
Abstract
Background
The relationship between Vitamin D levels and pediatric celiac disease (CD) remains controversial. In this study, we conducted a systematic review and meta-analysis to examine the relationship between Vitamin D and pediatric CD. Methods: We screened relevant studies from PubMed, EMBASE, and Web of Science published in English from January 1, 2000, to August 1, 2023. The included studies were assessed according to the STROBE checklist. Heterogeneity was quantified by Cochran’s Q test and the I2 statistic. Publication bias was estimated by Begg’s test and Egger’s test. Meta‐regression was used to detect potential sources of heterogeneity. Results: A total of 26 studies were included in the meta-analysis. Nineteen articles compared 25(OH)D3 levels between CD patients and control groups, average 25-hydroxyvitamin D3 [25(OH)D3 or calcidiol], and 1,25-dihydroxyvitamin D3 [1,25(OH)2D3 or calcitriol] levels, as the main forms of Vitamin D, there was a significant difference in CD patients and healthy controls (weighted mean difference (WMD) = − 5.77, 95% confidence interval (CI) = [− 10.86, − 0.69] nmol/L). Meanwhile, eleven articles reported the numbers of patients and controls with Vitamin D deficiency, there was a significant difference in the incidence of 25(OH)D3 deficiency between CD patients and healthy controls (odds ratio 2.20, 95% CI= [1.19, 4.08]). Nine articles reported changes in 25(OH)D3 levels before and after administering a GFD in patients with CD, the result of this study revealed the increase of 25(OH)D3 levels in CD patients after a gluten-free diet (GFD) (WMD = − 6.74, 95% CI = [− 9.78, − 3.70] nmol/L). Conclusions: Vitamin D levels in pediatric CD patients were lower than in healthy controls, and 25(OH)D3 deficiency was more prevalent in CD patients. We found that 25(OH)D3 levels were elevated in CD patients after GFD, which is consistent with previous research. Further well-designed, longitudinal, prospective cohort studies focusing on the role of Vitamin D in the pathogenesis of CD are therefore needed.
Similar content being viewed by others


Introduction
Celiac disease (CD) is an immune-mediated systemic disorder caused by intolerance to gluten found in barley and rye [1]. CD affects the small intestine in genetically susceptible individuals [2]. Improvements in the diagnosis and awareness of the disease have greatly increased the apparent incidence of CD [3], with a 2–4-fold increase in the number of confirmed CD patients in Europe and the United States during the last two decades [4, 5]. Research has shown that the incidence of CD to be increasing by 7.5% per year over the past several decades [5]. Of 65,957 screened children, 891 had CD, with a prevalence of CD is 0.9%, which was significantly greater in children than adults (0.5%) according to the global prevalence of CD [6]. The prevalence of CD varied from 0.3% in Iran to 0.7% in Israel between various Asian countries [7]. CD mainly affects the small intestine, however, the clinical manifestations are extensive, with both intestinal and parenteral symptoms [8]. The intestinal and extra-intestinal clinical symptoms of CD vary, but the most prominent symptom is proximal intestinal malabsorption, and chronic diarrhea, which can appear over weeks or months [1, 9]. The extra-intestinal symptoms include iron deficiency anemia, faltering growth, weight loss, failure to thrive, delayed puberty, and mouth ulcers [9, 10]. Although the incidence of pediatric CD is increasing, its pathogenesis remains unclear. CD generally occurs in genetically susceptible individuals who respond to unknown environmental factors with an immune response that is subsequently triggered by the intake of gluten [11]. Environmental factors, such as the duration of gluten exposure, play important roles in the development of CD [12]. However, CD occurs only in about 1% of the population, suggesting that other environmental factors besides gluten are probably important, such as Vitamin D, infant feeding practices, delivery method, the season of birth, elective cesarean section, intestinal microbiome, time of gluten introduction, acute viral gastrointestinal infection, and micronutrient deficiency [13,14,15,16,17,18]. Vitamin D levels may also be associated with CD, and Yavuz et al. revealed significantly reduced levels of Vitamin D in pediatric patients with newly diagnosed CD [19]. The main treatment for CD remains adherence to a lifelong GFD, which requires significant education, motivation, and follow-up of the patient, with improvement and resolution of symptoms usually occurring within days or weeks [20]. Two advanced clinical trials actively developing and testing pharmacological approaches to treat CD, include AT-1001 (Larazotide acetate, which aims to close the villi’s tight junctions) and IMGX-003 (Latiglutenase; formerly known as ALV003, acts as a gluten endopeptidase that degrades gluten before being absorbed in the small intestine) therapies [21].
Vitamin D is a fat-soluble vitamin that exerts its biological effects by binding to Vitamin D receptors [22], which are distributed in various tissues and cells throughout the human body, and subsequently participates in numerous biological processes, including immunity, metabolism, and inflammation [23, 24]. Vitamin D, as an immune modulator, is known to regulate immune response and maybe implicated in disease pathogenesis or susceptibility of CD. Components of the immune system, such as B-lymphocytes, T-lymphocytes, and dendritic cells, are influenced by the regulatory effects of Vitamin D and expressed Vitamin D receptor (VDR), which is involved in the biological activity of 1,25(OH)2D3, and these cells also have the capability of locally synthesizing active 1,25(OH)2D3 [25]. Increasing evidence also suggests that Vitamin D deficiency increases the risk and worsens the outcome of extraskeletal diseases such as cancer, irritable bowel syndrome, and inflammatory bowel disease [26].
GFD remains the only effective treatment for CD [27]. Strict adherence to a GFD over a year has been shown to lead to partial healing of the duodenal mucosa along with the resolution of gastrointestinal and extraintestinal manifestations as well as complications such as malabsorption and osteoporosis while having similar results in mucosal structural recovery, reduction in intestinal mucosal inflammation, antibody concentrations, and symptom improvement [28,29,30]. Cross-contamination of GFD foods has emerged as a threat to chronic low-dose gluten exposure in CD patients, daily gluten intake below a specific threshold should be determined [31]. Several studies established a safe threshold of daily gluten intake, 100 mg gliadin/day (= about 200 mg of gluten or 2–5 g wheat flour) displayed minimal morphometric changes in the jejunal histology [32]. Gluten-free foods are less available and cost more, while in CD with GFD, symptoms can relieved and quality of life can be significantly improved [33, 34]. Beyond patients with CD, GFD is also recognized in the treatment of gluten ataxia, dermatitis herpetiformis, cognitive impairment, inflammatory bowel disease and irritable bowel syndrome, dermatitis herpetiformis, and non-celiac gluten sensitivity [27]. Adverse events of GFD may worsen the gut microbiota while having nutritional deficiencies in iron, calcium, and fiber, also include the negative social and psychological impacts that many GFD adherents experience [35, 36].
However, the relationship between Vitamin D and pediatric CD presents new challenges. For example, Ahlawat et al. found no significant difference in Vitamin D levels between patients with newly diagnosed CD and controls [37]. We therefore conducted a systematic review and meta-analysis to quantify the relationship between Vitamin D and pediatric CD, with the aim of providing new clues to the cause of pediatric CD.
Methods
Data selection
We searched for relevant articles published in English from January 1, 2000, to July 1, 2023, in the PubMed, EMBASE, and Web of Science databases. The following search terms were used: ((Coeliac disease) OR (gluten-induced enteropathy) OR (gluten-sensitive enteropathy) OR (Celiac disease) OR (Celiac sprue)) AND ((Vitamin D) OR (25(OH)D3) OR (Cholecalciferol) OR (25-Hydroxyvitamin D) OR (Hydroxycholecalciferols) OR (Ergocalciferols) OR (Dihydrotachysterol)) AND ((children) OR (adolescent) OR (pediatric)). The inclusion criteria were: (1) published as full English research articles; (2) pediatric CD; (3) unified definition and diagnosis of CD; and (4) supporting data for Vitamin D. Articles that did not meet the above criteria and duplicate publications were excluded. The main form of Vitamin D is 25(OH)D3 level, which is usually tested as a measure of Vitamin D levels. A 25(OH)D3 unit is defined as 1 ng/mL = 2.5 nmol/L, and levels of 25(OH)D3 were categorized as normal (≥ 70 nmol/L), insufficient (< 70 nmol/L), and deficient (< 50 nmol/L) [38].
Articles for selection were screened independently by two authors, who also screened the identified full articles. In the case of disagreement, the articles were evaluated by a third author to reach a final agreement.
Article assessment
Risk of bias and quality assessment were assessed according to the STROBE checklist for the included studies [39]. The meta-analysis was also conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [40].
Data extraction
Data were extracted to Numbers (Apple Distribution International, Seattle, USA) for statistical analysis. The following data were obtained from the included studies: basic characteristics including author, published year, country, detection method of 25(OH)D3, and diagnostic criteria of CD; 25(OH)D3 levels (mean ± standard deviation (SD)) in CD patients and controls; numbers of CD patients and controls; and treatment method of CD. Finally, all data were double-checked by two authors.
Statistical analysis
In this study, we analyzed weighted mean difference (WMD) after combining mean and SD values for 25(OH)D3 levels. Odds ratios (ORs) and 95% confidence intervals (CIs) were used to calculate the incidences of 25(OH)D3 deficiency in CD patients and healthy controls. Statistical heterogeneity was assessed by Cochran’s Q test and the I2 statistic. For heterogeneous results, publication bias was estimated by Begg’s test and Egger’s test (P > 0.5, there is no publication bias). Pooled estimates were obtained using a fixed-effects model (Mantel and Haenszel, M-H) if I2 ≤ 50% and P > 0.1, or a random‐effects model (M‐H heterology) if I2 > 50% and P ≤ 0.1. Potential sources of heterogeneity were detected by meta-regression analysis (Monte Carlo permutation test) to enhance the credibility of the results. All analyses were carried out using STATA (Version 15.1, StataCorp., College Station, TX, USA) and Review Manager (Version 5.3, The Nordic Cochrane Centre, Rigshospitalet, Denmark).
Results
Basic characteristics
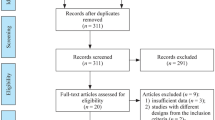
A total of 813 potential unique references were searched, of which 26 studies [19, 37, 41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65] met the inclusion criteria. A flowchart describing the study-selection process is shown in Fig. 1. The 26 studies included 3,120 subjects, comprising 1,495 CD patients and 1,607 non-CD participants. Most of the subjects were from the Middle East, Europe, and North America. CD was mainly diagnosed in the duodenal mucosa and by positive serological markers of disease. Most studies analyzed 25(OH)D3 by chemiluminescent immunoassay. Nineteen articles compared 25(OH)D3 levels between CD patients and control groups [19, 37, 41,42,43,44, 46, 49,50,51,52, 54,55,56,57, 59, 60, 66, 67], of which eleven found lower 25(OH)D3 levels in CD patients compared with controls [41, 42, 44, 49, 52, 55, 57, 59, 60, 66, 67]. Eleven articles reported the numbers of patients and controls with Vitamin D deficiency [19, 37, 42, 46, 49, 50, 52, 54, 57, 59, 67], and eight showed that 25(OH)D3 deficiency was more prevalent in CD patients [19, 42, 49, 50, 52, 57, 59, 67]. In addition, nine articles reported changes in 25(OH)D3 levels before and after administering a GFD in patients with CD [41, 47, 48, 52, 56, 61,62,63,64,65], all concluded a significant increase in Vitamin D levels after a GFD treatment [41, 56, 61,62,63,64]. The meta-analysis was conducted using a random-effect model or fixed effect model.

Flowchart of study-selection process
Comparison of 25(OH)D3 levels in CD patients and healthy controls
The included studies, comprising 1,495 CD patients and 1,607 healthy controls, are listed in Table 1. The mean 25(OH)D3 levels were 57.39 nmol/L in CD patients and 64.08 nmol/L in healthy controls. The average 25(OH)D3 level in CD patients was 6.7 nmol/L lower than that in controls, and the difference was significant (WMD = − 5.77 95% CI = [− 10.86, − 0.69] nmol/L) (Fig. 2). As shown in Fig. 3, the funnel plot was used to identify the presence of the publication bias preliminary. Funnel plot is a simple scatter plot that reflects estimates of the intervention effects of a single study with a given sample size or accuracy, a useful tool for meta-analysis, which can be combined with relevant statistical tests to check for reporting bias in systematic reviews preliminary [68]. Funnel plot asymmetry cannot be equated with publication bias, because it has several other possible causes, such as heterogeneity, reporting bias, and chance may all lead to asymmetry or other shapes in funnel plots [69]. Funnel plots can help guide the choice of meta-analysis method. Random effects meta-analyses weight studies relatively more equally than fixed effect analyses by incorporating the between study variance into the denominator of each weight [70]. The asymmetry of the distribution of studies in the plot may be due to selection bias, publication bias citation bias, or multiple publication bias. The P values of Begg’s test and Egger’s test are 0.95 and 0.54, respectively, both > 0.5, indicating no publication bias. There was no abnormal sensitivity analysis, and meta-regression found no heterogeneity in terms of location, race, or publication year.

Forest plot showing significant difference in average 25(OH)D3 levels between pediatric CD patients and controls (WMD = − 5.77, 95% CI = [− 10.86, − 0.69] nmol/L)

Funnel plot of the meta-analysis
The pooled data from four included studies showed 25(OH)D3 deficiency in of 33.96% patients with CD and 18.60% of healthy controls. The meta-analysis found a significant difference in the incidence of 25(OH)D3 deficiency between CD patients and healthy controls (OR = 2.20, 95% CI = [1.19, 4.08]) (Fig. 4).

Forest plot showing significant difference in the incidence of 25(OH)D3 deficiency between patients with CD and healthy controls (OR = 2.20, 95% CI = [1.19, 4.08])
Changes in 25(OH)D3 levels after CD treatment
We examined changes in 25(OH)D3 levels in patients with CD before and after a GFD treatment in nine articles with relevant information (Table 2). All articles concluded the increase in Vitamin D levels after a GFD treatment, comprising 624 CD patients and 532 healthy controls. The results produced by STATA software, WMD were analyzed after combining mean and SD values for 25(OH)D3 levels, and 95% CIs were used to calculate the changes of 25(OH)D3 before and after a GFD treatment in CD patients. Overall WMD = − 6.74, 95% CI = [− 9.78, − 3.70] nmol/L, the diamond shape did not pass through the origin, indicating a significant increase in 25(OH)D3 levels in CD patients before and after a GFD treatment. (Fig. 5).

Forest plot showing no significant difference in 25(OH)D3 levels between CD patients pre-treatment and post-treatment with GFD (WMD = − 6.74, 95% CI = [− 9.78, − 3.70] nmol/L)
Discussion
The results of previous studies regarding differences in Vitamin D levels between pediatric patients with CD and healthy controls have been inconsistent. The results of the current meta-analysis suggested that Vitamin D levels in pediatric CD patients were lower than healthy individuals, the 25(OH)D3 deficiency was more prevalent in CD patients. However, the Vitamin D levels in CD patients did not change before and after GFD. Overall, these results indicate the need for further research into the role of Vitamin D in the pathogenesis of CD.
The current study demonstrates a relationship between pediatric CD and Vitamin D, Vitamin D may be related to the incidence of CD. Gastrointestinal infections may be related to CD [71], and rotavirus infection in children has been reported to be a risk factor for the development of CD [72]. In addition, early infection in the neonatal period and childhood and antibiotic exposure have also been closely related to the occurrence of CD [73, 74]. Meanwhile, Vitamin D is involved in the process of resistance to infection. Vitamin D has been reported to induce the antibacterial peptide cathelicidin [75], which has in turn demonstrated direct antibacterial, antifungal, and antiviral properties [76]. The anti-infective properties of Vitamin D may thus be related to the onset of CD. Vitamin D levels may be influenced by three potential sources: nutrient sources, UVB-dependent endogenous production, and supplements. Most of the studies were from the Middle East, Europe, and North America. Some countries like the United States and Canada fortify staple products such as dairy products with Vitamin D. Thus, the individual Vitamin D dietary intake is highly dependent on nutritional habits, and the country’s fortification strategy [25]. However, a global perspective review found that 6 to 47% of Vitamin D intake may come from dietary supplements [77, 78]. Thus, Vitamin D status in the absence of supplementation is largely determined by endogenous Vitamin D production, which is also influenced by genetic determinants, latitude, season, skin pigmentation, and lifestyle [79, 80]. Because Vitamin D levels have been shown to be seasonally dependent, an individual’s 25(OH)D3 levels are lowest after winter and highest in late summer [81]. This factor should therefore be taken into account when interpreting individual Vitamin D levels.
Vitamin D can regulate both innate and adaptive immune system activity [82]. The risk of CD development is greater when patients with potentially associated Vitamin D hypovitaminosis [83]. Vitamin D may have a key role in CD onset by two key factors: immune response regulation through action on dendritic cells and T-cells, and on intestinal permeability by regulating inflammatory cytokines and zonulin release pathway [84]. Vitamin D in the intestines can maintain gut homeostasis by synthesis 1α,25(OH)2D3 and VDR expression, especially since an optimal 1α,25(OH)2D3 status is vital, as it participates in regulatory activities regarding not only calcium absorption but also infection protection, epithelial barrier function preservation, and gut microbiota modulation [85]. Vitamin D in CD can also affect tight junctions, which are the major junctions responsible for intestinal mucosa barrier regulation [86]. Research showed 25(OH)D3 concentrations < 30 nmol/L and > 75 nmol/L during early infancy were associated with an increased risk of developing celiac disease autoimmunity in genetically at-risk children [87]. However, the conclusion on VD supplementation in patients with celiac disease is still unclear. Patients with Vitamin D deficiency (< 30 nmol/L) were given 60,000 IU of Vitamin D per week during the first 3 months of treatment, after which vitamin D was discontinued and they were advised to follow GFD, after 6 months, showed a significant increase in Vitamin D serum levels (from 23.63 ± 1.13 nmol/L to 33.83 ± 3.8 nmol/L), but no case reached normal VD values [64]. Vitamin D status could be affected by compliance with the gluten-free diet, poor absorption, and decreased intake [88]. However, regardless of Vitamin D levels at onset or during GFD, most experts recommend monitoring Vitamin D serum levels in all patients, especially when Vitamin D deficiency is recommended to correct with Vitamin D supplements [89]. More studies are warranted to evaluate the effect of strict dietary adherence to the GFD and its effect on Vitamin D supplements.
Previous studies have shown that vitamin D levels in the CD group are negatively correlated with symptom severity, which means the lower the vitamin D levels, the more severe the symptoms of CD patients [44]. Vitamin D deficiency is associated with reduced expression of the Vitamin D receptor and epithelial barrier proteins E-cadherin and claudin-2, which play an important role in children with CD in correlation with histological manifestations of disease severity [59]. These findings suggest that in CD patients, the structure of the paracellular pathway responsible for calcium absorption is disturbed and that Vitamin D deficiency exacerbates CD.
The proximal small intestine is the most commonly implicated intestine segment in CD, leading to disrupted absorption of some nutrients such as Vitamin D and the occurrence of diarrhea, further suggesting a possible relationship between Vitamin D deficiency and CD progression. Since the amount of those autoantibodies such as anti-endomysium and anti-transglutaminase is positively correlated to the degree of intestinal atrophy and the magnitude of the inflammatory infiltrate, the minor role played by Vitamin D malabsorption in CD is supported [90]. However, no deficiencies in other fat-soluble vitamins, such as vitamins K and A, have been found. The limited number of studies has led to inconsistent results. For example, Imam et al. observed that deficiencies of fat-soluble vitamins were uncommon in children with a new diagnosis of CD, suggesting that routine measurement of fat-soluble vitamin levels may not be necessary [91]. However, Vitamin D levels are known to be affected by many factors, such as diet and sun exposure, especially in children [22]. These issues may be affected by various factors during childhood. The Fok1 T-allele of Vitamin D receptor has an association with serum 25(OH)D3 deficiency in patients with CD, which plays a critical role in immunomodulation and maintaining barrier integrity [92]. The current meta-analysis shows an association between Vitamin D levels and the deficiency and CD, whether it is involved or not in the pathogenesis cannot be ruled out.
Significant difference in 25(OH)D3 levels between CD patients pre-treatment and post-treatment with GFD, research showed that oligofructose-enriched inulin added to the GFD essentially can improve Vitamin D and E status in pediatric CD patients [62]. Lu et al. observed CD had decreased serum 25(OH)D3 levels, which returned to normal after treatment [93]. Further studies of the effects of GFD in CD patients are needed to clarify the correlation. Given that GFD is a strict lifelong gluten-free therapy to maintain a healthy status, the nutrient intakes will change, calcium, magnesium, iron, and Vitamin D intakes were particularly insufficient in pediatric CD, it may expose CD patients to high fat and low essential micronutrient intakes, nutrition intake must be monitored to prevent the occurrence of diseases during treatment, such as cardiovascular or bone disorders [94].
Deficiency of Vitamin D related to nutrient malabsorption secondary to epithelial damage is frequent in untreated CD patients,
This study had several limitations. First, we did not perform subgroup analysis because the number of included studies was relatively small. Second, there were high heterogeneity and confounding factors in this meta-analysis, including age, sex, ethnicity, season, diet intake, and treatment. Compared to the normal controls, children with CD had a high intake of fiber, glycemic index, and glycemic load and lower intakes of folate [95]. However, not all the included studies provided adjusted values and we were therefore unable to pool the results by adjusting for these confounders. Finally, there was a lack of prospective studies and randomized controlled trials. Thus, although the study found a correlation between Vitamin D levels and CD, it lacks causal relationships, and we could only state that Vitamin D levels seem to differ between pediatric patients with CD and healthy controls. Further studies of the effects of Vitamin D supplementation in patients with CD could provide further evidence for any relationship. In addition, previous original studies did not adjust for potentially important confounders, such as body mass index, race, and dietary habits. Finally, although the existence of heterogeneity might bias the results, the current analysis found no major source of heterogeneity, suggesting that it was appropriate to carry out pooled analyses.
Conclusion
Our study showed that 11 articles found that 25(OH)D3 levels were lower in CD patients compared to controls, 8 articles showed that 25(OH)D3 deficiency was more prevalent in CD patients, and 9 articles concluded that vitamin D levels increased significantly after a GFD treatment. In summary, Vitamin D levels were lower in pediatric patients with CD compared with healthy controls, Vitamin D deficiency was prevalent in pediatric CD patients, while Vitamin D levels increased after a GFD according to the result of meta-analysis, demonstrating that Vitamin D may play a critical role in pediatric CD. Further prospective studies are therefore needed to clarify the association between Vitamin D and CD, including randomized controlled trials of the effects of Vitamin D supplementation in patients with CD.
Data availability
All data generated or analysed during this study are included in this published article.
References
Catassi C, Verdu EF, Bai JC, Lionetti E. Coeliac disease. Lancet. 2022;399(10344):2413–26.
Trynka G, Hunt KA, Bockett NA, Romanos J, Mistry V, Szperl A, et al. Dense genotyping identifies and localizes multiple common and rare variant association signals in celiac disease. Nat Genet. 2011;43(12):1193–201.
Choung RS, Larson SA, Khaleghi S, Rubio-Tapia A, Ovsyannikova IG, King KS, et al. Prevalence and morbidity of undiagnosed Celiac Disease from a community-based study. Gastroenterology. 2017;152(4):830–e8395.
Rubio-Tapia A, Kyle RA, Kaplan EL, Johnson DR, Page W, Erdtmann F, et al. Increased prevalence and mortality in undiagnosed celiac disease. Gastroenterology. 2009;137(1):88–93.
King JA, Jeong J, Underwood FE, Quan J, Panaccione N, Windsor JW, et al. Incidence of Celiac Disease is increasing over time: a systematic review and Meta-analysis. Am J Gastroenterol. 2020;115(4):507–25.
Singh P, Arora A, Strand TA, Leffler DA, Catassi C, Green PH, et al. Global prevalence of Celiac Disease: systematic review and Meta-analysis. Clin Gastroenterol Hepatol. 2018;16(6):823–e8362.
Singh P, Arora S, Singh A, Strand TA, Makharia GK. Prevalence of celiac disease in Asia: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2016;31(6):1095–101.
Green PH, Jabri B. Coeliac disease. Lancet. 2003;362(9381):383–91.
Paul SP, Kirkham EN, Pidgeon S, Sandmann S. Coeliac disease in children. Nurs Stand. 2015;29(49):36–41.
Downey L, Houten R, Murch S, Longson D. Recognition, assessment, and management of coeliac disease: summary of updated NICE guidance. BMJ. 2015;351:h4513.
Lebwohl B, Sanders DS, Green PHR. Coeliac disease. Lancet. 2018;391(10115):70–81.
Fasano A, Berti I, Gerarduzzi T, Not T, Colletti RB, Drago S, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med. 2003;163(3):286–92.
Ivarsson A, Persson LA, Nyström L, Ascher H, Cavell B, Danielsson L, et al. Epidemic of coeliac disease in Swedish children. Acta Paediatr. 2000;89(2):165–71.
Tanpowpong P, Obuch JC, Jiang H, McCarty CE, Katz AJ, Leffler DA, et al. Multicenter study on season of birth and celiac disease: evidence for a new theoretical model of pathogenesis. J Pediatr. 2013;162(3):501–4.
Lionetti E, Castellaneta S, Francavilla R, Pulvirenti A, Catassi C. Mode of Delivery and Risk of Celiac Disease: risk of Celiac Disease and Age at Gluten introduction Cohort Study. J Pediatr. 2017;184:81–e862.
Galipeau HJ, McCarville JL, Huebener S, Litwin O, Meisel M, Jabri B, et al. Intestinal microbiota modulates gluten-induced immunopathology in humanized mice. Am J Pathol. 2015;185(11):2969–82.
Gunasekar A, Seth A, Kumar P, Jain A. Relationship between vitamin D deficiency and coeliac disease in children. Paediatr Int Child Health. 2022;42(3–4):175–6.
Verdu EF, Schuppan D. Co-factors, microbes, and Immunogenetics in Celiac Disease to Guide Novel approaches for diagnosis and treatment. Gastroenterology. 2021;161(5):1395–e14114.
Tokgöz Y, Terlemez S, Karul A. Fat soluble vitamin levels in children with newly diagnosed celiac disease, a case control study. BMC Pediatr. 2018;18(1):130.
Al-Toma A, Volta U, Auricchio R, Castillejo G, Sanders DS, Cellier C, et al. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur Gastroenterol J. 2019;7(5):583–613.
Kulkarni A, Patel S, Khanna D, Parmar MS. Current pharmacological approaches and potential future therapies for celiac disease. Eur J Pharmacol. 2021;909:174434.
Lu C, Yang J, Yu W, Li D, Xiang Z, Lin Y, et al. Association between 25(OH)D Level, Ultraviolet exposure, geographical location, and inflammatory bowel Disease Activity: a systematic review and Meta-analysis. PLoS ONE. 2015;10(7):e0132036.
Bouillon R, Carmeliet G, Verlinden L, van Etten E, Verstuyf A, Luderer HF, et al. Vitamin D and human health: lessons from vitamin D receptor null mice. Endocr Rev. 2008;29(6):726–76.
Gascon-Barré M, Demers C, Mirshahi A, Néron S, Zalzal S, Nanci A. The normal liver harbors the vitamin D nuclear receptor in nonparenchymal and biliary epithelial cells. Hepatology. 2003;37(5):1034–42.
Prietl B, Treiber G, Pieber TR, Amrein K. Vitamin D and immune function. Nutrients. 2013;5(7):2502–21.
Feldman D, Krishnan AV, Swami S, Giovannucci E, Feldman BJ. The role of vitamin D in reducing cancer risk and progression. Nat Rev Cancer. 2014;14(5):342–57.
Aljada B, Zohni A, El-Matary W. The Gluten-Free Diet for Celiac Disease and Beyond. Nutrients, 2021. 13(11).
Laurikka P, Salmi T, Collin P, Huhtala H, Mäki M, Kaukinen K et al. Gastrointestinal symptoms in Celiac Disease patients on a long-term gluten-free Diet. Nutrients, 2016. 8(7).
Pantaleoni S, Luchino M, Adriani A, Pellicano R, Stradella D, Ribaldone DG, et al. Bone mineral density at diagnosis of celiac disease and after 1 year of gluten-free diet. ScientificWorldJournal. 2014;2014:p173082.
Kurppa K, Collin P, Viljamaa M, Haimila K, Saavalainen P, Partanen J, et al. Diagnosing mild enteropathy celiac disease: a randomized, controlled clinical study. Gastroenterology. 2009;136(3):816–23.
Wieser H, Segura V, Ruiz-Carnicer Á, Sousa C, Comino I. Food Safety and Cross-contamination of Gluten-Free products: a narrative review. Nutrients, 2021. 13(7).
Itzlinger A, Branchi F, Elli L, Schumann M. Gluten-Free Diet in Celiac Disease-Forever and for all? Nutrients, 2018. 10(11).
Singh J, Whelan K. Limited availability and higher cost of gluten-free foods. J Hum Nutr Diet. 2011;24(5):479–86.
Mustalahti K, Lohiniemi S, Collin P, Vuolteenaho N, Laippala P, Mäki M. Gluten-free diet and quality of life in patients with screen-detected celiac disease. Eff Clin Pract. 2002;5(3):105–13.
Deora V, Aylward N, Sokoro A, El-Matary W. Serum Vitamins and Minerals at diagnosis and follow-up in Children with Celiac Disease. J Pediatr Gastroenterol Nutr. 2017;65(2):185–9.
Silvester JA, Weiten D, Graff LA, Walker JR, Duerksen DR. Living gluten-free: adherence, knowledge, lifestyle adaptations and feelings towards a gluten-free diet. J Hum Nutr Diet. 2016;29(3):374–82.
Ahlawat R, Weinstein T, Markowitz J, Kohn N, Pettei MJ. Should we assess vitamin D status in Pediatric patients with Celiac Disease? J Pediatr Gastroenterol Nutr. 2019;69(4):449–54.
Madden K, Feldman HA, Smith EM, Gordon CM, Keisling SM, Sullivan RM, et al. Vitamin D deficiency in critically ill children. Pediatrics. 2012;130(3):421–8.
Skrivankova VW, Richmond RC, Woolf BAR, Davies NM, Swanson SA, VanderWeele TJ, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomisation (STROBE-MR): explanation and elaboration. BMJ. 2021;375:n2233.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100.
Volkan B, Fettah A, İşlek A, Kara SS, Kurt N, Çayır A. Bone mineral density and vitamin K status in children with celiac disease: is there a relation? Turk J Gastroenterol. 2018;29(2):215–20.
Setty-Shah N, Maranda L, Nwosu BU. Increased risk for vitamin d deficiency in obese children with both celiac disease and type 1 diabetes. Gastroenterol Res Pract. 2014;2014:561351.
Villanueva J, Maranda L, Nwosu BU. Is vitamin D deficiency a feature of pediatric celiac disease? J Pediatr Endocrinol Metab. 2012;25(5–6):607–10.
Işıkay S, Işıkay N, Per H, Çarman KB, Kocamaz H. Restless leg syndrome in children with celiac disease. Turk J Pediatr. 2018;60(1):70–5.
Armagan O, Uz T, Tascioglu F, Colak O, Oner C, Akgun Y. Serological screening for celiac disease in premenopausal women with idiopathic osteoporosis. Clin Rheumatol. 2005;24(3):239–43.
Lerner A, Shapira Y, Agmon-Levin N, Pacht A, Ben-Ami Shor D, López HM, et al. The clinical significance of 25OH-Vitamin D status in celiac disease. Clin Rev Allergy Immunol. 2012;42(3):322–30.
Margoni D, Chouliaras G, Duscas G, Voskaki I, Voutsas N, Papadopoulou A, et al. Bone Health in Children with Celiac Disease assessed by dual X-ray absorptiometry: Effect of Gluten-free Diet and Predictive Value of serum biochemical indices. J Pediatr Gastroenterol Nutr. 2012;54(5):680–4.
Kavak US, Yuce A, Kogak N, Demir H, Saltik IN, Gurakan F, et al. Bone mineral density in children with untreated and treated celiac disease. J Pediatr Gastroenterol Nutr. 2003;37(4):434–6.
Zanchi C, Di Leo G, Ronfani L, Martelossi S, Not T, Ventura A. Bone metabolism in celiac disease. J Pediatr. 2008;153(2):262–5.
Nwosu BU, Maranda L. Vitamin D status and adiposity in Pediatric Malabsorption syndromes. Digestion. 2015;92(1):1–7.
Simmons KM, McFann K, Taki I, Liu E, Klingensmith GJ, Rewers MJ, et al. Reduced bone Mineral density is Associated with Celiac Disease autoimmunity in children with type 1 diabetes. J Pediatr. 2016;169:44–.
Bjorck S, Brundin C, Karlsson M, Agardh D. Reduced bone Mineral Density in Children with screening-detected Celiac Disease. J Pediatr Gastroenterol Nutr. 2017;65(5):526–32.
Ballestero Fernandez C, Varela-Moreiras G, Ubeda N, Alonso-Aperte E. Nutritional Status in Spanish Children and adolescents with Celiac Disease on a Gluten Free Diet compared to Non-celiac Disease controls. Nutrients, 2019. 11(10).
Pham-Short A, Donaghue KC, Ambler G, Briody J, Garnett S, Munns CF, et al. Abnormal cortical and trabecular bone in Youth with type 1 diabetes and Celiac Disease. Diabetes Care. 2019;42(8):1489–95.
Weintraub Y, Ben-Tov A, Dotan G, Yerushalmy-Feler A, Weiner D, Levy D, et al. Vitamin A levels are comparable between children with newly diagnosed coeliac disease and non-coeliac controls. Acta Paediatr. 2019;108(11):2095–9.
Bayrak NA, Volkan B, Haliloglu B, Kara SS, Cayir A. The effect of celiac disease and gluten-free diet on pubertal development: a two-center study. J Pediatr Endocrinol Metabolism. 2020;33(3):409–15.
Lionetti E, Galeazzi T, Dominijanni V, Acquaviva I, Catassi GN, Iasevoli M, et al. Lower level of plasma 25-Hydroxyvitamin D in children at diagnosis of Celiac Disease compared with healthy subjects: a case-control study. J Pediatr. 2021;228:132–e1371.
G A, Seth A, Kumar P, Jain A. Prevalence and management of vitamin D deficiency in children with newly diagnosed coeliac disease: cohort study. Paediatr Int Child Health. 2021;41(4):247–52.
Aydemir Y, Erdogan B, Türkeli A. Vitamin D deficiency negatively affects both the intestinal epithelial integrity and bone metabolism in children with celiac disease. Clin Res Hepatol Gastroenterol. 2021;45(4):101523.
Karpuz D, Tezol O, Senguel MT, Usta Y. Comparison of early atherosclerosis markers in children with celiac disease and their healthy peers. Cukurova Med J. 2022;47(4):1600–9.
Mager DR, Qiao J, Turner J. Vitamin D and K status influences bone mineral density and bone accrual in children and adolescents with celiac disease. Eur J Clin Nutr. 2012;66(4):488–95.
Drabinska N, Krupa-Kozak U, Abramowicz P, Jarocka-Cyrta E. Beneficial effect of oligofructose-enriched inulin on vitamin D and E status in children with Celiac Disease on a long-term gluten-free Diet: a preliminary Randomized, Placebo-controlled nutritional intervention study. Nutrients, 2018. 10(11).
Moya DA, Nugent CA, Baker RD, Baker SS. Celiac Disease Nutritional Status and poor adherence to follow-up. Clin Pediatr. 2020;59(7):649–55.
Verma A, Lata K, Khanna A, Singh R, Sachdeva A, Jindal P, et al. Study of effect of gluten-free diet on vitamin D levels and bone mineral density in celiac disease patients. J Family Med Prim Care. 2022;11(2):603–7.
Bodas A, Perez O, Martin P, Junguito A, Sanchez R, Blanco MV, et al. Iron, vitamins and minerals status in pediatric patients with celiac diseaseand non celiac gluten sensitivity prior to diagnosis and three months later. J Trace Elem Med Biology: Organ Soc Minerals Trace Elem (GMS). 2023;79:127237.
Fernandez CB, Varela-Moreiras G, Ubeda N, Alonso-Aperte E. Nutritional status in Spanish children and adolescents with celiac disease on a gluten free diet compared to non-celiac disease controls. Nutrients. 2019;11(10):2329–2329.
Akhshayaa G, Seth A, Kumar P, Jain A. Prevalence and management of vitamin D deficiency in children with newly diagnosed coeliac disease: cohort study. Paediatrics Int Child Health. 2021;41(4):247–52.
Sterne JA, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. 2000;53(11):1119–29.
Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J Clin Epidemiol. 2005;58(9):882–93.
Sterne JA, Sutton AJ, Ioannidis JP, Terrin N, Jones DR, Lau J, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343:d4002.
Canova C, Zabeo V, Pitter G, Romor P, Baldovin T, Zanotti R, et al. Association of maternal education, early infections, and antibiotic use with celiac disease: a population-based birth cohort study in northeastern Italy. Am J Epidemiol. 2014;180(1):76–85.
Stene LC, Honeyman MC, Hoffenberg EJ, Haas JE, Sokol RJ, Emery L, et al. Rotavirus infection frequency and risk of celiac disease autoimmunity in early childhood: a longitudinal study. Am J Gastroenterol. 2006;101(10):2333–40.
Mårild K, Ye W, Lebwohl B, Green PH, Blaser MJ, Card T, et al. Antibiotic exposure and the development of coeliac disease: a nationwide case-control study. BMC Gastroenterol. 2013;13:109.
Mårild K, Kahrs CR, Tapia G, Stene LC, Størdal K. Infections and risk of celiac disease in childhood: a prospective nationwide cohort study. Am J Gastroenterol. 2015;110(10):1475–84.
White JH. Vitamin D as an inducer of cathelicidin antimicrobial peptide expression: past, present and future. J Steroid Biochem Mol Biol. 2010;121(1–2):234–8.
Bandurska K, Berdowska A, Barczyńska-Felusiak R, Krupa P. Unique features of human cathelicidin LL-37. BioFactors. 2015;41(5):289–300.
Calvo MS, Whiting SJ. Overview of the proceedings from Experimental Biology 2004 symposium: vitamin D insufficiency: a significant risk factor in chronic diseases and potential disease-specific biomarkers of vitamin D sufficiency J Nutr, 2005. 135(2): p. 301-3.
Tripkovic L, Lambert H, Hart K, Smith CP, Bucca G, Penson S, et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysis. Am J Clin Nutr. 2012;95(6):1357–64.
van der Mei IA, Ponsonby AL, Engelsen O, Pasco JA, McGrath JJ, Eyles DW, et al. The high prevalence of vitamin D insufficiency across Australian populations is only partly explained by season and latitude. Environ Health Perspect. 2007;115(8):1132–9.
Pittaway JK, Ahuja KD, Beckett JM, Bird ML, Robertson IK, Ball MJ. Make vitamin D while the sun shines, take supplements when it doesn’t: a longitudinal, observational study of older adults in Tasmania, Australia. PLoS ONE. 2013;8(3):e59063.
Andersen R, Brot C, Jakobsen J, Mejborn H, Mølgaard C, Skovgaard LT, et al. Seasonal changes in vitamin D status among Danish adolescent girls and elderly women: the influence of sun exposure and vitamin D intake. Eur J Clin Nutr. 2013;67(3):270–4.
Pecora F, Persico F, Argentiero A, Neglia C, Esposito S. The role of micronutrients in support of the Immune response against viral infections. Nutrients, 2020. 12(10).
Unalp-Arida A, Ruhl CE, Choung RS, Brantner TL, Murray JA. Lower prevalence of Celiac Disease and Gluten-Related disorders in persons living in Southern vs Northern latitudes of the United States. Gastroenterology, 2017. 152(8): p. 1922–1932.e2.
Vici G, Camilletti D, Polzonetti V. Possible role of vitamin D in Celiac Disease Onset. Nutrients, 2020. 12(4).
Malaguarnera L. Vitamin D and microbiota: two sides of the same coin in the immunomodulatory aspects. Int Immunopharmacol. 2020;79:106112.
Dong S, Singh TP, Wei X, Yao H, Wang H. Protective effect of 1,25-Dihydroxy vitamin D3 on pepsin-trypsin-resistant Gliadin-Induced tight Junction injuries. Dig Dis Sci. 2018;63(1):92–104.
Andrén Aronsson C, Liu X, Norris JM, Uusitalo U, Butterworth MD, Koletzko S, et al. 25(OH)D levels in infancy is Associated with Celiac Disease Autoimmunity in At-Risk children: a case-control study. Front Nutr. 2021;8:720041.
O’Malley T, Heuberger R. Vitamin D status and supplementation in pediatric gastrointestinal disease. J Spec Pediatr Nurs. 2011;16(2):140–50.
Infantino C, Francavilla R, Vella A, Cenni S, Principi N, Strisciuglio C et al. Role of vitamin D in Celiac Disease and Inflammatory Bowel diseases. Nutrients, 2022. 14(23).
Rossi TM, Kumar V, Lerner A, Heitlinger LA, Tucker N, Fisher J. Relationship of endomysial antibodies to jejunal mucosal pathology: specificity towards both symptomatic and asymptomatic celiacs. J Pediatr Gastroenterol Nutr. 1988;7(6):858–63.
Imam MH, Ghazzawi Y, Murray JA, Absah I. Is it necessary to assess for fat-soluble vitamin deficiencies in pediatric patients with newly diagnosed celiac disease? J Pediatr Gastroenterol Nutr. 2014;59(2):225–8.
Shree T, Banerjee P, Senapati S. A meta-analysis suggests the association of reduced serum level of vitamin D and T-allele of Fok1 (rs2228570) polymorphism in the vitamin D receptor gene with celiac disease. Front Nutr. 2022;9:996450.
Lu C, Zhou W, He X, Zhou X, Yu C. Vitamin D status and vitamin D receptor genotypes in celiac disease: a meta-analysis. Crit Rev Food Sci Nutr. 2021;61(12):2098–106.
Gessaroli M, Frazzoni L, Sikandar U, Bronzetti G, Pession A, Zagari RM, et al. Nutrient intakes in adult and pediatric coeliac disease patients on gluten-free diet: a systematic review and meta-analysis. European Journal of Clinical Nutrition; 2023.
Alzaben AS, Turner J, Shirton L, Samuel TM, Persad R, Mager D. Assessing Nutritional Quality and Adherence to the gluten-free Diet in Children and adolescents with Celiac Disease. Can J Diet Pract Res. 2015;76(2):56–63.
Acknowledgements
Not applicable.
Funding
This work was supported by grants from the Public Welfare Technology Application Research Program of Zhejiang Province, China (LGF21H190001).
Author information
Authors and Affiliations
Contributions
YS designed research; YS and QZ searched articles and collected data; DT and JZ evaluated the disagreement; YS and SD performed the statistical analysis; YS wrote the paper; SD revised the paper. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sun, Y., Zhou, Q., Tian, D. et al. Relationship between vitamin D levels and pediatric celiac disease: a systematic review and meta-analysis. BMC Pediatr 24, 185 (2024). https://doi.org/10.1186/s12887-024-04688-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-024-04688-0