
Abstract
Background
As the phenomenon of ageing continues to intensify, home and community-based services (HCBSs) have been increasingly important in China. However, the association between HCBSs utilization and depressive symptoms in older adults in China is unclear. Consequently, this study aimed to examine the association between HCBSs utilization and depressive symptoms in Chinese older adults.
Methods
This study included 7,787 older adults (≥ 60 years old) who were recruited within the framework of the 2018 China Health and Retirement Longitudinal Study (CHARLS). Depressive symptoms were assessed using the 10-item Center for Epidemiological Studies Depression Scale (CES-D-10). HCBSs utilization was assessed via the question, “What kind of HCBSs were being utilized in their community?”. Data were analyzed using binary logistic regression models and generalized hierarchical linear models (GHLM).
Results
Of the 7,787 participants, 20.0% (n = 1,556) reported that they utilized HCBSs, and 36.7% (n = 2,859) were evaluated that they had depressive symptoms. After adjusting for individual- and province-level covariates, the HCBSs utilization was found to be associated with depressive symptoms (OR = 1.180, 95% CI: 1.035–1.346, p < 0.05). Additionally, the depressive symptoms were significantly associated with gender, residence, educational level, marital status, number of chronic diseases, self-rated health (SRH), smoking, and provincial Gross Domestic Product (GDP) per capita.
Conclusions
This study found HCBSs utilization might be a protective factor against depressive symptoms in Chinese older adults. It is of utmost significance for the government to provide targeted HCBSs at the community level to address the unmet care needs of older adults, which can reduce the occurrence of negative emotions, consequently contributing to less severe depressive symptoms.
Similar content being viewed by others


Introduction
By the end of 2020, the number of people aged 60 years and over had surged to 264.02 million in China, which accounted for 18.70% of the overall population [1]. As the phenomenon of aging continues to intensify, the mental health of older adults, especially depression, requires more attention. Depression, one of the leading causes of the global disease burden, is a common mental health problem worldwide [2]. The World Health Organization (WHO) suggested that there is an increased incidence of depression in older adults [3], with over 10% of global older adults having experienced depressive symptoms [4]. Similarly, the prevalence rate of depressive symptoms in older adults is the highest among the general population in China [5].
In tandem with the aging population, China is also undergoing a massive social transition and changes in family structure [6, 7]. These shifts challenge the conventional family-based care arrangement for older adults, resulting in the decline of older adults’ mental health due to childlessness and an “empty nest” [8]. In addition, owning to financial burdens and dwelling preference, the institutional endowment resources cannot meet the elderly care needs of most older adults in China anymore [9]. Hence, the huge demand for home and community-based services (HCBSs) among older adults in China is evident and urgent.
HCBSs originated in Western countries and have reached a relatively high level of maturity [10, 11]. In contrast, HCBSs in China are still evolving, encompassing a variety of non-institutional services for older adults living in the community, which is provided by the government, community, and social organizations [9, 12]. HCBSs in China are primarily in line with some Western countries, except for the absence of church services and religious services, which include mainly health care services (e.g., in-home medical care services, therapy care services), social support services (e.g., entertainment, emergency call services), daily care services (e.g., meal delivery, housekeeping) [13, 14].
The positive effects of HCBSs on health status in older adults have been acknowledged, such as enhancing life satisfaction [15], promoting cognitive function [16], and reducing the risk of depressive symptoms [17]. Depressive symptoms are a prevalent and serious mental health issue that deserve attention [2]. However, as mentioned in the previous study’s limitations [17], only the relationship between depressive symptoms and HCBSs provision based on the Chinese Longitudinal Healthy Longevity Survey (CLHLS), rather than the utilization of HCBSs, was examined, which may have led to a misjudgment of the role of HCBSs on older adults’ depressive symptoms. Moreover, the health status of older adults was confirmed to be a hierarchical structure, meaning that individuals were nested within specific provinces [18]. Thus, individual- and province-level factors would affect the health status. However, the previous studies conducted a regression analysis to examine the effect of HCBSs on older adults’ health only adjusting individual-level covariates [15,16,17]. In contrast, the province-level covariates might bias these estimations.
Therefore, to fill these research gaps, the current study assessed the HCBSs utilization and depressive symptoms in Chinese older adults, and examined their relationship with generalized hierarchical linear models (GHLM) based on the 2018 China Health and Retirement Longitudinal Study (CHARLS). The findings of this study could shed light on the future policy implementation on the development of HCBSs in China.
Methods
Study participants
Data were obtained from the fourth wave of survey data from the CHARLS, which is a survey of middle-aged and older adults in China based on a sample of households with members aged 45 years or above. With the purpose of establishing a high-quality public database, it contained a wide range of information, ranging from socioeconomic status to health conditions, needed for scientific research on middle-aged and older adults [19, 20]. To ensure sample representative, the survey followed strict randomization procedures and used a multi-stage sampling method. When sampling county and rural administrative units, a Probability-Proportional-to-Size (PPS) sampling method was adopted [21].
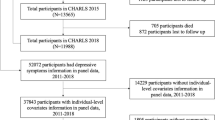
In this study, participants were excluded if they (1) were younger than 60 years old, or lacked data regarding (2) utilization of HCBSs, (3) 10-item Center for Epidemiological Studies Depression (CES-D-10), or (4) values in the main variables. A total of 19,816 participants completed the CHARLS in 2018. Crucially, 8,762 participants aged lower than 60 years, 35 participants lacking utilization of HCBSs data, 2,668 participants lacking CES-D-10 data, 530 participants with Memory-Related Disease or Emotional Problems, and 34 participants lacking values in main variables were excluded. Accordingly, the final study sample consisted of 7,787 participants.
Measurement
Dependent variable
Depressive symptoms were assessed using the CES-D-10 [22]. Ten of 20 items from the original version of the scale were grouped to the shortened CES-D-10 scale by its internal correlations [23]. This scale was widely used in older adults and showed high reliability and validity among Chinese older adults [24]. The CES-D-10 was comprised of ten questions about depression, and the answers included four options: (1) rarely, (2) some days (1–2 days per week), (3) occasionally (3–4 days per week), and (4) most of the time (5–7 days per week). Among the ten questions, eight questions were negative statements, and two questions were positive statements. The answers were recorded as 0 (rarely) to 3 (most of the time) for the negative questions and were recorded as 3 (rarely) to 0 (most of the time) for the positive questions. The total score ranged from 0 to 30 points. A score ≥ 10 in the CES-D-10 was considered to indicate depressive symptoms, as validated by previous studies [23].
Independent variable
HCBSs utilization was measured by asking participants, “Have you ever received the following home and community care services?” The response options included: (a) day care centers, nursing homes, senior dining tables, etc.; (b) regular physical examinations; (c) on-site visits; (d) family beds; (e) community nursing; (f) health management; (g) entertainment. If participants used one or more HCBS, they were classified as HCBSs utilization group, otherwise they were classified as HCBSs non-utilization group.
Covariates
Covariates were considered at individual- and province-levels [25,26,27,28]. Individual-level covariates included sociodemographic characteristics, health status, and lifestyle. Sociodemographic characteristics included age, gender, marital status, educational level, residence, income, and health insurance; health status included the number of chronic diseases and self-rated health (SRH); lifestyle factors included smoking, drinking, and exercising. Further, the province-level covariates included 2018 provincial Gross Domestic Product (GDP) per capita and Number of beds in medical institutions per 10,000 persons, reflecting economic and medical resources respectively.
Statistical analysis
Descriptive statistics were used to analyze characteristics of the study participants. Binary logistic regression was used to compare depressive symptoms risk across groups based on the categorical variables. GHLM were constructed using mixed model procedures, given that the data had a hierarchical structure composed of individuals (Level 1) nested within provinces (Level 2). These models not only estimated fixed effects of individual- and province-level factors on depressive symptoms, but also tested for the variance components for the random intercepts, representing the differences in older adults’ depressive symptoms at the province-level. Data were analyzed using SPSS version 26.0. The level of significance was set at p < 0.05.
Results
Table 1 presents the basic characteristics of the total sample included in this study. The final sample included 7,787 participants from 28 provinces, representing approximately 264 million Chinese residents aged ≥ 60 years. Of the 7,787 participants, 20.0% (n = 1,556) utilized HCBSs, and 36.7% (n = 2,859) with depressive symptoms. A majority of the respondents were male (n = 4,034, 51.8%), aged 60–69 (n = 5,074, 65.2%), partnered (n = 6,378, 81.9%), with an educational level of elementary school (n = 3,580, 46.0%), living in rural areas (n = 5,627, 72.3%), without income (n = 6,651, 85.4%), and without health insurance (n = 7,584, 97.4%). Additionally, a significant number of the respondents did not drink (n = 5,127, 65.8%) and smoke (n = 5,582, 71.7%), exercised (n = 7,041, 90.4%), had fair SRH (n = 3,897, 50.1%), and had three or more chronic diseases (n = 3,106, 39.9%). Most of the participants lived in the provinces with the third quartile of GDP per capita (n = 2,396, 30.8%) and provinces with the second quartile of Number of beds in medical institutions per 10,000 persons (n = 2,221, 28.5%).
Further, we analyzed the odds ratio (OR) for older adults with depressive symptoms (vs. non-depressive symptoms) for each predictor using binary logistic regression. The analysis showed that older adults who did not utilize HCBSs (OR = 1.164, 95% CI: 1.035–1.308, p = 0.011) had a greater risk of depressive symptoms than those who utilized HCBSs. In addition, older adults who were female, single, illiterate, living in rural areas, without income, with health insurance, with chronic diseases, with worse SRH, and who did not smoke, drink, or exercise had greater risk of depressive symptoms. For the province-level characteristics, older adults living in provinces with the fourth quartile of GDP per capita were less likely to suffer from depressive symptoms, and provinces with fourth quartile of Number of beds in medical institutions per 10,000 persons were more likely to suffer from depressive symptoms.
Table 2 summarizes the relationship between HCBSs utilization and depressive symptoms. Further, Model 1 identifies significant variations between provinces in the empty model (i.e., model without explanatory covariates included). The HCBSs utilization was significantly associated with depressive symptoms (OR = 1.149, 95% CI: 1.019–1.296, p < 0.05) in Model 2, which included HCBSs utilization as the only predictor. In Model 3, utilization of HCBSs was significantly associated with depressive symptoms (OR = 1.186, 95% CI: 1.040–1.352, p < 0.05) after controlling for other individual-level covariates. In Model 4, depressive symptoms were greatly associated with HCBSs utilization (OR = 1.180, 95% CI: 1.035–1.346, p < 0.05) after adjusting for individual- and province-level variables. Older adults utilizing HCBSs were more likely to have a lower risk of depressive symptoms. Several covariates (i.e., gender, marital status, educational level, residence, number of chronic diseases, SRH, and smoking) were associated with depressive symptoms. In addition, provincial GDP per capita emerged as significant predictors of depressive symptoms.
Discussion
To the best of our knowledge, this is the first study to explore the association between HCBSs utilization and depressive symptoms in Chinese older adults using nationally representative survey data with GHLM. Moreover, this study assessed the association between individual- and provincial-level covariates and depressive symptoms in older adults. Results showed that older adults who utilized HCBSs were less likely to suffer from depressive symptoms, even after adjusting for individual- and province-level covariates.
In the early 1980s, HCBSs provision systems were first established in the United States and Denmark to match the demands of older adults [10, 11]. However, the implementation of HCBSs in Western countries occurred earlier than in China. In response to the aging population, China did not strongly encourage the implementation of HCBSs to protect the health of older adults until 2008. Due to the implementation and rapid promotion of national policies, from 2008 to 2018, the provision rate of HCBSs has increased dramatically from 26.1 to 62.0% in China [29]. However, the utilization rate of HCBSs was just 20.0% in 2018, which was significantly lower than the provision rate of HCBSs in China. This gap may be due to the provision of HCBSs that cannot precisely match the demand of HCBSs among Chinese older adults.
The prevalence of depressive symptoms in older adults aged 60 years and above was 36.7% in 2018, which was significantly higher than that in 2015 [25], despite the same measurement and cut-off points being used. In traditional Chinese society, positive family relations are beneficial to mental health and act as a social security system for older adults [30]. However, rapid industrialization and urbanization have shifted these traditional arrangements. Nowadays, older adults are less likely to live with younger generations and interact with them. This has direct implications on access to social care and financial security and even affects the mental health of older adults [31, 32].
Previous studies on depressive symptoms in older adults focused only on individual factors [27, 33, 34], leading to scientific bias in the research. In this study, GHLM was used to comprehensively consider the influence of individual- and province-level factors, making the results more reliable. The present study found that individual characteristics, including gender, marital status, educational level, residence, number of chronic diseases, SRH, and smoking might be associated with depressive symptoms, which is in line with previous research [35,36,37,38,39,40,41]. Notably, the provincial factor (GDP per capita) was also found to be an important factor being associated with depressive symptoms. Older adults living in provinces with higher economic levels were less likely to suffer from depressive symptoms. This is mainly due to good financial status, which could guarantee a certain amount of public expenditure to build a superior older adults’ care service system to reduce loneliness and depressive symptoms [42]. However, this study found no significant association between individual factors including age, income, health insurance, drinking, exercising, and provincial factor (Number of beds in medical institutions per 10,000 persons) and depressive symptoms.
Our findings supported the hypothesis that HCBSs utilization was associated with depressive symptoms in the aging population in China. Firstly, the family’s ability to provide older adults’ care has been reduced following demographic shifts and socioeconomic changes [43], and older adults may feel a sense of loneliness or disappointment if they fail to receive care from their children [44]. However, the daily care services of HCBSs, such as day care centers, nursing homes, senior dining tables, etc., could be an alternative to accompanying children, reduce feelings of loneliness and marginalization, and prevent older adults from depressive symptoms. Secondly, HCBSs included not only daily care services, but also health care services, such as regular physical examinations, onsite visits, family beds, community nursing, and health management, which are significant approaches to promote somatic symptoms and alleviate depressive symptoms in older adults to a certain extent [45]. Thirdly, some entertainment activities organized by the volunteers or self-organized by the older adults through community spaces and equipment are also an important part of HCBSs and could provide an opportunity to interact with others and reduce negative affect among older adults who live alone at home [46]. Thus, providing targeted HCBSs at the community level could meet elderly care needs and may reduce the incidence of adverse emotions and consequently lower the risk of depressive symptoms.
This study aims to enhance our understanding of the role of HCBSs in benefiting mental health. To ease the depressive symptoms in community-dwelling older adults, it is expected that more financial and human resources will be allocated to extend the coverage of HCBSs further and make them more accessible to older adults in China, especially to those who are female, single, with chronic diseases, with worse SRH, not smoking, and living in a rural and the area with the lag of economic development. What’s more, policymakers should not only strive to improve the quantity of HCBSs but also lay more emphasis on their quality. In particular, HCBSs should be provided pointedly in terms of the preferences of distinct types of older adult to match the provision and demand of HCBSs, thus truly improving the utilization of HCBSs.
Limitation
There are also some limitations in this study. First, the data regarding HCBSs utilization was not included in the CHARLS until 2018, so we can only conduct the cross-sectional study. Hence the causal relationship between the utilization of HCBSs and depressive symptoms was not examined in this study. Prospective studies should further investigate the relationship as long as longitudinal data is available. Second, the associations between specific types of HCBSs, such as daily care, health care, and in Chinese older adults were not measured in this study. Further research is needed to examine the associations between specific types of HCBS and depressive symptoms. Third, CHARLS might exist some missing cases regarding depressive symptoms of the participants, resulting in selection bias. In the future, the surveys we conduct should take this issue fully into account.
Conclusions
This study shows that depressive symptoms were associated with HCBSs utilization in China applying GHLM to partly address potential selection bias issues. Better depressive symptoms are more prevalent among Chinese older adults with HCBSs utilization. The findings of this study provide a better understanding about the association between HCBSs and depressive symptoms in Chinese older adults and imply that government should strive to extend HCBSs coverage and promote the quality of these services to match the demand of HCBSs, thus improving older adults’ mental health.
Data Availability
All data used in this study were stored at http://charls.pku.edu.cn/ and available upon request.
Abbreviations
- CES-D-10:
-
10-item Center for Epidemiological Studies Depression Scale
- CHARLS:
-
China Health and Retirement Longitudinal Study
- GDP:
-
Gross Domestic Product
- GHLM:
-
Generalized Hierarchical Linear Models
- HCBSs:
-
Home and Community-Based Services
- OR:
-
Odds Ratio
- PPS:
-
Probability-Proportional-to-Size
- SRH:
-
Self-Rated Health
References
National Bureau of Statistics: Annual Data. 2020. Available online: https://data.stats.gov.cn/easyquery.htm?cn=C01
Whiteford HA, Ferrari AJ, Degenhardt L, Feigin V, Vos T. The global burden of mental, neurological and substance use disorders: an analysis from the global burden of Disease Study 2010. PLoS ONE. 2015;10(2):e0116820.
Organization WH. Depression and Other Common Mental Disorders: Global Health Estimates. 2017.
Beekman AT, Copeland JR, Prince MJ. Review of community prevalence of depression in later life. Br J Psychiatry. 1999;174:307–11.
Li D, Zhang DJ, Shao JJ, Qi XD, Tian L. A meta-analysis of the prevalence of depressive symptoms in chinese older adults. Arch Gerontol Geriatr. 2014;58(1):1–9.
Yang W, Wu B, Tan SY, Li B, Lou VWQ, Chen ZA, Chen X, Fletcher JR, Carrino L, Hu B, et al. Understanding Health and Social Challenges for Aging and Long-Term Care in China. Res Aging. 2021;43(3–4):127–35.
Zhu Y, Österle A. China’s policy experimentation on long-term care insurance: implications for access. Int J Health Plann Manage. 2019;34(4):e1661–74.
Kalache A. Ageing in developing countries: are we meeting the challenge? Health Policy Plann. 1986;1(2):171–3.
Xu Q, Chow JC. Exploring the community-based service delivery model: Elderly care in China. Int Social Work. 2011;54(3):374–87.
Birnbaum H, Burke R, Swearingen C, Dunlop B. Implementing Community-Based Long-TermCare: experience of New York’s Long Term Home Health Care Program. Gerontologist. 1984;24(4):380–6.
Stuart M, Weinrich M. Home-and community-based long-term care: Lessons from Denmark. Gerontologist. 2001;41(4):474–80.
Peng C, Burr JA, Kim K, Lu N. Home and community-based service utilization among older adults in urban China: the role of social capital. J Gerontol Soc Work. 2020;63(8):790–806.
Lehnert T, Günther O, Hajek A, Riedel-Heller S, König H. Preferences for home-and community-based long-term care services in Germany: a discrete choice experiment. Eur J Health Econ. 2018;19:1213–23.
Lam BT, Cervantes AR, Lee WK. Late-life depression, social support, instrumental activities of daily living, and utilization of in-home and community-based services in older adults. J Hum Behav social Environ. 2014;24(4):499–512.
Chen Q, Amano T, Park S, Kim B. Home and community-based services and life satisfaction among homebound and poor older adults. J Gerontol Soc Work. 2019;62(7):708–27.
Yu Y, Yuan C, Zhang Q, Song C, Cui S, Ye J, Zhang X, Chen C. Longitudinal association between home and community-based services provision and cognitive function in chinese older adults: evidence from the chinese longitudinal healthy longevity survey. Health Soc Care Community. 2021;29(6):e288–98.
Yu Y, Zhang J, Song C, Petrovic M, Pei X, Zhang WH. Perceived availability of home- and community-based services and self-reported depression among chinese older adults: a cross-sectional study. Health Soc Care Community. 2022;30(5):e2827–37.
Nie X, Li Y, Li C, Wu J, Li L. The association between health literacy and self-rated health among residents of China aged 15–69 years. Am J Prev Med. 2021;60(4):569–78.
Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China health and retirement longitudinal study (CHARLS). Int J Epidemiol. 2014;43(1):61–8.
Lei X, Sun X, Strauss J, Zhang P, Zhao Y. Depressive symptoms and SES among the mid-aged and elderly in China: evidence from the China Health and Retirement Longitudinal Study national baseline. Soc Sci Med. 2014;120:224–32.
Feng XL, Pang M, Beard J. Health system strengthening and hypertension awareness, treatment and control: data from the China Health and Retirement Longitudinal Study. Bull World Health Organ. 2013;92:29–41.
Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401.
Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D. American journal of preventive medicine 1994, 10(2):77–84.
Chang S-H, Chen M-C, Chien N-H, Lin T-Y, Chang Y-Y. Gender differences in the relationship of lifestyle and depressive symptoms among taiwanese older people. Collegian. 2016;23(3):249–55.
Liao S, Zhou Y, Liu Y, Wang R. Variety, frequency, and type of internet use and its association with risk of depression in middle-and older-aged Chinese: a cross-sectional study. J Affect Disord. 2020;273:280–90.
Wang R, Chen Z, Zhou Y, Shen L, Zhang Z, Wu X. Melancholy or mahjong? Diversity, frequency, type, and rural-urban divide of social participation and depression in middle-and old-aged Chinese: a fixed-effects analysis. Soc Sci Med. 2019;238:112518.
Feng Z, Li Q, Zhou L, Chen Z, Yin W. The relationship between depressive symptoms and activity of daily living disability among the elderly: results from the China Health and Retirement Longitudinal Study (CHARLS). Public Health. 2021;198:75–81.
Liu H, Fan X, Luo H, Zhou Z, Shen C, Hu N, Zhai X. Comparison of depressive symptoms and its influencing factors among the elderly in urban and rural areas: evidence from the China Health and Retirement Longitudinal Study (CHARLS). Int J Environ Res Public Health. 2021;18(8):3886.
Xu T, Zhao Q, Chen Y, Lu Y, Huang Y, Zhai Q, Zhu T, Chen C. Researches on the spatial and temporal differences in the Provision of Home and Community - based pension services in China based on CLHLS (2008–2018) Longitudinal Data. Chin Health Service Manage. 2022;39(03):170–2. (in Chinnese).
Lendon JP. The measurement, life course patterns, and outcomes of intergenerational ambivalence among parent-adult child dyads. University of Southern California; 2012.
Lim LL, Chang W, Yu X, Chiu H, Chong MY, Kua EH. Depression in Chinese elderly populations. Asia-Pacific Psychiatry. 2011;3(2):46–53.
Mjelde-Mossey LA, Chi I, Lou VW. Relationship between adherence to tradition and depression in chinese elders in China. Aging Ment Health. 2006;10(1):19–26.
Shen K, Zhang B, Feng Q. Association between tea consumption and depressive symptom among chinese older adults. BMC Geriatr. 2019;19:1–8.
Tan J-Y, Zeng Q-L, Ni M, Zhang Y-X, Qiu T. Association among calf circumference, physical performance, and depression in the elderly chinese population: a cross-sectional study. BMC Psychiatry. 2022;22(1):1–9.
Thompson AH, Bland RC. Gender similarities in somatic depression and in DSM depression secondary symptom profiles within the context of severity and bereavement. J Affect Disord. 2018;227:770–6.
Hossain B, Yadav PK, Nagargoje VP, Vinod Joseph K. Association between physical limitations and depressive symptoms among indian elderly: marital status as a moderator. BMC Psychiatry. 2021;21(1):1–11.
Taple BJ, Chapman R, Schalet BD, Brower R, Griffith JW. The impact of education on depression assessment: differential item functioning analysis. Assessment. 2022;29(2):272–84.
Li LW, Liu J, Xu H, Zhang Z. Understanding rural–urban differences in depressive symptoms among older adults in China. J Aging Health. 2016;28(2):341–62.
Jiang C-h, Zhu F, Qin T-t. Relationships between chronic diseases and depression among middle-aged and elderly people in China: a prospective study from CHARLS. Curr Med Sci. 2020;40(5):858–70.
Peleg S, Nudelman G. Associations between self-rated health and depressive symptoms among older adults: does age matter? Soc Sci Med. 2021;280:114024.
Weinberger AH, Kashan RS, Shpigel DM, Esan H, Taha F, Lee CJ, Funk AP, Goodwin RD. Depression and cigarette smoking behavior: a critical review of population-based studies. Am J Drug Alcohol Abus. 2017;43(4):416–31.
Feng Z, Jones K, Wang WW. An exploratory discrete-time multilevel analysis of the effect of social support on the survival of elderly people in China. Soc Sci Med. 2015;130:181–9.
Feng Z, Liu C, Guan X, Mor V. China’s rapidly aging population creates policy challenges in shaping a viable long-term care system. Health Aff. 2012;31(12):2764–73.
Wang D. Intergenerational transmission of family property and family management in urban China. China Q. 2010;204:960–79.
Yang L, Wang L, Di X, Dai X. Utilisation of community care services and self-rated health among elderly population in China: a survey-based analysis with propensity score matching method. BMC Public Health. 2021;21:1–11.
Zhang Y, Yeager VA, Hou S. The impact of community-based supports and services on quality of life among the elderly in China: a longitudinal study. J Appl Gerontol. 2018;37(10):1244–69.
Acknowledgements
The authors thank the CHARLS team for their hard work and unselfish sharing of survey data. We also acknowledge Editage editorial team for their English editing.
Funding
This work was supported by National Natural Science Foundation of China [72274141], Zhejiang Provincial Natural Science Foundation [LY22G030006], Philosophy and Social Science Project of Zhejiang Province, China [22NDJC104YB], 2023 Joint Project of Science and Technology Department of National Administration of Traditional Chinese Medicine and Zhejiang Administration of Traditional Chinese Medicine [GZY-ZJ-KJ-23084], and Zhejiang Provincial Science and Technology Innovation Program (New Young Talent Program) for College Students [2022R413B053].
Author information
Authors and Affiliations
Contributions
Chun Chen, Xiangyang Zhang, Tingke Xu and Zishuo Huang conceived and designed the study. Tingke Xu and Zishuo Huang participated in acquisition of the data. Tingke Xu and Chun Chen contributed to data analysis. Tingke Xu and Zishuo Huang wrote the original draft. Tingke Xu took charge of the submission. Chun Chen, Xiangyang Zhang, Tingke Xu, Zishuo Huang, Yucheng Huang, Shanshan Wang, Xinxin Zhang, Yaqi Hu, Yue Zhu, Dayi Cheng, and Yating Fu substantively revised the manuscript. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The current study is a secondary analysis of public data of CHARLS. The ethical review committee of Peking University approved the conduct of CHARLS (Code of the ethical approval: IRB00001052-11015) and informed consents are signed by participants before their participation.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xu, T., Huang, Z., Huang, Y. et al. Association between home and community-based services and depressive symptoms in Chinese older adults: a multilevel analysis. BMC Public Health 23, 1406 (2023). https://doi.org/10.1186/s12889-023-16008-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16008-9