey. Clin Pract Epidemiol Ment Health. 2005;1: 9.
Meevissen YMC, Peters ML, Alberts HJEM. Become more optimistic by imagining a best possible self: effects of a two week intervention. J Behav Ther Exp Psychiatry. 2011;42(3):371–8.
Peters ML, Flink IK, Boersma K, Linton SJ. Manipulating optimism: can imagining a best possible self be used to increase positive future expectancies? J Posit Psychol. 2010;5(3):204–11.
Peters ML, Meevissen YMC, Hanssen MM. Specificity of the best possible self intervention for increasing optimism: comparison with a gratitude intervention. Ter Psicol. 2013;31(1):93–100.
Carrillo A, Rubio-Aparicio M, Molinari G, Enrique Á, Sánchez-Meca J, Baños RM. Effects of the best possible self intervention: a systematic review and meta-analysis. PLoS ONE. 2019;14(9): e0222386.
Heekerens JB, Eid M. Inducing positive affect and positive future expectations using the best-possible-self intervention: a systematic review and meta-analysis. J Posit Psychol. 2021;16(3):322–47.
Miller DL, Manne SL, Taylor K, Keates J, Dougherty J. Psychological distress and well-being in advanced cancer: the effects of optimism and coping. J Clin Psychol Med Settings. 1996;3(2):115–30.
Rasmussen HN, Scheier MF, Greenhouse JB. Optimism and physical health: a meta-analytic review. Ann Behav Med. 2009;37(3):239–56.
Carver CS, Gaines JG. Optimism, pessimism, and postpartum depression. Cogn Ther Res. 1987;11(4):449–62.
Hirsch JK, Wolford K, LaLonde SM, Brunk L, Morris AP. Dispositional optimism as a moderator of the relationship between negative life events and suicide ideation and attempts. Cogn Ther Res. 2007;31(4):533–46.
Ang WHD, Lau ST, Cheng LJ, Chew HSJ, Tan JH, Shorey S, et al. Effectiveness of resilience interventions for higher education students: a meta-analysis and metaregression. J Educ Psychol. 2022;114(7):1670–94.
Koay S-H, Ng A-T, Tham S-K, Tan C-S. Gratitude intervention on Instagram: an experimental study. Psychol Stud. 2020;65(2):168–73.
Lambert L, Passmore H-A, Joshanloo M. A positive psychology intervention program in a culturally-diverse University: boosting happiness and reducing fear. J Happiness Stud. 2019;20(4):1141–62.
Ouweneel E, Le Blanc PM, Schaufeli WB. Do-it‐yourself. Career Dev Int. 2013;18(2):173–95.
Krohne HW, Egloff B, Kohlmann CW, Tausch A. Untersuchungen mit einer deutschen version der positive and negative affect schedule (PANAS). In Diagnostica. 1996;42:139–56.
Acknowledgements
We want to thank Helen Copeland-Vollrath for proofreading the manuscript. We also want to thank Inga Schecker, Lara Steinfeldt, Lucia Ueckert and Lisa Weiß for being part of the data collection. We acknowledge support by the Open Access Publication Funds of the Ruhr-Universität Bochum.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
“LN and CvG: designed and executed the study, conducted the data analyses, and wrote the paper. XCZ: collaborated in the analyses of the data and edited part of the results. JM: collaborated in the editing of the final manuscript. CT: designed the study, collaborated in the writing and editing of the manuscript. All authors approved the final version of the manuscript for submission.“
Corresponding author
Ethics declarations
Ethics approval and consent to participate
After being informed about the procedure of the study, all participants gave written informed consent. This study was approved by the Local Ethics Committee for Psychological Studies of Ruhr-University Bochum. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Niemann, L., von Gruner, C., Zhang, X.C. et al. Positive Emotions Training (PoET) as an online intervention to improve mental health: a feasibility study. BMC Public Health 23, 1543 (2023). https://doi.org/10.1186/s12889-023-16424-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16424-x