
Abstract
Background
Depression and sarcopenia are common diseases in the elderly population. However, the association between them is controversial. Based on the Chinese Longitudinal Healthy Longevity Survey (CLHLS) database, a cross-sectional study was conducted to explore the relationship of calf circumference and physical performance with depression.
Methods
From the 8th wave of CLHLS conducted in 2018, data on calf circumference, physical performance, depressive symptoms, and demographic, socioeconomic, and health-related characteristics were collected. Multiple logistic regression was conducted to explore the impact of calf circumference, physical performance and their combination on depressive symptoms.
Results
We enrolled a total of 12,227 participants aged 83.4 ± 11.0 years, including 5689 (46.5%) men and 6538 (53.5%) women. Patients with depression were more likely to have low calf circumference (2274 [68.2%] vs. 5406 [60.8%], p<0.001) and poor physical performance (3[0, 6] vs. 1[0, 4], p<0.001). A significant multiplicative interaction was found between calf circumference and physical performance in their effect on depression. After adjusting for confounding factors, multiple logistic regression showed that a significant inverse correlation persisted between physical performance and depressive symptoms in normal (odds ratio [OR] = 1.20, 95% confidence interval [CI]: 1.15–1.26, p<0.001) and low (OR = 1.14, 95% CI: 1.11–1.18, p<0.001) calf circumference group, while the association between calf circumference and depression disappeared. Participants with low calf circumference and poor physical performance were 2.21 times more likely to have depression than those with normal calf circumference and physical performance. All results were found to be robust in sensitivity analyses.
Conclusions
Physical performance was significantly associated with depression in the elderly Chinese population. Attention should be paid to assess depressive symptoms in patients with poor physical performance.
Similar content being viewed by others


Background
Depression, the most common type of mood disorder, is characterized by significant and persisting sadness [1]. According to a statistical analysis by the World Health Organization, depression is the leading cause of disability [2]. Depressive symptoms are common in later life, affecting approximately 10% of the elderly population [3].
Sarcopenia is characterized by age-related loss of skeletal muscle mass and function [4]. Its prevalence ranges from 5.5 to 25.7% in Asian countries [4] and may be underestimated in the elderly population [5]. The pathophysiology of sarcopenia includes oxidative stress, chronic inflammation, hormonal deficiency, physical inactivity, and malnutrition [6], which may also be involved in the pathogenesis of depression [7,8,9,10,11].
Exercise can improve mood in patients with depression and strengthen muscles, thus improving physical performance. In a randomized controlled trial, exercise intervention using a physical activity program positively affected the depressive status. Moreover, muscles are the largest group of tissues involved in exercise and endocrine metabolism. Therefore, many studies have investigated the relationship between sarcopenia and depression [12,13,14,15,16,17]. However, none of the studies considered a large sample size of the elderly Chinese population. Therefore, the aim of the present study was to investigate the association between calf circumference, physical performance and their combination on depression in the elderly Chinese population utilizing the Chinese Longitudinal Healthy Longevity Survey (CLHLS) database, a nationally representative sample.
Methods
Study population
Data from the 8th wave of the CLHLS conducted in 2018/2019 were utilized. Of all interviews, 82.1% were conducted in half of the randomly selected counties and cities from 22 provinces except the eight longevity areas, whereas 17.9% were conducted in the eight longevity areas and were relatively more in-depth [18]. The CLHLS attempted to interview all centenarians who voluntarily agreed to participate in the study in the sampled counties and cities. They adopted a targeted random-sample design to ensure representativeness. In the sampled counties, for every 3 centenarians, 4 participants aged 80–89, 4 participants aged 90–99, and 5 participants aged 65–79 were recruited based on predesignated age and sex. If there was no such matched person, a person will be recruited in neighboring county with same predesignated age and sex. In CLHLS, the trained staff had collected data from the elderly Chinese population through face-to-face interviews. The information included demographic, socioeconomic, lifestyle-related, and health-related characteristics. Detailed information of the CLHLS has been previously reported [19, 20].
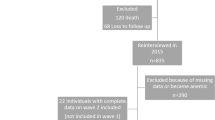
We collected information on calf circumference and physical performance from the 2018 wave of the CLHLS and assessed depressive symptoms based on the Center for Epidemiologic Studies Depression Scale (CES-D). After excluding 3560 individuals with missing data on calf circumference or CES-D and 87 individuals aged below 65 years, a total of 12,227 participants were included in this study (Fig. 1).

Flowchart of the selection of study population from participants of the Chinese Longitudinal Healthy Longevity Survey
Measurements
The questionnaire in the 2018 wave of the CLHLS included calf circumference measured in cm. According to previous studies and the Asian Working Group for Sarcopenia (AWGS) 2019 consensus [4], calf circumference was used as a measure of muscle mass. The muscle mass is considered low when the calf circumference<34 cm in men and<33 cm in women [4, 21,22,23].
The questionnaire in the 2018 wave of the CLHLS assessed physical performance on a four-item scale. Muscle strength was assessed using the question “Are you able to lift 5 kg of weight?” Walking ability was assessed using the question “Are you able to walk 1 km?” The strength of the lower extremities was assessed using the question “Are you able to crouch and stand three times?” Finally, core strength was assessed using the question “How do you stand up after sitting in a chair?” The respondents were requested to choose from responses “without problem,” “with problem,” and “not able to,” which were assigned scores of 0, 1, and 2 points, respectively. The total score ranged from 0 to 8 points. A higher score indicated low physical performance. The internal consistency reliability using Cronbach’s α coefficient was 0.87. The principal component analysis generated one factor with eigenvalues ≥1, explaining 72% of the total variance. The 10-item CES-D-10 was used to assess depressive symptoms, as reported previously [24]. The options were “rarely,” “some days,” “occasionally,” and “most of the time,” which were assigned scores of 0, 1, 2, and 3 points, respectively. There were two positive questions: “Do you feel as happy as you did when you were young?” and “Are you full of hope for the future?” The results of these questions were reversely coded before summation. The total score ranged from 0 to 30 points. A higher score indicated greater severity of depressive symptoms. A score ≥ 10 in the CES-D-10 was considered to indicate depression, as validated by previous studies [25].
Potential confounding factors
The accuracy of results was improved by adjusting for confounding factors, including demographic characteristics (age and sex), socioeconomic characteristics (residence, education, marital status, and retirement status), lifestyle- and health-related behaviors (smoking status, drinking status, activities of daily living [ADL]), social and leisure activity index, travel in the past two years, regular dietary intake of vegetables/fruits/meat/fish/milk products/food made from beans/eggs/nuts, regular tea drinking, and exercise), and health status (body mass index [BMI], cognitive function, and medical history).
The educational level was dichotomized according to the number of years of schooling (0 and ≥ 1 year). ADL ability was assessed on an eight-item scale. ADL disability was defined as the need for an assistant to perform one or more of the five activities (bathing, dressing, toileting, indoor transferring, and feeding) or being incontinent. The social and leisure activity index was calculated using questions on gardening, tai chi chuan, square dancing, reading, raising animals/pets, playing mah-jongg/cards, watching television/listening to the radio, and participating in social activities. The options were “almost every day,” “sometimes,” and “never,” which were assigned scores of 1, 2, and 3 points, respectively. The total score ranged from 8 to 24 points. A higher score indicated lack of social and leisurely activities.
The Chinese version of the 30-point Mini-Mental State Examination (MMSE) was used for cognitive function assessment. Cognitive impairment was defined as a total score < 24 on MMSE [19]. Medical history included a history of diabetes, heart disease, stroke, cancer.
Statistical analysis
The data were statistically analyzed using the chi-square test, Student’s t test, or Mann–Whitney U test, as appropriate. Multiple imputations were used to fill in missing variables. No significant difference in baseline data was found before and after multiple imputations (data not shown). Multiple logistic regression was used to calculate the odds ratio (OR) of depressive symptoms for calf circumference and physical performance. In the multiplicative interaction analysis, low calf circumference, physical performance, and their product terms were included in regression analysis to investigate multiplicative interaction. In the additive interaction analysis, the Excel form provided by Mirjam J Knol et al. was used to calculate the RERI(relative excess risk due to interaction), AP(the attributable proportion due to interaction), and S(the synergy index) values [26]. Regarding significant interactions, analyses were stratified according to the type of calf circumference(normal and low calf circumference groups) and physical performance score(normal: 0 or 1 point; poor: 2–8 points). As 4909 (40.6%) and 1301 (10.8%) participants scored 0 and 1 point for physical performance, we merged them into one group for statistical analyses. Further, we merged those with 2–8 points into one group. To clarify the effects of calf circumference and physical performance on depression, a stepwise approach was used to adjust for different sets of confounding factors. Model 1 was adjusted for socioeconomic characteristics. Model 2 was additionally adjusted for lifestyle- and health-related behaviors. Model 3 was additionally adjusted for the health status.
Considering the interaction of calf circumference and physical performance, we combined them as two dichotomous variables and included them as a four dichotomous variables in multivariate logistic regression to evaluate the combined effect of these two factors on depression. The four categories were: normal calf circumference with normal physical performance; low calf circumference with normal physical performance; normal calf circumference with poor physical performance; and low calf circumference with poor physical performance.
Sensitivity analyses were conducted. First, multiple linear regression was conducted with calf circumference and depressive symptoms as continuous variables, considering interaction term. Second, multiple imputation was used to test the influence of missing data. Multiple logistic regression was conducted on the imputed datasets adjusted for model 3.
The data were analyzed using IBM SPSS Statistics version 20.0 for Windows (SPSS Inc., Chicago, IL). Two-tailed p-value <0.05 was considered statistical significance.
Results
General characteristics
This study involved 12,227 participants aged 83.4 ± 11.0 years, including 4904 participants aged 65–79 years and 7323 participants aged ≥80 years. The mean CES-D-10 score was 7.4 ± 4.5 (95% CI: 7.31–7.47). A CES-D-10 score ≥ 10, indicating depression, was found in 3335 (27.3%) participants (95% CI: 26.5–28.1%). Participants with depression were more likely to have low calf circumference (2274 [68.2%] vs. 5406 [60.8%], p<0.001) and poor physical performance(3 [0, 6] vs. 1 [0, 4], p<0.001; Table 1). Participants with depression were significantly older, predominantly female, less educated, more likely to be separated from their spouse or living alone, and retired without pension. They were more likely to have disability in ADL, and be less active in social and leisure activities. They traveled and exercised less and consumed an unhealthy diet. They had lower BMI, poor cognitive function, and more kinds of chronic diseases.
Association of combined calf circumference and physical performance with depressive symptoms
To verify the possible interaction between calf circumference and physical performance, the interaction terms of the two factors were included in the regression model. After adjusting for confounding factors, the interaction term remained statistically significant(OR = 0.94, 95% CI: 0.91–0.98, p< 0.05), implying that multiplicative interaction exists between calf circumference and physical performance (Table 2) [27]. RERI(95%CI) = −0.03(−0.09–0.04), AP(95%CI) = −0.02(−0.06–0.02), S(95%) = 0.95(0.85–1.08), which means there is no significant additive interaction between low calf circumference and physical performance [26,27,28]. Stratified by the type of calf circumference, physical performance showed a significant association with depression after adjusting for confounding factors. In the normal calf circumference group, with every 1-point increase in physical performance, the risk of depression increased by 20% (OR = 1.20, 95% CI: 1.15–1.26, p<0.001). In the low calf circumference group, with every 1-point increase in physical performance, the risk of depression increased by 14% (OR = 1.14, 95% CI: 1.11–1.18, p<0.001). Conversely, in the normal physical performance group(score 0 or 1 point), the association between calf circumference and depression attenuated after adjusting for confounding factors (OR = 1.13, 95% CI: 0.98–1.30, p = 0.06). No significant association was found in the poor physical performance group between calf circumference and depression.
We explored patterns of the joint effect of calf circumference and physical performance on depressive symptoms. Table 3 shows the OR estimates for the strata as defined by the four pairs formed from two categories of calf circumference and two categories of physical performance. Participants with low calf circumference and poor physical performance were 2.21 times more likely to have depression than those with normal calf circumference and physical performance. The highest depression rate, at 36.9%, was found in the group with low calf circumference and poor physical performance. Trend test showed that the risk of depression increased as the number of factors increased. (p for trend< 0.001).
Sensitivity analysis
In the sensitivity analysis, we conducted multiple linear regression to test the robustness of the results. Depressive symptoms expressed as scores and calf circumference as cm. Because of the statistical significance of the interaction term (p = 0.01). We conducted a stratified analysis. Physical performance showed a consistent association with depression in both normal and low circumference group after adjusting for model 3. However, the impact of calf circumference attenuated after adjusting for confounding factors in both groups of physical performance (scores: 0 or 1 point and 2–8 points; Supplementary Table 1). The results of multiple logistic regression after multiple imputations as sensitivity analysis were consistent with the final results.
Discussion
Utilizing a nationally representative large-scale survey of the elderly (aged ≥65 years) Chinese population, a cross-sectional study was conducted to investigate the relationship of calf circumference and physical performance with depression. The association between physical performance and depression was found to be pronounced, consistent with previous studies [29, 30]. Physical inactivity was a common risk factor for sarcopenia and depression and could mediate the relationship between them [31]. Furthermore, skeletal muscle and the brain show crosstalk [32]. Contracting skeletal muscles secrete neurotrophic factors, which play a role in mood. Neurotrophins, such as brain-derived neurotrophic factor and neurotrophin-3, which promote neuronal differentiation, survival, and synaptic potentiation, are produced by both the brain and skeletal muscle and are associated with mood and muscle regeneration [33]. This may be the potential mechanism underlying the association between sarcopenia and mental illness, as decreased neurotrophic support of the brain is associated with depression and anxiety [34]. Chronic low-grade inflammation and oxidative stress, which are associated with both depression and sarcopenia, may be another possible mechanism [7, 35]. These studies imply that the relationship between sarcopenia and depression may be mediated by physical activity, brain plasticity and inflammation. Potential intervention of these factors might not only relieve depression but also improve sarcopenia.
In this study, people with larger calf circumferences were less likely to have depressive symptoms. Further, after adjusting for potential confounding factors, the impact of calf circumference attenuated, consistent with previous studies [30, 36]. A European consensus indicates that age-related changes in fat deposits and loss of skin elasticity can lead to estimation errors of the calf circumference in the elderly population [37]. Therefore, calf circumference may not be a good predictor of muscle mass in that population. Individuals may have developed sarcopenic obesity because of lack of exercise, which can result in a reduced predictive value of the calf circumference for muscle mass.
The interaction analysis showed a multiplicative interaction between low calf circumference and physical performance. Considering no addictive interaction was found, the biological effect of joint exposure needs to be elucidated in further study. Subsequently, in the joint effect analysis, we found that people with both low calf circumference and the poor physical performance had the highest morbidity of depression. They were 2.21 times more likely to have depression than those with normal calf circumference and physical performance. These analyses suggest that low calf circumference and physical performance may work in a synergistic way to increase the risk of depression in older adults. The above results suggest we should provide professional medical services on time for susceptible groups. Some similar previous studies have been conducted in ethnic groups other than the Chinese. An English study showed that reduction in grip strength is associated with a higher risk of depressive symptoms in participants with obesity [16]. A Japanese cross-sectional study found a significant association between sarcopenia and depression in elderly male patients with diabetes, measured by “Strength, assistance with walking, rising from a chair, climbing stairs, and falls” (SARC-F) and CES-D questionnaires [38]. A Korean study found that the coexistence of low muscle mass and low muscle function(assessed using dual-energy X-ray absorptiometry scanning and sit-to-stand mean power based on a 30 s chair stand test) is significantly associated with an increased risk of depressive symptoms [39]. Because of the complexity of sarcopenia diagnosis, many studies have shown a correlation with one component of its diagnostic criteria, insufficient to prove a link between muscle condition (muscle mass, muscle strength, or physical performance) and depression. More prospective and large-scale studies are required to clarify the relationship between muscle condition and depression.
The advantage of our study was the use of a large sample size of the elderly Chinese population. To obtain robust results, we adjusted for many confounding factors. However, the study has some limitations. First, we selected four questions in the questionnaire to evaluate physical performance in reference to SARC-F, which was recommended to screening sarcopenia by AWGS 2019 Consensus [3]. However, the evaluation efficiency of the questionnaire composed of these four questions has not been tested. Therefore, the results of the present study may lack universality. Second, we excluded 3414 participants because of missing data on CES-D. Comparing the baseline characteristics of the excluded participants with the included participants, revealed that the data were not missing completely at random, which might influenced the results. Therefore, we used multiple imputation to evaluate the impact of missing data on the results. Third, we evaluated physical performance by a subjective questionnaire, which might be inaccurate because of the depressive symptoms of the participants, making them choose more negative answers rather than actual answers. Or we can’t rule out the possibility that their physical performance is reduced due to depression-induced low physical activity. Causality is difficult to investigate because of our cross-sectional study design. Prospective studies are required to address this limitation.
Conclusions
Depression and sarcopenia are common diseases in the elderly population. This study showed a strong association between physical performance and depression, but no significant association between calf circumference and depressive symptoms. Future studies should focus on the comorbidities of depression and sarcopenia in the elderly population.
Availability of data and materials
The data that support the findings of this study are available in https://opendata.pku.edu.cn/dataverse/CHADS [40].
Abbreviations
- CLHLS:
-
Chinese Longitudinal Healthy Longevity Survey
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- CES-D:
-
Center for Epidemiologic Studies Depression Scale
- AWGS:
-
Asian Working Group for Sarcopenia
- ADL:
-
Activities of daily living
- BMI:
-
Body mass index
- MMSE:
-
Mini-Mental State Examination
- RERI:
-
Relative Excess Risk due to Interaction
- AP:
-
Attributable Proportion
- S:
-
the Synergy index
References
Chand SP, Arif H. Depression. StatPearls. Treasure Island: StatPearls Publishing. Copyright © 2021, StatPearls Publishing LLC.; 2021.
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–858.
Beekman AT, Copeland JR, Prince MJ. Review of community prevalence of depression in later life. Br J Psychiatry J Ment Sci. 1999;174:307–11.
Chen LK, Woo J, Assantachai P, Auyeung TW, Chou MY, Iijima K, et al. Asian working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–7.e2.
Cohen S, Nathan JA, Goldberg AL. Muscle wasting in disease: molecular mechanisms and promising therapies. Nat Rev Drug Discov. 2015;14(1):58–74.
Budui SL, Rossi AP, Zamboni M. The pathogenetic bases of sarcopenia. Clinical cases in mineral and bone metabolism : the official journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases. 2015;12(1):22–6.
Sepehrmanesh Z, Kolahdooz F, Abedi F, Mazroii N, Assarian A, Asemi Z, et al. Vitamin D supplementation affects the Beck depression inventory, insulin resistance, and biomarkers of oxidative stress in patients with major depressive disorder: a randomized, controlled clinical trial. J Nutr. 2016;146(2):243–8.
Berk M, Williams LJ, Jacka FN, O'Neil A, Pasco JA, Moylan S, et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013;11:200.
Velázquez-Alva MC, Irigoyen-Camacho ME, Cabrer-Rosales MF, Lazarevich I, Arrieta-Cruz I, Gutiérrez-Juárez R, et al. Prevalence of Malnutrition and Depression in Older Adults Living in Nursing Homes in Mexico City. Nutrients. 2020;12(8):2429.
Vancampfort D, Firth J, Schuch FB, Rosenbaum S, Mugisha J, Hallgren M, et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: a global systematic review and meta-analysis. World Psychiatry. 2017;16(3):308–15.
Islam MZ, Disu TR, Farjana S, Rahman MM. Malnutrition and other risk factors of geriatric depression: a community-based comparative cross-sectional study in older adults in rural Bangladesh. BMC Geriatr. 2021;21(1):572.
Dunn AL, Trivedi MH, Kampert JB, Clark CG, Chambliss HO. Exercise treatment for depression: efficacy and dose response. Am J Prev Med. 2005;28(1):1–8.
Kokkeler KJE, van den Berg KS, Comijs HC, Oude Voshaar RC, Marijnissen RM. Sarcopenic obesity predicts nonremission of late-life depression. Int J Geriatr Psychiatry. 2019;34(8):1226–34.
Kim NH, Kim HS, Eun CR, Seo JA, Cho HJ, Kim SG, et al. Depression is associated with sarcopenia, not central obesity, in elderly korean men. J Am Geriatr Soc. 2011;59(11):2062–8.
Cho Y, Shin SY, Shin MJ. Sarcopenic obesity is associated with lower indicators of psychological health and quality of life in Koreans. Nutrition research (New York, NY). 2015;35(5):384–92.
Hamer M, Batty GD, Kivimaki M. Sarcopenic obesity and risk of new onset depressive symptoms in older adults: English longitudinal study of ageing. Int J Obes (2005). 2015;39(12):1717–20.
Fukumori N, Yamamoto Y, Takegami M, Yamazaki S, Onishi Y, Sekiguchi M, et al. Association between hand-grip strength and depressive symptoms: locomotive syndrome and health outcomes in Aizu cohort study (LOHAS). Age Ageing. 2015;44(4):592–8.
Zeng Y, Poston DL, Vlosky DA, Gu D. Healthy longevity in China: demographic, socioeconomic, and psychological dimensions: Springer Science & Business Media; 2009.
Zeng Y, Feng Q, Gu D, Vaupel JW. Demographics, phenotypic health characteristics and genetic analysis of centenarians in China. Mech Ageing Dev. 2017;165(Pt B):86–97.
Zeng Y, Feng Q, Hesketh T, Christensen K, Vaupel JW. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet. 2017;389(10079):1619–29.
Kawakami R, Miyachi M, Sawada SS, Torii S, Midorikawa T, Tanisawa K, et al. Cut-offs for calf circumference as a screening tool for low muscle mass: WASEDA'S health study. Geriatr Gerontol Int. 2020;20(10):943–50.
Gonzalez MC, Mehrnezhad A, Razaviarab N, Barbosa-Silva TG, Heymsfield SB. Calf circumference: cutoff values from the NHANES 1999-2006. Am J Clin Nutr. 2021;113(6):1679–87.
Chen CY, Tseng WC, Yang YH, Chen CL, Lin LL, Chen FP, et al. Calf circumference as an optimal choice of four screening tools for sarcopenia among ethnic Chinese older adults in assisted living. Clin Interv Aging. 2020;15:2415–22.
Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am J Prev Med. 1994;10(2):77–84.
Liu Y, Chen X, Yan Z. Depression in the house: the effects of household air pollution from solid fuel use among the middle-aged and older population in China. Sci Total Environ. 2020;703:134706.
Knol MJ, VanderWeele TJ. Recommendations for presenting analyses of effect modification and interaction. Int J Epidemiol. 2012;41(2):514–20.
Knol MJ, van der Tweel I, Grobbee DE, Numans ME, Geerlings MI. Estimating interaction on an additive scale between continuous determinants in a logistic regression model. Int J Epidemiol. 2007;36(5):1111–8.
Naimi AI, VanderWeele TJ. Explanation in causal inference: methods for mediation and interaction. Eur J Epidemiol. 2016;31(10):1065–6.
Szlejf C, Suemoto CK, Brunoni AR, Viana MC, Moreno AB, Matos SMA, et al. Depression is associated with sarcopenia due to low muscle strength: results from the ELSA-Brasil study. J Am Med Dir Assoc. 2019;20(12):1641–6.
Hayashi T, Umegaki H, Makino T, Cheng XW, Shimada H, Kuzuya M. Association between sarcopenia and depressive mood in urban-dwelling older adults: a cross-sectional study. Geriatr Gerontol Int. 2019;19(6):508–12.
Hallgren M, Herring MP, Owen N, Dunstan D, Ekblom Ö, Helgadottir B, et al. Exercise, physical activity, and sedentary behavior in the treatment of depression: broadening the scientific perspectives and clinical opportunities. Front Psych. 2016;7:36.
Delezie J, Handschin C. Endocrine crosstalk between skeletal muscle and the brain. Front Neurol. 2018;9:698.
Pasco JA, Williams LJ, Jacka FN, Stupka N, Brennan-Olsen SL, Holloway KL, et al. Sarcopenia and the common mental disorders: a potential regulatory role of skeletal muscle on brain function? Curr Osteoporos Rep. 2015;13(5):351–7.
Molendijk ML, Bus BA, Spinhoven P, Penninx BW, Prickaerts J, Oude Voshaar RC, et al. Gender specific associations of serum levels of brain-derived neurotrophic factor in anxiety. World J Biol Psychiatry. 2012;13(7):535–43.
Schaap LA, Pluijm SM, Deeg DJ, Harris TB, Kritchevsky SB, Newman AB, et al. Higher inflammatory marker levels in older persons: associations with 5-year change in muscle mass and muscle strength. J Gerontol A Biol Sci Med Sci. 2009;64(11):1183–9.
Chen L, Sheng Y, Qi H, Tang T, Yu J, Lv S. Correlation of sarcopenia and depressive mood in older community dwellers: a cross-sectional observational study in China. BMJ Open. 2020;10(9):e038089.
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(4):601.
Ida S, Murata K, Nakai M, Ito S, Malmstrom TK, Ishihara Y, et al. Relationship between sarcopenia and depression in older patients with diabetes: An investigation using the Japanese version of SARC-F. Geriatr Gerontol Int. 2018;18(9):1318–22.
Jin YA-O, Kang S, Kang HA-O. Individual and Synergistic Relationships of Low Muscle Mass and Low Muscle Function with Depressive Symptoms in Korean Older Adults. https://doi.org/10.3390/ijerph181910129 [doi] LID - 10129. (1660–4601 (Electronic)).
The Chinese Longitudinal Healthy Longevity Survey (CLHLS)-Longitudinal Data(1998–2018). V2ed: Peking University Open Research Data Platform; 2020. https://opendata.pku.edu.cn/dataverse/CHADS.
Acknowledgements
The authors acknowledge the efforts of this research team and appreciate all the participants for attending this research.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
JYT and TQ designed the research. JYT, TQ and MN wrote the manuscript and analyzed the data. JYT, QLZ, MN and YXZ contributed to the data collection. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was carried out in accordance with the Declaration of Helsinki as revised 1989. The 2018 wave of CLHLS study was approved by the Biomedical Ethics Committee of Peking University (IRB00001052–13074). All participants or their legal representatives signed written consent forms in the baseline and follow-up surveys.
Consent for publication
Not applicable.
Competing interests
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary table 1.
Sensitivity analysis of the multiple linear regression for the association of calf circumference and physical performance with depressive symptoms. Supplementary table 2. Sensitivity analysis of the multiple logistic regression for the association of calf circumference and physical performance with depressive symptoms after multiple imputation.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tan, JY., Zeng, QL., Ni, M. et al. Association among calf circumference, physical performance, and depression in the elderly Chinese population: a cross-sectional study. BMC Psychiatry 22, 278 (2022). https://doi.org/10.1186/s12888-022-03925-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-03925-z