
Abstract
Background
In addition to the threat of the COVID-19 pandemic to physical health, mental health is challenged by the emotional response to the situation and the official measures taken to stop the pandemic. This study aimed to assess the prevalence of impaired mental well-being due to COVID-19 and explore associated factors.
Methods
The study was an observational, population-based, nationwide, cross-sectional online survey of a representative sample of the general Swiss population performed between March and April 2020. Participants reported on mental well-being, self-isolation/quarantine, their risk for developing severe COVID-19, and their work situation. Multivariable logistic regression analyses assessed risk factors for impaired mental well-being due to the pandemic.
Results
Data from 1022 individuals were analysed. The median age was 44 years (range 18 to 78) and 49% were women. A third of respondents reported that the COVID-19 pandemic impaired their mental well-being and almost half reported specific mental health concerns. Impaired mental well-being was associated with having health problems (OR = 1.88, 95% CI: 1.29–2.74, vs no problems), being or living with someone at risk for severe COVID-19 (OR = 1.38, 95% CI: 1–1.9,), smoking (OR = 1.8, 95% CI: 1.24–2.61), living in urban residential environments (OR = 1.62, 95% CI: 1.13–2.32, vs rural), not being able to work due to closed workplace (OR = 1.66, 95% CI: 1.04–2.67), aged between 18 and 29 years old (OR = 1.99, 95% CI: 1.32–3.01, vs 45 to 59 years old), and living in a single household (living with someone, OR = 0.65, 95% CI: 0.44–0.97,vs single household). Overall, the most significant covariates of impaired mental well-being were specific mental health concerns: feeling depressed (OR = 7.21, 95% CI: 4.5–11.55), feeling less pleasure in doing things than before (OR = 6.28, 95% CI: 4.1–9.62), feeling anxious (OR = 6.13, 95% CI: 3.91–9.59) and feeling lonely (OR = 4.08, 95% CI: 2.53–6.58).
Conclusion
Impaired mental well-being can carry long-term consequences. We encourage policymakers to implement strategies to promote mental health during this pandemic situation. Special attention should be addressed to the youngest, those at risk for severe COVID-19 and those with government-imposed work restrictions.
Similar content being viewed by others


Introduction
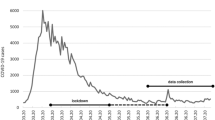
During the first outbreak of the COVID-19 pandemic, governments all over the globe had to restrict activities of daily life to avoid the further spread of the disease [1,2,3]. In Switzerland and other countries, the authorities requested the population to follow hygiene and physical distancing rules. On March 16th, 2020, the Swiss federal government declared a state of emergency due to COVID-19 and imposed severe disease control measures, including the closure of schools, universities, shops, and other businesses, as well as sports, cultural events, and club activities [4]. This lockdown lasted until the withdrawal of the first measures on April 27th. During the lockdown period, up to 17 new cases of SARS-CoV-2 per 100,000 inhabitants were reported each day in Switzerland [5]. Because of this high incidence, it was impossible to test each suspected case and trace their contacts. Persons with respiratory symptoms or fever were advised to undergo a 10-day self-isolation period, and those who had had contact with someone with a positive test for SARS-CoV-2 were strictly recommended to undergo a 10-day period of self-quarantine [6].
Measures to control disease affect daily life, and impact the population’s mental health state [7]. Research shows that pandemics can lead to high levels of stress resulting in mental health problems, such as anxiety, symptoms of depression, insomnia, denial, anger, and fear [8], affecting the general population, healthcare workers, and clinical populations [9,10,11,12,13]. Quarantine heightens feelings of uncertainty and isolation. These feelings are coupled with efforts to cope with the situation within the restrictions imposed by the quarantine itself [14], which include but are not limited to lack of mobility, change of routines, changes in working patterns, and loss of social support [15]. Furthermore, psychological side effects of quarantine and social distancing may include post-traumatic stress, confusion, anger, and symptoms of depression [16,17,18]. Projections with Swiss data have estimated 0.205 years of life lost due to psychosocial consequences of the COVID-19 disease control measures [19]. Likewise, stress and depression during quarantine induce changes in diet and physical activity, which can have a detrimental impact on physical health [20]. In particular, an unhealthy lifestyle coupled with anxiety increases the risk of long-term cardiovascular disease [20, 21].
Collecting high-quality data on the mental health effects driven by the COVID-19 pandemic was outlined in a recently published position paper by Holmes and colleagues as an immediate priority for mental health research in response to the pandemic [22]. Reliable evidence on the mental health effects of the pandemic is paramount to understand the population’s needs and inform current and future interventions to support mental well-being (particularly in vulnerable groups). These interventions would include all attempts to improve mental health, like population-level policy, occupational health guidelines, and psychological interventions [22].
Thus, the current study aimed to explore how the COVID-19 pandemic broadly affected the mental well-being of the general population in Switzerland. We were interested in well-being as the complete and broad concept of mental health, to which everyone could relate. The World Health Organization defines mental health as an integral part of health, characterised by a state of well-being, in which the person can realize his or her abilities, cope with the stresses of life, be productive and contribute to his or her community [23]. More specifically, and as defined in the literature ‘well-being refers to how people experience and evaluate their lives and specific domains and activities in their live’ [24]. Usually, the concept of well-being relates to health and how well a person’s life is going for that particular person [25]. Therefore, mental well-being is paramount for the complete state of health of the individual and the community. Further, we were interested in assessing demographic, health, and work-related factors associated with impaired mental well-being to better understand which sub-groups of the general population were most affected by the pandemic. This information would be useful for physicians and policymakers to know to which groups would be worth to focus their attention and explore mental well-being, with the aim to improve this aspect of public health during the pandemic and beyond.
Methods
Sample selection and data collection
Between March and April 2020, the LINK Institute Lucerne, Switzerland (https://www.link.ch) invited 4110 persons to participate in the Web-based survey to acquire 1000 complete and valid surveys. For 1000 interviews, the sampling error at a 95% confidence interval lies within +/− 3.2% for a percentage of 50% reporting “yes” in a yes/no poll. This sample size enables meaningful analyses between different socio-demographic groups.
Participants were part of the LINK online panel consisting of 115,000 active members. All participants regularly take part in studies, and when a contact is incorrect or ineligible it is removed. No self-selection is possible in the panel, as participants cannot register themselves in the LINK Institute, but the Institute contacts them specifically. The consent to participate in surveys is signed when participants declare themselves available and part of the online panel. Also, they consent when they choose to complete each specific survey.
Participants were selected with quota sampling. They were stratified according to population data from the Federal Statistical Office [26] with quotas based on sex, age (18 to 29, 30 to 44, 45 to 59, and 60 to 79 years old), and language region (German, French and Italian speaking). For example, quota 1 included men between 18 and 29 years old from the German-speaking region. Quota 2 included men between 30 and 44 years old from the German-speaking region, and so on and so forth. Within each quota participants selection was made at random. Additionally, to collect enough interviews per quota, each one was oversampled by 5%.
Demographic weighting
After data collection, random iterative method (Rim) weighting [27, 28], also known as raking [29], was applied to adjust the survey sample weights to the population for age, sex and language region. This correction adjusts the weights on the specified characteristics until they matched the corresponding proportions (marginal totals) of the population, therefore ensuring that the sample was representative of the general population. This iterative weighting method is efficient for adjusting a survey sample for more than two variables simultaneously with their interlocking quotas. It starts adjusting one variable and then uses the previous adjusted results as the initial values for the next iteration. The process repeats until results converge [30].
Survey design
The study was an observational, population-based, nationwide, cross-sectional online survey.
Potential participants were sent an invitation by email with the link to the online survey. The invitation specified that if they were part of the target population (as assessed by a few questions at the beginning of the survey), the survey would take about 5 min to complete.
Upon accessing the survey, programmed with IBM® SPSS® Data Collection V7.0 [31], participants read about the department running the survey and the topic (health during the COVID-19 pandemic). Then, they were reminded about data protection and that the data was collected anonymously. By clicking, they agreed to participate in the study, and the survey began.
The questionnaire was fully structured with semi-open and closed questions (see Supplementary Materials). Where relevant, the question had a time reference to the last 2 months (corresponding to the first COVID-19 pandemic wave in Switzerland). Alternatively, some questions referred explicitly to the COVID-19 situation.
Mental well-being questions
Participants responded to “Does the current COVID-19 situation impair your mental/emotional well-being?”. This question was naturally worded and easy to understand. It was developed given the lack of standardized tools to assess subjective mental well-being during this pandemic. Alongside, participants also responded to questions relating to specific mental health concerns adapted from two mental health screening tools. From the Patient Health Questionnaire-2 [32, 33] we used the questions a) feeling down or depressed, b) having less interest or pleasure in doing things. The Patient Health Questionnaire-2 was developed to assess the frequency of depressed mood and anhedonia over the past 2 weeks as a first screening approach for depression. Scoring of this questionnaire ranges from 0 to 6 (each question is scored from 0 to 3 based in how frequent the person experiences the symptom, and the total score is the sum of both questions). When the person scores 3 or more it is recommended to follow up with a complete evaluation to assess the possible presence of depressive disorder. From the Generalized Anxiety Disorder-2 questionnaire [34] we developed the item: c) increased worries or feeling more anxious. Originally, the Generalized Anxiety Disorder-2 item has two questions. Scoring ranges from 0 to 6 (0 to 3 for each question, and total score the sum of both). This 2-item questionnaire is used as a first screening tool for generalized anxiety disorder. With a result of 3 or more it is recommended to evaluate the presence of a generalized anxiety disorder. Further, we also asked about d) increased feelings of loneliness. These questions referred to the period spanning the last 2 months. Respondents who indicated the presence of any of the four previous symptoms were then asked: “Did you get advice from a psychologist or physician for your mental health problems?” (yes/no).
General health questions
Respondents reported if they had health problems with the question: “Have you had any health problems in the last two months? These include serious illnesses but also minor illnesses, such as headaches, a cold or hay-fever” (possible answers: one health problem, more than one health problem, no health problems). They also responded to specific COVID-19 related questions: 1) if they were part of the population at risk for severe COVID-19 symptoms, as defined by the Swiss Federal Office of Public Health (age over 65 years, patients with cancer, high blood pressure, diabetes, cardiovascular disease, respiratory disease, and diseases that weaken the immune system [35], 2) if someone in their household was part of the population at risk for severe COVID-19, 3) if someone in their household had been in self-quarantine or self-isolation, or 4) if they were tested for COVID-19.
Demographics and employment questions
Regarding their employment situation, participants indicated whether they had to stop going to work due to COVID-19. If they had to stop going to work in-person, they chose the reason among the following options. a) they had to work from home, b) they had to stop working because the workplace was closed due to COVID-19 disease control measures (e.g., bars, restaurants, hairdressers, etc.), and it was not possible to work from home, c) they had to stop working because of childcare obligations due to closed day-care centres, d) they had to stop working for other reasons.
Demographic characteristics encompassed age, sex, smoking, household size (1,2, 3 or more people), residential environment (urban or rural), employment status (full-time employment, part-time employment or unemployed), and language region (German, French, or Italian).
Analyses
All analyses presented were performed on the weighted data in R [36]. The R package “survey” was used to analyse weighted data [37]. The functions of this R package perform weighted estimations, with each observation being weighted by the inverse of its sampling probability. To compute weighted cross-tabulations, we used the “svytable” function. The standard error of proportions was estimated using the functions “svytotal” or “svymean”. Confidence intervals for proportions were calculated using the R function svyciprop with the “likelihood” method which uses the (Rao-Scott) scaled Chi-squared distribution for the loglikelihood from a binomial distribution. We tested the association between impaired mental well-being due to COVID-19 (binary outcome, 1 = impaired, 0 = not impaired mental well-being) and demographic variables (age, sex, household size, urban/rural residential environment, employment status, language region), COVID-19 risk factors (smoking, being oneself or a family member part of the risk group for COVID-19, being in self-quarantine or self-isolation), mental health concerns (feeling lonely, worried or anxious, feeling down or depressed, feeling less pleasure in doing things than before), and changes at work due to COVID-19. For this purpose, we fitted univariable and multivariable generalised linear models of the binomial family to the data with inverse-probability weighting and design-based standard errors using the function “svyglm”. To check for multicollinearity, we performed a bivariate correlation matrix with all covariates using the function “hetcor” from the R package “polycor”. Variance-inflation factors (VIF) for generalized linear models were calculated using the function “VIF” of the R package “DescTools”. The highest VIF value for the model is indicated in the table legend.
Results
Weighting
Demographic respondent weightings ranged between a minimum weight of 0.82, and a maximum of 1.36, with 99.8% efficiency, values indicative of a well-balanced and reliable sample [38, 39].
Participants
From 4110 initially contacted people, 1022 (24.9%) completed the survey. The median age of the weighted sample was 44 years (IQR = 33 to 58, range = 18 to78), and 51% were male. Per regions, 72% were German-speaking, 24% French-speaking, and 4% Italian-speaking respondents. Table 1 shows the demographic characteristics of the sample. Regarding employment, 75% were employed, and among them 47% stopped going to work, mainly because it was recommended that they work from home (27%) or because their workplace was closed due to COVID-19 (14%, see Table 2).
How many people were affected directly or indirectly by COVID-19?
Regarding the population at risk, 391 people or 38% of respondents or their co-habitants were at risk of severe COVID-19 symptoms (Table 2). However, only 59 people, or 5.9%, had been in self-isolation or self-quarantine due to COVID-19. Six respondents had a positive test result for COVID-19.
Impaired mental well-being due to COVID-19
Thirty-four percent of the interviewed population reported that the pandemic impaired their mental well-being. Further screening questions for mental health concerns revealed that 56% of the whole population showed some signs of impaired mental health (feeling lonely, feeling worried or anxious, feeling down or depressed, or feeling less pleasure in doing things than before, see Table 2). Respondents reporting impaired well-being due to the COVID-19 pandemic were significantly more likely to additionally report mental health concerns than respondents not reporting impaired mental well-being (Chi-square test = 350, P < 0.001, see Table 1 in Supplementary materials). In those with impaired well-being due to COVID-19, 57% felt anxious or worried, 49% felt lonely, 62% felt down or depressed, and 60% lost interest or pleasure in doing things. In those without impaired well-being due to COVID-19, 14% felt anxious or worried, 13% lost interest or pleasure in doing things, 10% felt lonely, and 10% felt down or depressed. Considering those respondents who reported at least one of the four mental health concerns 8% (45 out of 570 people) contacted a psychologist or physician due to their mental health problems.
Association of mental health with demographic variables, COVID-19 risk factors, and work situation
Figure 1 presents the proportion of impaired mental well-being across demographic characteristics, COVID-19 risk factors, mental health, and employment-related variables. Table 3 shows the results of a multivariable regression model explaining impaired mental well-being by demographic, health, and employment variables. The likelihood of reporting impaired mental well-being due to COVID-19 was highest in the young, in urban dwellers (vs. rural), in people with health problems (several health problems vs. none), in people being or living with someone at risk of severe COVID-19, in smokers, and people who had to stop working because their workplace was closed due to official disease control measures. In comparison, characteristics associated with a smaller likelihood to report impaired well-being include older age or living in a household of two or more people (compared to living alone).

Proportion of people reporting impaired mental well-being due to the COVID-19 pandemic across demographic, health and work-related factors for all participants (N = 1022). Legend: * = P-value < 0.05, ** = P-value < 0.01, *** = P-value < 0.001. Stopped work = those who stopped work due to imposed disease control measures, Childcare = those who stopped working to care for their children
Table 4 presents a multivariable regression model including all independent variables from the previous model and the four mental health concerns. The likelihood of impaired mental well-being was most likely in those respondents being or living with someone at risk for severe COVID-19 symptoms and those reporting any of the four mental health concerns (feeling lonely, feeling worried or anxious, feeling down or depressed, or feeling less pleasure in doing things).
Discussion
This study highlighted how the first wave of the COVID-19 pandemic broadly impaired the mental well-being of the general Swiss population. Precisely, one-third (34%) of respondents reported impaired mental well-being. Variables associated with impaired mental well-being were being young, being at risk for a severe outcome, having one or more health problems, smoking, living in a single household, and stopping work due to disease control measures.
Our finding is coherent with another study conducted in Switzerland by de Quervain and colleagues focusing on stress. Their study collected data at two time points: the beginning of lockdown and during the partial lifting of lockdown measures. They focused on changes in stress levels and symptoms of depression. The comparative time point between the two studies is the beginning of lockdown. They found that about half of their sample (49.6%) had increased stress during confinement compared to stress levels before the COVID-19 pandemic. Respondents also reported a 57% increase in symptoms of depression, which were highly correlated with the changes in stress. The authors identified several reasons for the increased stress levels, such as changes at work, problems with childcare, or not being able to spend time with others [40]. In our study, we also found a significant association with increased impaired mental well-being in those respondents who could not go to work because the workplace was closed as mandated by the government. Our results are also comparable with findings from the UK, Spain, and Italy during the first wave lockdown (between April 24th and May 1st). There, around 43% of the population was expected to be at risk of stress, anxiety, and depression [41]. Perhaps because of the stricter lockdown measures imposed on those countries, the proportion of impaired mental health was higher. For example, Spain had hard confinement with internal travel restrictions, and with strict stay-at-home requirements. The population was allowed to leave home only to go to the grocery store, the doctor or the pharmacy. These restrictions were also valid for children. Meanwhile, in Switzerland stay at home was also expected but was not enforced and remained a recommendation from the authorities appealing to the citizens’ sense of personal responsibility. Likewise, it was recommended to self-isolate and self-quarantine as necessary. Additionally, closures of public spaces and restrictions to freedom of movement were the responsibility of the Cantons, and the Federal Government did not impose a general rule for the whole country [4, 42,43,44]. We were further able to highlight the characteristics of those respondents who self-rated their mental well-being as impaired.
Demographic covariates of impaired mental well-being: age, residential environment and, household size
Older people had a smaller likelihood to report impaired mental well-being due to COVID-19 than younger people. In comparison, people aged between 18 and 29 had a doubling in the odds of reporting impaired mental well-being than respondents between 45 and 59 years old (OR = 1.99, P = 0.001). This finding is consistent with the literature showing older age as a resilience factor for mental well-being [40, 45,46,47,48] and younger age as a predictor for poor mental health and well-being [49, 50]. According to Pro Juventute, a charitable foundation in Switzerland, its helpline has registered increasing demand from young people. Psychological consultations increased 40% between October and December 2020 compared to the same period last year. Their survey indicated that nearly 60% of 15–34-year-olds felt isolated and alone in society, more than any other age group [51].
Regarding the type of residential environment, we found that urban living was associated with a 62% increase in the odds of reporting impaired mental well-being (OR = 1.62, P = 0.008) compared to living in a rural environment. The environmental and social conditions of urban areas might challenge mental well-being. On the one hand, urban areas provide more opportunities for socializing, education, culture, work, and easier access to health care. On the other hand, urban-living includes easier access to drugs, exposure to crime and violence, poverty, pollution, traffic, loneliness, and a consequent higher need for stress processing [52, 53]. To these life challenges occurring during everyday life, we have to add the restrictions imposed by the government during the lockdown and the higher risk of SARS-CoV-2 infection [54].
We also found that respondents living with more people reported less impaired mental well-being than those living in single households. For example, respondents living in a household of two people had a 35% lower odds of reporting impaired mental well-being than those living alone (OR = 0.65, P = 0.036). This protective effect of living with more people corresponds to other studies showing a potential association between living alone and low positive mental health (defined as comprising both hedonic and eudaimonic elements of mental wellbeing) as shown in a systematic review of studies published between 2014 and 2017 [55]. During the pandemic, this might be especially important as people might fear spending the period of self-quarantine or self-isolation alone at home [56].
Health covariates of impaired mental well-being: risk for severe COVID-19, smoking, and health problems
Our study showed that participants at risk of severe COVID-19 or sharing their household with someone at risk for severe COVID-19, had a 38% higher odds of reporting impaired mental well-being than participants not in this situation (OR = 1.38, P = 0.05). These results correspond with literature showing chronic medical conditions as risk factors for anxiety and depression [57, 58], and therefore impaired mental well-being.
Regarding smoking, our results are in line with other studies that show that smoking is associated with poor mental health [49]. Smokers in our study were more likely to report impaired mental well-being than non-smokers (OR = 1.8, P = 0.002). There is some contradictory evidence in the literature regarding the effect of smoking on COVID-19 infection severity. A preliminary meta-analysis suggested that active smoking was not significantly associated with the severe progression of COVID-19 [59]. Nevertheless, increasing evidence indicates that smoking is more prevalent among severe cases of COVID-19 and probably also COVID-19 related deaths [60]. In addition, risk factors for a severe COVID-19 outcome are often present in smokers, i.e., lung and cardiovascular disorders [61].
We found that respondents with more health problems were more likely to report impaired mental well-being than their counterparts with no health problems (OR = 1.88, P = 0.001). This was expected, as physical and mental health are both considered by the World Health Organization (WHO) as integral dimensions of health and well-being [62], and they are dynamically related [63, 64].
Employment-related covariates of impaired mental well-being
Considering only the employed population, respondents who had to stop going to work due to a closed workplace had a 66% increased odds of reporting impaired mental well-being than other employed respondents who could continue going to work (OR = 1.66, P = 0.035). Beyond the physical infection, the pandemic brings along also economic effects derived from changes in the work situation that might trigger worries about losing one’s job, and therefore falling into a challenging personal financial situation and ultimately contributing to higher income inequality in society. Evidence suggests that this inequality affects population health and well-being and that this is most likely mediated through psychological stress (which leads to impaired general health and depression) [65, 66].
Access to mental health interventions and contact restrictions
Access to mental health care was diminished due to the COVID-19 pandemic disruption of services around the world. Factors that affect mental health services include, among others, risk of infection in long-stay institutions, barriers to meeting in-person or even reduction of available mental health professionals due to infection [67]. Given the need to reduce personal interactions, online mental health services start to be widely accepted internationally [12] and are well suited to providing access to health services without carrying any risk of infection [68]. In Switzerland, psychiatric and psychological ambulatory care providers seem to have maintained the same level of service during the lockdown as before the pandemic, thanks to the government measures to finance teleconsultations [69]. Remote sessions allowed service-provision while complying with the need for physical distancing. Simultaneously, there was an increase in demand for psychological support, especially from the younger citizens [70], with some services reporting a 12% increase in calls compared to the previous year [71]. Furthermore, we need to consider that depending on the evolution of the pandemic (i.e., duration and economic consequences), it is possible that still more people than usual will need psychosocial support, and this support would be most efficient when delivered through different channels. As reported by the Swiss Federal Office of Public Health, different generations, for example, tend to seek information and support in different ways: older residents tend to use the phone, the internet is mostly used by those in their middle age, and the younger tend to prefer mobile apps [72], chat, email or SMS [69].
Promotion of mental well-being
Depending on how strict the governmental lockdown measures are, the promotion and support of mental health during a pandemic might become necessary. Strategies to cover pandemic-related mental health difficulties include the long-term maintenance of helplines for mental health support (in Switzerland currently financed by the Federal Office of Public Health) and the creation of new ones. New helplines could be advertised through several media (radio, TV, social media) to reach all population segments. Other strategies could involve increasing the support offered by psychiatric and psychotherapeutic care entities, especially as patients with previous mental illnesses are vulnerable to further impairment of their well-being during the pandemic. Besides, also mental health care could be further supported by general practitioners and pediatricians. Our findings suggest that public health initiatives providing social support and information about where to get help and remain connected (e.g., via helplines) should target particularly young people, people at risk for severe COVID-19, and those with an insecure financial situation as a result of the lockdown. As suggested by Gloster et al., [73], interventions that promote psychological flexibility may alleviate the negative mental health consequences of the pandemic. Gloster et al., exemplify psychological flexibility as holding one’s thoughts lightly, be accepting of one’s experiences, engage in what is important to one despite challenging situations. On the economic level, those whose finances have worsened because of the pandemic measures should get quick and uncomplicated financial aid.
Limitations
The study was conducted in Switzerland and given cultural differences among countries, and the reactions of their governments to the pandemic, results might not be generalisable to populations other than the Swiss one. Within Switzerland, we also found differences among language regions. Residents from the Italian-speaking region reported significantly less impaired mental well-being than those from the German-speaking region. This result seems to reflect the cultural differences between regions in Switzerland, which we wanted to control for.
Also, the cross-sectional nature of the study has certain limitations. To be able to generalise results to the population the study sample has to be representative. For a population of about 8 million people and a survey sample of 1022 individuals, sampled at random per quotas from a very extensive panel, we estimated a margin of error of +/− 3.2% (for questions with two possible answers). Further, results were weighted based on age, sex, and language-speaking region data published by the Federal Office of Public Health, therefore ensuring that the sample was representative of the general population of Switzerland. Also, it is to be acknowledged that a cross-sectional design does not allow us to establish causal relationships, and thus our results show the strength of associations.
This study focused on self-reported impaired well-being during the lockdown during March and April 2020, using a simple question formulated to be understood by everyone. However, this question has not yet been validated. To validate this question it would be interesting to investigate objective measures of well-being, during the same period or even long-term, given that psychological effects after a pandemic tend to last long-term [74, 75]. Nonetheless, we found a strong association between impaired mental well-being and the mental health concerns variables from validated instruments (namely feeling lonely, feeling worried or anxious, feeling down or depressed, or feeling less pleasure in doing things). This strong association (see Supplementary materials) suggests that the question about “impaired mental well-being” measured what we intended. It might have worked as a general well-being concept which included the emotional components of the four mental health concerns.
We highlight here the possibility that our question “Does the current COVID-19 situation impair your mental/emotional well-being? might feel leading to some readers. In hindsight, we think that it would have been appropriate to build this question in a more neutral way. For example, avoiding the word ‘impair’ directly in the question and perhaps rephrasing it as ‘influenced in any direction your mental well-being’. Consequently, we cannot completely exclude the possibility that our results might be biased given the structure of the question. Nevertheless, we do not think this is the case for the following reasons. (1) The COVID-19 pandemic, specially the first wave, had such an unprecedented and important impact in peoples’ lives, that we do not think anyone would be easily led by our question. On the one hand some people had their mental well-being challenged, while others felt a relieve from their daily habits. (2) The cross-tabulation between mental well-being and the screening questions (felt lonely, anxious, depressed, had less pleasure in doing things than before), shows significant differences in mental well-being between the group of participants who reported impaired mental well-being (who had significantly more symptoms) and the group reporting not-impaired mental well-being (less symptoms). This significant relationship between the variables is evidence that our main question was measuring mental well-being. It would have been suspicious if there were no significant differences between the groups. (3) Other studies, measuring different aspects of mental well-being found similar proportions of people affected [40, 41]. If our question would have been leading, then we can imagine that our results would have been inflated and a much higher proportion of the population would have reported impaired mental well-being.
Also, it would have been interesting to study the link between local area deprivation and mental well-being status. Local area deprivation indices measure certain socioeconomic conditions, including social and material disadvantages [76] in relatively small geographical areas [77]. Deprivation indices are usually associated with health outcomes [78] and therefore interesting to associate with measures of well-being. We could not calculate such an index with the current dataset, nor are we aware of such an index validated for Switzerland. Also, we did not control for other economic factors like respondent’s salary or household total income. Other studies in Switzerland have shown that there is an effect of economic deprivation in psychological well-being [79], and others have found that participants with a lower socio-economic profile have a low participation rate in health surveys [80]. Thus, we cannot exclude the possibility that our results are slightly biased and that the real impact of the first wave of COVID-19 pandemic was indeed even more challenging for the population.
It would have been interesting to ask those two-thirds of respondents who did not report impaired mental well-being, how they felt. Other studies have shown some people remained neutral, while for others the pandemic brought a situation to stress relief compared to their lives before the pandemic [40]. Given the importance of resilience, it would have also been interesting to ask about factors that people consider useful to keep physically and mentally healthy while facing stressful life events.
Conclusion
We studied self-reported mental well-being status during the first wave of the COVID-19 pandemic in a representative sample of the Swiss population. Impaired mental well-being was associated with younger age, urban residential environment, single household, health problems, being at risk for severe COVID-19 symptoms, smoking, and not being able to go to work because the workplace was closed as imposed by the government. Given the current figures on the effect of COVID-19 on mental well-being in the Swiss population, it seems necessary to increase the focus on mental well-being in the young and people at risk for COVID-19. Given the possible long-term consequences of impaired mental well-being, it is in the best interest of public health to promote and increase measures to improve the mental health of those populations. We, therefore, encourage policymakers to keep developing, funding, and implementing strategies for mental health assessment, support, treatment, and promotion during this extraordinary pandemic situation.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Brauner JM, Mindermann S, Sharma M, Johnston D, Salvatier J, Gavenčiak T, Stephenson AB, Leech G, Altman G, Mikulik V, Norman AJ, Monrad JT, Besiroglu T, Ge H, Hartwick MA, Teh YW, Chindelevitch L, Gal Y, Kulveit J. Inferring the effectiveness of government interventions against COVID-19. Science. 2021;371(6531):eabd9338. PMID: 33323424; PMCID: PMC7877495. https://pubmed.ncbi.nlm.nih.gov/33323424/, https://doi.org/10.1126/science.abd9338.
News B. Coronavirus: What measures are countries taking to stop it? - BBC News. [Internet]. [cited 2021 Apr 8]. Available from: https://www.bbc.com/news/world-51737226
Flaxman S, Mishra S, Gandy A, Unwin HJT, Mellan TA, Coupland H, et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature. 2020;584(7820):257–61 [cited 2021 Apr 8]. Available from: https://pubmed.ncbi.nlm.nih.gov/32512579/.
Burci GL, Hasselgard-Rowe J. Switzerland’s Response to the COVID-19 Pandemic | Bill of Health [Internet]. [cited 2021 Apr 20]. Available from: https://blog.petrieflom.law.harvard.edu/2020/05/14/switzerland-global-responses-covid19/
Federal Office of Public Heatlh F. Situation in Switzerland [Internet]. [cited 2020 Dec 1]. Available from: https://www.bag.admin.ch/bag/en/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/situation-schweiz-und-international.html#-1199962081
Federal Office of Public Heatlh F. Isolation and quarantine [Internet]. [cited 2020 Dec 2]. Available from: https://www.bag.admin.ch/bag/en/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/isolation-und-quarantaene.html
Pfefferbaum B, Schonfeld D, Flynn BW, Norwood AE, Dodgen D, Kaul RE, et al. The H1N1 crisis: a case study of the integration of mental and behavioral health in public health crises. Disaster Med Public Health Prep. 2012;6(1):67–71. [cited 2020 Dec 2]. Available from. https://doi.org/10.1001/dmp.2012.2.
Torales J, O’Higgins M, Castaldelli-Maia JM, Ventriglio A. The outbreak of COVID-19 coronavirus and its impact on global mental health [internet]. Int J Soc Psychiatry. 2020;66:317–20 [cited 2020 Dec 2]. SAGE Publications Ltd. Available from: https://pubmed.ncbi.nlm.nih.gov/32233719/.
Lee AM, Wong JGWS, McAlonan GM, Cheung V, Cheung C, Sham PC, et al. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can J Psychiatr. 2007;52(4):233–40.
Sønderskov KM, Dinesen PT, Santini ZI, Østergaard SD. The depressive state of Denmark during the COVID-19 pandemic. Acta Neuropsychiatr. 2020;1 [cited 2020 Sep 28]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7176490/.
Li S, Wang Y, Xue J, Zhao N, Zhu T. The impact of covid-19 epidemic declaration on psychological consequences: a study on active weibo users. Int J Environ Res Public Health. 2020;17(6) [cited 2020 Sep 28]. Available from: https://pubmed.ncbi.nlm.nih.gov/32204411/.
Talevi D, Socci V, Carai M, Carnaghi G, Faleri S, Trebbi E, et al. Mental health outcomes of the covid-19 pandemic. Riv Psichiatr. 2020;55(3):137–44.
Spoorthy MS. Mental health problems faced by healthcare workers due to the COVID-19 pandemic–a review. Asian J Psychiatr. 2020;51:102119. https://doi.org/10.1016/j.ajp.2020.102119 Elsevier B.V.; [cited 2020 Dec 2]. Available from.
Cava MA, Fay KE, Beanlands HJ, McCay EA, Wignall R. The experience of quarantine for individuals affected by SARS in Toronto. Public Health Nurs. 2005;22(5):398–406.
Banerjee D, Rai M. Social isolation in Covid-19: the impact of loneliness. Int J Soc Psychiatry. 2020;66:525–7 SAGE Publications Ltd; [cited 2021 Apr 14]. Available from: http://journals.sagepub.com/doi/10.1177/0020764020922269.
Reissman DB, Watson PJ, Klomp RW, Tanielian TL, Prior SD. Pandemic influenza preparedness: adaptive responses to an evolving challenge. J Homel Secur Emerg Manag. 2006;3(2):13 [cited 2020 Dec 2]. Available from: https://www.degruyter.com/view/journals/jhsem/3/2/article-jhsem.2006.3.2.1233.xml.xml.
Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. Rapid review the psychological impact of quarantine and how to reduce it: rapid review of the evidence. 2020;395 [cited 2020 Dec 2]. www.thelancet.com [Internet]. Available from: https://doi.org/10.1016/S0140-6736(20)30460-8.
Peterson JA, Chesbro G, Larson R, Larson D, Black CD. Short-term analysis (8 weeks) of social distancing and isolation on mental health and physical activity behavior during COVID-19. Front Psychol. 2021;12 [cited 2021 Apr 13]. Available from: https://pubmed.ncbi.nlm.nih.gov/33815233/.
Moser DA, Glaus J, Frangou S, Schechter DS. Years of life lost due to the psychosocial consequences of COVID-19 mitigation strategies based on Swiss data. Eur Psychiatry. 2020;63(1) [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/32466820/.
Mattioli AV, Sciomer S, Cocchi C, Maffei S, Gallina S. Quarantine during COVID-19 outbreak: changes in diet and physical activity increase the risk of cardiovascular disease. Nutr Metab Cardiovasc Dis. 2020;30:1409–17 Elsevier B.V.; [cited 2021 Apr 13]. Available from: /pmc/articles/PMC7260516/.
Ghozy S, Abdelaal A, Shah J, Parker KE, Islam SMS. COVID-19 and physical inactivity: teetering on the edge of a deadlier pandemic? J Glob Health. 2021;11:2021 [cited 2021 Apr 13]. Available from: /pmc/articles/PMC7914401/.
Holmes EA, O’Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. 2020;7:547–60 Elsevier Ltd; [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/32304649/.
World Health Organization W. Mental health: strengthening our response [Internet]. [cited 2021 Apr 13]. Available from: https://www.who.int/en/news-room/fact-sheets/detail/mental-health-strengthening-our-response
Stone AA, Mackie C, Framework P on MSW-B in a, Policy-Relevant, Statistics C on N, et al. In: Arthur AS, Mackie C, editors. Subjective well-being measuring happiness, suffering, and other dimensions of experience [internet]. Washington, D.C.: National Academies Press; 2013. [cited 2021 Jun 15]. Available from: http://www.nap.edu/catalog/18548.
Crisp R. Well-being. In: Edward NZ, editor. Stanford encyclopedia of philosophy. [Internet]. [cited 2021 Jun 15]. Available from: https://plato.stanford.edu/archives/fall2017/entries/well-being/.
Federal Statiscal Office B. Permanent and non-permanent resident population by institutional units, citizenship (category), sex and age - 2010-2018 | Table | Federal Statistical Office [Internet]. [cited 2020 Dec 2]. Available from: https://www.bfs.admin.ch/bfs/en/home/statistics/catalogues-databases/tables.assetdetail.9566416.html
Sharot T. Weighting survey results. J Mark Res Soc. 1986;28(3):269–84.
Little RJA, Wu M-M. Models for contingency tables with known margins when target and sampled populations differ. J Am Stat Assoc. 1991;86(413):87.
Kalton G. Compensating for missing survey data. Univ. of Michigan, Survey Res. Center, Inst. for Social Res.; 1983. (Research report series / Institute for Social Research).
Kalton G, Flores CI. Weighting methods. J Off Stat. 2003;1:19.
IBM SPSS Data Collection V7.0 [Internet]. [cited 2021 Mar 23]. Available from: https://www.01.ibm.com/common/ssi/ShowDoc.wss?docURL=/common/ssi/rep_ca/9/897/ENUS213-069/index.html&request_locale=en
Kroenke K, Spitzer RL, Williams JBW. The patient health questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–92 [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/14583691/.
Spitzer RL, Kroenke K, Williams JBW. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. J Am Med Assoc. 1999;282(18):1737–44 [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/10568646/.
Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007;146(5):317–25 [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/17339617/.
The Federal Council T portal of the S government. CC 818.101.24 Ordinance 3 of 19 June 2020 on Measures to Combat the Coronavirus (COVID-19) (COVID-19 Ordinance 3). [Internet]. [cited 2020 Dec 2]. Available from: https://www.admin.ch/opc/en/classified-compilation/20200744/index.html
R Core Team. R: a language and environment for statistical computing [internet]. Vienna: Foundation for Statistical Computing; 2019. Available from: https://www.r-project.org/
Lumley T. Survey: analysis of complex survey samples; 2020.
Deming WE, Stephan FF. On a least squares adjustment of a sampled frequency table when the expected marginal totals are known. Ann Math Stat. 1940;11(4):427–44 [cited 2021 Jun 15]. Available from: http://projecteuclid.org/euclid.aoms/1177731829.
Pfeffermann D, Rao CR. Sample Surveys: Design, Methods and Applications, Volume 29A - 1st Edition. North Holland; 2009. [cited 2021 Jun 15]. Available from: https://www.elsevier.com/books/sample-surveys-design-methods-and-applications/pfeffermann/978-0-444-53124-7
de Quervain D, Aerni A, Amini E, Bentz D, Coynel D, Gerhards C, et al. The Swiss Corona stress study; 2020. [cited 2020 Dec 2]; Available from: https://osf.io/jqw6a/
Codagnone C, Bogliacino F, Gómez CE, Charris RA, Montealegre F, Liva G, et al. Assessing concerns for the economic consequence of the COVID-19 response and mental health problems associated with economic vulnerability and negative economic shock in Italy, Spain, and the United Kingdom. 2020. [cited 2020 Dec 7]; Available from: https://osf.io/preprints/socarxiv/x9m36/
Gobierno de España. Crisis sanitaria COVID-19 - Atención e información - Inicio [Internet]. [cited 2021 Apr 14]. Available from: https://administracion.gob.es/pag_Home/atencionCiudadana/Crisis-sanitaria-COVID-19.html#-b58db57c154b
Santamaría L, Hortal J. Chasing the ghost of infection past: identifying thresholds of change during the COVID-19 infection in Spain. Epidemiol Infect. 2020;148 [cited 2021 Apr 14]. Available from: https://pubmed.ncbi.nlm.nih.gov/33323424/.
Hale T, Angrist N, Goldszmidt R, et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat Hum Behav. 2021;5:529–38. https://doi.org/10.1038/s41562-021-01079-8.
Pierce M, Hope H, Ford T, Hatch S, Hotopf M, John A, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. The Lancet Psychiatry. 2020;7(10):883–892. [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/32707037/
Carstensen LL, Turan B, Scheibe S, Ram N, Ersner-Hershfield H, Samanez-Larkin GR, et al. Emotional experience improves with age: evidence based on over 10 years of experience sampling. Psychol Aging. 2011;26(1):21–33 [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/20973600/.
Charles ST, Reynolds CA, Gatz M. Age-related differences and change in positive and negative affect over 23 years. J Pers Soc Psychol. 2001;80(1):136–51 [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/11195886/.
Blanchflower DG, Oswald AJ. Is well-being U-shaped over the life cycle? Soc Sci Med. 2008;66(8):1733–49.
Smith L, Jacob L, Yakkundi A, McDermott D, Armstrong NC, Barnett Y, et al. Correlates of symptoms of anxiety and depression and mental wellbeing associated with COVID-19: a cross-sectional study of UK-based respondents. Psychiatry Res. 2020;291 [cited 2020 Sep 28]. Available from: https://pubmed.ncbi.nlm.nih.gov/32562931/.
Andrade EF, Pereira LJ, de Oliveira APL, Orlando DR, Alves DAG, de Guilarducci JS, et al. Perceived fear of COVID-19 infection according to sex, age and occupational risk using the Brazilian version of the fear of COVID-19 scale. Death Stud. 2020:1–10 [cited 2021 Apr 21]. Available from: https://www.tandfonline.com/doi/full/10.1080/07481187.2020.1809786.
Foundation Pro Juventute. Corona-Report: So geht es Kindern und Jugendlichen | Pro Juventute [Internet]. [cited 2021 Apr 21]. Available from: https://www.projuventute.ch/de/corona-report
Lecic-Tosevski D. Is urban living good for mental health? Curr Opinion Psychiatry. 2019;32:204–9 Lippincott Williams and Wilkins; [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/30695002/.
Okkels N, Kristiansen CB, Munk-Jørgensen P, Sartorius N. Urban mental health. Curr Opin Psychiatry. 2018;31(3):258–64 [cited 2021 Apr 14];Available from: https://journals.lww.com/00001504-201805000-00014.
Andersen LM, Harden SR, Sugg MM, Runkle JD, Lundquist TE. Analyzing the spatial determinants of local Covid-19 transmission in the United States. Sci Total Environ. 2021;754:142396 [cited 2021 Apr 28]. Available from: https://pubmed.ncbi.nlm.nih.gov/33323424/.
Tamminen N, Kettunen T, Martelin T, Reinikainen J, Solin P. Living alone and positive mental health: a systematic review. Syst Rev. 2019;8:134 BioMed Central Ltd.; [cited 2020 Dec 2]. Available from: https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-019-1057-x.
Selby K, Durand M-A, Gouveia A, Bosisio F, Barazzetti G, Hostettler M, et al. Citizen responses to government restrictions in the COVID-19 pandemic: a cross-sectional survey in Switzerland (preprint). JMIR Form Res. 2020; [cited 2020 Dec 2]; Available from: https://pubmed.ncbi.nlm.nih.gov/33156809/.
Özdin S, Bayrak Özdin Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: the importance of gender. Int J Soc Psychiatry. 2020;66(5):504–11 [cited 2020 Sep 28]. Available from: https://pubmed.ncbi.nlm.nih.gov/32380879/.
Mazza C, Ricci E, Biondi S, Colasanti M, Ferracuti S, Napoli C, et al. A nationwide survey of psychological distress among italian people during the covid-19 pandemic: immediate psychological responses and associated factors. Int J Environ Res Public Health. 2020;17(9) [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/32370116/.
Lippi G, Henry BM. Active smoking is not associated with severity of coronavirus disease 2019 (COVID-19) [internet]. Eur J Inter Med. 2020;75:107–8 Elsevier B.V.; [cited 2021 Apr 14]. Available from: /pmc/articles/PMC7118593/.
Patanavanich R, Glantz SA. Smoking is associated with COVID-19 progression: a meta-analysis [internet]. Nicotine Tob Res. 2020;22:1653–6 Oxford University Press; [cited 2021 Apr 12]. Available from: https://pubmed.ncbi.nlm.nih.gov/32399563/.
Berlin I, Thomas D, Le Faou AL, Cornuz J. COVID-19 and smoking [internet]. Vol. 22, nicotine & tobacco research : official journal of the Society for Research on nicotine and tobacco. NLM (Medline). 2020:1650–2 [cited 2020 Sep 28]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7184428/.
World Health Organization W. Mental Health action plan 2013–2020 [Internet]. [cited 2020 Dec 2]. Available from: https://apps.who.int/iris/bitstream/handle/10665/89966/9789241506021_eng.pdf
Ohrnberger J, Fichera E, Sutton M. The dynamics of physical and mental health in the older population. J Econ Ageing. 2017;9:52–62.
Ohrnberger J, Fichera E, Sutton M. The relationship between physical and mental health: a mediation analysis. Soc Sci Med. 2017;195:42–9.
Patel V, Burns JK, Dhingra M, Tarver L, Kohrt BA, Lund C. Income inequality and depression: a systematic review and meta-analysis of the association and a scoping review of mechanisms [internet]. World Psychiatry. 2018;17:76–89 Blackwell Publishing Ltd; [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/29352539/.
Pickett KE, Wilkinson RG. Income inequality and health: a causal review [internet]. Soc Sci Med. 2015;128:316–26 Elsevier Ltd; [cited 2020 Dec 2]. Available from: https://pubmed.ncbi.nlm.nih.gov/25577953/.
United Nations. Policy brief: COVID-19 and the need for action on mental health; 2020.
Zhou X, Snoswell CL, Harding LE, Bambling M, Edirippulige S, Bai X, et al. The role of Telehealth in reducing the mental health burden from COVID-19. Telemed e-Health. 2020;26:377–9 Mary Ann Liebert Inc.; [cited 2020 Dec 2]. Available from: www.blackdoginstitute.org.au/getting-help/self-help-tools-apps.
Stocker D, Jäggi J, Liechti L, Schläpfer D, Németh P, Künzi K. Einfluss von Covid-19 auf die psychische Gesundheit. Bundesamt für Gesundheit. 2020; [cited 2020 Dec 2]. Available from: https://www.bag.admin.ch/bag/de/home/das-bag/aktuell/news/news-20-11-2020.html.
Berner Zeitung. Psychische Folgen von Corona – So viel Jugendliche in der Berner Psychiatrie wie noch nie [Internet]. [cited 2021 Apr 21]. Available from: https://www.bernerzeitung.ch/die-jugendpsychiatrie-in-bern-ist-am-anschlag-819099057755
Landeskirchen im Kanton Luzern. kirche-kommt-an.ch/ – “Die Dargebotene Hand”: Corona lässt viele zum Telefonhörer greifen [Internet]. [cited 2021 Apr 21]. Available from: https://www.kirche-kommt-an.ch/blog/die-dargebotene-hand-corona-laesst-viele-zum-telefonhoerer-greifen/
Serlachius A, Schache K, Boggiss A, Lim D, Wallace-Boyd K, Brenton-Peters J, et al. Coping skills mobile app to support the emotional well-being of young people during the COVID-19 pandemic: protocol for a mixed methods study. JMIR Res Protoc. 2020;9(10) [cited 2021 Apr 28]. Available from: https://pubmed.ncbi.nlm.nih.gov/32991303/.
Gloster AT, Lamnisos D, Lubenko J, Presti G, Squatrito V, Constantinou M, et al. Impact of COVID-19 pandemic on mental health: an international study. Francis JM, editor. PLoS One. 2020;15(12):e0244809 [cited 2021 Apr 21]. Available from: https://dx.plos.org/10.1371/journal.pone.0244809.
Esterwood E, Saeed SA. Past epidemics, natural disasters, COVID19, and mental health: learning from history as we Deal with the present and prepare for the future. Psychiatry Q. 2020:1–13. Springer; [cited 2020 Sep 28]. Available from. https://doi.org/10.1007/s11126-020-09808-4.
Raker EJ, Zacher M, Lowe SR. Lessons from hurricane Katrina for predicting the indirect health consequences of the COVID-19 pandemic. Proc Natl Acad Sci U S A. 2020;117(23):12595–7 [cited 2020 Sep 28]. Available from: www.pnas.org/cgi/doi/10.1073/pnas.
Townsend P, Phillimore P, Beattie A. Health and deprivation. Inequality and the north. Health Policy (New York). 1988;10(2):207.
Bell N, Schuurman N, Oliver L, Hayes MV. Towards the construction of place-specific measures of deprivation: a case study from the Vancouver metropolitan area. Can Geogr. 2007;51(4):444–61.
Maroko AR, Doan TM, Arno PS, Hubel M, Yi S, Viola D. Integrating social determinants of health with treatment and prevention: a new tool to assess local area deprivation. Prev Chronic Dis. 2016;13(9):160221 [cited 2021 Apr 15]. Available from: http://www.cdc.gov/pcd/issues/2016/16_0221.htm.
Vetter S, Endrass J, Schweizer I, Teng HM, Rossler W, Gallo WT. The effects of economic deprivation on psychological well-being among the working population of Switzerland. BMC Public Health. 2006;6(1):223 [cited 2021 Jun 9]. Available from: http://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-6-223.
Demarest S, Van der Heyden J, Charafeddine R, Tafforeau J, Van Oyen H, Van Hal G. Socio-economic differences in participation of households in a Belgian national health survey. Eur J Pub Health. 2013;23(6):981–5 [cited 2021 Jun 9]. Available from: https://academic.oup.com/eurpub/article-lookup/doi/10.1093/eurpub/cks158.
Acknowledgments
We thank all participants for their valuable time and for participating in our study. Furthermore, we are grateful for the support of the LINK Institute (Luzern, Switzerland, https://www.link.ch/).
Funding
Authors were funded by the Sitftung für Hausarztmedizin (foundation of family medicine), Basel, Switzerland.
Author information
Authors and Affiliations
Contributions
L.D.H. made substantial contributions to the conception of the work, interpretation of results, drafted the manuscript, and substantively revised it. S.G. made substantial contributions to the conception of the work, data analysis, interpretation of results, and substantively revised the manuscript. R.F. made substantial contributions to the conception of the work, interpretation of results, and substantively revised the manuscript. A.Z. made substantial contributions to the conception of the work, interpretation of results and substantively revised the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations. Ethical approval of the study was submitted to the Ethics Committee of Northwest and Central Switzerland (EKNZ), which advised that formal ethical approval was not required (Project-ID: Req-2020-00449) since the survey complies with the general ethical principles for human research. Participants gave informed consent while accepting to participate in the survey.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
Questionnaire in English. Table S1 Cross-tabulation of mental health well-being reported impairment due to COVID-19 and screening questions of impaired mental health.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Diaz Hernandez, L., Giezendanner, S., Fischer, R. et al. The effect of COVID-19 on mental well-being in Switzerland: a cross-sectional survey of the adult Swiss general population. BMC Fam Pract 22, 181 (2021). https://doi.org/10.1186/s12875-021-01532-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-021-01532-7