
Abstract
Background
Hypertension is becoming an increasingly common health issue worldwide, especially in countries in Sub-Saharan Africa. Hypertension is the leading risk factor for premature death and disability worldwide, and it is the leading risk factor for mortality from cardiovascular diseases worldwide. The data on hypertension in Sudan that has been published is limited. We conducted this study to assess the prevalence of hypertension and its associated risk factors.
Methods
A multistage sampling survey was conducted in Gadarif, Eastern Sudan, from January to May 2018 to investigate the prevalence of hypertension and associated factors in adults in Eastern Sudan. The World Health Organization (WHO) three-level stepwise approach questionnaire was used to gather sociodemographic characteristics (age, sex, height, weight marital status, education level, smoking habit, alcohol consumption habit, and family history of hypertension). Hypertension was defined as the presence of an average blood pressure of ≥140/90 mmHg or the reported use of anti-hypertensive medications for high blood pressure.
Results
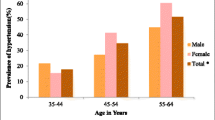
A total of 600 participants (mean age: 44.9 years) were enrolled in this study. Four hundred twenty-two (70.3%) participants were women, and 196 (32.7%) participants were obese. Of the 600 enrolled participants, 245 (40.8%) individuals had hypertension, 44 (7.3%) had been previously diagnosed with hypertension, and 201 (33.5%) were newly diagnosed with hypertension. A logistic regression analysis showed no significant associations across the education level, marital status, overweight and hypertension factors. However, an older age (adjusted OR = 3.20, 95% CI = 2.28–4.51, P < 0.001) and obesity (adjusted OR = 2.41, 95% CI = 1.57–3.69, P < 0.001) were associated with the presence of hypertension.
Conclusion
There is a high rate of hypertension in Eastern Sudan, especially among older and obese individuals. Preventive measures, such as dietary measures, should be implemented.
Similar content being viewed by others

Background
It has been estimated that one out of four adults worldwide (1.39 billion people) have hypertension, and this rate is expected to increase as a result of various epidemiological and demographic factors, such urbanization, especially in low- and middle-income countries [1]. Approximately 74.7 million individuals have hypertension in Sub-Saharan Africa (SSA), and this number is expected to reach 125.5 million individuals by 2025 [2]. High blood pressure is the leading risk factor worldwide for premature death and disability measured in disability adjusted life years (DALYs) [3]. Hypertension is the leading risk factor worldwide for mortality from cardiovascular diseases, such as stroke and ischaemic heart disease [4, 5]. Various factors, such as an individual’s age [6, 7], smoking [8], consuming alcohol [9] and obesity [8, 10,11,12], were reported as factors associated with hypertension.
The prevalence of hypertension varies widely across countries and across regions within the same country. Thus, there is a need to assess the epidemiology (prevalence and risk factors) of hypertension in different settings. Investigating the epidemiology of hypertension is of paramount importance for health planners and academics, as well as physicians.
The epidemiology of hypertension (prevalence and associated risk factors) has been extensively investigated in many African countries, e.g., Ethiopia [9, 10], Tanzania [13], Uganda [14] and Madagascar [12], but little published data exist on the epidemiology of hypertension in Sudan [6, 7, 15]; in addition, there are no published data on the prevalence of and risk factors for hypertension in Eastern Sudan. The current study was conducted to investigate the prevalence and associated factors of hypertension in Gadarif in Eastern Sudan.
Methods
Study area
Gadarif is located on the Ethiopian and Eritrean borders. It is 400 km from the capital of Sudan (Khartoum). It is located at an altitude of 496 m above sea level between latitudes 14° and 16° north and longitudes 33° and 36° east. Gadarif has a population of 1,727,401 inhabitants.
Study design and sampling
A multistage sampling survey was conducted in Gadarif, Eastern Sudan from January to May 2018. Initially, four localities (lowest administrative units in Sudan) were randomly selected from the 11 localities of Gadarif. Five districts within each locality were chosen using the systematic sampling method. Then, 150 subjects from 15 households from each district were selected based on the lottery method. The first member in each household who agreed to participate and met our inclusion criteria was elected. If the selected household was not inhabited or the inhabitants refused to participate, the next household was selected until the target number of subjects for the study was met. Two trained general practitioners were recruited to collect the data and perform the clinical examinations under the supervision of the primary investigator.
After signing an informed consent form, all adult (aged ≥ 18 years) Sudanese residents (including both the men and women) who were selected from households using a lottery method were enrolled in the study. Participants aged younger than 18 years, pregnant women, patients with poor cognitive functions and severely ill patients were excluded from this survey.
Data collection
The World Health Organization (WHO) three-level stepwise approach questionnaire was used for data collection [16]. The questionnaire was used to gather data on the sociodemographic characteristics of the participants, including their age; sex; marital status, which was categorized as married, divorced or unmarried; education level (≤ secondary level or > secondary level); and family history of hypertension. In addition, smokers were identified as those “who had smoked more than 100 cigarettes in their lives and reported smoking in the past year” [17], and participants who consumed alcohol were identified as those who consumed “one or more drinks in the past month”.
Procedures
Blood pressure was measured using an appropriate cuff size and a standard mercury sphygmomanometer after the participant rested for at least 10 min in a sitting position and with his or her arm resting at the level of the heart. With an appropriately sized cuff, the mean of two (at an interval of 1–2 min) blood pressure readings was calculated. If the difference between the two readings was > 5 mmHg, the blood pressure was measured again until the readings were consistent.
Patients were considered hypertensive if the reading for systolic BP was ≥140 mmHg, that for diastolic BP was ≥90 mmHg, or both criteria were met in both of the repeated measurements [18]. Each patient’s weight was measured in kilograms using (well-calibrated scales and adjusted to zero before each measurement) standard procedures; the person stood with minimal movement and his or her hands by his or her side. Moreover, the participants’ shoes and excess clothing were removed. Then, their heights were measured in centimetres after they stood straight with their backs against the wall and their feet placed side by side. The body mass index (BMI) was computed using the equation weight/height (m2). The BMI was categorized according to the WHO classification as underweight (< 18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 (kg/m2) or obese (≥30.0 kg/m2) [19]. Participants with a BP of > 140/90 mmHg were given a document to be followed in the nearest health centre. The data were gathered through a questionnaire that we developed for this study (Additional file 1).
The sample size of 600 individuals was selected based on previous studies on the prevalence of hypertension in Sudan [6, 7, 15], where 25.0% of participants were expected to have hypertension. The proportions of the main proposed risk factor (obesity) were expected to be 37.5% for hypertensive individuals and 25% for nonhypertensive individuals. It was calculated that a difference of 5% at α = 0.05 with a power of 80% can be detected with a sample size of 600 participants. It was assumed that 10% of the individuals might not respond or might have incomplete data.
Statistical analysis
The software SPSS for Windows (version 20.0) was used to analyse the data. The chi-square test was used to compare the proportions between the participants who were diagnosed with hypertension and participants who did not have hypertension. A t-test and Mann-Whitney test were used to compare the continuous parametric and nonparametric data, respectively, between the two groups (hypertensive and nonhypertensive). Logistic regression analyses were performed with hypertension as the dependent variable and age, sex, marital status, education level, BMI and waist circumference as the independent variables. The independent variables were entered into the model if their univariate P value was < 0.20. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated, and a P value of less than 0.05 was considered statistically significant. Then, adjustments were performed using the backward likelihood ratio (LR) in the different models.
Ethics
The study received ethical approval from the Research Board at the Faculty of Medicine at the University of Gadarif in Sudan. The reference number is 2016/39. Written informed consent was obtained from all enrolled patients.
Results
General characteristics
Seventy-eight households were approached, and the response rate for inclusion in the study was 96.1% (75 households). Six hundred participants were enrolled in the survey, and the mean and SD of the age of the participants was 44.9 and 16.5 years. Four hundred twenty-two (70.3%) participants were women, and the remaining 178 (29.7%) were men. The basic characteristics of the enrolled individuals are shown in Table 1.
Of the 600 enrolled participants, 44 (7.3%) had been previously diagnosed with hypertension, and 201 (33.5%) were newly diagnosed with hypertension. Thus, in this survey, 245 (40.8%) individuals had hypertension (44 individuals were diagnosed previously, and 201 were newly diagnosed with hypertension).
The mean (95% CI) age [50.4 (48.4–52.3) years vs. 41.1 (39.4–42.8) years, P < 0.001] and the median (interquartile) of the BMI [28.6 (24.0–34.6) kg/m2 vs. 25.6 (21.7–29.7) kg/m2, P < 0.001] were significantly higher in the hypertensive individuals than in the nonhypertensive individuals.
There was no significant difference in the sex (P = 0.982), smoking (P = 0.606), alcohol consumption (P = 0.516) or family history of hypertension (P = 0.927) factors between the individuals with hypertension and those without hypertension. The patients with hypertension were more likely to be older, have a lower education level, be married and be obese (Table 2).
The logistic regression analysis showed no significant associations across the education level, marital status, overweight or hypertension factors. However, an older age (adjusted OR = 3.20, 95% CI = 2.28–4.51, P < 0.001) and obesity (adjusted OR = 2.41, 95% CI = 1.57–3.69, P < 0.001) were associated with hypertension (Table 3).
Discussion
The current study showed a high prevalence (40.8%) of hypertension in this region of Sudan. This result is consistent with the recent findings of one study, which reported that 39.6% of the village inhabitants in Northern Sudan had hypertension [20]. A similar rate (38.2%) of undiagnosed hypertension was reported in rural communities along the Nile River in Northern Sudan [6]. Approximately one-third (35.7%) of 954 individuals in Northern Sudan were found to have hypertension [7]. The high prevalence of hypertension in the different communities may be explained by improved statistics, increased awareness of hypertension [21], an increased prevalence of modern lifestyles that are associated with an increased prevalence of diabetes mellitus and obesity [22], and the widespread use of medication, such as steroids and non-steroidal anti-inflammatory drugs [23]. The prevalence rates of hypertension found in this study were much higher than those (15.9%) recently reported for four states (Khartoum, Gezira, Blue Nile, and Kassala) in Sudan [15]. Interestingly, a much higher prevalence (49.1%) of hypertension was reported among 513 adults in a rural setting in Madagascar [12].
Conversely, a lower rate (28.0%) of hypertension was reported in Tanzania [13] and in a population-based sectional study that enrolled 67,397 participants in Ethiopia (31.9%) [24]. In neighbouring Ethiopia, while a low rate (10.5%) of hypertension was reported in a hospital-based study [8], a prevalence rate of 34.7% for hypertension was reported in the capital, Addis Ababa [10]. In a meta-analysis of 43,025 older adults (> 53 years) in 15 African countries, it was reported that the overall pooled prevalence of hypertension was 57.0% (ranging from 22.3 to 90.0%) [25]. Differences in age, culture, dietary habits, behaviour, race and genetics in the different settings may explain the differences in the prevalence of hypertension in the various populations.
In the current study, an older age was associated with hypertension (adjusted OR = 3.20, 95% CI = 2.28–4.51). This result is consistent with the finding in a previous study, showing a significant association between an increasing age and the prevalence of hypertension in Northern Sudan [6]. A significant association between an increasing age and the prevalence of hypertension was reported in Northern Sudan [7]. Because of our study design (controlled for age), it might not be valid to compare our results (age and hypertension) with the results of the large study that was recently conducted in four states (Khartoum, Gezira, Blue Nile and Kassala) in Sudan [15]. Several studies have shown that an older age is significantly associated with hypertension in neighbouring countries, including Ethiopia [8, 9, 11], Tanzania [13] and Madagascar [12]. Similarly, a recent meta-analysis including 43,025 older adults (> 53 years) in 15 African countries showed that an older age is independently associated with hypertension [25]. The high prevalence of hypertension in elderly patients may be explained by the increased stiffness of the aorta and the other arteries as a result of the ageing process.
Our results showed that obese individuals had a 2.41 times higher risk for hypertension. A significant association between obesity and hypertension has been found in Northern Sudan [7]. Our finding showing an association between obesity and hypertension is consistent with the findings that were recently reported for four states (Khartoum, Gezira, Blue Nile and Kassala) in Sudan [15]. Several previous studies conducted in Africa—e.g., Uganda [14], Ethiopia [8, 10, 11] and Madagascar [12]—have reported significant associations between obesity and hypertension. In a recent meta-analysis of 43,025 adults in 15 African countries, overweight/obesity was shown to be independently associated with hypertension [25]. The association between obesity and hypertension may be explained by the increased plasma endothelin-1 and nitric oxide production and adiposity among obese individuals [26, 27]. Moreover, up to a 63% resolution of hypertension can be achieved by the reduction of one’s body weight [28, 29].
Our results and the results of a recent meta-analysis showed there is no association between an individual’s sex and the presence of hypertension [25]. In the current study, there were no significant associations between hypertension and the marital status, education level, alcohol consumption or smoking habit factors. No significant associations were found between hypertension and the marital status, education level, alcohol consumption or smoking habit factors in Uganda [14]. Previous studies have shown that smoking is associated with hypertension [8]. Interestingly, the rates for both smoking (2.5%) and alcohol consumption (0.33%) were low in our survey. Perhaps the rates of smoking and alcohol consumption were underestimated, as many individuals may not have been willing to reveal these habits.
Limitations
It is worth mentioning that our results should be compared with the results of other studies with caution; the differences in the participant selection method used, size of the study population, and lifestyles and ethnicities of the participants should be considered. This study required only two readings, and the time for which the test administrators needed to visit the households may have affected the selection of the participants. Perhaps the predominance of females (70.3%) in the current study population might be explained by the idea that more males than females were working during the time of the survey, and many females were housewives. Some factors, e.g., physical inactivity [11], dietary factors [10] and high fasting blood glucose levels [9], which have reportedly been associated with hypertension, were not explored in our survey, which should be considered limitations of the study.
Conclusion
There is a high prevalence of hypertension in Eastern Sudan, especially among older and obese individuals. Preventive measures, such as dietary measures, should be implemented.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- CI:
-
Confidence interval
- ORs:
-
Odds ratios
- SD:
-
Standard deviation
References
Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134:441–50.
Ogah OS, Rayner BL. Recent advances in hypertension in sub-Saharan Africa. Heart. 2013;99:1390–7.
GBD 2015 Risk Factors Collaborators MH, Afshin A, Alexander LT, Anderson HR, Bhutta ZA, Biryukov S, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1659–724.
Roth GA, Nguyen G, Forouzanfar MH, Mokdad AH, Naghavi M, Murray CJL. Estimates of global and regional premature cardiovascular mortality in 2025. Circulation. 2015;132:1270–82.
Feigin VL, Roth GA, Naghavi M, Parmar P, Krishnamurthi R, Chugh S, et al. Global burden of stroke and risk factors in 188 countries, during 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet Neurol. 2016;15:913–24.
Bushara SO, Noor SK, Elmadhoun WM, Sulaiman AA, Ahmed MH. Undiagnosed hypertension in a rural community in Sudan and association with some features of the metabolic syndrome: how serious is the situation? Ren Fail. 2015;37:1022–6.
Bushara S, Noor S, Ibraheem AA, Elmadhoun W, Ahmed M. Prevalence of and risk factors for hypertension among urban communities of North Sudan: detecting a silent killer. J Fam Med Prim Care. 2016;5:605.
Kassa A, Woldesemayat EM. Hypertension and diabetes mellitus among patients at Hawassa University comprehensive specialized hospital, Hawassa, Southern Ethiopia. Int J Chronic Dis. 2019;2019:1–8.
Abebe SM, Berhane Y, Worku A, Getachew A. Prevalence and associated factors of hypertension: a Crossectional community based study in Northwest Ethiopia. PLoS One. 2015;10:e0125210.
Abebe S, Yallew WW. Prevalence of hypertension among adult outpatient clients in hospitals and its associated factors in Addis Ababa, Ethiopia: a hospital based cross-sectional study. BMC Res Notes. 2019;12:87.
Awoke A, Awoke T, Alemu S, Megabiaw B. Prevalence and associated factors of hypertension among adults in Gondar, Northwest Ethiopia: a community based cross-sectional study. BMC Cardiovasc Disord. 2012;12:113.
Manus MB, Bloomfield GS, Leonard AS, Guidera LN, Samson DR, Nunn CL. High prevalence of hypertension in an agricultural village in Madagascar. PLoS One. 2018;13:1–12.
Galson SW, Staton CA, Karia F, Kilonzo K, Lunyera J, Patel UD, et al. Epidemiology of hypertension in northern Tanzania: a community-based mixed-methods study. BMJ Open. 2017;7:1–10.
Chin JH, Twinobuhungiro A, Sandhu A, Hootsmans N, Kayima J, Kalyesubula R. Determinants of hypertension in urban Uganda: a community-based case-control study. Ethn Dis. 2017;27:15.
Ali I, Behairy H, Abugroun A, Beaney T, Kobeissi E, Abdalla A, et al. May measurement month 2017: an analysis of blood pressure screening in Sudan—northern Africa and Middle East. Eur Hear J Suppl. 2019;21:D111–4.
Riley L, Guthold R, Cowan M, Savin S, Bhatti L, Armstrong T, et al. The World Health Organization STEPwise approach to noncommunicable disease risk-factor surveillance: methods, challenges, and opportunities. Am J Public Health. 2016;106:74–8.
CDC. Current Cigarette Smoking Among Adults in the United States | CDC. 2017.https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm (accessed 22 Nov2019).
Weber MA, Schiffrin EL, White WB, Mann S, Lindholm LH, Kenerson JG, et al. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich). 2014;16:14–26.
World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. ; 2000.
Al-Sofi S, Elamin S, Abu-Aisha H. Arab journal of nephrology and transplantation. Arab Society of Nephrology and Renal Transplantationhttps://www.ajol.info/index.php/ajnt/article/view/84345 (accessed 8 Jun2019).
Fang J, Gillespie C, Ayala C, Loustalot F. Prevalence of self-reported hypertension and antihypertensive medication use among adults aged ≥ 18 years - United States, 2011-2015. Morb Mortal Wkly Rep. 2018;67:219–24.
Inoue Y, Qin B, Poti J, Sokol R, Gordon-Larsen P. Epidemiology of obesity in adults: latest trends. Curr Obes Rep. 2018;7:276–88.
Aronow WS. Drug-induced causes of secondary hypertension. Ann Transl Med. 2017;5:349.
Abebe SM, Andargie G, Shimeka A, Alemu K, Kebede Y, Wubeshet M, et al. The prevalence of non-communicable diseases in Northwest Ethiopia: survey of Dabat health and demographic surveillance system. BMJ Open. 2017;7:e015496.
Bosu WK, Reilly ST, Aheto JMK, Zucchelli E. Hypertension in older adults in Africa: a systematic review and meta-analysis. PLoS One. 2019;14:e0214934.
Orlando A, Viazzi F, Giussani M, Nava E, Cazzaniga E, Bonino B, et al. Endothelin-1/nitric oxide balance and HOMA index in children with excess weight and hypertension: a pathophysiological model of hypertension. Hypertens Res Published Online First: March 2019. doi:https://doi.org/10.1038/s41440-019-0253-3.
He H, Pa L, Pan L, Simayi A, Mu H, Abudurexiti Y, et al. Effect of BMI and its optimal cut-off value in identifying hypertension in Uyghur and Han Chinese: a Biethnic study from the China National Health Survey (CNHS). Int J Hypertens. 2018;2018:1508083.
Pareek M, Bhatt DL, Schiavon CA, Schauer PR. Metabolic surgery for hypertension in patients with obesity. Circ Res. 2019;124:1009–24.
Chrysant SG. Pathophysiology and treatment of obesity-related hypertension. J Clin Hypertens. 2019;21:555–9.
Acknowledgements
We would like to thank the patients for participating in this study.
Funding
None received.
Author information
Authors and Affiliations
Contributions
SMO and IA conceived and designed the study. SMO and OEO recruited the participants. IRM, OSO performed the laboratory work. IRM and IA analysed the data and wrote the manuscript. All contributed authors of this original manuscript authorized the final version of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study received ethical approval from the Research Board at the Faculty of Medicine, University of Gadarif, Sudan. The reference number is 2016/39. Written informed consent was obtained from all the enrolled patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
questionnaire for the prevalence and associated factors of hypertension among adults in Gadarif in Eastern Sudan: a community based study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Omar, S.M., Musa, I.R., Osman, O.E. et al. Prevalence and associated factors of hypertension among adults in Gadarif in eastern Sudan: a community-based study. BMC Public Health 20, 291 (2020). https://doi.org/10.1186/s12889-020-8386-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-020-8386-5