
Abstract
Background
Population surveys across the world have examined the impact of the COVID-19 pandemic on mental health. However, few have simultaneously examined independent cross-sectional data with longitudinal data, each of which have different strengths and weaknesses and facilitate the investigation of distinct research questions. This study aimed to investigate psychological distress and life satisfaction during the first and second lockdowns in the state of Victoria, Australia, and the social factors that may be affected by lockdowns and could affect mental health.
Methods
The VicHealth Victorian Coronavirus Wellbeing Impact Study included two 20-min opt-in online panel surveys conducted in May and September 2020 in Victoria, each with a sample of 2000 adults aged 18 + . A two-part study design was used: a repeated cross-sectional study of respondents who participated in Survey One and Survey Two, followed by a longitudinal nested cohort study. The primary exposures were social solidarity, social connectedness and staying connected with family and friends. Using logistic regression modelling, we explored the associations between our exposures and primary outcomes of psychological distress and life satisfaction with and without adjustment for covariates, both cross-sectionally and longitudinally. The results from the multivariable models were summarised using adjusted Odds Ratios (aOR), 95% Confidence Intervals (CI).
Results
Cross-sectional results indicated that the percentage of participants with low life satisfaction was significantly higher in the second survey sample (53%) compared to the first (47%). The percentage of participants with high psychological distress was higher but not significantly different between the two survey samples (14% first survey vs 16% second survey). Longitudinal study results indicated that lower social connectedness was significantly associated with higher psychological distress (aOR:3.3; 95% CI: 1.3–8.4) and lower life satisfaction (aOR:0.2; 95% CI: 0.1–0.4). Younger adults had higher psychological distress compared to older adults (aOR:6.8; 95% CI:1.5–31.1). Unemployment at the time of the first survey was significantly associated with lower life satisfaction at the second survey (aOR:0.5; 95% CI: 0.3–0.9).
Conclusion
This study supports the findings of other international studies. It also highlights the need to promote increased social connection and maintain it at times of isolation and separation, particularly amongst younger adults.
Similar content being viewed by others

Introduction
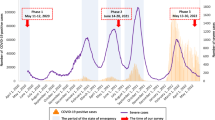
The COVID-19 global pandemic is ongoing, caused by the SARS-CoV-2 virus. The first outbreak of infection was in China in December 2019, which was followed by spread to many other countries. The first case was detected in Australia on 25th January 2020. This case was in Melbourne, the capital of the state of Victoria. In the absence of vaccines at the time, the Victorian government attempted to control the spread of the virus using lockdowns, beginning on the 30th March 2020. Victoria, and the city of Melbourne in particular, was the region of Australia most impacted by the pandemic and by series of lockdowns, which are summarized in Table 1. As in the rest of the world, the initial concern about the pandemic was the effect on mortality and hospitalizations. However, as the pandemic progressed, the potential effects on mental health have also been recognized [1]. Given the strong evidence for increased psychological distress and mental disorders after disasters [2], the prevalence of mental health problems was expected to rise due to infection and fear of infection, as well as the impacts of lockdowns, including social isolation, loss of employment and income, and intensification of pressures on families.
There is now an extensive international literature exploring the mental health consequences of the pandemic. Early studies involved cross-sectional comparisons of the prevalence of symptoms of distress, anxiety and depression during the early months of the pandemic (March–April 2020) compared to pre-pandemic data; they found that the prevalence of symptoms was higher than pre-pandemic [5, 6]. Subsequent studies used stronger longitudinal designs and repeated cross-sectional surveys of representative samples. Systematic reviews and meta-analyses of these studies found that symptoms of distress, anxiety and depression increased during the early months (March–April) of the pandemic in 2020 but returned to pre-pandemic levels by the middle of that year [7, 8].
While longitudinal studies with frequent waves have been proposed as the best methodology for investigating pandemic-related mental health impacts [9], survivorship bias has been raised as a limitation of these studies. Czeisler et al. [10] analysed a 4-wave longitudinal study from the USA and found that people who participated in only 1 or 2 waves had a higher prevalence of depression and anxiety symptoms. This selective pattern of retention could lead to an overly optimistic interpretation of mental health over time. Czeisler et al. [10] therefore recommended the simultaneous use of independent cross-sectional data along with longitudinal data, as these approaches have different strengths and weaknesses, and facilitate the investigation of distinct research questions.
Most studies of the impact of the pandemic have assessed symptoms of mental disorders. However, Keyes [11] argued that a complete assessment of mental health should take account of a dimension of positive mental health as well as symptoms. Relevant to this two-dimensional concept, there have also been some studies on the effects of the pandemic on positive mental health, including subjective well-being, life satisfaction and positive affect. There has been less research carried out on positive mental health than on symptoms, but one systematic review and meta-analysis of studies up to June 2020 found no significant effect of COVID-19 pandemic lockdowns on measures of life satisfaction, positive affect, well-being and quality of life [12].
In addition to research examining changes in mental health measures, there have been studies of factors that may impact any changes found. A particular focus of pandemic studies has been social isolation and loneliness, as these are potentially adversely affected during lockdowns. While there was some evidence of an increase in these factors during the early phases of the pandemic [13], other systematic reviews found a lack of effect [7, 12]. One explanation of these findings is that there was an initial impact of restrictions and lockdowns on social relationships, but people soon adapted by finding alternative online means of social contact [12, 13] and that the shared experience of the pandemic may have increased social cohesion [12]. Studies from other types of disasters have also indicated that social factors such as access to social support and sense of social solidarity are associated with more positive mental health outcomes [14]. However, it was also shown that these factors can deteriorate over time.
The above findings mainly come from studies in Europe and North America and may not be generalizable to all countries. We focus on the studies with stronger methodologies involving more systematic and representative samples.
From early in the pandemic, the Australian Bureau of Statistics (ABS) has monitored the health and social impacts [15]. It found that symptoms of psychological distress increased in April 2020 when the nation was first affected by lockdowns, declined to pre-pandemic levels by June as restrictions eased, and then increased again in August when there was another wave of lockdowns. Another source of longitudinal data has come from the Life in Australia Panel [16]. This study found that the prevalence of severe psychological distress rose in April 2020 compared to pre-pandemic, but then fell in May. It worsened again from May to August, mainly due to the effects of a second lockdown in the state of Victoria. This impact subsequently declined, with Victoria showing little difference from the rest of the country by November 2020. A third longitudinal panel study is the Australian National COVID-19 Mental Health and Risk Communication Survey, which involved fortnightly on-line surveys from March to June 2020 [17]. This study found that any changes in depression and anxiety symptoms were generally transitory. The study also found that while suicidal ideation was high, it did not vary over time [18]. Later work from this study reported greater psychological distress in parents and caregivers who were home schooling, but no effect on wellbeing [19]. Overall, the Australian data show a worsening of mental health which was associated with lockdowns, but this effect diminished over time.
Australian studies of mental health outcomes from other types of disaster are also of relevance, including an epidemiological study showing increased risk of psychiatric disorders post disaster [20], cross-sectional analyses demonstrating a complex relationship between social networks and individual mental health post bushfires [21], and longitudinal analyses indicating moderate involvement in community groups can be a protective factor for mental health following bushfire exposure [22].
In the present study, we report new repeated cross-sectional and longitudinal data from the Australian state of Victoria, which was the region of Australia most affected by pandemic lockdowns. The capital city of Melbourne was particularly affected and by 2021 was one of the most locked-down cities in the world [23]. Consistent with Keyes’ [11] two-factor concept of mental health, the study aimed to assess both symptoms of psychological distress and life satisfaction. We aimed to investigate cross-sectional factors associated with higher psychological distress and life satisfaction at each survey, and also social connection factors associated with longitudinal changes between the two surveys.
Method
This paper builds on the descriptive findings of the Victorian Coronavirus Wellbeing Impact Study surveys [24], which showed significantly higher rates of low-medium life satisfaction over time and a non-significant trend towards higher rates of psychological distress over time.
Study design
The current analysis has a two-part study design: a repeated cross-sectional study of respondents who participated in Survey One and Survey Two, followed by a longitudinal nested cohort study of these same respondents. The surveys were undertaken by the Victorian Health Promotion Foundation (VicHealth), a state-based government agency in Victoria, Australia, with a remit to promote health and prevent illness.
The VicHealth Coronavirus Victorian Wellbeing Impact Surveys of Victorian residents aged 18 years and over were conducted via an opt-in ‘research only’ online panel (i.e. non-probability panel). The surveys were designed to track the impact of the pandemic and associated lockdowns on a range of behavioural and attitudinal health risk factors during the first two waves of the pandemic in Victoria, from March to June in 2020 and from July through to October 2020.
Survey One commenced on 31 May 2020 and concluded 8 June 2020. The total achieved sample size was 2,000. Survey Two, which was conducted during the second pandemic wave, commenced on 10 September 2020 and concluded on 21 September 2020. Survey Two included 1,008 respondents who were re-contacted from Survey One and 992 ‘new’ respondents (i.e. those who did not complete Survey One), to boost the total sample size to 2,000.
Participants
The opt-in online panel used for both surveys was LiveTribe, a research-only panel operated and managed by i-Link Research https://www.i-linkresearch.com/. LiveTribe panellists are recruited via print media, online marketing initiatives, direct mail, social media platforms, affiliate partnerships, personal invitations and a range of other ad-hoc initiatives. For Survey One and Two the sample size of 2,000 was chosen as it provides a reasonable margin of error for the purposes of estimating population level results within an expedited fieldwork turnaround period.
Survey questionnaire
The 20-min survey questionnaire (see Supplementary file 1) covered a range of health and wellbeing factors, including life satisfaction, subjective wellbeing, psychological distress and social connection, as well as socio-demographics. The selection of health and wellbeing indicators for the questionnaire was guided by several key principles previously used in population surveys conducted by VicHealth [25]. These principles included: sensitivity to change across person, place and time; strong psychometric properties; being amenable to action at a range of jurisdiction levels including local government; non-duplication of other Victorian population surveys; and brief questions that could be feasibly used in local program evaluations, thus allowing the population measure to act as a comparator for local evaluations.
Different question styles were used to minimise respondent fatigue and enhance engagement with the survey, such as Likert scales, closed-ended questions and open-ended questions. Current guidelines were followed to ensure questions were as user-friendly as possible for respondents, regardless of the device being used to access the survey (for example, mobile phones, tablets, desktops or laptops) [26]. Respondents were also asked to provide their nearest cross-street to enable the application of geo-codes to participants’ identification codes and their question responses.
No formal pilot testing of the survey was undertaken. However, a soft launch was undertaken to confirm the integrity of the questionnaire. The soft launch involved inviting a small number of participants to complete the survey, with the aim of securing approximately 20 completed surveys. The data from these surveys were carefully checked against the Microsoft Word version of the survey to ensure the survey was error free and had been scripted as expected. No errors were detected as a result of this process and the survey was launched in full without any amendment. The average completion time of the questionnaire was 20 min.
Measures
Our primary outcomes were psychological distress and life satisfaction, and the primary exposures were feeling connected with others, staying connected with family and friends, and social solidarity.
‘Psychological distress’ was measured using the Kessler Psychological Distress Scale-6 (K6) which has excellent internal consistency reliability (Cronbach's alpha = 0.89) [27]. The K6 is a combined score across 6 areas of psychological distress; each person can score a minimum of 6 and maximum of 30. Scores of 19 or more are classified as probable serious mental illness, while scores of 6 to 18 are classified as no probable serious mental illness. Null responses to 2 or more of the 6 statements were excluded from the mean calculation, with adjustments made for those who gave a null response to 1 statement.
‘Life satisfaction’ [28] was derived from a rating of satisfaction with life as a whole using a scale of 0 to 10 where 0 is completely dissatisfied and 10 is completely satisfied. The measure correlates highly with the Personal Wellbeing Index measure of life satisfaction (r = 0.79) [29]. Low to medium life satisfaction was defined as a score between 0 and 6 out of 10. Null responses were excluded from mean calculation.
The measure of ‘Feeling connected with others’ [30] uses a six item Likert scale to assess level of agreement with the statement ‘I feel connected with others’. The measure has a high positive correlation (+ 0.79) with the Social Connectedness Revised Scale and a high negative correlation (-0.69) with the UCLA Loneliness Scale [30]. For analysis, responses were divided into the percentage of people who selected strongly disagree, disagree, mildly disagree, mildly agree, and those who selected agree or strongly agree.
‘Staying connected with family and friends’ was a question developed for the survey and to the best of our knowledge it is the first time that this measure has been used. It measures the extent to which people find it easy or hard to stay connected with those close to them. For analysis, the five-point Likert scale was coded as the percentage of people who reported it was 1. very easy or easy; 2. neither or 3. hard or very hard.
The ‘Social solidarity’ measure [31] was designed to determine how close people feel with their communities using a combined score across six questions and has good reliability across samples (Cronbach’s alpha ranging from 0.78 to 0.89). These questions ask respondents whether they agree with statements regarding their connection with their local community. Responses for all six questions were assigned the following values: Strongly disagree = 1, Disagree = 2, Neither agree nor disagree = 3, Agree = 4, Strongly agree = 5. Any respondent providing a ‘don’t know’ or ‘prefer not to answer’ response to any of the six questions was excluded from the analysis. The final score was calculated by summing the values of the six categories out of a maximum of 30 and minimum of six.
In addition to the above, the variables age, gender, disability, income, the main activity in September, region, and household composition were used as covariates in the longitudinal analysis. The covariates used for each analysis are shown in the corresponding tables.
Ethics
Ethics approval for Survey One was provided by the Australian National University Human Research Ethics Committee (2020/264) on 20 May 2020. Ethics approval for Survey Two was provided by the Australian National University Human Research Ethics Committee (2020/540) on 8 September 2020. All methods were carried out in accordance with relevant guidelines and regulations. Online written informed consent was obtained from study participants as this survey was carried out as an online survey.
Statistical analysis
Data were analysed using Stata, V.17 [32] and R software [33]. Categorical data were summarised using frequency with percentages, continuous data using means with standard deviations, and skewed data using medians with interquartile ranges (25th –75th centile). Our primary outcomes, exposures and covariates are described in the Measures section. To assess differences in dependent means and proportions paired sample t-tests and McNemar’s tests were used respectively. Using logistic regression modelling, we explored the associations between our exposures and primary outcomes of psychological distress and life satisfaction with and without adjustment for covariates. The results from the multivariable models were summarised using adjusted Odds Ratios (aOR), 95% Confidence Intervals (CI) and p-values. To identify confounding variables for the regression analyses, we used information from previous literature and Directed Acyclic Graphs (DAG) [34, 35]. For each outcome, we conducted three separate analyses: (i) a cross-sectional analysis at the first lockdown, (ii) a cross-sectional analysis at the second lockdown, and (iii) a longitudinal analysis exploring the change in outcome measures between the two lockdowns. We tested for exposure-outcome associations that may have been modified by other covariates using interaction terms and likelihood ratio tests, and used measures of fit for logistic regression [36] to test model assumptions. We used complete-case analysis (i.e., analysis restricted to participants with complete data), and investigated the baseline first-lockdown characteristics of those missing and not-missing at the second lockdown using summary statistics.
Results
Cohort characteristics
The cohort characteristics for the 1008 participants who completed the survey at both lockdowns are shown in Table 2. Table 2 indicates that this sample consists of a higher proportion of female participants (56%) compared to male, a higher proportion living in Melbourne (77%) compared to regional areas, and a higher proportion reporting not having a disability (75%). Approximately 56% were employed in February 2020 and 55% employed in September 2020, while the rest consisted of retired, student and other in February and September 2020. Approximately 32% of the household composition consisted of couples with children, and the rest consisted of couple living alone, person living alone, single parent with children and other. Compared to the first lockdown, at the second lockdown participants had lower life satisfaction, felt less connected with others, had a harder time connecting with family and friends, and had lower social solidarity.
The cohort characteristics are summarised separately at the first and the second lockdowns in Supplementary File 2 Table S1. The participants’ characteristics at the first lockdown for those who were missing and not missing at the second lockdown are shown in Supplementary File 2 Table 1. Supplementary File 2 Table S2 shows that those who were missing at the second lockdown compared to those who were not missing, had higher psychological distress, and were more likely to be male, live in Melbourne, and be employed in February 2020.
Cross-sectional results at the first lockdown
Cross-sectional results from logistic regression modelling at the first lockdown with psychological distress and life satisfaction as outcomes are shown in Table 3.
At the first lockdown, participants who found it hard to stay connected with others had 1.86 (95% CI: 1.2–2.9) times higher odds of psychological distress compared to those who found it easy to stay connected after adjusting for covariates. Participants who did not feel connected with others had 3.8 (95% CI: 2.4–6.2) times higher odds of psychological distress than those who felt connected. Higher social solidarity was associated with lower odds of psychological distress (Odds Ratio, OR = 0.96, 95% CI: 0.9–1.0). Melbourne residents had higher odds of psychological distress compared to those who lived outside Melbourne. Psychological distress was higher for younger participants. Participants who reported a disability had higher odds of psychological distress compared to those who did not report disability. In addition, lower income was associated with higher psychological distress.
A similar range of variables were found to be associated with life satisfaction at the first lockdown (Table 3). Participants who did not feel connected with others had 0.3 (95% CI: 0.2–0.4) times lower odds of life satisfaction than those who felt connected after accounting for covariates. Those who found it hard to stay connected with others had 0.5 (95% CI: 0.3–0.6) times lower odds of life satisfaction compared to those who found it easy to stay connected. Higher social solidarity was associated with higher odds of life satisfaction (OR = 1.09, 95% CI: 1.06–1.12). Life satisfaction was lower for younger participants. Participants who reported disability had lower odds of life satisfaction compared to those who did not report disability. Lower income was associated with lower life satisfaction.
Cross-sectional results at the second lockdown
Cross-sectional results at the second lockdown for the outcome variables psychological distress and life satisfaction are shown in Table 4.
The cross-sectional results at the second lockdown were comparable to the first lockdown. Participants who did not feel connected with others had 2.6 (95% CI: 1.7–4.0) times higher odds of psychological distress than those who felt connected after adjusting for covariates. Higher social solidarity was associated with lower odds of psychological distress (OR = 0.94, 95% CI: 0.9–1.0). Psychological distress was higher for younger participants. Participants who reported a disability had higher odds of psychological distress compared to those who did not report disability. Melbourne residents had higher odds of psychological distress compared to those who lived outside Melbourne.
Participants who did not feel connected with others had lower life satisfaction compared to those who felt connected (OR = 0.2, 95% CI: 0.2–0.3). The participants who found it hard to stay connected with others had 0.3 (95% CI: 0.2–0.4) times lower odds of life satisfaction compared to those who found it easy to stay connected. Higher social solidarity was associated with higher odds of life satisfaction (OR = 1.06, 95% CI: 1.03–1.09). Participants who reported a disability had lower odds of life satisfaction compared to those who did not report disability. Participants who were unemployed in the September had lower odds of life satisfaction compared to those who were employed.
Longitudinal results
Longitudinal results for psychological distress and life satisfaction are presented in Table 5.
The results showed that participants who did not feel connected with others at the second lockdown had 3.3 (95% CI: 1.3–8.4) times higher odds of psychological distress at the second lockdown after controlling for their psychological distress status at the first lockdown and other covariates (Table 5). The younger participants aged less than 35 years had higher odds of psychological distress compared to participants over 65 years of age. Participants who did not feel connected with others and found it hard to stay connected with the family and friends at the second lockdown had lower life satisfaction at the second lockdown—with OR = 0.2 (95% CI: 0.1–0.4) and OR = 0.4 (95% CI: 0.2–0.6) respectively—after accounting for their life satisfaction at the first lockdown and other covariates (Table 5). No significant associations between social connection (feeling connected, staying connected, social solidarity) at the first lockdown and psychological distress or life satisfaction at the second lockdown were found after controlling for covariates.
Discussion
This study aimed to investigate psychological distress and life satisfaction during the first and second lockdowns in the state of Victoria in 2020, as well as social factors that may be affected by lockdowns and which could affect mental health. The main finding was that adults aged 18 years and over who did not feel connected with others at the second lockdown had 3.3 times higher odds of psychological distress at the second lockdown, after controlling for their psychological distress status at the first lockdown and other covariates. This odds ratio is considered to be a small to medium effect size [38].
Cross-sectional findings
Using life satisfaction as an indicator of positive mental health, we found that the percentage of participants with low life satisfaction was significantly higher in the second survey sample (53.1%) compared to the first survey sample (46.9%). Because the survey samples are not representative, these percentages could be biased figures as estimates for prevalence. However, a previous descriptive analysis that weighted the data by population characteristics found a similar significant change for prevalence of low life-satisfaction from 49 to 53% [24]. This result differs from a previous systematic review and meta-analysis of studies up to June 2020 which found no significant effect of COVID-19 pandemic lockdowns on life satisfaction. However, these studies examined the effects of single lockdowns, whilst the results of this study indicate that a second lockdown led to a decrease in life satisfaction.
By contrast, the percentage of participants with high psychological distress was not significantly different between the two survey samples, with high distress found in 14.3% in the first survey sample compared to 15.6% in the second survey sample. In comparison to the prevalence percentages reported previously where weighted data had been used, the prevalence percentages were higher, but again there was no change across surveys (16% vs 17%) [24]. These results are different to other studies that have found that psychological distress reduced after initially increasing during the early months (March–April 2020) of the pandemic [7, 8]. As the first survey was conducted in May–June 2020, it may be that this study did not capture the initial peak in psychological distress.
Whilst this study did not have a pre-COVID baseline, we can get some indication of the impact of lockdowns in general through examining the Melbourne region, which was subjected to greater restrictions than the rest of Victoria, particularly during the second lockdown. In the cross-sectional analyses from both lockdowns, residents of Melbourne had a higher level of psychological distress after adjusting for other factors, indicating that greater lockdown is likely to be a risk factor. These findings are consistent with studies internationally showing that lockdowns have a negative impact on symptoms of mental health problems [5, 6]. On the other hand, we found no effect of living in Melbourne compared to the rest of the state on life satisfaction, whereas there was a decrease in life satisfaction across the state as a whole from the first to the second lockdown.
When the social connection factors were examined, there was a higher proportion of participants in the second survey reporting not feeling connected to others and finding it hard to stay connected to family and friends. There was also a lower social solidarity mean score. These findings are consistent with the international literature that there was an increase in social isolation and loneliness in the early phase of the pandemic [13], but are not consistent with suggestions that the effect of social isolation diminished over time as people adapted by finding alternative online means of social contact [12, 13]. However, the findings are consistent with the broader literature on disasters showing a potential deterioration in social support and social solidarity over time following a critical incident [14].
Longitudinal findings
The longitudinal analysis facilitated the investigation of factors associated with changes in life satisfaction and psychological distress from the first to the second lockdown.
Lower social connectedness was associated with worsening of both psychological distress and life satisfaction. Not feeling connected with others was associated with both mental health variables, while finding it hard to stay connected was specifically associated with lower life satisfaction. This is consistent with the research following the Black Saturday bushfires which showed the relationship between social networks and mental health post disaster [21] and identified connection to community groups as a protective factor [22]. These associations point to interventions targeting social connectedness as a potential response to future lockdowns.
While lower social connectedness was associated with both increases in psychological distress and decreases in life satisfaction, there were also some differential associations. A notable longitudinal finding was that younger adults had a greater increase in psychological distress across lockdowns. This association was found even after adjustment for social risk factors and indicates that young people should be a particular target for intervention to reduce the psychological impact of lockdowns. This has been shown in other post-disaster studies and may reflect lower maturity and life experience [39]. However, by contrast, the younger adult age group was not associated with greater declines in life satisfaction.
Unemployment at the time of the first survey was also associated with declines in life satisfaction. Although the association with psychological distress was not statistically significant at our pre-set significance level, there was a trend in the same direction. However, any negative impact on mental health in the second lockdown may have been ameliorated by changes to Australian government policy in March 2020, that came into full effect after the first lockdown. This policy increased welfare payments to people who were unemployed in an effort to stimulate the economy (the JobSeeker scheme). There was also a JobKeeper scheme to subsidize wages of people in employment where the pandemic was adversely affecting the business of their employer, which may have reduced distress associated with fear of unemployment.
In the longitudinal analysis, we found no effect of living in Melbourne on changes in either psychological distress or life satisfaction, indicating that any worsening of mental health across lockdowns was not greater in Melbourne, despite the greater restrictions on the city in the second lockdown. At the time of the second survey (10–21 September 2020), Melbourne had been in lockdown for two months and had been under curfew for one month, whereas the rest of Victoria had been in lockdown only for approximately one month. It may be that the difference in accumulated lockdown ‘dose’ between Melbourne and the rest of Victoria at the time of the second survey was not significant enough to show a difference in psychological distress and life satisfaction. Alternatively, given that the cross-sectional analysis did show a difference in Victorian regions, the lack of effect in the longitudinal analysis may be an indicator of survivorship bias, with those experiencing higher psychological distress not participating in the second survey, consistent with the limitations of longitudinal studies reported previously [10].
Limitations
An important limitation is that the samples were taken from an opt-in online panel with complex recruitment strategies, which is unlikely to be representative. Some sub-groups are likely to be excluded by the survey method, such as people without digital access and/or without digital literacy or English literacy. While representativeness is not required for the longitudinal analysis of risk factors, it potentially affects prevalence estimates in the cross-sectional analyses. However, prevalence changes between surveys were similar when there was weighting of the sample by population characteristics [24], which adds to confidence in the findings.
In their longitudinal study of mental health during the pandemic, Czeisler et al. [10] found that there was a high dropout rate in people with worse mental health, which could lead to an overly optimistic interpretation of mental health over time. Our data are consistent with this finding, with the proportion of participants with high psychological distress in the first survey being greater for those who did not participate in the second survey compared to those who did (16% vs 12%). Thus, the proportion of people with high psychological distress is likely to be under-estimated at the second survey. However, we did not find a significant difference between these groups in the proportion of participants with low life satisfaction (48% vs 46%).
Conclusion
The state of Victoria, and the city of Melbourne in particular, was the area of Australia most impacted by COVID lockdowns. The cross-sectional data collected in the first and second lockdowns, reported here, facilitated an investigation of the factors associated with higher psychological distress and life satisfaction, consistent with Keyes’ [11] two-continua model of mental health, while the longitudinal data enabled an exploration of the change between the two lockdowns. The data showed that lower social connectedness was associated with worsening psychological distress and life satisfaction, and that the young adults had a greater increase in psychological distress across the lockdowns.
The results in this study support and expand on findings of other international studies. They also indicate that in any future pandemics or lockdowns, interventions designed to maintain social connectedness may ameliorate the risk of decreased well-being and increased psychological distress. This is particularly important for younger adults. Routine promotion of involvement in community groups may be protective [22].
Availability of data and materials
The de-identified dataset used and analysed during this current study is available from the corresponding author on reasonable request.
Change history
13 January 2023
A Correction to this paper has been published: https://doi.org/10.1186/s12889-022-14963-3
Abbreviations
- ABS:
-
Australian Bureau of Statistics
- CI:
-
Confidence Interval
- DAG:
-
Directed Acyclic Graphs
- K6:
-
Kessler Psychological Distress Scale-6
- OR:
-
Odds Ratio
- aOR:
-
Adjusted Odds Ratio
- SD:
-
Standard Deviation
- VicHealth:
-
Victorian Health Promotion Foundation
References
Carbone SR. Flattening the curve of mental ill-health: the importance of primary prevention in managing the mental health impacts of COVID-19. Mental Health and Prevention. 2020;19. https://doi.org/10.1016/j.mhp.2020.200185.
Beaglehole B, Mulder RT, Frampton CM, Boden JM, Newton-Howes G, Bell CJ. Psychological distress and psychiatric disorder after natural disasters: systematic review and meta-analysis. Br J Psychiatry. 2018;213(6):716–22. https://doi.org/10.1192/bjp.2018.210. Epub 20181010. Cited in: Pubmed; PMID 30301477.
Victoria State Government Health and Human Services. Coronavirus (COVID-19) Updates. 2021 31 January 2022. [October 2021]. Available from: https://www.dhhs.vic.gov.au/coronavirus/updates.
Parliament of Australia. COVID-19: a chronology of state and territory government announcements (up until 30 June 2020). 2020 31 January 2022. Available from: https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/rp/rp2021/Chronologies/COVID-19StateTerritoryGovernmentAnnouncements. [22 October 2020].
Kunzler AM, Röthke N, Günthner L, Stoffers-Winterling J, Tüscher O, Coenen M, Rehfuess E, Schwarzer G, Binder H, Schmucker C, Meerpohl JJ, Lieb K. Mental burden and its risk and protective factors during the early phase of the SARS-CoV-2 pandemic: systematic review and meta-analyses. Glob Health. 2021;17(1). https://doi.org/10.1186/s12992-021-00670-y.
Schafer KM, Lieberman A, Sever AC, Joiner T. Prevalence rates of anxiety, depressive, and eating pathology symptoms between the pre- and peri-COVID-19 eras: a meta-analysis. J Affect Disord. 2022;298:364–72. https://doi.org/10.1016/j.jad.2021.10.115.
Aknin LB, De Neve JE, Dunn EW, Fancourt DE, Goldberg E, Helliwell JF, Jones SP, Karam E, Layard R, Lyubomirsky S, Rzepa A, Saxena S, Thornton EM, VanderWeele TJ, Whillans AV, Zaki J, Karadag O, Ben AY. Mental health during the first year of the COVID-19 pandemic: a review and recommendations for moving forward. Perspect Psychol Sci. 2022. https://doi.org/10.1177/17456916211029964.
Robinson E, Sutin AR, Daly M, Jones A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J Affect Disord. 2022;296:567–76. https://doi.org/10.1016/j.jad.2021.09.098.
Lin YH, Chen CY, Wu SI. Efficiency and quality of data collection among public mental health surveys conducted during the COVID-19 pandemic: Systematic review. Journal of Medical Internet Research. 2021;23(2). https://doi.org/10.2196/25118.
Czeisler M, Wiley J, Czeisler C, Rajaratnam S, Howard M. Uncovering survivorship bias in longitudinal mental health surveys during the CoviD-19 pandemic. Epidemiol Psychiatr Sci. 2020. https://doi.org/10.1017/S204579602100038X.
Keyes CLM. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J Consult Clin Psychol. 2005;73(3):539–48. https://doi.org/10.1037/0022-006X.73.3.539.
Prati G, Mancini AD. The psychological impact of COVID-19 pandemic lockdowns: a review and meta-analysis of longitudinal studies and natural experiments. Psychol Med. 2021;51(2):201–11. https://doi.org/10.1017/S0033291721000015.
Buecker S, Horstmann KT. Loneliness and social isolation during the COVID-19 pandemic: a systematic review enriched with empirical evidence from a large-scale diary study. Eur Psychol. 2021;26(4):272–84. https://doi.org/10.1027/1016-9040/a000453.
Kaniasty K. Social support, interpersonal, and community dynamics following disasters caused by natural hazards. Curr Opin Psychol. 2020;32:105–9. https://doi.org/10.1016/j.copsyc.2019.07.026. Epub 20190718. Cited in: Pubmed; PMID 31445427.
Australian Bureau of Statistics. Household Impacts of COVID-19 Survey. 2021 27 January 2022. Available from: https://www.abs.gov.au/statistics/people/people-and-communities/household-impacts-covid-19-survey/latest-release.
Australian Institute of Health and Welfare. Suicide & self-harm monitoring. Australian Institute of Health and Welfare; 2022. [10 January 2022]. Available from: https://www.aihw.gov.au/suicide-self-harm-monitoring/data/covid-19. Accessed 21 January 2022.
Batterham PJ, Calear AL, McCallum SM, Morse AR, Banfield M, Farrer LM, Gulliver A, Cherbuin N, Rodney Harris RM, Shou Y, Dawel A. Trajectories of depression and anxiety symptoms during the COVID-19 pandemic in a representative Australian adult cohort. Med J Aust. 2021;214(10):462–8. https://doi.org/10.5694/mja2.51043.
Batterham PJ, Calear AL, Shou Y, Farrer LM, Gulliver A, McCallum SM, Dawel A. Effects of the COVID-19 pandemic on suicidal ideation in a representative Australian population sample–Longitudinal cohort study. J Affect Disord. 2022;300:385–91. https://doi.org/10.1016/j.jad.2022.01.022.
Calear AL, McCallum S, Morse AR, Banfield M, Gulliver A, Cherbuin N, Farrer LM, Murray K, Rodney Harris RM, Batterham PJ. Psychosocial impacts of home-schooling on parents and caregivers during the COVID-19 pandemic. BMC Public Health. 2022;22(1). https://doi.org/10.1186/s12889-022-12532-2.
Reifels L, Mills K, Duckers MLA, O’Donnell ML. Psychiatric epidemiology and disaster exposure in Australia. Epidemiol Psychiatr Sci. 2019;28(3):310–20. https://doi.org/10.1017/S2045796017000531. Epub 20170927. Cited in: Pubmed; PMID 28950925.
Bryant RA, Gallagher HC, Gibbs L, Pattison P, MacDougall C, Harms L, Block K, Baker E, Sinnott V, Ireton G, Richardson J, Forbes D, Lusher D. Mental Health and Social Networks After Disaster. Am J Psychiatry. 2017;174(3):277–85. https://doi.org/10.1176/appi.ajp.2016.15111403. Epub 20161114. Cited in: Pubmed; PMID 27838935.
Gallagher HC, Block K, Gibbs L, Forbes D, Lusher D, Molyneaux R, Richardson J, Pattison P, MacDougall C, Bryant RA. The effect of group involvement on post-disaster mental health: a longitudinal multilevel analysis. Soc Sci Med. 2019;220:167–75. https://doi.org/10.1016/j.socscimed.2018.11.006. Epub 20181107. Cited in: Pubmed; PMID 30447481.
ABC News. Melbourne marks 200 days of COVID-19 lockdowns since the pandemic began. 19 August 2021 ed. Australian Broadcasting Corporation; 2021 19 August 2021. Available from: https://www.abc.net.au/news/2021-08-19/melbourne-200-days-of-covid-lockdowns-victoria/100386078.
VicHealth Coronavirus Victorian Wellbeing Impact Study: Follow-up survey. Melbourne; 2020. Victorian Health Promotion Foundation.
Wright A, Shill J, Honey N, Jorm AF, Bolam B. The VicHealth Indicators population survey: methodology, prevalence of behavioural risk factors, and use in local policy. BMC Public Health. 2020;20(1):1497. https://doi.org/10.1186/s12889-020-09605-5. Epub 20201002. Cited in: Pubmed; PMID 33008351.
Link M, Murphy J, Schober MF, Buskirk TD, Childs JH, Tesfaye CL. Mobile Technologies for Conducting, Augmenting and Potentially Replacing Surveys: Report of the AAPOR Task Force on Emerging Technologies in Public Opinion Research. American Association for Public Opinion Research; 2014. Available from: https://www.aapor.org/Education-Resources/Reports/Mobile-Technologies-for-Conducting,-Augmenting-and.aspx. [Cited 3 May 2022].
Furukawa TA, Kessler RC, Slade T, Andrews G. The performance of the K6 and K10 screening scales for psychological distress in the Australian national survey of mental health and well-being. Psychol Med. 2003;33(2):357–62. https://doi.org/10.1017/S0033291702006700. Epub 2003/02/14.
Cummins RA, Eckersley R, Pallant J, van Vugt J, Misajon R. Developing a national index of subjective wellbeing: the Australian unity wellbeing index. Soc Indic Res. 2003;64(2):159–90. https://doi.org/10.1023/A:1024704320683.
Anglim J, Weinberg MK, Cummins RA. Bayesian hierarchical modeling of the temporal dynamics of subjective well-being: a 10 year longitudinal analysis. J Res Pers. 2015;59:1–14. https://doi.org/10.1016/j.jrp.2015.08.003.
Nicholson M, O'Halloran P. Establishing a Single Item Measure of Social Connectedness: A Research Report Prepared for VicHealth. Melbourne; 2019. Victorian Health Promotion Foundation.
Hawdon J, Räsänen P, Oksanen A, Ryan J. Social solidarity and wellbeing after critical incidents: three cases of mass shootings. J Crit Incident Anal. 2012;3(1):2–25.
StataCorp. Stata Statistical Software: Release 17. College Station, TX: StataCorp LP; 2021. Available from: http://www.stata.com/. [3 May 2022].
R Core Team. R: A language and environment for statistical computing. . Vienna, Austria: R Foundation for Statistical Computing; 2021. Available from: https://www.R-project.org/. [3 May 2022].
Rothman KJ, Greenland S, Lash TL. Modern epidemiology. 3rd ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008. x, 758 p. p. ISBN: 97807817556410781755646. Publisher description http://www.loc.gov/catdir/enhancements/fy0743/2007036316-d.html Table of contents only http://www.loc.gov/catdir/enhancements/fy0828/2007036316-t.html.
Shrier I, Platt RW. Reducing bias through directed acyclic graphs. BMC Med Res Methodol. 2008;8(1):70. https://doi.org/10.1186/1471-2288-8-70.
Hosmer DW, Lemeshow S, Cook ED. Applied Logistic Regression. 2nd ed. New York: John Wiley & Sons, Inc.; 2000.
Wasserstein RL, Lazar NA. The ASA statement on p-values: context, process, and purpose. Am Stat. 2016;70(2):129–33. https://doi.org/10.1080/00031305.2016.1154108.
Chen H, Cohen P, Chen S. How Big is a Big Odds Ratio? Interpreting the magnitudes of odds ratios in epidemiological studies. Commun Stat - Simul Comput. 2010;39(4):860–4. https://doi.org/10.1080/03610911003650383.
Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry. 2002;65(3):207–39. https://doi.org/10.1521/psyc.65.3.207.20173. Cited in: Pubmed; PMID 12405079.
Acknowledgements
Nikki Honey, Anna Truong, Jason Marriot, Jane Shill, VicHealth staff, VicHealth COVID-19 Response Research Advisory Group
Funding
This survey was funded by VicHealth. AW held a position at VicHealth at the time of the survey, the views expressed in this paper are those of the author rather than her current affiliation.
Author information
Authors and Affiliations
Contributions
AW led the design of the survey and acquisition of data, and co-led the conception and design of the study, interpretation of the data and the drafting of the manuscript and contributed to the analysis of data. ADL co-led the design of the study, the analysis of data, interpretation of the data and the drafting of the manuscript. KHL and CH contributed to the analysis of the data, interpretation of the data and the drafting of the manuscript. MN and LG contributed to the design of the survey, interpretation of data and drafting of manuscript. AJ contributed to writing the manuscript, planning of data analysis and interpretation of the findings. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The survey was approved by the Australian National University’s Human
Research Ethics Committee (Approval number 2020/264 and 2020/540). Online written informed consent was obtained from study participants as this survey was carried out as an online survey. This method of consent was approved by the Australian National University’s
Human Research Ethics Committee. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
VicHealth Coronavirus Victorian Wellbeing Impact Survey Questionnaire.
Additional file 2:
Table S1. Cohort characteristics at the first lockdown & the second lockdowns. Table S2. Baseline characteristics of the cohort with and without missing at the second lockdown. Table S3. Results from univariable logistic regression modelling with psychological distress and life satisfaction asoutcome at the first lockdown**. Table S4. Results from univariable logistic regression modelling with psychological distress and life satisfaction as outcome at the second lockdown**. Table S5. Longitudinal associations of change in psychological distress and life satisfaction between the first and the second lockdowns**.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wright, A., De Livera, A., Lee, K.H. et al. A repeated cross-sectional and longitudinal study of mental health and wellbeing during COVID-19 lockdowns in Victoria, Australia. BMC Public Health 22, 2434 (2022). https://doi.org/10.1186/s12889-022-14836-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-14836-9