
Abstract
Introduction
Indonesia has not optimally provided complete and reliable civil registration and vital statistics (CRVS). Death certification is one of the elements of the CRVS system. Reliable data on death rates and causes serve as the basis for building a strong evidence base for public health policy, planning, monitoring, and evaluation. This study aims to implement an approach to identifying the cause of death through verbal autopsy by empowering community health workers during the pandemic.
Method
This study is implementation research with the empowerment of the community, in this case, health cadres and health facilitators/workers, to identify the cause of death through a mobile-based verbal autopsy. This implementation research consisted of four main activities: community-based verbal autopsy, mobile-based verbal autopsy development, data collection, and analysis of the suspected causes of death using InterVA-5.
Result
From October to November 2020, a total of 143 respondents were willing to do a verbal autopsy interview (response rate of 58%). Of 143 respondents, most of them were women (112 or 78.3%), was the child of the deceased (61 or 42.7%) and lived with the deceased until before he/she died (120 or 83.9%). Based on the characteristics of the deceased, of 143 deceased, 78 (54.5%) were male, 134 (93.7%) were adults, 100 (69.9%) died at home, and 119 (83.2%) did not have a death certificate stating the cause of death. The cause of death of 143 deceased mainly was infectious disease (92 or 64.3%), followed by non-communicable disease (39 or 27.3%), external factors (5 or 3.5%), and unknown factors (4 or 2.8%). In sequence, the top five suspected causes of death are acute respiratory infection, including pneumonia (72 or 50.3%), other and unspecified infectious disease (18 or 12.6%), other and unspecified cardiac disease (17 or 11.9%), acute cardiac disease (4 or 2.8%), and Digestive neoplasms (4 or 2.8%).
Conclusion
The findings showed that the mobile-based verbal autopsy using a community-based mechanism was feasible during the COVID-19 pandemic.
Similar content being viewed by others


Introduction
Indonesia has not optimally provided complete and reliable civil registration and vital statistics (CRVS) from Department of Population and Civil Registration (Dinas Kependudukan dan Pencatatan Sipil/Disdukcapil) at the district level under The Ministry of Home Affairs (MoHA) [1]. Vital statistics depend on a country's legal framework but typically include birth, death, cause of death, marriage and divorce, as well as adoption [2].
Death certification is one of the elements of the CRVS system. In Indonesia, the death certification system in Indonesia is still weak, and the cause of death of people mostly remains unknown [3, 4]. Reliable data on the rates and causes of death serve as the basis for building a strong evidence base for public health policy, planning, monitoring, and evaluation [5, 6]. Accurate, real-time statistics on causes of death are critical to developing public health policies and supporting a country’s ability to respond to emerging health threats and epidemics [7]. The availability of robust data related to vital statistics, including causes of death, is important for calculating, accountability, and monitoring the progress of achieving the Sustainable Development Goals (SDGs) and national targets [5, 8,9,10].
Globally, two-thirds (38 million) of 56 million annual deaths are still not registered [11]. A comparison of the findings of the leading causes of death is influenced by variations in certification skills of physicians, availability of diagnostic and pathological data when filling out death certificates, differences in medical culture when selecting the root cause, and the availability of trained mortality coders to accurately code the cause of death information [12,13,14]. For other deaths without medical certification, multiple data sources and diagnostic approaches, including surveillance systems, demographic research sites, surveys, censuses, disease records, verbal autopsies, and police records, should be utilized to obtain an overview of the causes of death in various populations [15, 16].
Civil registration in Indonesia has not realized the usefulness of death information as a reliable source of data [17]. The mortality measurement is the basic indicator for evaluating population health and is best derived from the death registration system. Nonetheless, such information is unavailable in Indonesia [18]. Consequently, indirect demographic techniques and life table models were utilized to estimate Indonesian mortality [19, 20].
The best alternative without a death certificate to ascertain the probable cause of death is a verbal autopsy (VA). VA mostly discusses the causes of death of individuals in countries with inadequate civil registration and death certification systems, where the majority of people die at home without interacting with the health system. Previous research has shown that VA can improve the diagnosis of the cause of death, and this method continues to be used in many countries [21, 22]. The face-to-face interview has been the standard method of communication for VA interviews [23]. During the coronavirus disease 2019 (COVID-19) pandemic, the face-to-face VA process has been delayed due to the physical distancing preventive measures implemented [24]. During pandemics or other instances where face-to-face interviews are not possible, the telephone interview method ensures VA data collection is not delayed and provides accuracy for mortality data [25].
This study aims to implement an approach to identifying the cause of death through verbal autopsy by empowering community health workers during the pandemic. With this approach, it is hoped that quality and sustainable data and information on causes of death at the community level can be provided to strengthen the death registration system and improve health program planning.
Method
This study is implementation research [26] with the empowerment of the community, in this case, health cadres and health facilitators/workers, to identify the cause of death through a mobile-based verbal autopsy. This study was conducted in Babakan Madang Sub-District, Bogor District, between September and December 2020. This implementation research consisted of four main activities, namely:
Community-based verbal autopsy
This study developed a mechanism for empowering health cadres and health facilitators/workers in conducting a verbal autopsy to determine the suspected cause of death in the community. Health cadres were recruited by program managers at the public health centers based on their activeness in implementing health programs in their respective villages, while the researchers recruited health facilitators/workers. The health facilitators/workers involved in this study were specifically recruited for Verbal Autopsy, while the health cadres involved in this study were not specific for Verbal Autopsy but also carried out their routine work as health cadres. Then, the selected health cadres and facilitators/workers were given education, training, and role play related to the strategy for implementing verbal autopsy. A total of 18 health cadres were selected from nine villages, and nine health facilitators/workers participated in the training.
Mobile-based verbal autopsy
This mobile-based verbal autopsy application was developed using the Kobotoolbox platform with the questions adopted based on the WHO 2016 verbal autopsy instrument version 1.5.3 and translated to Indonesian [27]. All the input data were stored in the cloud server of the data collection application using the Kobo toolbox platform.
Data collection
This research involved the residents of Babakan Madang Sub-District aged 18 years and over, who had WhatsApp, and family members who died within six weeks to 12 months before the study. The selection of the period between the date of death and the interview date was based on the VA Field Interviewer Manual for 2016 WHO VA Instrument [28]. The minimum period of six weeks allows sufficient time for the family to recover from the bereavement and be emotionally ready to share details of the event, while the maximal period of 12 months has been designed to reduce the potential for details to be forgotten or confused. Health cadres first recorded the people who died during that period and approached the family to perform a verbal autopsy. After they were ready, health facilitators/workers performed a verbal autopsy over the WhatsApp call (according to the health protocol during the COVID-19 pandemic) using a mobile-based verbal autopsy.
Analysis of suspected causes of death
The collected verbal autopsy data were then adjusted to the InterVA-5 format (comma-separated values or.csv file) using Ms. Excel [29]. The formatted data were then analyzed using InterVA-5 to generate suspected causes of death for the individual. The InterVA-5 analysis generated up to three suspected specific causes of death with likelihood and provided an ICD-10 code according to the specific cause of death [27, 30]. The results of the suspected cause of death were reported in the aggregate at the sub-district level.
Result
During this COVID-19 pandemic, all activities are carried out online following applicable health protocols. Based on the data collected by cadres from local villages, it was identified that 246 people died from six weeks to 12 months before the study. Overall, from October to November 2020, 246 potential respondents were contacted by health cadres, and 143 respondents were willing for a verbal autopsy interview (response rate of 58%) (Fig. 1). Of the nine villages, five villages (Sumur Batu, Kadumangu, Babakan Madang, Citaringgul, and Karangtengah) had a response rate of more than 60%, and four villages (Bojong Koneng, Cijayanti, Sentul, and Cipambuan) had a response rate below 50%. Monitoring was carried out every week through weekly reports by health cadres and facilitators to ensure the quality of research activities. The active role of health cadres as local contacts is important to explain and approach family members so that health workers/facilitators can perform a verbal autopsy.

VA Response Rate in Babakan Madang Sub-District
Analysis of suspected causes of death
The characteristics of respondents who were willing to do a verbal autopsy are shown in Table 1. Of 143 respondents, most of them were women (112 or 78.3%), was the child of the deceased (61 or 42.7%) and lived with the deceased until before he/she died (120 or 83.9%). Based on the characteristics of the deceased, of 143 deceased, 78 (54.5%) were male, 134 (93.7%) were adults, 100 (69.9%) died at home, and 119 (83.2%) did not have a death certificate stating the cause of death.
Table 2 describes VA's suspected causes of death in Babakan Madang Sub-District and integration with ICD-10. The results showed that the cause of death of 143 deceased mainly was infectious disease (92 or 64.3%), followed by non-communicable disease (39 or 27.3%), external factors (5 or 3.5%), and unknown factors (4 or 2.8%). In sequence, the top five suspected causes of death are acute respiratory infection, including pneumonia (72 or 50.3%), other and unspecified infectious disease (18 or 12.6%), other and unspecified cardiac disease (17 or 11.9%), acute cardiac disease (4 or 2.8%), and Digestive neoplasms (4 or 2.8%).
Discussion
The extent to which this system can identify suspected causes of death at the community level
Currently, the government lacks information regarding the specific causes of death at the community level. Knowing the cause of death at the population/community level is crucial since significant disparities exist between the causes of death in the community and the medical setting [31]. Based on data from Bogor District Central Statistic Agency in 2018, the number of deaths in Babakan Madang Sub-District was 702 deaths [32]. However, only 31 death certificates (4.4%) were issued by the Population and Civil Registration Service [32, 33]. The low percentage of ownership of death certificates can occur because most deaths are outside health facilities and are not officially recorded in the passive surveillance system [34]. The results of the Sample Registration System also show that 64.5% of deaths in Indonesia occur at home [3]. The critical finding also showed that most deaths occurred outside health facilities (n = 106, 74.1%).
The rules regarding reporting of deaths already exist, but they are still passive and rely on the family to report the incident of death to the head of the neighborhood unit for further reporting to Department of Population and Civil Registration no later than 30 days from the date of death [35]. There is also already a mechanism for reporting death data in health care facilities, in which every health care facility operator must report data on deaths and causes of natural and unnatural deaths to the local Health Office once a month, with a copy submitted to Department of Population and Civil Registration [35]. However, the data sharing mechanism between the Health Office and Department of Population and Civil Registration does not run optimally [36], resulting in a low death notification rate in the population. Thus, verbal autopsies using the WHO VA instrument are recommended.
The WHO VA instrument has been utilized extensively, particularly in low- and middle-income countries where routine data on causes of death are lacking and where most persons die at home [21, 22, 34, 37]. The analysis using InterVA-5 carried out in this study is also recommended by WHO as a tool for analyzing VA [27]. Previous research has shown that the results of VA analysis using InterVA-5 compared with established causes at participating tertiary hospitals can obtain concordance correlation coefficients of 0.92 for children and 0.86 for adults and provide the ICD-10 code according to the specific cause of death [30].
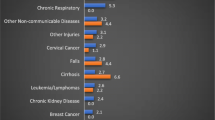
The results of this study indicate that the top five suspected causes of death are acute respiratory infection, including pneumonia, other and unspecified infectious disease, other and unspecified cardiac disease, acute cardiac disease, and pulmonary tuberculosis. In accordance with Wahab's research, the major cause of mortality is stroke (20.6%), followed by acute respiratory infections (ARIs), including pneumonia (15.7%), other and nonspecific cardiovascular illnesses (9.8%), malaria (6.0%), and tuberculosis (5.9%) [38]. According to national data, stroke is the main cause of death, followed by ischemic heart disease, diabetes, cirrhosis, and tuberculosis [39]. There will be discrepancies when compared to national data on death causes. The result of this research is a pattern of causes of death that is representative of a limited community in the Babakan Madang subdistrict and occurs during a pandemic. However, the use of mobile-based verbal autopsies in this study seems to indicate that this approach has the potential to get data on causes of death at the population level, whereas these data are difficult to collect at the district level. Of course, further research in the broader area is needed to get a more solid conclusion.
To what extent can this system be implemented during the COVID-19 pandemic
The COVID-19 pandemic has limited the mobility and face-to-face activities of the community-based verbal autopsy in this study, but with the use of information and communication technology, it can still be implemented. According to research from Siregar et al., in the conditions of the COVID-19 pandemic, community empowerment using information and communication technology has a high scope in reaching the community [40].
The mechanism developed in this study allows researchers, health service officers, public health center officers, health facilitators/workers, health cadres, and the community to be connected by using smartphones and communication media such as WhatsApp or Zoom. Previous research has shown that the use of smartphones is effective in various social learning and communication contexts in health and healthcare, including patient care, monitoring, rehabilitation, communication, diagnosis, education, and research [41]. Research conducted by Henry et al. showed that WhatsApp had exhibited a sort of innovation that can aid community-based initiatives in times of emergency [42]. Mandy et al. also stated that the use of the Zoom application as a tool for qualitative data collection has great potential due to its relative ease of use, cost-effectiveness, data management features, and security options [43]. A study from Nasarudin et al. also said that VA via telephone interviews was feasible, acceptable, and could be used as an alternative to face-to-face interviews without affecting the data quality. As long as face-to-face interviews are not possible, VA telephone interviews can be used for data collection for mortality surveillance [25].
All activities in this study, ranging from meetings, training, implementation, and monitoring to evaluation, were carried out online via Zoom Meetings or WhatsApp calls. Although the response rate in the four regions was below 50% and several obstacles were found, this activity could be carried out well during the pandemic. After the pandemic, of course, this research needs to be continued so that the effectiveness of face-to-face in this community-based verbal autopsy can also be studied.
There are some obstacles and challenges in community-based VA. First, the prospective respondents refused and were offended because they were asked about their deceased family members. There was still a sense of loss, which made them sad, and some people believe that asking about the deceased is not permissible by religion. Therefore, health cadres were asked to explain the objectives of the VA research according to the format provided, in a kind, polite, and personal way to build trust, but if they still refused, the health cadres could contact other prospective respondents. Second, the respondents feared their data being misused as the data of COVID-19 patients. The health cadres were asked to explain that the respondents’ data would not be misused and that this activity had received approval and guidance from the Bogor District Health Office and the local public health center. Third, as a mode of communication in implementing VA in the field, Whatsapp use has challenges related to connectivity experienced by health cadres and respondents. For example, limited internet quota, lack of digital literacy, and the existence of remote areas in several villages so that access to telephone or internet networks is inadequate.
Potential for integrating with health and demographic surveillance system and routine data
In 2019, the researchers conducted a pilot study of the Health and Demographic Surveillance System (HDSS) in the Babakan Madang Sub-District, which was planned to be carried out continuously. The application of HDSS in Babakan Madang Sub-District could provide vital statistics, including births, deaths, transfers (in and out), and health situations through PIS-PK (Program Indonesia Sehat-Pendekatan Keluarga/Healthy Indonesia Program through Family Approach) which a passive surveillance system cannot record. With the HDSS in Babakan Madang Sub-District, data on the deceased have been collected, but the cause is not yet known. Integration with existing systems such as routine data recording in health facilities, vital statistics, and civil registration is also required to link death-related registration. Integrating death data and the implementation of mobile-based VA to find out the suspected causes of death in the population allows policymakers to know Cause-Specific Death rates at the population level. Several studies have also shown the possible integration between VA and HDSS to corroborate vital statistics and cause-specific mortality figures at the population level [44,45,46]. This integration can strengthen local potentials that ensure the functioning of health cadres to be actively involved in participatory community-based health programs. Additionally, prior research has emphasized the need for a functional community surveillance system to help record accountable deaths [40].
Limitation
The level of acceptance of families to be interviewed regarding the death of their family members can vary, so the activeness of health cadres is very important in reaching and explaining to them. In addition, there are remote areas in this sub-district with no internet network, so using WhatsApp calls/Zoom Meetings is not possible. Thus, the deaths in the work area of each cadre cannot be recorded.
We did not validate and confirm the cause of death with physicians. Moreover, most of the deaths occurred at home, so no historical data were found for analyzing the causes of death in health services. This can lead to misclassification of the suspected causes of death or unspecified suspected death in some individuals. With the VA method, which in the future could be integrated with existing systems such as routine data recording in health facilities, vital statistics, and civil registration, it is hoped that program holders and policymakers can obtain an unprecedented overview of the causes of death at the population level.
Conclusion
The findings indicated that VA using a community-based mechanism was feasible to run during the COVID-19 pandemic. The mobile-based VA application can also be used to identify the causes of death at the population level. The availability of data related to suspected causes of death at the population level can hopefully serve as the basis for health program holders in making policies and plans to improve public health.
Recommendation
Integrating death registration with HDSS and existing systems such as routine data recorded in health facilities, vital statistics, and civil registration is needed to strengthen death registration and implement VA. For some areas that lack internet access, if face-to-face verbal autopsies are still not possible, VA can be done by telephone (no internet signal required).
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due to recommendations from the ethics commission but are available from the corresponding author on reasonable request.
Abbreviations
- COVID-19:
-
Coronavirus Disease-19
- CRVS:
-
Civil Registration and Vital Statistics
- CSV:
-
Comma-separated values
- Disdukcapil:
-
Dinas Kependudukan dan Pencatatan Sipil (Department of Population and Civil Registration)
- HDSS:
-
Health and Demographic Surveillance System
- ICD:
-
International Classification of Diseases
- MoHA:
-
Ministry of Home Affairs
- PIS-PK:
-
Program Indonesia Sehat dengan Pendekatan Keluarga (Healthy Indonesia Program through Family Approach)
- SDGs:
-
Sustainable Development Goals
- VA:
-
Verbal Autopsy
- WA:
-
WhatsApp
- WHO:
-
World Health Organization
References
Siagian C, Wandasari W, Sahputra F, Kusumaningrum S. Strategic yet delicate: the dilemma of involving health workers in facilitating birth registration in Indonesia. BMC Health Serv Res. 2019;19:1–12.
Abouzahr C, Stein C, Chapman N, Toole D, LeFranc C, Joshi K, et al. A development imperative: civil registration and vital statistics systems in the Asia-Pacific region. Asia-Pacific Population Journal. 2014;29(1):9–37.
Ministry of Health Republic of Indonesia. Indonesia: Sample Registration System 2014. Jakarta: Lembaga Penerbitan Balitbangkes; 2015.
Indriasih E. The performance of the tariff method and physicians in determining stroke as cause of deaths using verbal autopsy in areas where physicians are not widely available, Indonesia 2017. Health Sci J Indonesia. 2021;12:39–46.
Mikkelsen L, Phillips DE, AbouZahr C, Setel PW, De Savigny D, Lozano R, et al. A global assessment of civil registration and vital statistics systems: monitoring data quality and progress. Lancet. 2015;386:1395–406.
World Health Organization. Strengthening civil registration and vital statistics for births, deaths and causes of death: resource kit. Geneva: World Health Organization; 2013.
de Savigny D, Riley I, Chandramohan D, Odhiambo F, Nichols E, Notzon S, et al. Integrating community-based verbal autopsy into civil registration and vital statistics (CRVS): system-level considerations. Glob Health Action. 2017;10:1272882.
Adair T, Firth S, Phyo TPP, Bo KS, Lopez AD. Monitoring progress with national and subnational health goals by integrating verbal autopsy and medically certified cause of death data. BMJ Glob Health. 2021;6:e005387.
Richards N, Sorchik R, Brolan C. Why the Sustainable Development Goal Agenda Needs Strong Civil Registration and Vital Statistics Systems. CRVS Development Series. Melbourne: Bloomberg Philanthropies Data for Health Initiative, Civil Registration and Vital Statistics Improveme; 2019.
World Health Organization. World health statistics 2019: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization; 2019.
World Health Organization. Civil registration: why counting births and deaths is important. 2014 [cited 2022 Jul 27];Available from: https://www.who.int/news-room/fact-sheets/detail/civil-registration-why-counting-births-and-deaths-is-important
Sibai AM. Mortality certification and cause-of-death reporting in developing countries. Bull World Health Organ. 2004;82:83.
Nielsen GP, Björnsson J, Jonasson JG. The accuracy of death certificates. Virchows Archiv A. 1991;419:143–6.
Muñoz DC, Abouzahr C, de Savigny D. The ‘Ten CRVS Milestones’ framework for understanding civil registration and vital statistics systems. BMJ Glob Health. 2018;3:e000673.
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–128.
AbouZahr C. New estimates of maternal mortality and how to interpret them: choice or confusion? Reprod Health Matters. 2011;19:117–28.
Hartono B. Current situation in mortality statistics: Indonesia. In: Regional Consultation on Mortality Statistics. New Delhi: World Health Organization; 2007.
Mahapatra P, Shibuya K, Lopez AD, Coullare F, Notzon FC, Rao C, et al. Civil registration systems and vital statistics: successes and missed opportunities. Lancet. 2007;370:1653–63.
Kosen S, Soemantri S, Agung IG, Ananta I, Kosdiatmono W, Moehdin S, et al. The Indonesian Abridged Life Table 2000. National Institute of Health Research and Development Indonesia: Jakarta; 2004.
Hidajat M, Hayward MD, Best LE. The Life Table without the Vital Registration System: Alternative models of Indonesian Mortality. In: International Population Conference, International Union for the Scientific Study of Populations. Tours; 2005. Available from: https://www.researchgate.net/publication/267717519_The_Life_Table_without_the_Vital_Registration_System_Alternative_Models_of_Indonesian_Mortality.
Aggarwal AK, Kumar P, Pandit S, Kumar R. Accuracy of WHO verbal autopsy tool in determining major causes of neonatal deaths in India. PLoS ONE. 2013;8:e54865.
Anteneh A, Araya T, Misganaw A. Factors associated with place of death in Addis Ababa. Ethiopia BMC Palliat Care. 2013;12:1–9.
World Health Organization. Verbal autopsy standards: The 2016 WHO verbal autopsy instrument. Geneva, Switzerland: WHO; 2016.
Ministry of Health. Minister of Health Regulation No. 9 of 2020 concerning Guidelines for Large-Scale Social Restrictions in the Context of Accelerating Handling of Corona Virus Disease 2019 [Peraturan Menteri Kesehatan No. 9 Tahun 2020 tentang Pedoman Pembatasan Sosial Berskala Besar Dalam Rangka Percepatan Penanganan Corona Virus Disease 2019]. Indonesia: https://peraturan.bpk.go.id/Home/Details/135220/permenkes-no-9-tahun-2020; 2020 [cited 2022 Jul 27]. Available from: https://peraturan.bpk.go.id/Home/Details/135220/permenkes-no-9-tahun-2020
binti Nasaruddin NH, Ganapathy SS, Awaluddin SM, Anuar MFM, binti Alias N, Mang CY, et al. Conducting verbal autopsy by telephone interview during the pandemic to support mortality surveillance: a feasibility study in Malaysia: Verbal autopsy telephone interview. Western Pacific Surveillance and Response. 2022;13(2):1–7.
UNICEF/UNDP/World Bank/WHO Special. Programme for Research and Training in Tropical Diseases, Global Fund to Fight AIDS, Tuberculosis and Malaria, Agency for International Development, World Health Organization, UNAIDS. Framework for operations and implementation research in health and disease control programs. World Health Organization; 2008. Available from: https://apps.who.int/iris/handle/10665/44686.
World Health Organization. Verbal autopsy standards: ascertaining and attributing causes of death tool. 2016 [cited 2022 Jul 17]. Available from: https://www.who.int/standards/classifications/other-classifications/verbal-autopsy-standards-ascertaining-and-attributing-causes-of-death-tool.
World Health Organization. Verbal autopsy standards: VA Field Interviewer Manual for the 2016 WHO VA Instrument. Geneva: World Health Organization; 2017.
Byass P. InterVA-5.1 User Guide. 2020 [cited 2022 Jul 27];Available from: http://www.byass.uk/interva/products.htm
Byass P, Hussain-Alkhateeb L, D’Ambruoso L, Clark S, Davies J, Fottrell E, et al. An integrated approach to processing WHO-2016 verbal autopsy data: the InterVA-5 model. BMC Med. 2019;17:1–12.
Nabukalu D, Ntaro M, Seviiri M, Reyes R, Wiens M, Sundararajan R, et al. Community health workers trained to conduct verbal autopsies provide better mortality measures than existing surveillance: results from a cross-sectional study in rural western Uganda. PLoS One. 2019;14:e0211482.
Badan Pusat Statistik Kabupaten Bogor. Kecamatan Babakan Madang dalam Angka. Bogor: Badan Pusat Statistik Kabupaten Bogor; 2019.
Dinas Kependudukan dan Pencatatan Sipil Kabupaten Bogor. Jumlah Penerbitan Akta Kematian di Kabupaten Bogor. 2019 [cited 2021 Nov 4];Available from: http://www.opendata.bogorkab.go.id/
Dedefo M, Zelalem D, Eskinder B, Assefa N, Ashenafi W, Baraki N, et al. Causes of death among children aged 5 to 14 years old from 2008 to 2013 in Kersa health and demographic surveillance system (Kersa HDSS). Ethiopia PLoS One. 2016;11:e0151929.
Ministry of Home Affairs, Ministry of Health. Joint Regulation of the Minister of Home Affairs and the Minister of Health Number 15 of 2010 Number 162/Menkes/PB/I/2010 concerning Reporting of Deaths and Causes of Death [Peraturan Bersama Menteri Dalam Negeri dan Menteri Kesehatan Nomor 15 Tahun 2010 Nomor 162/Menkes/PB/I/2010 Tentang Pelaporan Kematian Dan Penyebab Kematian]. Indonesia: 2010 [cited 2022 Jul 27]. Available from: https://jdih.mkri.id/mg58ufsc89hrsg/16e064dea2d32118076e64546337ce45e9ccc8df5.pdf
Sulistiowati E, Handayani K. Pelaksanaan Registrasi Kematian dan Penyebab Kematian di Kota Ambon Tahun 2014. Media Penelitian dan Pengembangan Kesehatan. 2019;29:1–12.
Kusumaningrum S, Bennouna C, Siagian C, Agastya NLP. Back to what counts: birth and death in Indonesia. Jakarta: Indonesia PUSKAPABAPPENAS-KOMPAK; 2016.
Wahab A, Choiriyyah I, Wilopo SA. Determining the cause of death: mortality surveillance using verbal autopsy in Indonesia. Am J Trop Med Hyg. 2017;97:1461.
Institute for Health Metrics and Evaluation. Indonesia: What causes the most deaths?; 2019 [cited 2022 Jul 27]. Available from: https://www.healthdata.org/indonesia.
Siregar KN, Kurniawan R, BaharuddinNur RJ, Nuridzin DZ, Handayani Y, Retnowati, et al. Potentials of community-based early detection of cardiovascular disease risk during the COVID-19 pandemic. BMC Public Health. 2021;21:1308. Available from: https://doi.org/10.1186/s12889-021-11384-6.
Kamel Boulos MN, Giustini DM, Wheeler S. Instagram and WhatsApp in health and healthcare: an overview. Future Internet. 2016;8:37.
Henry JV, Winters N, Lakati A, Oliver M, Geniets A, Mbae SM, et al. Enhancing the supervision of community health workers with WhatsApp mobile messaging: qualitative findings from 2 low-resource settings in Kenya. Global Health Sci Practice. 2016;4:311–25.
Archibald MM, Ambagtsheer RC, Casey MG, Lawless M. Using zoom videoconferencing for qualitative data collection: perceptions and experiences of researchers and participants. Int J Qual Methods. 2019;18:1609406919874596.
Soura AB, Lankoande B, Millogo R, Bangha M. Comparing causes of death between formal and informal neighborhoods in urban Africa: evidence from Ouagadougou Health and Demographic Surveillance System. Glob Health Action. 2014;7:25523.
Coates MM, Kamanda M, Kintu A, Arikpo I, Chauque A, Mengesha MM, et al. A comparison of all-cause and cause-specific mortality by household socioeconomic status across seven INDEPTH network health and demographic surveillance systems in sub-Saharan Africa. Glob Health Action. 2019;12:1608013.
Melaku YA, Sahle BW, Tesfay FH, Bezabih AM, Aregay A, Abera SF, et al. Causes of death among adults in northern Ethiopia: evidence from verbal autopsy data in health and demographic surveillance system. PLoS ONE. 2014;9:e106781.
Acknowledgements
This study was funded on behalf of the Directorate of Research and Community Engagement, Universitas Indonesia, under contract number BA-381/UN2.RST/PPM.00.03.01/2021. Special thanks to the Public Health Center in the Babakan Madang district of Bogor Regency, West Java.
Funding
This study was funded on behalf of the Directorate of Research and Development (Direktorat Riset dan Pengembangan), Universitas Indonesia.
Author information
Authors and Affiliations
Contributions
This study was designed by KNS, RK, DZ, and RJ. KNS, RK, DZ, RJ, LH, and RY supervised the fieldwork and data collection. The analysis was performed by DZ, RT, RJ, and YH with input and guidance from KNS and RK. The draft of the paper was written by KNS, RK, DZ, and RJ, and all authors reviewed various versions. The authors read and approved the final manuscript. KNS = Kemal N. Siregar. RK = Rico Kurniawan. RJ = Ryza Jazid BaharuddinNur. DZ = Dion Zein. RT = Retnowati. RY = Rohjayanti. LH = Lindawati Halim. YH = Yolanda Handayani.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study has been ethically approved by the Institutional Review Board (ethics commission) of the Faculty of Public Health Universitas Indonesia, with a registration number of 601/UN2.F10.D11/ PPM.00.02/2020. The authors confirm that all methods were performed in accordance with relevant guidelines and regulations. Informed consent for participation was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that there are no conflicts of interest related to this article or this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Siregar, K.N., Kurniawan, R., Nuridzin, D.Z. et al. Strengthening causes of death identification through community-based verbal autopsy during the COVID-19 pandemic. BMC Public Health 22, 1607 (2022). https://doi.org/10.1186/s12889-022-14014-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-14014-x