
Abstract
Background
Hypertension is an emerging public health problem in Sub Saharan Africa (SSA) and urbanization is considered to favor its emergence. Given a paucity of information on hypertension and associated risk factors among urban slum dwellers in SSA, we aimed to characterize the distribution of risk factors for hypertension and investigate their association with hypertension in an urban slum in Kenya.
Methods
We conducted a community based cross-sectional survey among adults 35 years and older living in Kibera slum Nairobi, Kenya. Trained interviewers collected data on socio demographic characteristics and self reported health behaviours using modified World Health Organization stepwise surveillance questionnaire for chronic disease risk factors. Anthropometric and blood pressure measurements were performed following standard procedures. Multiple logistic regression was used for analysis and odds ratios with 95 % confidence intervals were calculated to identify risk factors associated with hypertension.
Result
A total of 1528 adults were surveyed with a mean age of 46.7 years. The age-standardized prevalence of hypertension was 29.4 % (95 % CI 27.0–31.7). Among the 418 participants classified as hypertensive, over one third (39.0 %) were unaware they had hypertension. Prevalence of current smoking and alcohol consumption was 8.5 and 13.1 % respectively. Over one quarter 26.2 % participants were classified as overweight (Body Mass Index [BMI] ≥25 to ≤29.9 kg/m2), and 17 % classified as obese (BMI ≥30 kg/m2). Overweight, obesity, current smoking, some level of education, highest wealth index, moderate physical activity, older age and being widowed were each independently associated with hypertension. When fit in a multivariable logistic regression model, being a widow [AOR = 1.7; (95 % CI, 1.1–2.6)], belonging to the highest wealth index [AOR = 1.6; (95 % CI, 1.1–2.5)], obesity [AOR = 1.8; 95 % CI, 1.1–3.1)] and moderate physical activity [AOR = 1.9; (95 % CI, 1.2–3.0)], all remained significantly associated with hypertension.
Conclusion
Hypertension in the slum is a public health problem affecting at least one in three adults aged 35–64 years. Age, marital status, wealth index, physical inactivity and body mass index are important risk factors associated with hypertension. Prevention measures targeting the modifiable risk factors associated with hypertension are warranted to curb hypertension and its progressive effects.
Similar content being viewed by others

Background
Hypertension has been identified as the leading risk factor for mortality worldwide [1]. Once regarded a problem only in high-income countries, hypertension is currently a global problem increasing the risk for cardiovascular diseases (CVD) in both wealthy and poor nations [2]. Over 80 % of the world’s deaths from CVD occur in low and middle-income countries [3]. In African adults the prevalence of hypertension has risen to rates similar to and sometimes exceeding that in many high income countries [4]. The increasing prevalence of hypertension in low income countries represent a substantial public health problem with associated economic and social impacts [5].
In Kenya the high rate of urbanization has led to emergence of slums and slum dwellers. The slums residents live below the poverty line and are referred to as the ‘urban poor’ [6]. The urban poor often adopt less healthy lifestyles. They are more sedentary than rural residents and tend to consume foods high in saturated fat, salt and sugar [7]. In addition, they have limited access to healthcare (especially when compared with wealthier urban residents), partly related to their poor purchasing ability which places them at a higher risk for complications resulting from untreated hypertension [8]. Underlying socioeconomic parameters also affect their exposure and vulnerability to hypertension risk factors [9]. Studies document higher prevalence of hypertension and its associated risk factors in urban areas compared to the rural areas [4, 10, 11].
Hypertension is not only a major risk factor for CVD but also an asymptomatic condition with its own risk factors [12]. In recent studies conducted in similar slums in Kenya [13, 14], there is marginal reporting on risk factors for hypertension. The present study aims to assess prevalence of these risk factors and their association with hypertension among adult slum dwellers living in Kibera Slum, Nairobi, Kenya.
Methods
Study area
The study was conducted in Kibera, one of Africa’s largest urban slums with an estimated population of 200,000 inhabitants [15]. The slum is approximately 2.5 km2 in size and is located approximately five kilometers south west of Nairobi, Kenya. The slum is further divided into 13 geographic demarcations called villages. Consistent with conditions in most urban slums, Kibera is characterized by sub-standard housing, poor security, insufficient garbage disposal, lack of formal sewers, overcrowding and inadequate water drainage [16].
Study design and procedures
We conducted a community based cross sectional study in Soweto, Gatwikira and Mashimoni villages in Kibera during the period June to August 2013. Soweto and Gatwikira villages have population range between 25,000 and 29,000 and are involved in active population based infectious disease surveillance, while the adjacent Mashimoni village has approximately 24,000 inhabitants. Details and activities of the surveillance population have been described elsewhere [17]. The study sample comprised of 1700 households randomly selected in equal numbers from the surveillance population and the adjacent village. Residency was defined as having lived in the selected villages for at least four consecutive months in a year. All adults residents aged 35–64 years within the selected households were eligible to participate in the study. Only one participant per household was enrolled into the study. Individuals less than 35 and older than 64 years were excluded from the study. Pregnant women, severely ill and bedridden residents were also excluded from the survey.
The survey data was collected using an adapted World Health Organization (WHO) stepwise surveillance questionnaire for chronic disease risk factors (STEPS) [18]. The WHO STEPS is a validated and standardized approach that can be applied in any setting depending on resources available and facilitates comparisons of risk factors within the country or across countries [19]. Eighteen research assistants who had completed their secondary school education were trained on interviewing skills and standard methods of anthropometric and blood pressure measurements.
Information on socio demographic variables and behavioral risk factors, such as tobacco-use, alcohol-use, physical exercise, and diet, were collected using the adapted questionnaire translated into Kiswahili (the local language). Education, occupation status and wealth index were used as independent measures of socio economic status. Wealth index was determined by possession of durable household assets, which included possession of a 1) radio 2) television 3) video player 4) mobile phone 5) refrigerator 6) sofaset 7) bicycle 8) motorcycle and/or access to 9) electricity and/or 10) gas. The principal components analysis (PCA), a standard approach that generates scores based on measures of the household assets was used to derive wealth index [20]. Using the PCA scores generated we classify the study population into wealth index quintiles indicating the poorest 20 % to the richest 20 %.
Measurements
Weight, height, waist and hip circumference measurements were performed using standardized methods. Height was measured to the nearest 0.1 cm using a portable Seca stadiometer. Weight was measured to the nearest 0.1 kg using a calibrated Seca weight scale with the participant dressed in light clothing and without shoes. Waist circumference (cm) was determined using Seca circumference tape measure placed on a horizontal plane at the level midpoint of the superior border of the iliac crest and the inferior margin of the last rib mid-axillary plane. Hip circumference (cm) measured at the widest portion of hips using Seca tape.
Blood pressure was measured on the left arm using a validated OMRON M6 digital automatic blood pressure monitor [21]. Respondents were asked to remain seated, relaxed, and blood pressure measurements taken as per WHO steps protocol. In summary three blood pressure measurements were taken with at least a 3 min interval between each measurement. The mean value of the 2nd and 3rd measurement was used for analysis [19]. Blood pressure (BP) was classified according to the Seventh Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VII) [22].
Data quality was controlled in the field by a team lead and the investigator. They performed random audits of the interviews and checked questionnaires for completeness and validity of data collected.
Operational definitions
Hypertension: defined as mean measured blood pressure of ≥140 mmHg systolic and/or the mean measured diastolic blood pressure of ≥90 mmHg or self-reported current use of hypertensive medications.
Awareness of hypertension: based on the subjects’ verbal report of a prior diagnosis of hypertension (or high blood pressure) by a health professional.
Treatment: verbal report on current use of medication for lowering elevated blood pressure.
Control: Blood pressure <140 systolic and <90 mmHg diastolic among the population defined as having hypertension and treated.
Body Mass Index (BMI): calculated as weight in kilograms divided by height in meters squared (weight (kg)/height (m2). BMI was categorized as per the World Health Organization guidelines [23], underweight (BMI <18.5), normal (BMI ≥18.5 to ≤ 24.9), overweight (BMI ≥ 25.0 to ≤ 29.9) or obese (BMI ≥30.0).
Waist circumference: was used as a measure of abdominal obesity. Waist-circumference ≥102 cm in men and ≥88 cm in women is defined as elevated and having abdominal obesity [24].
Smoking: Participants who smoked one or more cigarettes in the last 30 days were referred to as current smokers. Non smokers had never smoked any cigarette while ex-smokers who had stopped smoking more than one month before the survey.
Alcohol consumption: A show card with pictures was used to illustrate what was meant by a ‘standard’ drink, stated to be equivalent to 10 g of ethanol.
One standard drink: Equivalent to consuming half standard bottle of regular beer (500 ml), one single measure of spirits (30 ml) or one medium size glass of wine (120 ml).
Harmful alcohol consumption was defined as drinking ≥4 standard alcoholic beverages in a single occasion in the last 30 days for females and ≥5 standard drinks in a single occasion in the last 30 days among males [25].
Fruit and vegetable intake was considered insufficient if consumption was less than less than five servings per day [3].
Physical activity: Physical activity included questions on number of days and time spent on vigorous and/or moderate activities for work, travel and leisure activities. Physical activity responses were then converted to Metabolic Equivalent of Task (MET) minutes/week low activity: < 600 MET minutes per week, moderate activity: 600–1500 MET minutes per week and High activity: > 1500 MET minutes per week [18].
Statistical analyses
Data management and analysis were conducted using STATA software (version 12.0 (StataCorp LP, Texas, USA). The prevalence of hypertension was age standardized using WHO world population for people aged 15 years and above. Descriptive statistics were generated using cross-tabulations. The independent Student’s t -test was used for continuous variables and Chi-square tests were used to assess significant differences between categorical variables. Bivariate logistic regression was used to ascertain the individual influence of the risk factors on hypertension. Multivariate backward regression model was used to determine significant risk factors associated with hypertension. We report crude odds ratios (COR), adjusted odds ratios (AOR), and their respective 95 % confidence intervals (CI) as the measure of association.
Ethical considerations
We obtained the ethical clearance from Makerere University School of Public Health Higher Degrees Research and Ethics Committee and the Kenya Medical Research Institute (SSC No 2514 and CDC no 6529). Informed written consent was obtained from all participants. Participants having hypertension defined by our measurement were referred to nearby health facilities for further diagnosis and treatment.
Results
Table 1 describes the socio demographic characteristics of the respondents. Out of 1710 residents eligible for the survey, 1528 (89 %) adults participated, including 641 (42 %) males and 887 (58 %) females. The median age for male and female respondents was 42 (38–49) years and 45 (39–53) respectively. At least half (51.8 %) had completed the basic level of education. Most of the respondents 1041 (68.1 %) were permanent residents and had resided in the slum for more than 10 years.
Table 2 shows the overall and gender frequencies of risk factors of hypertension.
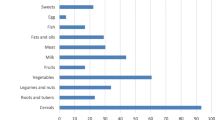
Dietary habits
A majority (1510; 98.8 %) of the study participants consumed insufficient amount of fruit and vegetables. In a typical week, fruits were consumed on average 3 days. At least 965 (63.3 %) participants consumed one serving of fruit daily, however 140 (9.1 %) did not consume any fruit at all in a typical week. Vegetables were consumed on average 6 days per week with a mean of 2.1 servings of vegetables consumed per day. Overall, only 5.5 and 4.2 % males and females, respectively, consumed ≥5 servings/day of fruits and/or vegetables.
In a typical week, almost half 737 (48.8 %) of the respondents reported that they consumed meals outside the home. More males, 67.8 % compared to females 34.9 % consumed meals prepared outside their homes.
Smoking
Current smoking was reported by 8.5 % of the participants. Males reported a nearly ten-fold higher prevalence of smoking 17.8 % (95 % CI 15.0–20.9) compared to females 1.8 % (95 % CI 1.1–2.9). Of the men who smoked, 75.7 % smoked daily. Smoking prevalence increased with age in both males and females. The mean age of initiation of smoking was 26 years in males and 18 years in females. The most common type of tobacco smoked was manufactured cigarettes 87 (66.9 %). Males smoked an average eight cigarettes daily while females smoked average five cigarettes daily. Only 21 (1.4 %) participants consumed smokeless tobacco. Though not statistically significant current smoking was prevalent among hypertensive participants compared to normotensive participants (10.1 % vs7.9 %; p = 0.185).
Alcohol consumption
Almost one third of the study population had ever consumed alcohol. In the past 12 months, 17 % reported consuming alcohol. The prevalence of current drinkers (alcohol consumption in the past 30 days) was four times higher for males (24.9 %) than females (5.9 %). On average, the study participants who currently consumed alcohol drank a mean of eight standard drinks in one sitting. A higher proportion of females (73.1 %) who drank alcohol consumed more than the recommended standard drink compared to males 67.3 %. In a typical day the most common type of alcohol consumed were local brews (changaa or busaa) (50.3 %) and beer (45.3 %). Similar proportion of hypertensive 61(14.9 %) and normotensive participants 150 (13.5 %) reported current consumption of alcohol (in the last 30 days).
Physical activity
The surveyed population was physically active. Prevalence of physical activity was distributed as follows; 4.1 % low physical activity, 76.4 % moderate physical activity and 19.6 % high physical More females 4.6 % (95 % CI 3.4–6.2) reported a higher prevalence of low physical activity compared to males 3.2 % (95 % CI 2.1–4.9) and was observed more among those who were unemployed. Similar proportion of hypertensive (4.2 %) and normotensive participants reported low physical activity.
Overweight and obesity
The prevalence of being overweight and obese was 26.2 and 17.3 %, respectively. Females had higher mean BMI than males (26 vs 22 kg/m2, p <0.001). The prevalence of obesity (BMI ≥30.0 kg/m2) among females was 4-fold higher than in males (25.9 % vs. 6.0 %, [PRR = 4.3 95 % CI 3.1–6.0]). Overall, 19.3 and 80.3 % of the males and females, respectively, had abdominal obesity. The overall prevalence of abdominal obesity was 54.6 %. Prevalence of hypertension differed significantly between obese and non-obese individuals (36.0 % vs. 25.8 %, p < 0.001).
Blood pressure
The distribution of blood pressure as per the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) classification [22] is shown in Table 3. The mean distribution of systolic blood pressure (SBP) and diastolic blood pressure (DBP) in males versus females was 131.4 ± 18.9 mmHg vs 128.1 ± 19.9 mmHg (p <0.001) and 81.5 ± 11.9 mmHg vs 81.7 ± 11.8 mmHg (p = 0.710) respectively. Mean SBP and DBP increased steadily with increasing age.
Prevalence of hypertension
The prevalence of hypertension in the overall sample was 27.4 % (95 % CI 25.2–29.6). The age standardized prevalence was 29.4 %, among females 32.5 % (95 % CI 29.1–35.8) and among males 27.8 % (95 % CI 24.3–31.2). The prevalence of hypertension increased linearly with age peaking at 55–64 years Fig. 1. The prevalence of hypertension was higher among males compared to females (17.1 % vs 21.5 %) in the 35–44 age category, while above 44 years the trend reverses with the prevalence of hypertension being higher in females compared to males (43.2 % vs 27.8 %).

Prevalence of Hypertension by Age and Gender. *p < 0.001
Awareness treatment and control of hypertension
Overall 886 (58.0 %, 95 % CI 35.1–37.9 %) of the study participants indicated that they ever had their blood pressure measured. Females were more likely to have ever had their blood pressure measured compared to males [38.3 % vs19.6 %]. Among the 418 people that had hypertension 163 (39.0 %, 95 % CI 34.3–43.9) were aware that they have the condition and awareness was high among the females compared to males [29.2 % vs 9.8 %]. Of those aware of their hypertension, 119 (73.0 %, 95 % CI 65.5–79.6) were on treatment within two weeks of the interview. Control among those on treatment was achieved by 51 (42.8 %). Females were more likely than males to be aware of hypertension, as well as to be treated and controlled.
Factors associated with hypertension
Table 4 illustrates the risk factor associated with hypertension. Overweight, obesity, current smoking, some level of education, highest wealth index, moderate physical activity, older age and being widowed were each independently associated with hypertension.
The likelihood of hypertension increased with advancing age. Participants above 55 years were approximately five times [AOR = 4.9, (95 % CI, 3.6–6.8)] more at risk of hypertension compared to participants aged 34–44 years. In the logistic regression model adjusted for age and gender, widowed respondents had a 20 % greater risk of having hypertension [AOR =2.0, (95 % CI 1.4–2.9)] as compared to the married respondents. Wealth index was positively associated with hypertension. Participants considered the richest had increased odds of hypertension compared to their counterparts belonging to the middle wealth index [AOR = 1.6, (95 % CI: 1.1–2.5.
Body mass index above 25 kg/m2 was associated with hypertension. Being overweight or obese increased the odds of hypertension by [AOR = 1.7, (95 % CI: 1.5–2.7)] and [AOR = 2.0, (95 % CI: 1.7–3.4)] compared to having normal BMI.
Participants with moderate physical activity were one and half times more likely to be hypertensive compared to those with high physical activity [AOR = 1.5, (95 % CI: 1.1–2.1)]. In the adjusted model, behaviours including insufficient fruit and vegetable intake, smoking and current alcohol consumption were not significantly associated with hypertension.
Discussion
Our study has demonstrated that approximately one in every three adults aged 35 years and above is hypertensive. The age adjusted prevalence of hypertension 29.4 % in this study population is higher than that of populations in similar conditions in Kenya, [13] Peru [26] and India [8] but considerably lower than the prevalence of 38 % measured in a Nigerian slum population [27]. These differences can be attributed to the differences in respondents ages included in the surveys.
The prevalence of hypertension is coupled by low awareness and complications of hypertension are bound to occur in those who are unaware of being hypertensive. The reason for low awareness is explained by screening levels for hypertension whereby almost half (42 %) of the population had never had their blood pressure measured. Other studies in Sub Sahara Africa [28] and China [29] show similar results as ours, documenting low rates of hypertension awareness, treatment and control especially among urban populations and in particular, disadvantaged urban communities. Screening and early diagnosis can help to avert hypertension and its progressive effects leading to CVD.
Similar to other studies [4, 30], our study confirms age as an important non modifiable risk factor for hypertension. The prevalence of hypertension increased with age and proved to be more marked among females compared to males. The prevalence of hypertension increased by almost 20 % in each 10 year age group, from 17.7 % among 34–44 years, 34.6 %, 45–55 years and 51.5 % among 55–64 years. As the population ages, it is likely that many pre hypertensive respondents (48.3 %) will progress to develop full hypertension, unless appropriate measures are undertaken.
Wealth index, marital status, BMI, and physical activity are lifestyle risk factors associated with hypertension. Our findings suggest widows living within the slum are vulnerable to hypertension as compared to their married counterparts. Consistent with results studies in Burkina Faso [11] widows had two times increased risk of being hypertensive compared to their married counterparts. This may point out the challenges females face in the event of loss of a husband, especially in a community with limited resources.
Having a body mass index ≥25 kg/m2 was independently associated with hypertension. Overweight and obese participants were approximately 2.0 times more likely to be hypertensive than their counterparts with normal BMI. In line with other studies [31–33] our findings show that rich females (proxied by wealth index) were more likely to be obese than their poorer counterparts as illustrated by both BMI and waist circumference. This finding could indicate that the obese females may have adopted sedentary lifestyles, and the consumption of energy dense foods that put them at increased risk of hypertension.
Creating a composite socioeconomic status (SES) (i.e. education, occupation, and durable household assets) index may not reflect the true relationship between SES and hypertension consistently as different components in the index could have varying influences on hypertension [34]. SES wealth index as measured by durable household assets was the only SES indicator independently associated with hypertension. These results are contrary to other studies in Uganda [35, 36] that used household assets as a measure of SES and found no association with hypertension. However, Fernald in a study of low income rural women in Mexico [34] observed a positive association of household assets with hypertension. Increased knowledge of health risks and greater motivation to control weight could explain the inverse association of wealth index and hypertension in high income countries. We hypothesize that among the urban poor population, increased wealth plays a less significant role in averting hypertension than the purchase of fatty, energy dense processed foods and sedentary lives among women of highest wealth quintile.
Our study revealed significantly higher odds for hypertension among individuals with moderate level of physical activity as compared to high level of physical activity. The high or moderate physical activity is directed towards work and travel and not recreational activities. Gaps in the literature still exist whether or not these types of physical activities confer the same benefit as regular exercise or recreational physical activities.
Limitations
The study is subject to recall bias. The behavioral risk factors in this study (i.e. fruit and vegetable consumption, tobacco use, alcohol use, and physical activity) were self-reported which might under or overestimate the actual levels of risk factors reported. In communities where certain behaviors are discouraged, there may be under reporting of these behaviors (eg. alcohol and tobacco consumption) especially among the females. As in many population based studies blood pressure measurements were based on average of two measurements at a single visit. The data was collected in a cross sectional study thus we cannot ascribe causality to any of the associated factors in the study. The beneficial approach of using the standardized WHO STEPs risk factor questionnaire allows for comparability on presence of risk factors between various communities, regions and countries.
Conclusion
Hypertension in the slum is a public health problem affecting at least one in three adults aged 35–64 years. Age, marital status, wealth index, physical inactivity and body mass index are important risk factors associated with hypertension. Prevention measures targeting the modifiable risk factors associated with hypertension are warranted to curb hypertension and its progressive effects.
References
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–60.
Lloyd-Sherlock P, Beard J, Minicuci N, Ebrahim S, Chatterji S. Hypertension among older adults in low- and middle-income countries: prevalence, awareness and control. Int J Epidemiol. 2014;43(1):116–28.
World Health Organization. Global status report on noncommunicable diseases 2010. Geneva: World Health Organization; 2011.
Addo J, Smeeth L, Leon DA. Hypertension in sub-saharan Africa: a systematic review. Hypertension. 2007;50(6):1012–8.
World Health Organization. A global brief on hypertension: silent killer, global public health crisis: World Health Day 2013. Geneva: World Health Organization; 2013.
World Bank: Kenya - Inside informality: poverty, jobs, housing and services in Nairobi’s slums Washington, DC; 2006.
Popkin BM. Dynamics of the nutrition transition and its implications for the developing world. Forum Nutr. 2003;56:262–4.
Anand K, Shah B, Yadav K, Singh R, Mathur P, Paul E, et al. Are the urban poor vulnerable to non-communicable diseases? A survey of risk factors for non-communicable diseases in urban slums of Faridabad. Natl Med J India. 2007;20(3):115–20.
Vaidya A, Aryal UR, Krettek A. Cardiovascular health knowledge, attitude and practice/behaviour in an urbanising community of Nepal: a population-based cross-sectional study from Jhaukhel-Duwakot Health Demographic Surveillance Site. BMJ Open. 2013;3(10):e002976.
Agyemang C. Rural and urban differences in blood pressure and hypertension in Ghana, West Africa. Public Health. 2006;120(6):525–33.
Doulougou B, Kouanda S, Rossier C, Soura A, Zunzunegui MV. Differences in hypertension between informal and formal areas of Ouagadougou, a sub-Saharan African city. BMC Public Health. 2014;14(893):1471–2458.
Park K. Park’s Textbook of Preventive and Social Medicine 19th edition. Jabalpur: M/s Banarsidas Bhanot Publishers; 2007.
Joshi MD, Ayah R, Njau EK, Wanjiru R, Kayima JK, Njeru EK, et al. Prevalence of hypertension and associated cardiovascular risk factors in an urban slum in Nairobi, Kenya: a population-based survey. BMC Public Health. 2014;14(1177):1471–2458.
van de Vijver SJ, Oti SO, Agyemang C, Gomez GB, Kyobutungi C. Prevalence, awareness, treatment and control of hypertension among slum dwellers in Nairobi, Kenya. J Hypertens. 2013;31(5):1018–24.
Kenya National Bureau of Statistics (KNBS). The 2009 housing and population census. Nairobi: Kenya National Bureau of Statistics; 2010.
United Nations Human Settlement Programme (UN-HABITAT). State of the worlds cities 2012/2013. Nairobi: UN-HABITAT; 2012.
Feikin DR, Olack B, Bigogo GM, Audi A, Cosmas L, Aura B, et al. The Burden of Common Infectious Disease Syndromes at the Clinic and Household Level from Population-Based Surveillance in Rural and Urban Kenya. PLoS ONE. 2011;6(1):e16085.
World Health Organization. STEPS Manual, STEPS Instrument. Geneva: WHO; 2011.
WHO STEPS Instrument (Core and Expanded). [http://www.who.int/chp/steps/instrument/STEPS_Instrument_V3.1.pdf].
Rutstein SO, Johnson K. The DHS Wealth Index. DHS Comparative Reports No. 6. Calverton: ORC Macro; 2004.
Parati G, Mendis S, Abegunde D, Asmar R, Mieke S, Murray A, et al. Recommendations for blood pressure measuring devices for office/clinic use in low resource settings. Blood Press Monit. 2005;10(1):3–10.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. Jama. 2003;289(19):2560–72.
World Health Organization. Physical status: the use and interpretation of anthropometry. In Book Physical Status: The Use and Interpretation of Anthropometry. In: Physical Status: The Use and Interpretation of Anthropometry. Geneva: World Health Organization; 1995.
World Health Organization. Waist circumference and waist-hip ratio: report of a WHO expert consultation, 8–11 December 2008. Geneva: World Health Organization; 2011.
World Health Organization. International Guide for Monitoring Alcohol Consumption and Related Harm. Geneva: World Health Organization; 2000.
Heitzinger K, Montano SM, Hawes SE, Alarcon JO, Zunt JR. A community-based cluster randomized survey of noncommunicable disease and risk factors in a peri-urban shantytown in Lima, Peru. BMC Int Health Hum Rights. 2014;14:14–9.
Daniel OJ, Adejumo OA, Adejumo EN, Owolabi RS, Braimoh RW. Prevalence of hypertension among urban slum dwellers in Lagos, Nigeria. J Urban Health. 2013;90(6):1016–25.
Hendriks ME, Wit FW, Roos MT, Brewster LM, Akande TM, de Beer IH, et al. Hypertension in sub-Saharan Africa: cross-sectional surveys in four rural and urban communities. PLoS One. 2012;7(3):e32638.
Meng XJ, Dong GH, Wang D, Liu MM, Lin Q, Tian S, et al. Prevalence, awareness, treatment, control, and risk factors associated with hypertension in urban adults from 33 communities of China: the CHPSNE study. J Hypertens. 2011;29(7):1303–10.
Musinguzi G, Nuwaha F. Prevalence, awareness and control of hypertension in Uganda. PLoS One. 2013;8(4):e62236.
Christensen DL, Eis J, Hansen AW, Larsson MW, Mwaniki DL, Kilonzo B, et al. Obesity and regional fat distribution in Kenyan populations: impact of ethnicity and urbanization. Ann Hum Biol. 2008;35(2):232–49.
Ziraba AK, Fotso JC, Ochako R. Overweight and obesity in urban Africa: A problem of the rich or the poor? BMC Public Health. 2009;9(465):1471–2458.
Mbochi RW, Kuria E, Kimiywe J, Ochola S, Steyn NP. Predictors of overweight and obesity in adult women in Nairobi Province, Kenya. BMC Public Health. 2012;12(823):1471–2458.
Fernald LC, Adler NE. Blood pressure and socioeconomic status in low-income women in Mexico: a reverse gradient? J Epidemiol Community Health. 2008;62(5):e8.
Wamala JF, Karyabakabo Z, Ndungutse D, Guwatudde D. Prevalence factors associated with hypertension in Rukungiri district, Uganda--a community-based study. Afr Health Sci. 2009;9(3):153–60.
Mayega RW, Makumbi F, Rutebemberwa E, Peterson S, Ostenson CG, Tomson G, et al. Modifiable socio-behavioural factors associated with overweight and hypertension among persons aged 35 to 60 years in eastern Uganda. PLoS One. 2012;7(10):e47632.
Acknowledgements
We are grateful to the study participants in Kibera for their willingness to participate in the survey. The KEMRI/CDC International Emerging Infections Program (IEIP) is duly acknowledged for the platform on which this work was accomplished. This study was funded by a grant from Training Health Researchers into Vocational Excellence (THRiVE) in East Africa, Grant number 087540, funded by Wellcome Trust.
Declaration
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
BO coordinated the study, analysed the data and wrote the original manuscript. LS, RB, FW, JM and NK participated in development of the study, and helped to draft the manuscript. All co-authors contributed to subsequent revisions and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Olack, B., Wabwire-Mangen, F., Smeeth, L. et al. Risk factors of hypertension among adults aged 35–64 years living in an urban slum Nairobi, Kenya. BMC Public Health 15, 1251 (2015). https://doi.org/10.1186/s12889-015-2610-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-015-2610-8