
Abstract
Objectives
This study aimed to evaluate and compare the abilities of waist circumference (WC), body mass index (BMI), hip circumference (HC), waist-to-hip ratio (WHR) and waist-to-height ratio (WHtR) to predict recently and previously diagnosed diabetes and hypertension and assess their appropriate cut-off values among Jordanian adults.
Methods
Data from the 2017 cardiovascular risk factors survey were analyzed to achieve the study objective. The survey collected extensive data from a national population-based sample of Jordanian residents. A structured questionnaire was used to collect sociodemographic variables and clinical data. Blood samples were taken for biochemical measurements. Anthropometric characteristics were measured by the same team of trained field researchers.
Results
This study included a total of 1193 men and 2863 women. Their age ranged from 18 to 90 year with a mean (SD) of 43.8 (14.2) year. WHtR performed better than other anthropometric measures and had a good ability (AUC > 0.80) among women and fair ability among men to predict newly diagnosed diabetes and previously diagnosed diabetes and hypertension. The appropriate cut-off points for anthropometric measures among women were 92 cm form WC, 104 cm for HC, 30 Kg/m2 for BMI, 0.85 for WHR, and 0.60 for WHtR. For men, the appropriate cut-off points were 100 cm for WC, 104 cm for HC, 27 Kg/m2 for BMI, 0.93 for WHR, and 0.57 for WHtR.
Conclusion
WHtR performed better than other anthropometric measures in predicting diabetes and hypertension among adult population in Jordan. We recommend WHtR as a measure of choice with a cut-off value of 0.6 for women and 0.57 for men to predict diabetes and hypertension among Jordanians.
Similar content being viewed by others


Introduction
The global burden of non-communicable diseases (NCDs) is immense and increasing. NCDs accounted for 70% of the estimated 56.4 million deaths worldwide in 2015, with almost 80% of these deaths are occurring in low- and middle-income countries [1]. In the Eastern Mediterranean Region (EMR), 57% of deaths in the region are attributed to NCDs [2]. Unhealthy diets, physical inactivity, and obesity are the main underlying risk factors of NCDs in the EMR [3]. In Jordan, the overall age-standardized prevalence rate of diabetes increased from 13.0% in 1994 to 23.7% in 2017 [4]. In 2017, the age-standardized prevalence of hypertension in Jordan was 33.8% among men and 29.4% among women [5].
Central obesity is a common cardiometabolic risk factor. Anthropometric measures including waist circumference (WC), body mass index (BMI), hip circumference (HC), waist-to-hip ratio (WHR) and waist-to-height ratio (WHtR) have been commonly used to predict the risk of diabetes and hypertension. BMI and WC are the most commonly used anthropometric measures for prediction of cardiometabolic risk factors [6]. However, BMI does not provide information on body fat distribution and WC does not take into account intraindividual and ethnic differences in lean body mass, body shape and height [6]. WHtR demonstrated higher ability than other anthropometric measures in predicting cardiometabolic abnormalities by taking into account both central fat deposition and intraindividual differences in height [7].
Considerable controversy still exists as to which measure most accurately defines body fat distribution. Studies from different countries and ethnicities in the world showed that anthropometric measures have different predictive powers for diabetes and hypertension [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24]. Therefore, the predictive power of anthropometric measures and their appropriate cut-off points should be established for different ethnicities. This study aimed to evaluate and compare the abilities of WC, BMI, WHR, HC and WHtR to predict recently and previously diagnosed diabetes and hypertension and assess their appropriate cut-off values among Jordanian adults.
Methods
Study design and sampling
A multipurpose national household survey was conducted among Jordanian adults over a period of four months in the year 2017. The detailed study design, methods, and procedures were described in previous publications [4, 5]. In brief, a multistage sampling technique was used to select a nationally representative sample from the population of Jordan. A village/city was selected from each of the 12 governorates of Jordan. The study procedures took place in the main health center in the selected villages/cities. The research team visited the households in the catchment area of the health center to invite adults to report to the center fasting in a given day after explaining the study for them. Subjects were asked not to take their medications in that day and to bring the medications with them to the health center. Subjects aged ≥18 years were eligible for inclusion in the study.
Data collection
Data were collected using a structured validated and pilot tested questionnaire by trained interviewers. The questionnaire was the same one that has been used in 2009 survey. The questionnaire included questions to assess the sociodemographic variables and clinical characteristics of participants, including self-reported diagnosis and treatment of diabetes and hypertension. Three blood samples were drawn from a cannula inserted into the antecubital vein and used for the different laboratory measurements. Tubes containing sodium fluoride potassium oxalate were used for glucose measurement. Samples were centrifuged within 1 h at the survey site, and transferred by separate labeled tubes in ice boxes to the central laboratory of the National Center of Diabetes, Endocrinology, and Genetics in Amman, Jordan. All biochemical measurements were carried out by the same team of laboratory technicians using the same method throughout the study period. Fasting plasma glucose was measured by the glucose oxidase method, using a Cobas Analyzer (Roche).
Anthropometric measurements
Single measurement was taken for each anthropometric measures. Weight was measured, while subjects minimally clothed without shoes using digital scales (seca). Height was measured using a portable stadiometer (SECA 214 portable stadiometer). BMI was calculated as weight in kilograms divided by height in meters squared. WC was measured at the midway between iliac crest and lower rib margin, over light clothing, using unstretchable tape (seca 203), without any pressure to body surface. WHR was calculated as WC divided by hip circumference and WHtR as WC divided by height in centimeter. Measurements were taken by the same team of well-trained persons using the same tools.
Variable definitions
Recently diagnosed diabetes was defined as having fasting blood sugar ≥126 mg/dl (≥7.0 mmol/l) at the time of the survey with no prior history of diabetes. Recently diagnosed hypertension was defined as having a blood pressure ≥ 140 mmHg systolic and/ or 90 mmHg diastolic at the time of the survey, with no prior history of hypertension. Previously diagnosis of diabetes and hypertension were self-reported by participants.
Statistical analysis
Data were entered and analyzed using the IBM SPSS, version 20. Data were described using means and percentages. Percentages were compared using chi-square test and difference between means were tested using independent t test. The performance of anthropometric measures was evaluated using receiver operating characteristics (ROC) analyses for each gender [25]. Validity of the test was assessed by calculating area under curve (AUC). The AUC values were classified as: 0.5–0.6 fail, 0.6–0.7 poor, 0.7–0.8 fair, 0.8–0.9 good and 0.9–1.0 excellent [26]. Appropriate cut-off values were defined based on Youden’s J statistic (maximum [sensitivity + specificity - 1]). To further judge the ability of anthropometric measures to predict previously and recently diagnosed diabetes and hypertension, anthropometric measures were dichotomized based on the established cut-off values in this study and tested for their associations using binary logistic regression after adjusting for age effect. All regression analyses were stratified by gender.
We did not adjust for multiple comparisons in analysis because almost all p-values were almost close to 0. A p-value < 0.05 was considered statistically significant.
Results
Participants’ characteristics
This study included a total of 1193 men and 2863 women. Their aged ranged from 18 to 90 years with a mean (SD) of 43.8 (14.2) year. About 27.3% of men and 15.1% of women were previously diagnosed with diabetes, 3.7% of men and 2.2% of women were recently diagnosed with diabetes, 28.2% of men and 21.4% of women were previously diagnosed with hypertension and 27.1% of men and 18.5% of women were recently diagnosed with hypertension. Table 1 shows the socio-demographic, anthropometric, and clinical characteristics of participants according to gender.
Table 2 shows the means and the 95% confidence intervals for the anthropometric characteristics for men and women. Women had significantly higher means of BMI, HC and WHtR and lower means of WC and WHR than men.
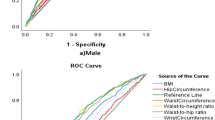
ROC analysis (Figs. 1 and 2) showed that all anthropometric measures had better performance to predict recently and previously diagnosed diabetes and hypertension among women than that among men. Table 3 shows the area under the ROC curve for men and women. Among women, WHtR performed better than other anthropometric measures and had a good accuracy (AUC > 0.80) to predict incident and prevalent cases of diabetes and prevalent cases of hypertension. It had fair accuracy to predict incident cases of hypertension. Among men, WHtR had fair accuracy and performed better than other anthropometric measures to predict recently and previously diagnosed diabetes and previously diagnosed hypertension. Moreover, WC had a good accuracy to predict recently diagnosed diabetes and previously diagnosed hypertension among women and fair accuracy to predict recently diagnosed diabetes and previously diagnosed hypertension among men. BMI and WHR had fair accuracy and HC had poor accuracy to predict the studied outcomes among women and had poor performance to predict the studied outcomes in men.

Receiver operating characteristic curve illustrating the ability of anthropometric measures to predict a recently diagnosed diabetes and b previously diagnosed diabetes according to gender

Receiver operating characteristic curve illustrating the ability of anthropometric measures to predict a recently diagnosed hypertension and b previously diagnosed hypertension according to gender
Youden’s J statistic was used to capture the performance of anthropometric measures and define appropriate cut-off values. The appropriate cut-off points for anthropometric measures among women were 92 cm for WC, 104 cm for HC, 30 Kg/m2 for BMI, 0.85 for WHR, and 0.60 for WHtR. For men, the appropriate cut-off points were 100 cm for WC, 104 cm for HC, 27 Kg/m2 for BMI, 0.93 for WHR, and 0.57 for WHtR (Table 4).
All anthropometric measures were dichotomized using the established cut-off values and tested for their associations with the studied outcomes after adjusting for age effect (Table 5). All dichotomized measures were significantly associated with increased odds of recently and previously diagnosed diabetes and hypertension, except HC that did not show significant association with recently and previously diagnosed diabetes. Among women, WC > 92 cm and WHtR> 0.60 were significantly associated with almost 3 to 5 times increased odds of recently and previously diagnosed diabetes and hypertension. Among men, WC > 100 cm and WHtR> 0.57 were significantly associated with almost 2 to 4 times increased odds of recently and previously diagnosed diabetes and hypertension.
Discussion
The findings of previous studies that compared the predictive power of anthropometric measures to predict cardiometabolic conditions are contradicting. Our study demonstrated a higher ability for WHtR to predict diabetes and hypertension among Jordanian adult men and women compared to other measures. This finding is consistent with the findings of other studies that showed WHtR a better predictor compared to other measures among women [8,9,10] and men [11] of different populations including a meta-analysis [12] of ten studies and a systematic review of 13 studies which demonstrated superiority of WHtR over other measures [13]. WHtR has been argued to be superior to a single measure of WC by taking into account intraindividual and ethnic differences in height [6]. However, there was a lot of inconsistency regarding the different anthropometric measures in predicting diabetes and hypertension. WHR was reported to be a better predictor in a number of countries [14,15,16,17]. Also, WC was reported to show superiority over other anthropometric measures in the prediction of type 2 diabetes in British women [18], U.S. men [19], German women [11], and Indian men and women [20].
Regarding BMI, systematic reviews [6, 21] encompassing Asian and Caucasian populations have consistently reported the inferior utility of BMI in identifying undiagnosed diabetes as compared with abdominal indices.
On the other hand, other studies demonstrated that BMI, WHR, WC, and WHtR had similar predictive powers for the risk of type 2 diabetes [24]. WHR, WC, and WHTR performed similarly well in Bangladeshi women [23]. A meta-analysis of 32 studies [24] showed that BMI, WHR, and WC had similar associations with incident diabetes.
Possible reasons for variation between studies might be due to ethnic and racial differences and differences in body composition and fat distribution between different ethnic groups, genders and age groups. Other reasons might include different study designs, different WC measurement protocols or different methods for defining cardiometabolic outcomes.
The appropriate cut-off points for predicting diabetes and hypertension among Jordanian women were 92 cm form WC, 104 cm for HC, 30 Kg/m2 for BMI, 0.85 for WHR, and 0.60 for WHtR. For men, the appropriate cut-off points were 100 cm for WC, 104 cm for HC, 27 Kg/m2 for BMI, 0.93 for WHR, and 0.57 for WHtR. Different cut-off values were reported for other populations. Ethnic and racial differences might explain the discrepancy in cut-off values between different studies.
The findings of ROC analysis in this study are supported by findings of the age-adjusted associations of dichotomized anthropometric measures with the outcome variables. WHtR and WC, using the established cut-off values, had strong association with previously and recently diagnosed diabetes and hypertension.
Our study had several strengths including a large national sample. In addition, the anthropometric measures were performed by the same team of field researchers. The main limitation of this study is the lower response rate (40%) in males. This is expected given that the employment rate in men in Jordan is much higher than that in women. An important limitation to consider when interpreting the findings is the possibility of measurement error (e.g. we measured the WC over light clothing). Another limitation is that the predictive ability of these anthropometric measures is correlated or associated with cardiovascular disease risk factors but not with cardiovascular disease events itself. So further studies are needed to correlate these measures with actual events.
Conclusions
WHtR performed the best in predicting diabetes and hypertension among adult population in Jordan. We recommend WHtR as a measure of choice with a cut-off value of 0.6 for women and 0.57 for men to predict diabetes and hypertension among Jordanians. Moreover, we recommend that WHtR should be measured routinely in health system and used as one of the indicators for the risk assessment of diabetes and hypertension.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AUC:
-
Area under curve
- BMI:
-
Body mass index
- EMR:
-
Eastern Mediterranean Region
- HC:
-
Hip circumference
- NCDs:
-
Non-communicable diseases
- ROC:
-
Receiver operating characteristics
- WC:
-
Waist circumference
- WHR:
-
Waist-to-hip ratio
- WHtR:
-
Waist-to-height ratio
References
World Health Organization. 2015. NCD mortality and morbidity, Global Health Observatory (GHO) data. Available at: http://www.who.int/gho/ncd/mortality_morbidity/en/ [Accessed 1 July, 2019].
World Health Organization. Regional Office of the Eastern Mediterranean: Non-Communicable diseases 2016. Available at: http://www.emro.who.int/entity/ncds/index.html [Accessed 1 July, 2019].
Rahim HF, Sibai A, Khader Y, Hwalla N, Fadhil I, Alsiyabi H, Mataria A, Mendis S, Mokdad AH, Husseini A. Non-communicable diseases in the Arab world. Lancet. 2014;383(9914):356–67.
Ajlouni K, Batieha A, Jaddou H, Khader Y, Abdo N, El-Khateeb M, Hyassat D, Al-Louzi D. Time trends in diabetes mellitus in Jordan between 1994 and 2017. Diabet Med. 2019. https://doi.org/10.1111/dme.13894.
Khader Y, Batieha A, Jaddou H, Rawashdeh SI, El-Khateeb M, Hyassat D, Khader A, Ajlouni K. Hypertension in Jordan: prevalence, awareness, control, and its associated factors. Int J Hypertens. 2019;2019:3210617.
Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. 2012;13:275–86.
Ashwell M, Gibson S. Waist-to-height ratio as an indicator of ‘early health risk': simpler and more predictive than using a ‘matrix' based on BMI and waist circumference. BMJ Open. 2016;6:e010159.
Lin WY, Lee LT, Chen CY, Lo H, Hsia HH, Liu IL, Lin RS, Shau WY, Huang KC. Optimal cut-off values for obesity:using simple anthropometric indices to predict cardiovascular risk factors in Taiwan. Int J Obes Relat Metab Disord. 2002;26(9):1232–8.
Zhang ZQ, Deng J, He LP, Ling WH, Su YX, Chen YM. Comparison of various anthropometric and body fat indices in identifying cardiometabolic disturbances in Chinese men and women. PLoS One. 2013;8:e70893.
Pua YH, Ong PH. Anthropometric indices as screening tools for cardiovascular risk factors in Singaporean women. Asia Pac J Clin Nutr. 2005;14(1):74–9.
Schulze MB, Heidemann C, Schienkiewitz A, Bergmann MM, Hoffmann K, Boeing H. Comparison of anthropometric characteristics in predicting the incidence of type 2 diabetes in the EPIC-Potsdam study. Diabetes Care. 2006;29(8):1921–3.
Lee CM, Huxley RR, Wildman RP, Woodward M. Indices of abdominal obesity are better discriminators of cardiovascular risk factors than BMI: a meta-analysis. J Clin Epidemiol. 2008;61(7):646–53.
Corrêa MM, Thumé E, De Oliveira ER, Tomasi E. Performance of the waist-to-height ratio in identifying obesity and predicting non-communicable diseases in the elderly population: A systematic literature review. Arch Gerontol Geriatr. 2016;65:174–82.
Esmaillzadeh A, Mirmiran P, Azizi F. Waist-to-hip ratio is a better screening measure for cardiovascular riskfactors than other anthropometric indicators in Tehranian adult men. Int J Obes Relat Metab Disord. 2004;28(10):1325–32.
Mirmiran P, Esmaillzadeh A, Azizi F. Detection of cardiovascular risk factors by anthropometric measures in Tehranian adults: receiver operating characteristic (ROC) curve analysis. Eur J Clin Nutr. 2004;58(8):1110–8.
Ta MT, Nguyen KT, Nguyen ND, Campbell LV, Nguyen TV. Identification of undiagnosed type 2 diabetes by systolic blood pressure and waist-to-hip ratio. Diabetologia. 2010;53(10):2139–46.
Mansour AA, Al-Jazairi MI. Cut off values for anthropometric variables that confer increased risk of type 2 diabetes mellitus and hypertension in Iraq. Arch Med Res. 2007;38(2):253–8.
Taylor AE, Ebrahim S, Ben-Shlomo Y, Martin RM, Whincup PH, Yarnell JW, Wannamethee SG, Lawlor DA. Comparison of the associations of body mass index and measures of central adiposity and fat mass with coronary heart disease, diabetes, and all-cause mortality: a study using data from 4 UK cohorts. Am J Clin Nutr. 2010;91(3):547–56.
Wang H, Liu A, Zhao T, Gong X, Pang T, Zhou Y, Xiao Y, Yan Y, Fan C, Teng W, Lai Y, Shan Z. Comparison of anthropometric indices for predicting the risk of metabolic syndrome and its components in Chinese adults: a prospective, longitudinal study. BMJ Open. 2017;7(9):e016062.
Mamtani MR, Kulkarni HR. Predictive performance of anthropometric indexes of central obesity for the risk of type 2 diabetes. Arch Med Res. 2005;36(5):581–9.
Browning LM, Hsieh SD, Ashwell M. A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0.5 could be a suitable global boundary value. Nutr Res Rev. 2010;23:247–69.
Sargeant LA, Bennett FI, Forrester TE, Cooper RS, Wilks RJ. Predicting incident diabetes in Jamaica: the role of anthropometry. Obes Res. 2002;10(8):792–8.
Bhowmik B, Munir SB, Diep LM, et al. Anthropometric indicators of obesity for identifying cardiometabolic risk factors in a rural Bangladeshi population. J Diabetes Invest. 2013;4:361–8.
Vazquez G, Duval S, Jacobs DR Jr, Silventoinen K. Comparison of body mass index, waist circumference, and waist/hip ratio in predicting incident diabetes: a meta-analysis. Epidemiol Rev. 2007;29:115–28.
Swets JA. Measuring the accuracy of diagnostic systems. Science. 1988;240:1285–93.
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–45.
Acknowledgements
Not applicable.
Funding
The study is funded by the Research Fund at Jordan Ministry of Higher Education. The funding body has no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
ME and KA conducted the laboratory analysis. YK, AB, AJ supervised the data collection and analyzed the data. All authors wrote, read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Institutional Review Board at the National Center for Diabetes, Endocrinology, and Genetics. All participants signed the informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Khader, Y., Batieha, A., Jaddou, H. et al. The performance of anthropometric measures to predict diabetes mellitus and hypertension among adults in Jordan. BMC Public Health 19, 1416 (2019). https://doi.org/10.1186/s12889-019-7801-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-019-7801-2