
Abstract
Background
In the past decades, the diet in Greenland has been in transition resulting in a lower intake of traditional food and a higher intake of imported western food. This diet transition can affect public health negatively, and thus, continued monitoring of dietary habits is important. The present study aimed to follow up on the dietary habits of pregnant women included in the Greenlandic ACCEPT birth cohort (2013–2015) and the children’s father.
Methods
The follow-up food intake was assessed in 2019–2020 using food frequency questionnaires for 101 mothers and 76 fathers aged 24–55 years living in Nuuk, Sisimiut, and Ilulissat. Non-parametric statistical methods were used (Mann-Whitney U test/Spearman correlation) to assess the dietary pattern and influencing factors.
Results
The proportion of traditional and imported food was 14 and 86%, respectively. Intake frequency differed by gender (vegetables, fruits, fast food), the living town (terrestrial animals, vegetables, fruits), and age (fish, meat products, fruits, fast food). Socioeconomic and lifestyle factors significantly correlated with the intake frequency of several traditional and imported foods. Few changes in the mother’s dietary habits from inclusion (during pregnancy) to follow-up (3–5 years later) were found, showing less frequent intake of seabirds and fruits and more frequent meat intake.
Conclusion
We identified several factors that could affect dietary habits, and the results may be used to target future food recommendation for relevant population groups.
Similar content being viewed by others

Background
People have inhabited Greenland for at least 4500 years and have traditionally had a hunting-based lifestyle and diet [1]. Marine mammals (seal, whale, walrus, and polar bear), seabirds, and fish have traditionally dominated the diet of Greenlandic Inuit, while roots, berries, and leaves were eaten as a supplement when in season. Since the beginning of the twentieth century, the Greenlandic population has experienced a transition towards a society more influenced by the Western world [2, 3]. This transition has included a change towards a more Western diet. The diet today includes many imported food items, such as meat products from farm animals, fruit, vegetables, dairy products, and sugary foods. Despite the transition away from the traditional Greenlandic diet, it remains an important cultural, spiritual, and social connection to the surrounding nature [3].
The traditional Greenlandic diet, including marine mammals and fish, is an essential contributor to the intake of long-chain omega-3 fatty acids (n-3), minerals/metals (Iron, Zink, Selenium, Iodine), and vitamin A, B, and D [4]; however, the level of dietary fibers and other vitamins such as vitamin C are low [5]. Several of the nutrients in the traditional diet have been suggested to have a positive impact on human health, such as protective effects against inflammation [6, 7] and cardiovascular disease [8, 9], together with beneficial effects on brain and nerve development in children [10, 11]. However, the marine mammals, on top of the food chain, also contain high levels of contaminants, such as persistent organic pollutants (POPs) and toxic metals [12]. These environmental contaminants have been associated with several negative health effects, including impaired fetal growth [13, 14], adverse effects on the immune-, neuro-, reproductive, and endocrine system, and increased risk of some cancers [12].
The imported food products are often energy-dense and can be nutrient-poor products, which have a long shelf life and some are low-priced, available in all places including remote settlements [15]. Some of the popular imported food items include carbonated sweets, chips, and farmed (red) meat with a high saturated fat content. Together with a decrease in physical activity, the dietary transition has contributed to the increasing incidence of overweight, obesity, and diabetes in Greenland [15].
In Greenland, the Population Health Surveys showed a reduction in intake of local traditional Greenlandic food items from 2005 to 2018 and an increased intake of imported meat, fruit, vegetables, and dairy products [16, 17]. In 2005–2010, the proportion of traditional food was 17% in towns and 32% in settlements, while in 2018, the traditional food intake decreased to 14 and 21%, respectively [17]. In 2005–2010, the Nordic Nutrition Recommendations for intake of added sugar were exceeded by 67–71% of the participants, for saturated fat by 39–44%, and for protein by 46–47%, while 77% were below the recommendation for fibre and 47–59% were below for carbohydrate [5].
Dietary habits were also assessed in the Greenlandic birth cohort ACCEPT (Adaptation to Climate Change, Environmental Pollution, and dietary Transition), which included pregnant women from all parts of Greenland in 2010–2015 [18, 19]. The proportion of traditional food among pregnant women was 12–18% [18, 19], thus comparable to the proportions found in the general population in the Population Health Surveys [16, 17]. The most frequently consumed traditional food groups were marine mammals and fish, while the most frequently consumed imported food groups were fruit, carbohydrate food (potato, pasta, and rice), and sweets and snacks [18, 19].
Dietary habits can affect health and the risk of diseases, including diabetes, heart disease, stroke, and cancer [20]. Foods related to a reduced disease risk include fish, whole grain products, fruit, and vegetables, and these are often referred to as healthy foods. Whereas intake of processed and red meat, sugary snacks and sweets, fast food, and sugary drinks can increase the risk of some diseases and could be referred to as unhealthy foods. However, the amount eaten and the total energy intake play an important role as well. Thus, one of the most important food recommendations is to eat a varied, well-balanced, and healthy diet [20]. The health implications of the ongoing dietary transition in Greenland are complex, as both traditional and imported food can positively and negatively affect health. The transition must be followed closely to be able to revise and update the food recommendations continuously.
From May 2019 to January 2020, we followed up 101 of the women included in the ACCEPT birth cohort from 2013 to 2015, fathers of the children, and the ACCEPT children age 3–5 years. The study presents dietary patterns of the father and mother (aged 24–55 years) with possible differences for gender, age, and living place. We also looked into possible correlations in dietary habits between parents living together. To our knowledge, this is the first time in Greenland, that longitudinal dietary changes are reported, as we report dietary changes for women from inclusion at pregnancy to follow-up (3–5 years later).
Materials and methods
Study population
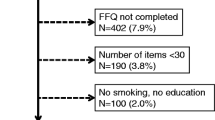
This study is based on the ACCEPT birth cohort [18, 19] established during 2010–2015 in Greenland with the overall aim of exploring environmental exposures, dietary changes, and health during a period of lifestyle transition and climate change. In total, 614 Greenlandic pregnant women were recruited from 16 towns distributed over five regions of Greenland (North, Disko bay, West, South, and East). To be included in the ACCEPT study, the women had to be over 18 years of age at the time of inclusion, lived more than 50% of their lives in Greenland, and have at least one Inuit parent. Of the recruited ACCEPT women, 504 fulfilled the inclusion criteria and 478 completed their pregnancy with available birth outcome (Fig. 1).

Flow chart for the study
During this ACCEPT follow-up study (May 2019 to January 2020), 295 live born singleton children were in the relevant age group of 3–5 years of age (children of mothers recruited in 2013–2015). Of these, 150 fulfilled the follow-up inclusion criteria (mothers had lived longest in the ACCEPT regions West or Disko Bay and currently lived in Nuuk, Sisimiut, or Ilulissat). The child’s biological father was included in this follow-up if possible. We contacted 133 ACCEPT mothers and her partner/child father, and 102 agreed to participate (one family participated with two children from two independent pregnancies). Finally, the total study population at follow-up included 101 mothers, 76 fathers, and 102 ACCEPT children (Fig. 1). The participation rate at follow-up was 76.6%, and those who did not accept to participate mainly gave lack of time as the reason.
After receiving a detailed description of the study, all participants gave signed informed consent to participate. They were informed that they could withdraw their consent at any time in the process and that their participation was voluntary.
The families got two home visits from a health nurse visitor and project researchers, respectively. At the first visit, the health nurse visitor interviewed the families, and questionnaires were filled out, and at the second visit, biological samples (blood, hair, urine, and nails) were collected.
The study was carried out in accordance with the Helsinki convention II, and was approved by the Commission for Scientific Investigations in Greenland (KVUG 2019–04).
Questionnaire data
The adult participants completed a self-administered questionnaire in Danish or Greenlandic. The health nurse visitors were available for assistance if the participants were in doubt about the meaning of the questions and possible answers. Two independent person’s double-entered data from the questionnaire into the validation program EpiData, and any disagreements were discussed.
The adult participants’ questionnaire was divided into two sections; section 1 contained questions about demographics, lifestyle, and health, and section 2 was a food frequency questionnaire (FFQ) about food intake for the last 12 months.
Data extracted from section 1 included age, history of living places (in and outside of Greenland), ethnicity, educational level, income, alcohol intake, smoking history, drug use, body mass index (BMI) (from self-reported height and weight), and number of children.
The dietary intake was calculated based on an FFQ (section 2 of the questionnaire), which was a slightly optimized version of the questionnaire used at inclusion at pregnancy during 2013–2015 [19]. It contained questions about 42 traditional and 23 imported food items, and it was possible to report the consumption frequencies in eight categories ranging from “never” to “several times a day” for each food item. The food items were divided into seven main traditional food groups: Marine mammals, Seabirds, Fish, Dried fish, Shellfish, Terrestrial animals, and Berries and seven main imported food groups: Meat products, Carbohydrate foods, Sauce, Fruit, Vegetables, Fast food, and Sweets and Snacks (Additional file 1: Table S1A). Each food item was given a frequency score representing the time(s) a month the food item was consumed. The food consumption frequencies for the food groups were calculated by summing the scores for the specific food items in the group. See additional file 1 for further explanation and examples of the calculation (Additional file 1: Table S1B, S1C). The frequency score method and similar FFQs have been used previously [18, 19, 21,22,23].
Furthermore, the FFQ included a column for seasonal information, with the possibility to answer if the food item was consumed in the spring/summer and/or autumn/winter. However, the percentage of missing data in these season variables was high (up to 60%), and the information was not included in the analyses. Please see Additional file 2: Table S2B.
Statistics
All statistical analyses were performed with SPSS software version 27 (SPSS Inc., Chicago, IL, USA). The statistically significant level was set to p ≤ 0.05.
For continuous variables, Mann-Whitney U test was used to test the difference between groups due to a high degree of non-normal distributed data (assessed by Q-Q plots) for the food variables. For categorical variables, Pearson’s Chi-square test was used to test the difference.
Correlations between intake frequency of food groups and socioeconomic and lifestyle factors were assessed with Spearman correlations.
The analyses of parent differences were restricted to mothers and fathers living together at the time of follow-up (n = 73). To assess the food intake differences between the individual parents, we subtracted the reported intake of the father from the reported intake of the mother (mother – father), thus zero (0) reflect equal intake for the mother and father, negative values reflect higher intake for the father, and positive values reflect higher intake for the mother.
To assess changes in food intake from inclusion at pregnancy to follow-up for the mother, the individual differences were calculated by subtraction of the reported intake from inclusion at pregnancy from the reported intake at follow-up (follow-up - inclusion). Thus zero (0) reflect equal intake at inclusion and follow-up, negative values reflect higher intake at inclusion during pregnancy, and positive values reflect higher intake at follow-up.
Wilcoxon Signed Rank test (median equal to 0) was used to test parent differences and changes from inclusion at pregnancy to follow-up (for mothers only) in food intake frequency. Furthermore, we assessed the pairwise correlations by calculating Spearman correlations for the food intake frequency. We also calculated partial Spearman correlations by adjusting for different predictors of the food intake frequency. The correlations between the parents were adjusted for the age difference between the parents (continuous), household income (categorical), percentage of life lived in Greenland for both the father and mother (continuous), and highest educational level for both the father and mother (categorical). Whereas, the correlations between inclusion at pregnancy and follow-up of the mother were adjusted for the time from inclusion to follow-up (continuous), change in education level (categorical), change in household income (categorical), change in BMI (continuous), and change in parity (categorical).
Sensitivity analyses by excluding non-Inuit and persons with less than 50% of their life spent in Greenland were conducted.
Results
Characteristics
Table 1presents the characteristics of the participants in the present study (101 mothers/ 76 fathers). The mothers were younger and leaner compared to the fathers. The mothers were also more likely to have a university degree and have never used hash and drugs, but less likely to have a personal income of more than 250.000 DKK per year.
Most of the participants lived in Nuuk (67.2%), while 32.8% lived in the other towns (Sisimiut, Ilulissat, Kangerlussuaq, and Qaqortoq). Due to the follow-up criteria, all mothers had lived longest in either Disko Bay or West, while some fathers had lived longest in other regions (11.4%) or outside Greenland (7.1%). Concerning the ethnic background, 80.0% were Inuit, 17.1% partly-Inuit, and 2.9% non-Inuit. An inclusion criterion for participating in the ACCEPT birth cohort was that the pregnant women were Inuit or partly-Inuit; thus, all non-Inuit participants in the present study were fathers (Table 1).
The results presented here were conducted on the full study population; however, the conducted sensitivity analyses excluding non-Inuit and persons with less than 50% of their life spent in Greenland showed similar results (not shown).
Food intake
Overall, the median intake frequency for traditional and imported food was distributed as 14 and 86%, respectively (Fig. 2 and Additional file 2, Table S2A). The most frequently consumed traditional food group was marine mammals (median: 6.0 times/month), followed by Greenlandic fish (median: 4.5 times/month) and terrestrial animals (median: 3.5 times/month), while the least frequently consumed traditional food groups were seabirds (median: 1.0 time/month) and berries (median: 1.0 time/month). The most consumed imported food group was carbohydrate food (median: 39.0 times/month) followed by sweets and snacks (median: 28.5 times/month), while fast food (median: 4.0 times/month) was the least consumed imported food group (Fig. 2 and Additional file 2: Table S2A). In Additional file 2 (Table S2B), the intake of the individual food items together with seasonal information can be seen. Of the traditional individual food items, caribou (wild-living Arctic reindeer) was most frequently consumed (median: 2.5 times/month), and 14.5% of the participants ate it at least once a week. For the imported food items, potato, pasta, rice, sauce, vegetables, and fresh fruit were all consumed 13.0 times/month (median), and 79.5–86.4% ate the food items at least once a week.

Traditional and imported food group intake (time(s) a month) (N = 177). The boxes display the 25th and 75th percentiles, and the line inside the boxes represents the median value. The whiskers display the minimum and maximum values. n: number of participants with information, The overall percentages of traditional (x) or imported food (y) food intake, were calculated by summing the medians of the main food groups and then the sum was divided by the total median intake (x + y)
Gender differences
For all traditional food groups, the intake frequency was similar for mothers and fathers (Table 2). However, for the imported food groups, mothers reported more frequently consuming fruit and vegetables and less frequently fast food than the fathers. Similarly, a higher percentage of mothers ate vegetables and fruit once a week or more, whereas more fathers ate fast food weekly (Table 2).
For mothers, the traditional and imported food was distributed as 13 and 87%, respectively. While for fathers, the percentages median food intake was 15% traditional and 85% imported food (Table 2).
Similarities and differences for parents living together
Within the study population, 73 mothers and fathers were living together. To assess the differences between the individual parent pairs, we subtracted the reported food intake of the father from the reported intake of the mother. There were no differences between parents in the intake frequency of the traditional food groups (Table 3). For the imported food groups, mothers had a significantly higher intake of fruit and vegetables and a less frequent intake of fast food than the fathers (Table 3).
Spearman pairwise correlations of the food groups between mothers and fathers were positive and moderate with an adjusted correlation coefficient ranging from 0.20 for fruits to 0.54 for terrestrial animals (Table 3). All correlations were significant in the unadjusted analyses, while seabirds, fruits, and sweets and snacks were non-significant in the adjusted analyses (Table 3).
Differences by geographical area (mothers and fathers pooled)
Table 4 shows the comparison of food intake by current living town. Significant lower consumption of terrestrial animals was observed for participants living in Nuuk compared to other towns. In comparison, significant higher intake frequency of fruit and vegetables were observed for participants living in Nuuk (Table 4). Nuuk and the other towns had different distributions regarding the percentage of median food intake for traditional and imported food, being 13 and 87% for participants in Nuuk, and 16 and 84% for participants living in other towns, respectively.
When comparing food intake frequency by the region where the participants had lived the longest, only the frequency of marine mammal intake was statistically significant different among regions (p = 0.027, not shown). Marine mammals were most frequently consumed in Disko bay (8.5 times/month, n = 25), followed by other Greenlandic regions (North, South, East) (8.0 times/month, n = 7), and West (5.3 times/month, n = 82), and less frequent by those who have lived > 50% of their life in other countries (1.8 times/month, n = 4). None of the other food groups differed by region (not shown).
Age differences (mothers and fathers pooled)
Table 5 shows the comparison of the median higher and lower age groups. The older age group (≥34.3 years) reported a more frequent intake of Greenlandic fish and fruit and less frequent intake of meat products and fast food compared to the younger age group (< 34.3 years) (Table 5). The two age groups had similar distributions regarding the percentage of median food intake for traditional and imported food, with 13 and 87% for the younger group and 14 and 86% for the older group (Table 5).
The age comparison stratified by gender showed similar tendencies as pooled data; however, only few of the results were significant (Additional file 3). Among mothers, Greenlandic fish intake was significantly lower in the younger age group (< 34.0y ears, 4.0 times/month) than in the older age group (≥34.0 years, 6.0 times/months) (p = 0.010) (Additional file 3: Table S3A). Among fathers, fruit was significantly lower in the younger age group (< 36.7 years, 5.8 times/month) than in the older age group (≥36.7 years, 14.3 times/months) (p = 0.015) (Additional file 3: Table S3B).
Correlations with socioeconomic and lifestyle factors (mothers and fathers pooled)
Several socioeconomic and lifestyle factors were significantly correlated with intake frequency of both traditional and imported food groups, and the correlations were weak to moderate (Fig. 3).

Spearman correlations between frequency intake of food groups and socioeconomic and lifestyle factors. Spearman correlation coefficients (rs in the upper line) with p-value for the correlation (below in smaller text size). Blue colors indicate negative correlations and red colors positive correlations, bold text indicate a significant correlation. Some variables were categorical with the following categories; 1Educational level (Primary School, High School, Technical college, and University), 2Personal income/ 3Household Income (< 100.000, 100.000–250.000, and > 250.000 DKK/year), 4Performing physical activities/sports (No and Yes), 5Current alcohol intake (0 drinks/week, 1–7 drinks/week, and ≥ 8 drinks/week), 6Smoking history (Never, Former, and Current). For Personal income, Household Income, and Alcohol intake the answer possibility “Don’t know” was omitted in the analysis
As shown in Fig. 3, socioeconomic factors (education and income) were generally positively correlated with the intake frequency of the food groups. High educational level was significantly positively correlated with frequent intake of Greenlandic fish, terrestrial animals, vegetables, and fruits, but negatively with carbohydrate foods. Significant positive correlations were also seen between high personal income and intake of terrestrial animals, vegetables, fruit, and sweets and snacks and between high household income and intake of shellfish and dried fish (Fig. 3).
For the lifestyle factors, BMI was positively correlated with seabird intake. Physical activity/sports was significantly positive correlated with intake of shellfish, berries, vegetables, fruit and sweets and snacks, and negatively with carbohydrate foods and sauce intake. High alcohol intake was correlated with terrestrial animals and sweets and snacks intake. Smoking history was correlated with several food groups. Current smokers had a less frequent intake of Greenlandic fish, shellfish, terrestrial animals, vegetables, and fruits than never smokers, but a more frequent fast food intake. Furthermore, the percentage of life in Greenland was significantly positive correlated with intake of marine mammals and carbohydrate foods and negatively with vegetables, fruit, and sweets and snacks (Fig. 3).
Changes from inclusion at pregnancy to the present follow-up (mothers only)
To assess changes from inclusion at pregnancy to follow-up for the mothers, the individual differences were calculated by subtraction intake at inclusion from intake at follow-up. The mothers generally reported similar intake at inclusion at pregnancy and follow-up (after 3–5 years) (Table 6). However, at follow-up, they reported significantly less frequent intake of seabirds and fruits and more frequent imported meat intake compared to inclusion at pregnancy (Table 6).
Spearman pairwise correlations for the food groups from inclusion at pregnancy and this follow-up study were all positive (Table 6). Most of the correlations were moderate, and the adjusted correlation coefficient ranged from 0.22 for berries to 0.53 for shellfish, except for meat products, which was weaker (rs = 0.035). All correlations were significant in the unadjusted analyses, except for meat products, while berries and carbohydrate foods were non-significant in the adjusted analyses. The correlation estimates were similar in the unadjusted and adjusted analyses (Table 6).
Discussion
In the present study, we followed up on the food intake of women included in the ACCEPT birth cohort and children’s fathers. The distribution between the intake frequency for traditional and imported food groups was 14 and 86%, respectively. Intake frequency for several of the food groups differed by gender (vegetables, fruit, and fast food), living town (terrestrial animals, vegetables, and fruits), and age (Greenlandic fish, meat products, fruits, and fast food). Socioeconomic and lifestyle factors significantly correlated with the intake frequency of both traditional and imported food groups. Smoking negatively correlated with intake of Greenlandic fish, shellfish, terrestrial animals, vegetables, and fruit and positively correlated with fast food intake. Generally, there were significant correlations in the food groups’ intake between the parents living together; however, the mothers reported a more frequent intake of vegetables and fruit and less for fast food. Few changes in the mother’s dietary habits from inclusion (at pregnancy) to this follow-up study (3–5 years later) were found, with less frequent intake of seabirds and fruit and more frequent meat intake.
In general, the proportion of traditional and imported food and the intake frequencies of the different food groups was similar to previously reported for the ACCEPT cohort [18, 19]. Compared to other studies in Greenland, more participants reported eating fish a least once a week in the present study (52.5%) than in the latest Population Health Survey from 2018 (42.8%) [17]. However, the percentage in the present study was comparable with two older Population Health Surveys from 2005 to 2010 (56.0%) and 2014 (50.2%) [16, 24]. The percentage reporting a daily fruit intake in the Population Health Surveys (2005–2010: 35.9%, 2014: 44.9%, and 2018: 35.9%) [16, 17, 24] are higher than the present study, where 30.8% consume fruit daily, with a difference between men (16.4%) and women (41.4%) (data not shown).
The health effects of the changing diet in Greenland is not fully understood. However, increased incidence in overweight and obesity in Greenland, may be linked to the western lifestyle and diet transition. Neither a diet consisting totally of traditional or imported food may be optimal for health in Greenland. The transition has resulted in increased consumption of sugar and saturated fat, and decreasing intake of n-3 fatty acids [5]. On the positive side, the intake of dietary fibre increased and the reduced intake of marine mammals and seabirds have resulted in reduced POP exposure. However, it must be noted that the POP exposure can be significantly reduced by omitting a few traditional food items (such as liver, kidney and blubber from seal and whales), without changing the intake of selenium and n-3 fatty acids significantly [25, 26].
Gender and parent differences in food intake
The intake frequency of traditional food groups was similar for mothers and fathers (Table 2); however, the percentage of traditional food was higher among the fathers (15%) compared to the mothers (13%). A similar difference between men and women has previously been seen in Greenland [24], as well as among other Indigenous populations, including the Sami population in Northern Norway [27] and the Eeyou Istchee communities in northern Quebec [28].
Mothers had significantly more frequent intake of fruit and vegetables and less frequent fast food intake (Table 2). These results are in line with previous observations, both in Greenland and internationally. Generally, studies find that women have a healthier lifestyle and diet [29, 30]. Among the Sami population in Northern Norway, fruit and vegetable intake positively correlated with the female gender [27]. In Greenland, women were more likely to comply with the national dietary guidelines [17], and the mean energy intake from fast food was higher for men (1850 kJ/day) than for women (1485 kJ/day) [24].
Among parents living together, intake from the food groups, both traditional and imported, was positively correlated (Table 3). However, mothers had a more frequent intake of vegetables and fruit and less frequent intake of fast food than the fathers, similarly to what was seen in the gender analyses (Table 2). The positive correlations are not surprising, as the parents share household larders and mostly consume main meals together. Other studies have found that couples tend to eat similar foods and have similar nutrient intakes [31,32,33,34,35,36,37]; however, female partners were often restricted in dinner choices by their male partners’ preferences for meat, fewer vegetables, and little food variety [38]. In the present study, the mothers reported a more healthy diet with more frequent intake of fruit and vegetables and less fast food intake than the fathers. The result may indicate that even though the parents most often eat together, the mothers more often eat fruit and vegetables as side dishes, whereas the fathers more often visit fast food places, for instance, at lunchtime.
Food differences by geographical area
The living place can affect the hunting possibility and the availability of traditional foods, and the degree of urbanization also influences the availability and supply of imported food. In the present study, terrestrial animal intake was lower in Nuuk than in the other towns (Sisimiut and Ilulissat), while vegetables and fruit were more frequent consumed in Nuuk. The percentage of traditional food was also higher among participants from the other towns (16%) than Nuuk (13%). The availability of the food items may very well explain these differences. Previously, the Population Health Surveys have reported that participants living in settlements were more likely to eat a meal from their own hunt/catch once a week (80%) than participants from towns (39%) and the main city Nuuk (20%) [24]. In compliance with the present study, in the study on Health Behavior in School-aged Children, the proportion of children eating fruit and vegetables daily was higher in Nuuk than in other towns and settlements [39].
In the ACCEPT cohort, geographical differences were investigated based on the region where the women had lived the longest and not by the current living place [18, 19]. Differences among regions were seen for terrestrial animals, berries, sauce, and fast food. Data from 2010 to 2011 showed a less frequent intake of terrestrial animals and berries in Disko Bay than in West, North, South, and East [18], but this difference was not seen during 2013–2015 [19] and neither in the present study. However, for terrestrial animals, we found that the participants living in Ilulissat (Disko Bay) did have a non-significantly less frequent intake (3.0 times/month) than participants living in Sisimiut (West, 5.0 times/month) and Nuuk (West, 3.5 times/month) (data not shown).
Age differences in food intake
The older age group (≥34.3 years) had a healthier lifestyle than the younger group (< 34.3 years), with more frequent fish and fruit intake and less frequent fast food intake. Similar results have been shown in other studies, internationally [40] and in Greenland [17,18,19, 24]. For the young population (18–24 years) in Greenland, the energy consumption from traditional food is lower, the intake of sugar and fast food is higher, and they are less likely to comply with the national dietary guidelines than the older population of ≥60 years of age [17, 24]. Similar to the results in the present follow-up study, at inclusion into the ACCEPT cohort, the younger pregnant women did also have a more frequent fast food intake than the older pregnant women [18, 19]. Thus, the present study is in accordance and confirms previous studies in Greenland.
Correlations with socioeconomic and lifestyle factors
Participants with high socioeconomic status seem to have a healthier lifestyle than participants with low socioeconomic status. High socioeconomic status (high educational level and high income) positively correlated with more frequent intake of Greenlandic fish, shellfish, dried fish, terrestrial animals, vegetables, and fruit. However, high personal income was also correlated with more frequent intake of sweets and snacks. Other studies have also shown that high educational status tends to correlate with consumption of a better-quality diet [41, 42]. In Greenland, occupation was previously associated with food insecurity (experienced times without any food or money to buy within the last 12 months) among adults, with more unemployed having experienced food insecurity (33%) compared to hunters/fishers (12%) and skilled/trained workers (4%) [16].
We also found that lifestyle factors (BMI, physical/sport activity, alcohol intake, and smoking history) correlated with the intake of several food groups. Only intake of seabird was significantly correlated with BMI. Physical/sport activities correlated positively with shellfish, berries, vegetables, fruit and sweets and snacks but negatively with carbohydrate food and sauce. Furthermore, alcohol intake correlated positively with the intake of terrestrial animals and sweets and snacks. Current smoking was negatively correlated with intake of Greenlandic fish, shellfish, terrestrial animals, vegetables, and fruit, but positively with fast food. Cigarette smoking is a significant source of oxidative stress. One potential mechanism for its problematic health effects is that smoking contributes to endogenous oxidant formation through the inflammatory-immune response [43, 44]. Thus, it is worrying that current smoking is negatively associated with vegetable and fruit intake, as antioxidants consumed in the diet may act to mitigate against some of the adverse effects of cigarette smoking [45]. Other studies have shown that smokers have lower blood levels of antioxidants (ascorbic acid, α-carotene, β-carotene, vitamin A and E) than non-smokers [45], which might be due to both the oxidants in cigarette smoke and lower intake of antioxidants in smokers than non-smokers [45]. Smoking continues to be a public health problem in Greenland with more than half of the general population being current smokers [17] and 29–46% of the pregnant women in the ACCEPT cohort (2010–2015) smoked during pregnancy [18, 19]. A connection of smoking with an unhealthy diet may worsen the health problems further.
Changes from inclusion at pregnancy to this follow-up study (3–5 years later)
Overall, the food intake frequency of both the traditional and imported food groups in the present follow-up study was similar to previously reported frequencies in the ACCEPT birth cohort [18, 19].
However, the individual intake frequency of fruit has decreased with a median of 1.5 times/months from pregnancy to this follow-up study, and meat intake increased a median of 2.5 times/month. The decreased frequency in fruit intake may be due to several factors. It may be explained by a decreased fruit intake in the general population seen in the same period in the Population Health Surveys [16, 17], or the women may have been more aware of having a healthy lifestyle during their pregnancy. A Canadian study investigated dietary changes during pregnancy and found that pregnant women reported increasing intake of milk products, fruit, and sweet items and decreased or eliminated intake of caffeine, alcohol, and meats during pregnancy [46]. Increased fruit intake during pregnancy has also been reported in several other studies (reviewed by SE Hillier and EK Olander [47]). In line with the increase in meat intake in the present follow-up study from inclusion at pregnancy, the Canadian study found decreased or eliminated meat intake during pregnancy, which were mainly due to concern for the baby’s health, aversion, and nausea [46].
It is, to our knowledge, the first time that longitudinal dietary changes are reported in Greenland. The results may suggest that the women changed their diet during pregnancy and that the dietary habits have “normalized” to non-pregnancy habits after pregnancy. However, we do not have any measurements of the women’s intake before pregnancy, and it is possible that the women did not change diet during pregnancy but have changed the diet afterward.
Strengths and limitations of the study
To estimate the food intake of the different food groups, participants were asked to fill out the FFQ with 65 traditional and imported food items based on their intake during the last 12 months. FFQ is a widely used dietary assessment method, especially in epidemiological studies, and compared to other dietary assessment methods, it is relatively simple, cost-effective, and time-efficient. The self-reported food intake may be subject to recall bias, as the participants must remember their intake 12 months back in time, which can be difficult. The portion size was not included in the questionnaire, and it is possible that the individual amount consumed differs, even though we do not see any difference in the frequency. However, other studies have reported that the between-person variation in portion size was smaller and less important than the variation in frequency [48]. A previous study in Greenland found good agreement between a very similar FFQ and duplicate portions, even though there was a slight overestimation of traditional food and underestimation of sweets in the FFQ [4]. Due to lack of nutritional data for some food items and missing portion sizes and seasonal information, we have not been able to calculate the nutritional intake for the participants and compare with Nutrition Recommendations.
For some of the Greenlandic food items, intake may depend on hunting season and availability; thus, we tried to include the seasonal variation in the FFQ. However, season information was missing for 5–56% in the Greenlandic food items, and we were unable to include the information in the analyses. However, looking at the available seasonal information (Additional file 2: Table S2B), the season variation was limited for most items, but for some items, the differences between the percentage of eating the food item in spring/summer and autumn/winter were more than 15%. For seabirds (guillemot, common eider, and kittiwake), hare and grouse more participants reported intake in the autumn/winter than in spring/summer, while some marine mammals (minke whale, fin whale, porpoise/grind and hooded seal), champs, and some fish (capelin and trout) were eaten by more participants in the spring/summer than in the autumn/winter.
Due to limited funding and the logistic difficulties connected with data collection in the remote settlements in Greenland, we could only follow up on the families in the three biggest towns (Nuuk, Sisimiut, and Ilulissat). However, Greenlandic statistic reports show that 50% of the Greenlandic population live in these three towns, with a distribution (64% living in Nuuk, 19% in Sisimiut, and 16% in Ilulissat) comparable with the distribution in the present study (67% in Nuuk, 21% in Sisimiut, and 11% in Ilulissat) [49]. Thus, even though the present study results may not reflect the food intake for the total Greenlandic population, the study population represents at least half of the Greenlandic population with a distribution reflecting the population among the included towns.
In the general Greenlandic population, a more western lifestyle and higher socioeconomic status are generally seen in the towns, especially in Nuuk [17]. Due to the fact that only ACCEPT women in Ilulissat, Sisimiut and Nuuk were followed up in this study, they differed slightly from the ACCEPT birth cohort women (2013–2015) not included in this ACCEPT follow-up study; the women included in this follow-up study were older at delivery (median: 29.2 versus 27.4, p = 0.001), less likely to smoke during pregnancy (20.6% versus 38.6%, p = 0.001), had higher educational level (66.3% with technical college or university degree versus 42.3%, p < 0.001) and had higher marine food intake as indicated by the n-3/n-6 fatty acids ratio (median: 0.24 versus 0.21, p = 0.001) (data not shown). The women included in this study were similar to the non-included ACCEPT women with regard to BMI, parity, and alcohol consumption (before and during pregnancy) at inclusion (data not shown).
Conclusion
In the present study, we follow-up on 101 women included in the ACCEPT birth cohort (2013–2015) to assess the current dietary intake for the mother and the children’s fathers using a FFQ including traditional Greenlandic food items and imported food items. Comparable to previously data in the ACCEPT cohort [18, 19] and other Greenlandic studies [17], the distribution between the intake frequency for traditional and imported food groups was 14 and 86%, respectively. In line with other studies, mothers seem to have more healthy dietary habits, although significant positive correlations were seen between parents living together. Age, living town, and several socioeconomic and lifestyle factors were related to the food frequency intake. This indicates that social classes highly influence the dietary habits, participants with higher education generally have healthier dietary habits, while current smokers generally eat more unhealthy food than never smokers.
The results from the present follow-up study suggest that the women changed their diet during pregnancy and that the dietary habits seems to go back to non-pregnancy habits after pregnancy. This suggest that some of the women adapted to the food recommendations given to pregnant women in Greenland. However, a study with dietary information before, during and after pregnancy is needed to confirm this.
For further diet recommendations, it is important to monitor the dietary and lifestyle habits frequently to follow the transition in Greenland. The health implications of the ongoing dietary transition in Greenland are complex, as both traditional and imported food can positively and negatively affect health, and the cultural aspect of traditional food intake must as well be taken into consideration. However, by omitting a few traditional food items (from seal and whale), the beneficial nutritional factors from the traditional diet can be kept while the intake of contaminants are reduced.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due to identifiable content, but are available from the corresponding author on reasonable request and ethical and legal approval.
Abbreviations
- ACCEPT:
-
Adaptation to Climate Change, Environmental Pollution, and dietary Transition
- BMI:
-
body mass index
- FFQ:
-
food frequency questionnaire
- n-3:
-
Omega 3 fatty acids
- POPs:
-
persistent organic pollutants
References
Tauber H. Age and diet of the mummified eskimos from Qilakitsoq. Meddr Grønland Man Soc. 1989;12:137–8.
Hansen JC, Deutch B, Odland JO. Dietary transition and contaminants in the Arctic: emphasis on Greenland. Int J Circumpolar Health. 2008;67(sup2):1–98.
Mulvad G: Food security in Greenland. In: Northern and Indigenous Health and Health Care. Edn. Edited by Exner-Pirot H, Norbye B, Butler L: Saskatoon, Saskatchewan: University of Saskatchewan; 2018: Available from: openpress.usask.ca/northernhealthcare.
Deutch B, Dyerberg J, Pedersen HS, Aschlund E, Hansen JC. Traditional and modern Greenlandic food - dietary composition, nutrients and contaminants. Sci Total Environ. 2007;384(1–3):106–19. https://doi.org/10.1016/j.scitotenv.2007.05.042.
Jeppesen C, Bjerregaard P. Consumption of traditional food and adherence to nutrition recommendations in Greenland. Scand J Public Health. 2012;40(5):475–81. https://doi.org/10.1177/1403494812454467.
Li K, Huang T, Zheng J, Wu K, Li D. Effect of marine-derived n-3 polyunsaturated fatty acids on C-reactive protein, interleukin 6 and tumor necrosis factor α: a meta-analysis. PLoS One. 2014;9(2):e88103. https://doi.org/10.1371/journal.pone.0088103.
Laird E, McNulty H, Ward M, Hoey L, McSorley E, Wallace JMW, et al. Vitamin D deficiency is associated with inflammation in older Irish adults. J Clin Endocr Metab. 2014;99(5):1807–15. https://doi.org/10.1210/jc.2013-3507.
Jain AP, Aggarwal KK, Zhang PY. Omega-3 fatty acids and cardiovascular disease. Eur Rev Med Pharmacol Sci. 2015;19(3):441–5.
Skaaby T, Thuesen BH, Linneberg A. Vitamin D, cardiovascular disease and risk factors. Adv Exp Med Biol. 2017;996:221–30. https://doi.org/10.1007/978-3-319-56017-5_18.
Helland IB, Smith L, Saarem K, Saugstad OD, Drevon CA: Maternal supplementation with very-long-chain n-3 fatty acids during pregnancy and lactation augments children's IQ at 4 years of age. Pediatrics 2003, 111(1):e39–e44, 1, DOI: https://doi.org/10.1542/peds.111.1.e39.
Strickland AD. Prevention of cerebral palsy, autism spectrum disorder, and attention deficit-hyperactivity disorder. Med Hypotheses. 2014;82(5):522–8. https://doi.org/10.1016/j.mehy.2014.02.003.
AMAP: AMAP Assessment 2015: Human Health in the Arctic. Arctic Monitoring and Assessment Programme (AMAP), Oslo, Norway. In., vol. vii + 165 pp.; 2016.
Bank-Nielsen PI, Long M, Bonefeld-Jørgensen EC. Pregnant Inuit Women’s Exposure to Metals and Association with Fetal Growth Outcomes: ACCEPT 2010–2015. Int J Environ Res Public Health. 2019;16(7):1171. https://doi.org/10.3390/ijerph16071171.
Hjermitslev MH, Long M, Wielsoe M, Bonefeld-Jorgensen EC. Persistent organic pollutants in Greenlandic pregnant women and indices of foetal growth: the ACCEPT study. Sci Total Environ. 2019;698:134118.
Bjerregaard P, Mulvad G. The best of two worlds: how the Greenland Board of Nutrition has handled conflicting evidence about diet and health. Int J Circumpolar Health. 2012;71(1):18588. https://doi.org/10.3402/ijch.v71i0.18588.
Dahl-Petersen IK, Larsen CVL, Nielsen NO, Jørgensen ME, Bjerregaard P. Befolkningsundersøgelsen i Grønland 2014. Levevilkår, livsstil og helbred. In: Statens Institut for Folkesundhed, Syddansk Universitet; 2016.
Larsen CVL, Hansen CB, Ingemann C, Jørgensen ME, Olesen I, Sørensen IK, et al. Befolkningsundersøgelsen i Grønland 2018. Levevilkår, livsstil og helbred. In: Statens Institut for Folkesundhed, Syddansk Universitet; 2019.
Knudsen AK, Long M, Pedersen HS, Bonefeld-Jorgensen EC. Lifestyle, reproductive factors and food intake in Greenlandic pregnant women: the ACCEPT - sub-study. Int J Circumpolar Health. 2015;74(1):29469. https://doi.org/10.3402/ijch.v74.29469.
Terkelsen AS, Long M, Hounsgaard L, Bonefeld-Jorgensen EC. Reproductive factors, lifestyle and dietary habits among pregnant women in Greenland: the ACCEPT sub-study 2013-2015. Scand J Public Health. 2017;1403494817714188.
WHO: Diet, nutrition, and the prevention of chronic diseases report of a joint WHO/FAO expert consultation: World Health Organization; 2003.
Wielsøe M, Gudmundsdottir S, Bonefeld-Jorgensen EC. Reproductive history and dietary habits and breast cancer risk in Greenlandic Inuit: a case control study. Public Health. 2016;137:50–8. https://doi.org/10.1016/j.puhe.2016.06.016.
Andersen S, Hvingel B, Kleinschmidt K, Jorgensen T, Laurberg P. Changes in iodine excretion in 50-69-y-old denizens of an Arctic society in transition and iodine excretion as a biomarker of the frequency of consumption of traditional Inuit foods. Am J Clin Nutr. 2005;81(3):656–63. https://doi.org/10.1093/ajcn/81.3.656.
Schaebel LH, Vestergaard H, Laurberg P, Rathcke CN, Andersen S. Intake of traditional Inuit diet vary in parallel with inflammation as estimated from YKL-40 and hsCRP in Inuit and non-Inuit in Greenland. Atherosclerosis. 2013;228(2):496–501. https://doi.org/10.1016/j.atherosclerosis.2013.03.022.
Bjerregaard P, Aidt EC. Levevilkår, livsstil og helbred - Befolkningsundersøgelsen i Grønland 2005–2009. Institut for Folkesundhed: København; 2010.
Laird BD, Goncharov AB, Egeland GM, Chan HM. Dietary advice on Inuit traditional food use needs to balance benefits and risks of mercury, selenium, and n3 fatty acids. J Nutr. 2013;143(6):923–30. https://doi.org/10.3945/jn.112.173351.
Johansen P, Muir D, Asmund G, Riget F. Human exposure to contaminants in the traditional Greenland diet. Sci Total Environ. 2004;331(1–3):189–206. https://doi.org/10.1016/j.scitotenv.2004.03.029.
Petrenya N, Rylander C, Brustad M. Dietary patterns of adults and their associations with Sami ethnicity, sociodemographic factors, and lifestyle factors in a rural multiethnic population of northern Norway - the SAMINOR 2 clinical survey. BMC Public Health. 2019;19(1):1632. https://doi.org/10.1186/s12889-019-7776-z.
Noreen W, Johnson-Down L, Jean-Claude M, Lucas M, Robinson E, Batal M. Factors associated with the intake of traditional foods in the Eeyou Istchee (Cree) of northern Quebec include age, speaking the Cree language and food sovereignty indicators. Int J Circumpolar Health. 2018;77(1):1536251. https://doi.org/10.1080/22423982.2018.1536251.
Rossaneis MA, Haddad Mdo C, Mathias TA, Marcon SS. Differences in foot self-care and lifestyle between men and women with diabetes mellitus. Revista latino-americana de enfermagem. 2016;24:e2761.
Varì R, Scazzocchio B, D'Amore A, Giovannini C, Gessani S, Masella R. Gender-related differences in lifestyle may affect health status. Annali dell'Istituto superiore di sanita. 2016;52(2):158–66. https://doi.org/10.4415/ANN_16_02_06.
Eastwood MA, Brydon WG, Smith DM, Smith JH. A study of diet, serum lipids, and fecal constituents in spouses. Am J Clin Nutr. 1982;36(2):290–3. https://doi.org/10.1093/ajcn/36.2.290.
Hur YM, Bouchard TJ Jr, Eckert E. Genetic and environmental influences on self-reported diet: a reared-apart twin study. Physiol Behav. 1998;64(5):629–36. https://doi.org/10.1016/S0031-9384(98)00101-2.
Kolonel LN, Lee J. Husband-wife correspondence in smoking, drinking, and dietary habits. Am J Clin Nutr. 1981;34(1):99–104. https://doi.org/10.1093/ajcn/34.1.99.
Lee J, Kolonel LN. Nutrient intakes of husbands and wives: implications for epidemiologic research. Am J Epidemiol. 1982;115(4):515–25. https://doi.org/10.1093/oxfordjournals.aje.a113333.
Louk KR, Schafer E, Schafer RB, Keith P. Comparison of dietary intakes of husbands and wives. J Nutr Educ Behav. 1999;31(3):145–52. https://doi.org/10.1016/S0022-3182(99)70421-8.
Lyu LC, Huang SH, Hsu CY, Lee MS, Lin SH. Inter-relationships of nutrient intakes for urban Chinese spouses in Taiwan. Int J Food Sci Nutr. 2004;55(3):227–36. https://doi.org/10.1080/09637480410001733851.
Brummett BH, Siegler IC, Day S, Costa PT. Personality as a predictor of dietary quality in spouses during midlife. Behav Med. 2008;34(1):5–10. https://doi.org/10.3200/BMED.34.1.5-10.
Brown JL, Miller D. Couples' gender role preferences and Management of Family Food Preferences. J Nutr Educ Behav. 2002;34(4):215–23. https://doi.org/10.1016/S1499-4046(06)60096-1.
Niclasen B: HBSC Greenland - Data fra Skolebørnsundersøgelsen 2018. In Statens Institut for Folkesundhed, SDU; 2019.
Hjartåker A, Lund E. Relationship between dietary habits, age, lifestyle, and socio-economic status among adult Norwegian women. The Norwegian women and Cancer study. Eur J Clin Nutr. 1998;52(8):565–72. https://doi.org/10.1038/sj.ejcn.1600608.
Robinson SM, Crozier SR, Borland SE, Hammond J, Barker DJ, Inskip HM. Impact of educational attainment on the quality of young women's diets. Eur J Clin Nutr. 2004;58(8):1174–80. https://doi.org/10.1038/sj.ejcn.1601946.
Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr. 2008;87(5):1107–17. https://doi.org/10.1093/ajcn/87.5.1107.
Cross CE, van der Vliet A, Eiserich JP. Cigarette smokers and oxidant stress: a continuing mystery. Am J Clin Nutr. 1998;67(2):184–5. https://doi.org/10.1093/ajcn/67.2.184.
MacNee W. Oxidants/antioxidants and COPD. Chest. 2000;117(5 Suppl 1):303S–17S. https://doi.org/10.1378/chest.117.5_suppl_1.303S-a.
Alberg A. The influence of cigarette smoking on circulating concentrations of antioxidant micronutrients. Toxicology. 2002;180(2):121–37. https://doi.org/10.1016/S0300-483X(02)00386-4.
Forbes LE, Graham JE, Berglund C, Bell RC. Dietary Change during Pregnancy and Women’s Reasons for Change. Nutrients. 2018;10(8):1032.https://doi.org/10.3390/nu10081032.
Hillier SE, Olander EK. Women's dietary changes before and during pregnancy: a systematic review. Midwifery. 2017;49:19–31. https://doi.org/10.1016/j.midw.2017.01.014.
Shim JS, Oh K, Kim HC. Dietary assessment methods in epidemiologic studies. Epidemiol Health. 2014;36:e2014009.
Grønlands statistik. https://www.bank.stat.gl/bedst4. Accessed 9 Oct 2020.
Acknowledgments
The authors thank all the participating families. We gratefully acknowledge the health nurse visitors at “Sundhedsplejen” in Nuuk and Sisimiut and the staff at the clinical hospital laboratory at The Regional Hospital Sisimiut and Dronning Ingrid’s Hospital in Nuuk, Greenland. The authors would also like to thank colleagues at the Centre for Arctic Health & Molecular Epidemiology, Department of Public Health, Aarhus University for their scientific support.
Funding
The establishment of the ACCEPT cohort was funded by the Danish Environmental Protection Agency (MST-112-00225 & MST-112-00289), and the follow-up was funded by the Danish Environmental Protection Agency (MST-113-00092) under the Danish Cooperation for Environment in the Arctic (DANCEA) programme.
Author information
Authors and Affiliations
Contributions
MW contributed to the data collection, planning of the study, entering of the questionnaire data into EPIDATA, performed the statistical analyses, interpreted the results, wrote the first manuscript draft, and was involved in the final manuscript editing. DB contributed to the data collection and reviewed and commented on the final manuscript draft. GM was project consultant on the data collection and reviewed and commented on the final manuscript draft. SI contributed to the data collection and reviewed and commented on the final manuscript draft. ML contributed to interpreting of the results, reviewed and commented on the drafts, and was involved in the final editing of the manuscript. ECB-J coordinated the overall project, was principal investigator on the research funding, contributed to the data collection, planning of the study, interpreting of the results, reviewed and commented on manuscripts, and was involved in the final editing of the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was carried out in accordance with the Helsinki convention II, and was approved by the Commission for Scientific Investigations in Greenland (KVUG 2019–04). After receiving a detailed description of the study, all participants gave signed informed consent to participate. They were informed that they could withdraw their consent at any time in the process and that their participation was voluntary.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wielsøe, M., Berthelsen, D., Mulvad, G. et al. Dietary habits among men and women in West Greenland: follow-up on the ACCEPT birth cohort. BMC Public Health 21, 1426 (2021). https://doi.org/10.1186/s12889-021-11359-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-021-11359-7