
Abstract
Background
Manganese (Mn) participates in lipid metabolism. However, the associations between Mn exposure and dyslipidaemia is unclear.
Methods
This was a cross-sectional study. Data were collected from the 2017 the Mn-exposed workers healthy cohort (MEWHC). Finally, 803 occupationally Mn-exposed workers included in the study. The workers were divided into two groups. The grouping of this study was based on Mn-Time Weighted Averages (Mn-TWA). The high-exposure group included participants with Mn-TWA greater than 0.15 mg/m3. The low-exposure group included participants with Mn-TWA less than or equal to 0.15 mg/m3. Mn-TWA levels and dyslipidaemia were assessed.
Results
After adjustment for seniority, sex, cigarette consumption, alcohol consumption, high-fat diet frequency, medicine intake in the past two weeks, egg intake frequency, drinking tea, WHR, and hypertension, Mn-TWA levels was negatively correlated with high triglycerides (TG) risk in workers overall (OR = 0.51; 95% CI: 0.36, 0.73; p < 0.01). The results of males and females were consistent (OR = 0.53; 95% CI: 0.34, 0.81; p < 0.01) and (OR = 0.47; 95% CI: 0.24, 0.94; p < 0.01), respectively. By performing interactions analyses of workers overall, we observed no significant interactions among confounders. Mn-TWA levels and pack-years on high TG risk (relative excess risk for the interactions (RERI = 2.29, 95% CI: − 2.07, 6.66), (RERI) = 2.98, 95% CI: − 2.30, 8.26). Similarly, smoking status, drinking status, high-fat diet frequency, and Waist-to-Hip Ratio (WHR) showed non-significant interactions with Mn-TWA levels on high TG risk.
Conclusions
This research indicates that high Mn exposure was negatively related to high TG risk in workers.
Similar content being viewed by others

Background
Mn is vital for human health and is reflected in physiological metabolism [1,2,3]. Equally, occupational overexposure to Mn exerts neurotoxic effects [4,5,6,7]. Mn participates in lipid metabolism. However, its mechanical effects are currently unclear. Mn reduces the total antioxidant status of rats and increases brain lipid peroxidation [8, 9]. Moreover, Mn enhances cholesterol biosynthesis in the rats’ liver microsome. And stimulates farnesyl pyrophosphate synthase activity. An important synthesis pathway for many lipids in the mevalonate pathway, with mevalonate being the first branch in this pathway [10, 11]. Moreover, Mn enhances cholesterol biosynthesis in the rats’ liver microsome. And stimulates farnesyl pyrophosphate synthase activity. An important synthesis pathway for many lipids in the mevalonate pathway, with mevalonate being the first branch in this pathway [12,13,14,15].
There are few studies on Mn and lipids. A recent study showed that exposure of low-level Mn reduced serum triglyceride (TG) levels in rats [16]. Besides, epidemiological data were concentrated only on the intake of Mn. A diet study from china indicated that dietary Mn negatively correlated with hypertriglyceridaemia in males. And females’ high-density lipoprotein cholesterol (HDL-C) levels increases with Mn intake [17]. Similarly, the HDL-C levels of obese males decreased with the increased in serum Mn levels [18]. Other Chinese diet study observed that Mn intake was inversely associated with serum TG and total cholesterol (T-CHO) levels [19].
In recent decades, welding and smelting associated leaded to Mn overexposure [20]. Additionally, with the use of methyl cyclopentadienyl Mn tricarbonyl (MMT) was added to the gasoline component, resulting in increased Mn exposure in the general population [21]. Public health issues related to Mn have attracted more attention.
The MEWHC was a vertically innovative and multi-course scientific study, which began in the iron and Mn concentrator from July to October 2011 [22]. The critical overall goal of MEWHC was to explore early or long-term physical and mental health hazards, potential exposure to biomarkers, and conditions related to Mn exposure. Therefore, we carried out this study to investigate the correlations between Mn external exposure and hyperlipidemia. And we tried to explore the relationship between Mn exposure and serum lipids among Mn exposed workers.
Methods
Data collection
It was a cross-sectional study based on the follow-up of the 2017 MEWHC study. Detailed inclusion criteria and exclusion criteria for the cohort have been described in detail before [22, 23]. And the information collected in this cohort follow-up has been described in detail [24]. It mainly covers three types of data, including the personal information of the participants in the questionnaire, the exposure data of Mn concentrations in the workplace, collection, and storage of biological specimens and biochemical detection data. Standardized and structured questionnaires were used to collect necessary worker information. And participants were surveyed face to face by professionally trained graduate students. The information collected by the participants includes cigarette consumption, alcohol consumption, high-fat diet frequency, medicine intake in the past two weeks, egg intake frequency, drinking tea, and medical history. Standardized methods were used to measure participants’ blood pressure. The definition of hypertension adopted the latest Chinese standards [25]. Waist-to-hip ratio (WHR) was deemed high if ≥0.9 for males, and ≥ 0.85 for females (WHO, 1999). Other indicators such as cigarette and alcohol consumption were defined in detail in our previous studies [26]. Smoking 20 cigarettes a day in a year was defined as a pack-year [27]. We further divided workers’ cigarette consumption into three categories, based on the median of pack-years: non-smokers, < 18 pack-years, and ≥ 18 pack-years. According to the exclusion criteria, we excluded workers with cancer, coronary heart disease, stroke disease, or diabetes. And we excluded workers whose serum lipids were not tested due to insufficient biological samples. In the end, 22 workers were excluded from the study. A total of 803 workers participated in this study.
Measurement of Mn levels in respirable dust
Recent researches by our team have introduced in detail the sampling and monitoring methods of Mn concentrations [24, 26]. Therefore, we briefly described the monitoring of air Mn. We have selected 20 types of jobs covering different levels of Mn exposure in the ferromanganese alloy smelter. We randomly selected three workers in each position for personal sampling. We used individual samplers to measure workers’ respiratory dust samples for three consecutive days. In the end, we collected 134 air samples. We strictly abided by China’s sampling and testing standards. The standards we adopted are as follows: “Determination of airborne dust in the workplace part 2: concentrations of respirable dust” (GBZ/T 192.2–2007); “Specifications of air sampling for hazardous substances monitoring in the workplace” (GBZ159–2004); “Ambient air and stationary source emission-determination of metals in ambient particulate matter-Inductively Coupled Plasma Mass Spectrometry (ICP-MS)” (HJ657–2013). After the digestion of the filter sample, it was measured by ICP-MS (Perkin Elmer, NexION 2000, USA). The limit of detection (LOD) of Mn was 0.076 μg/L. Based on the standard of China, PC-TWA of Mn was 0.15 mg/m3 (as MnO2). Five hundred twenty workers with Mn-TWA > 0.15 mg/m3 were defined as a high-exposure group. Two hundred eighty-three workers with Mn-TWA ≤ 0.15 mg/m3 were defined as the low-exposure group.
Smelter workers accounted for the most substantial proportion of the high exposure group. High exposure group also included ferromanganese alloy crushing operation workers, pouring crane workers, and crane workers with ferromanganese alloy raw materials. The low-exposure group mainly included circulating cooling water system operators, chemical analysts, office workers, security guards and workers in other auxiliary positions.
Measurement of serum lipids
The determination of serum lipids has been described before [24]. The definition of serum lipids abnormality adopted the 2016 Chinese guidelines on prevention and treatment of dyslipidaemia in adults [28]. High LDL-C was defined as Low-density lipoprotein cholesterol ≥4.14 mmol/L. High TG was defined as triglyceride ≥2.26 mmol/L, high T-CHO was defined as total cholesterol ≥6.22 mmol/L, and low HDL-C was defined as high-density lipoprotein cholesterol < 1.04 mmol/L. Dyslipidaemia can further develop into cardiovascular disease [29]. Dyslipidaemia guidelines suggested an LDL-C target should be set according to individual ASCVD risk. The Chinese guidelines suggested that LDL-C target should be set based on an individual’s ASCVD risk levels. The personal ASCVD risk level was evaluated to age, sex, Body Mass Index (BMI), hypertension history, and cigarette consumption [28].
Statistical analysis
The Mann-Whitney U test was used to compare serum lipids levels in different groups. We used logistic regression models to estimate Mn exposure levels and the risk of varying serum lipid abnormalities. Also, there was a high correlation between age and years of work. Only the working years were adjusted in the models. Corrected confounders included sex, cigarette consumption, alcohol consumption, high-fat diet frequency, medicine intake in the past two weeks, egg intake frequency, drinking tea, WHR, and hypertension.
We also conducted a hierarchical analysis. Besides, biological interactions between confounding factors were also evaluated. Rothman et al. suggested that studies should pay attention to epidemiological interactions or additive interactions. The method assessed whether the combined effect of exposure to two factors was higher than the sum of their independent effects.
The authors proposed the use of relative excess risk for interactions (RERI) in assessing additive interactions. Rothman et al. explained detailed RERI explanations and calculation methods in the article [30,31,32]. The interaction between Mn-TWA levels and confounders were evaluated. Confounders included cigarette consumption (smoking status and pack-years), alcohol consumption, high-fat diet frequency, medicine intake in the past two weeks, and WHR. The analysis software we use is R (version 3.4) and SPSS (version 19.0) A two-sided, p < 0.05 was considered statistically significant.
Results
In our participants, The median (IQR) ages were 41.75(36.58,46.92) and 45.42 (41.27,49.08) years for low, and high exposure groups, respectively. The median seniority was 18.92 years. And no significant difference was observed in seniority between two groups (p = 0.07). The proportion of males in the two groups was 57.6 and 72.5%, respectively. The ratio of males who consumed cigarettes was higher in high-exposure group, at 26.2% (p < 0.01). And 10.6% of consumed cigarettes in low exposure group. Similarly, the proportion of ≥18 pack-years was higher in the high exposure group, and the rates were 29.4, 14.5%, respectively (p < 0.01). Alcohol consumption at the high exposure was higher, at 32.7% (p < 0.01). Low-exposure was 23.0%. WHR, hypertension, drinking tea, and medicine intake in the past two weeks were not different in two groups (p>0.05) (Table 1). High TG (≥2.3 mmol / L), high T-CHO (≥6.1 mmol / L), high LDL-C (≥4.10 mmol / L) and low HDL-C (< 1.04 mmol / L) were 25.5, 15.7, 6.8 and 3.1%. According to the individual’s ASCVD risk, the overall goal of LDL-lowering was set, and the incidence rate is 27.4%. The incidence of high TG in the low-exposure group was higher than that in the high-exposure group, which were 30.7 and 22.7%, respectively (p < 0.01)) (Table 2).
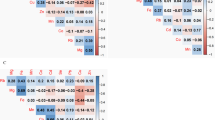
Adjusted for potential confounding factors as sex, seniority, WHR, high blood pressure, drug intake in the past half month, high-fat diet consumption, egg intake frequency, drinking tea, smoking and drinking status, high TG risk significantly decreased in high exposure group (OR = 0.66; 95% CI: 0.48, 0.92; p < 0.01), and consistent negative correlation was found in males (OR = 0.53; 95% CI: 0.34, 0.81; p < 0.01) and females (OR = 0.47; 95% CI: 0.24, 0.94; p < 0.01). Similarly, the results negative correlation between high Mn-TWA levels and high TG risk were found among subgroups current smokers (OR = 0.36; 95% CI: 0.20, 0.63), and < 18 pack-years group (OR = 0.37; 95% CI: 0.18, 0.77), ≥18 pack-years group (OR = 0.38; 95% CI: 0.18, 0.84), seniority < 18.92 years group (OR = 0.40; 95% CI: 0.23, 0.67), non-hypertension group (OR = 0.42; 95% CI: 0.27, 0.65), high-fat diet frequency < 3 times per week group (OR = 0.46; 95% CI: 0.31, 0.69), and normal WHR group (OR = 0.40; 95% CI: 0.25, 0.66) (Table 3, Fig. 1).

Adjusted ORs for Mn-TWA levels associated with high TG risk in subgroups. Logistic regression models was used for analysis, with high TG as the dependent variable and Mn-TWA levels (categorical variable) as the independent variable. We set subgroups according to gender, seniority, smoking status, pack years, drinking status, hypertension, egg intake frequency, drinking tea, medicine intake in the past two weeks, and WHR. Seniority was divided into two groups by median, and other variables were adjusted. When participants were males, or current smokers, or smoking ≥18 pack-years, seniority < 18.92 years, or non-hypertension, or high-fat diet frequency less than 3 times per week, or WHR, Mn-TWA levels showed negative associations with high TG risk
In the analysis of interaction, we did not observe that there was a significant cumulative scale interaction between Mn-TWA levels and cigarette consumption status or the pack-years of high TG risk (relative excess risk for the interactions for cigarette consumption (RERI = 2.29, 95% CI: − 2.07, 6.66), (RERI) = − 2.98, 95% CI: − 1.88, 7.85) for pack-years, respectively. Research showed that the mutual harm of high-quality Mn-TWA exposure and current smoking or previous smoking did not exceed the total number of their hazards, and consistent results were found in ≥18 pack-years or < 18 pack-years. In the same way, no obvious interactions between Mn-TWA levels and alcohol consumption, the frequency of high-fat diet, and the risk of high TG (Table 4).
Discussion
The associations between Mn exposure and dyslipidaemia in occupational workers were first discussed. The results showed that workers’ exposure to higher Mn-TWA levels was associated with lower TG risk. And there was no interaction with confounders. Most of the researches concentrated on the intake of Mn in the diet. One clinical study showed that when 14 adults filled the gluconic acid in the diet, Mn reduced body fat by increasing the body fat metabolism of excreta [33]. Another clinical study for 7 young men showed that adequate intake Mn could reduce blood carbohydrate levels [34]. One study on the diet of 2111 Chinese participants found that male’s Mn intake was inversely proportional to hypertriglyceriduria. And that females’ HDL-C concentrations increased with Mn intake [17]. One Chinese study on the absorption of polymetallic diets for 258 healthy males and females found that the consumption of Mn was negatively proportional to serum TG and T-CHO [19]. In this study, Mn exposure of workers was inversely proportional to serum TG. However, we did not observe correlations between Mn exposure and serum T-CHO, HDL-C, LDL-C, and LDL-lowering targets. Previous researches have already confirmed the critical efficacy of Mn in TG regulation. However, our participants were occupationally touched to Mn. Therefore, it was not appropriate to compare dietary Mn intake with the concentrations of occupational Mn exposure levels of our workers. It was essential to study the mechanism of Mn′s involvement in lipids metabolism and to assess the toxic doses of Mn to dyslipidaemia. It was essential to consider the mechanism of Mn′s involvement in lipids metabolism and to determine the toxic doses of Mn to dyslipidaemia. Besides, mammalian models must be established to show that inhalation Mn exposure concentrations were closer to the occupationally touched to Mn.
Mn can enter peripheral blood through intestinal absorption and olfactory channels. The steady-state Mn ions in the peripheral blood were further absorbed and metabolized by the liver. In contrast, excess Mn (in the form of Mn2+ is primarily excreted from the liver into the intestine, along with bile [35,36,37,38]. Previously published studies have shown that Mn metabolism was related to lipid peroxidation [39,40,41]. Also, studies have shown that Mn has participated in lipid metabolism through lipid synthesis [12,13,14,15]. Thus the influence of Mn in lipid mechanisms is equivocal.
In terms of lipid synthesis, two pathways exist for TG synthesis in the liver. One of the mechanisms was the entry of exogenous fatty acids into hepatocytes, which are then esterified to synthesize TG. TG can also pass on the de novo body fat production (DNL) pathway. Eventually, TG is placed in a storage tank or secretion tank. TG can also pass on the de novo body fat production (DNL) pathway. Eventually, TG is placed in a storage tank or secretion tank [42,43,44,45]. Acetyl-CoA carboxylase (ACC) was an important metal catalyst for the production of the Novo DNL acids (necessary phosphatases). Phosphatase was a necessary auxiliary enzyme to active ACC. And phosphatase relied on Mn2 + activation and dephosphorylation to participate in ACC activity [43, 46]. Therefore, Mn 2+ plays a crucial role in the synthesis of TG in the liver. The allosteric inhibition of liver ACC significantly reduces hepatic TG concentrations and increased plasma TG levels [47, 48]. It is speculated that the inhibition of ACC is the mechanism of manganese-induced hypertriglyceridemia [49]. We hypothesized that higher levels of Mn2+ were stored in the livers of workers exposed to higher Mn levels. And ACC was more likely to be activated in the liver. Eventually, TG levels in the liver may be higher, while TG levels in serum are reduce.
Gender is a common factor affecting Mn absorption. Previous studies have found that females have higher Mn absorption capabilities. And Males were found to have lower levels of Mn in their blood than females [50,51,52,53]. However, males are reported to be more prone to TG, lipid abnormalities, and metabolic diseases [54,55,56]. TG metabolism is regulated by endogenous estrogen and androgen [57]. Currently, several studies have observed that in hepatocyte-specific ERa-knock-out mice, estrogen cannot make liver fatty degeneration. This result suggests that estrogen directly acts on the liver via the Estrogen Receptor alpha (ERa), thereby decreasing TG [58,59,60]. In additionally, to cope with obesity, both males and females increase the flow of fatty acids into the peripheral blood. Visceral or visceral chamber fat contributes more to liver fatty acid delivery, than subcutaneous fat [46]. The fatty acids that are absorbed into the liver are assembled into TG. And then wrapped up in TG rich very low-density lipoprotein (VLDL) particles and expelled from the liver [61, 62]. Other studies have observed that females can produce more TGDL-rich VLDL particles, and these particles help reduce overall blood TG levels.
When the body ingests food, TG circulates in the form of chylomicrons containing apolipoprotein 48. Study through short-term and long-term high-fat feeding found that females can better clear diet-related TG [63,64,65]. Consistent with previous research results, the proportion of females with high TG was indeed lower in our study subjects, and that high TG was observed in males. But the high TG risk is not different between males and females workers after exposure to Mn. We speculate that we may have corrected WHR factors in the statistical analysis, to avoid confounding effects caused by sex hormones. Therefore, our research can reflect that manganese is involved in TG metabolism.
In our study, smoking and drinking rates were higher than the general population, our smoking and drinking rates were 40.7 and 28.4%, respectively, were wherein a survey of 163,641 Chinese adults between 2013 and 2014, the rates were 24.4 and 8.7%, respectively. Guidelines on the treatment of blood cholesterol to reduce atherosclerosis by The American Heart Associations (AHA, 2013) have indicated that smoking was an independent risk behaviour for dyslipidaemia. That small amounts of alcohol could raise TG levels further [29]. Previous studies have shown that WHR and high-fat diet are significantly and positively correlated with high TG levels [66,67,68,69,70]. However, from interactions analyses, we observed no interactions between Mn-TWA levels and smoking effects (both smoking status and pack-years), drinking status, high-fat diet, and the WHR on high TG risk. Although not statistically significant, regardless of whether the population’s high-fat diet frequency was high or low, we can observe a negative correlation between Mn-TWA levels exposure and high TG risk. This result suggests that the intensity of Mn exposure to decrease high TG risk was greater than that of a high-fat diet. Further investigations are required to confirm these findings.
This is the first study to examine the relationship between Mn exposure and dyslipidaemia in occupational workers. We comprehensively carried out a full range of accurate measurements and analysis of the risk sources and potential risks related to lipid metabolism. And we will further conduct follow-up the cohort to evaluate the risk of hyperlipidemia exposed to Mn. There were some limitations to our study. Firstly, non-Mn exposed individuals were not included as controls. Therefore, the confounding effect of regional diet mix, labor efficiency, genetic inheritance, and environmental hazards cannot be ruled out. Our data does not accurately reflect Mn cumulative exposure indices (Mn-CEI). So there is no way to comprehensively discuss the relationships between long-term Mn cumulative exposure and dyslipidaemia.
Conclusions
This study observed an inverse correlation between workers’ high TG and Mn exposure levels. We expect larger prospective studies to confirm the association between Mn exposure and dyslipidaemia.
Availability of data and materials
The data and material are available upon reasonable request from the corresponding author. E-mail: yxbo21021@163.com.
Abbreviations
- MMT:
-
Methyl cyclopentadienyl manganese tricarbonyl
- TWA:
-
Time-weighted Average
- TG:
-
Triglycerides
- T-CHO:
-
Total Cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- WHR:
-
Waist-to-Hip Ratio
- RERI:
-
Relative excess risk for the interactions
- ICP-MS:
-
Inductively Coupled Plasma Mass Spectrometry
- MEWHC:
-
Manganese-exposed Workers Healthy Cohort
- QC:
-
Quality control
- PC-TWA:
-
Permissible concentrations-time weighted average
- LOD:
-
Limit of detection
- DNL:
-
De novo lipogenesis
- VLDL:
-
Very Low density lipoprotein
- Mn-CEI:
-
Manganese-cumulative exposure index
References
Takeda A. Manganese action in brain function. Brain Res Brain Res Rev. 2003;41(1):79–87.
Aschner JL, Aschner M. Nutritional aspects of manganese homeostasis. Mol Asp Med. 2005;26(4–5):353–62.
Mertz W. The essential trace elements. Science. 1981;213(4514):1332–8.
Crossgrove J, Zheng W. Manganese toxicity upon overexposure. NMR Biomed. 2004;17(8):544–53.
Guilarte TR. Manganese and Parkinson's disease: a critical review and new findings. Environ Health Perspect. 2010;118(8):1071–80.
Santamaria AB, Sulsky SI. Risk assessment of an essential element: manganese. J Toxicol Environ Health A. 2010;73(2):128–55.
Aschner M, Guilarte TR, Schneider JS, Zheng W. Manganese: recent advances in understanding its transport and neurotoxicity. Toxicol Appl Pharmacol. 2007;221(2):131–47.
Ganeshan M, Sainath PB, Padmavathi IJ, Venu L, Kishore YD, Kumar KA, Harishanker N, Rao JS, Raghunath M. Maternal manganese restriction increases susceptibility to high-fat diet-induced dyslipidemia and altered adipose function in WNIN male rat offspring. Exp Diabetes Res. 2011;2011:486316.
Malhotra KM, Murthy RC, Srivastava RS, Chandra SV. Concurrent exposure of lead and manganese to iron-deficient rats: effect on lipid peroxidation and contents of some metals in the brain. J Appl Toxicol. 1984;4(1):22–5.
Bell LT, Hurley LS. Ultrastructural effects of manganese deficiency in liver, heart, kidney, and pancreas of mice. Lab Invest. 1973;29(6):732–6.
Robberecht HJ, Hendrix P, Van Cauwenbergh R, Deelstra HA. Daily dietary manganese intake in Belgium, using duplicate portion sampling. Zeitschrift Lebensmittel-Untersuchung Forschung. 1994;199(6):446–8.
McTaggart SJ. Isoprenylated proteins. Cell Mol Life Sci. 2006;63(3):255–67.
Curran GL, Azarnoff DL: Effect of certain transition elements on cholesterol biosynthesis. Fed Proc 1961, 20(3) Pt 2:109–111.
Curran GL. Effect of certain transition group elements on hepatic synthesis of cholesterol in the rat. J Biol Chem. 1954;210(2):765–70.
Park J, Zielinski M, Magder A, Tsantrizos YS, Berghuis AM. Human farnesyl pyrophosphate synthase is allosterically inhibited by its own product. Nat Commun. 2017;8:14132.
Oladipo OO, Ayo JO, Ambali SF, Mohammed B, Aluwong T. Dyslipdemia induced by chronic low dose co-exposure to lead, cadmium and manganese in rats: the role of oxidative stress. Environ Toxicol Pharmacol. 2017;53:199–205.
Zhou B, Su X, Su D, Zeng F, Wang MH, Huang L, Huang E, Zhu Y, Zhao D, He D, et al. Dietary intake of manganese and the risk of the metabolic syndrome in a Chinese population. Br J Nutr. 2016;116(5):853–63.
Rotter I, Kosik-Bogacka D, Dolegowska B, Safranow K, Lubkowska A, Laszczynska M. Relationship between the concentrations of heavy metals and bioelements in aging men with metabolic syndrome. Int J Environ Res Public Health. 2015;12(4):3944–61.
Kim M-H, Choi M-K. Seven dietary minerals (Ca, P, mg, Fe, Zn, cu, and Mn) and their relationship with blood pressure and blood lipids in healthy adults with self-selected diet. Biol Trace Elem Res. 2013;153(1–3):69–75.
Gerber GB, Leonard A, Hantson P. Carcinogenicity, mutagenicity and teratogenicity of manganese compounds. Crit Rev Oncol Hematol. 2002;42(1):25–34.
Joselow MM, Tobias E, Koehler R, Coleman S, Bogden J, Gause D. Manganese pollution in the city environment and its relationship to traffic density. Am J Public Health. 1978;68(6):557–60.
Lv Y, Zou Y, Liu J, Chen K, Huang D, Shen Y, Zhong Y, Liu Z, Jiang B, Li Q, et al. Rationale, design and baseline results of the Guangxi manganese-exposed workers healthy cohort (GXMEWHC) study. BMJ Open. 2014;4(7):e005070.
Zhou Y, Ge X, Shen Y, Qin L, Zhong Y, Jiang C, Su C, Huang J, Lin S, Li D, et al. Follow-up of the manganese-exposed workers healthy cohort (MEWHC) and biobank management from 2011 to 2017 in China. BMC Public Health. 2018;18(1):944.
Huang S, Liu Z, Ge X, Luo X, Zhou Y, Li D, Li L, Chen X, Huang L, Cheng H, et al. Occupational exposure to manganese and risk of creatine kinase and creatine kinase-MB elevation among ferromanganese refinery workers. Am J Ind Med. 2020;63(5):394–401.
Hypertension alliance (China) ea. Chinese guidelines for the prevention and treatment of hypertension (2018 revision). Chin J Cardiovasc Med. 2019;24(1):25.
Chen X, Liu Z, Ge X, Luo X, Huang S, Zhou Y, Li D, Cheng H, Li L, Huang L, et al. Associations between manganese exposure and multiple immunological parameters in manganese-exposed workers healthy cohort. J Trace Elements Med Biol. 2020;59:126454.
Bernaards CM, Twisk JW, Snel J, Van Mechelen W, Kemper HC. Is calculating pack-years retrospectively a valid method to estimate life-time tobacco smoking? A comparison between prospectively calculated pack-years and retrospectively calculated pack-years. Addiction. 2001;96(11):1653–61.
Junren zhu RG, Zhao S, Lu G, Zhao D, Li J. 2016 Chinese guidelines for the management of dyslipidemia in adults. J Geriatr Cardiol. 2018;15(1):1–29.
Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;129(25 Suppl 2):S1–45.
Chen Y, Graziano JH, Parvez F, Liu M, Slavkovich V, Kalra T, Argos M, Islam T, Ahmed A, Rakibuz-Zaman M, et al. Arsenic exposure from drinking water and mortality from cardiovascular disease in Bangladesh: prospective cohort study. BMJ. 2011;342:d2431.
Knol MJ, van der Tweel I, Grobbee DE, Numans ME, Geerlings MI. Estimating interaction on an additive scale between continuous determinants in a logistic regression model. Int J Epidemiol. 2007;36(5):1111–8.
Li R, Chambless L. Test for additive interaction in proportional hazards models. Ann Epidemiol. 2007;17(3):227–36.
Potter SM, Kies CV, Rojhani A. Protein and fat utilization by humans as affected by calcium phosphate, calcium carbonate, and manganese gluconate supplements. Nutrition. 1990;6(4):309–12.
Friedman BJ, Freeland-Graves JH, Bales CW, Behmardi F, Shorey-Kutschke RL, Willis RA, Crosby JB, Trickett PC, Houston SD. Manganese balance and clinical observations in young men fed a manganese-deficient diet. J Nutr. 1987;117(1):133–43.
Kim J, Buckett PD, Wessling-Resnick M. Absorption of manganese and iron in a mouse model of hemochromatosis. PLoS One. 2013;8(5):e64944.
Brenneman KA, Wong BA, Buccellato MA, Costa ER, Gross EA, Dorman DC. Direct olfactory transport of inhaled manganese ((54) MnCl (2)) to the rat brain: toxicokinetic investigations in a unilateral nasal occlusion model. Toxicol Appl Pharmacol. 2000;169(3):238–48.
Hauser RA, Zesiewicz TA, Rosemurgy AS, Martinez C, Olanow CW. Manganese intoxication and chronic liver failure. Ann Neurol. 1994;36(6):871–5.
Zeron HM, Rodriguez MR, Montes S, Castaneda CR. Blood manganese levels in patients with hepatic encephalopathy. J Trace Elements Med Biol. 2011;25(4):225–9.
Ismail HTH. Hematobiochemical disturbances and oxidative stress after subacute manganese chloride exposure and potential protective effects of Ebselen in rats. Biol Trace Elem Res. 2019;187(2):452–63.
Porter NA, Caldwell SE, Mills KA. Mechanisms of free radical oxidation of unsaturated lipids. Lipids. 1995;30(4):277–90.
Gutteridge JM, Halliwell B. The measurement and mechanism of lipid peroxidation in biological systems. Trends Biochem Sci. 1990;15(4):129–35.
Olofsson SO, Boren J. Apolipoprotein B: a clinically important apolipoprotein which assembles atherogenic lipoproteins and promotes the development of atherosclerosis. J Intern Med. 2005;258(5):395–410.
Sahini N, Borlak J. Recent insights into the molecular pathophysiology of lipid droplet formation in hepatocytes. Prog Lipid Res. 2014;54:86–112.
Trickett JI, Patel DD, Knight BL, Saggerson ED, Gibbons GF, Pease RJ. Characterization of the rodent genes for arylacetamide deacetylase, a putative microsomal lipase, and evidence for transcriptional regulation. J Biol Chem. 2001;276(43):39522–32.
Zammit Victor A. Hepatic triacylglycerol synthesis and secretion: DGAT2 as the link between glycaemia and triglyceridaemia. Biochem J. 2013;451(1):1–12.
Thampy KG, Wakil SJ. Activation of acetyl-CoA carboxylase. Purification and properties of a Mn2+−dependent phosphatase. J Biol Chem. 1985;260(10):6318–23.
Abu-Elheiga L, Matzuk MM, Abo-Hashema KA, Wakil SJ. Continuous fatty acid oxidation and reduced fat storage in mice lacking acetyl-CoA carboxylase 2. Science. 2001;291(5513):2613–6.
Kim CW, Addy C, Kusunoki J, Anderson NN, Deja S, Fu X, Burgess SC, Li C, Ruddy M, Chakravarthy M, et al. Acetyl CoA carboxylase inhibition reduces hepatic Steatosis but elevates plasma triglycerides in mice and humans: a bedside to bench investigation. Cell Metab. 2017;26(3):576.
Abu-Elheiga L, Oh W, Kordari P, Wakil SJ. Acetyl-CoA carboxylase 2 mutant mice are protected against obesity and diabetes induced by high-fat/high-carbohydrate diets. Proc Natl Acad Sci U S A. 2003;100(18):10207–12.
Bocca B, Madeddu R, Asara Y, Tolu P, Marchal JA, Forte G. Assessment of reference ranges for blood cu, Mn, se and Zn in a selected Italian population. J Trace Elements Med Biology. 2011;25(1):19–26.
Clark NA, Teschke K, Rideout K, Copes R. Trace element levels in adults from the west coast of Canada and associations with age, gender, diet, activities, and levels of other trace elements. Chemosphere. 2007;70(1):155–64.
Lee JW, Lee CK, Moon CS, Choi IJ, Lee KJ, Yi SM, Jang BK, Yoon BJ, Kim DS, Peak D, et al. Korea National Survey for environmental pollutants in the human body 2008: heavy metals in the blood or urine of the Korean population. Int J Hyg Environ Health. 2012;215(4):449–57.
Zhang LL, Lu L, Pan YJ, Ding CG, Xu DY, Huang CF, Pan XF, Zheng W. Baseline blood levels of manganese, lead, cadmium, copper, and zinc in residents of Beijing suburb. Environ Res. 2015;140:10–7.
Mihailidou AS, Ashton AW. Cardiac effects of aldosterone: does gender matter? Steroids. 2014;91:32–7.
Zhang X, Meng Z, Li X, Liu M, Ren X, Zhu M, He Q, Zhang Q, Song K, Jia Q, et al. The association between total bilirubin and serum triglyceride in both sexes in Chinese. Lipids Health Dis. 2018;17(1):217.
Onat A, Karadeniz Y, Tusun E, Yuksel H, Kaya A. Advances in understanding gender difference in cardiometabolic disease risk. Expert Rev Cardiovasc Ther. 2016;14(4):513–23.
Palmisano BT, Zhu L, Eckel RH, Stafford JM. Sex differences in lipid and lipoprotein metabolism. Mol Metab. 2018;15:45–55.
Villa A, Della Torre S, Stell A, Cook J, Brown M, Maggi A. Tetradian oscillation of estrogen receptor alpha is necessary to prevent liver lipid deposition. Proc Natl Acad Sci U S A. 2012;109(29):11806–11.
Palmisano BT, Le TD, Zhu L, Lee YK, Stafford JM. Cholesteryl ester transfer protein alters liver and plasma triglyceride metabolism through two liver networks in female mice. J Lipid Res. 2016;57(8):1541–51.
Zhu L, Brown WC, Cai Q, Krust A, Chambon P, McGuinness OP, Stafford JM. Estrogen treatment after ovariectomy protects against fatty liver and may improve pathway-selective insulin resistance. Diabetes. 2013;62(2):424–34.
Reaven GM, Bernstein RM. Effect of obesity on the relationship between very low density lipoprotein production rate and plasma triglyceride concentration in normal and hypertriglyceridemic subjects. Metab Clin Exp. 1978;27(9):1047–54.
Mittendorfer B, Patterson BW, Klein S. Effect of sex and obesity on basal VLDL-triacylglycerol kinetics. Am J Clin Nutr. 2003;77(3):573–9.
Matthan NR, Jalbert SM, Barrett PH, Dolnikowski GG, Schaefer EJ, Lichtenstein AH. Gender-specific differences in the kinetics of nonfasting TRL, IDL, and LDL apolipoprotein B-100 in men and premenopausal women. Arterioscler Thromb Vasc Biol. 2008;28(10):1838–43.
Votruba SB, Jensen MD. Sex-specific differences in leg fat uptake are revealed with a high-fat meal. Am J Phys Endocrinol Metab. 2006;291(5):E1115–23.
Santosa S, Hensrud DD, Votruba SB, Jensen MD. The influence of sex and obesity phenotype on meal fatty acid metabolism before and after weight loss. Am J Clin Nutr. 2008;88(4):1134–41.
Bhowmik B, Munir SB, Diep LM, Siddiquee T, Habib SH, Samad MA, Azad Khan AK, Hussain A. Anthropometric indicators of obesity for identifying cardiometabolic risk factors in a rural Bangladeshi population. J Diab Invest. 2013;4(4):361–8.
Chehrei A, Sadrnia S, Keshteli AH, Daneshmand MA, Rezaei J. Correlation of dyslipidemia with waist to height ratio, waist circumference, and body mass index in Iranian adults. Asia Pac J Clin Nutr. 2007;16(2):248–53.
Mota Dos Santos C, Sa Silva C, Cesar de Araujo E, Kruze Grande de Arruda I, da Silva Diniz A, Coelho Cabral P. Lipid and glucose profiles in outpatients and their correlation with anthropometric indices. Rev Port Cardiol. 2013;32(1):35–41.
Bibiloni MM, Salas R, Pons A, Tur JA. Prevalence of dyslipidaemia and associated risk factors among Balearic Islands adolescents, a Mediterranean region. Eur J Clin Nutr. 2015;69(6):722–8.
Wang L, Xu F, Zhang XJ, Jin RM, Li X. Effect of high-fat diet on cholesterol metabolism in rats and its association with Na(+)/K(+)-ATPase/Src/pERK signaling pathway. J Huazhong Univ Sci Technol Med Sci. 2015;35(4):490–4.
Acknowledgements
We thank all participants who volunteered to take part in this study, all researchers of the MEWHC research team and the nurses and administrators in the ferromanganese refinery.We thank all study participants and researchers of the MEWHC study. And all authors make significant contributions to this article.
Funding
This research was funded by the National Natural Science Foundation of China [grant number 81860573] and Guangxi Natural Science Fund for Innovation Research Team [grant number 2017GXNSFGA198003].
Author information
Authors and Affiliations
Contributions
XBY contributed to conception and design; SFH, YTZ, DFL, LML, XC, LLH, HC, QZH, LLX, CQL and YFZ contributed to acquisition of the data; XYL, ZFL, XTG and analyzed the data and drafted the manuscript. LXY, ZFL and XTG contributed equally to this study. All authors approved the final manuscript of this article prior to submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Medical Ethics Committee of Guangxi Medical University approved this study. All participants were fully informed about the study purpose and methods and provided written consent to participate.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Luo, X., Liu, Z., Ge, X. et al. High manganese exposure decreased the risk of high triglycerides in workers: a cross-sectional study. BMC Public Health 20, 874 (2020). https://doi.org/10.1186/s12889-020-09011-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-020-09011-x