
Abstract
Background
The dysfunction of optic nerve head (ONH) hemodynamics has been suggested to be involved in the pathogenesis of normal-tension glaucoma (NTG). The aim of this study was to compare vasoreactivity in the ONH, nailfold, and facial skin in response to cold-water provocation in NTG patients and healthy controls.
Methods
We performed cold-water provocation in 14 eyes of 14 NTG patients and 15 eyes of 15 age-matched control subjects. Laser speckle flowgraphy-derived tissue-area mean blur rate (MT), skin blood flowmetry-derived pulse wave amplitude (PA), nailfold capillaroscopy-derived nailfold capillary diameter, and other clinical parameters were recorded at baseline and 4 and 6 min after the cold stimulus. We compared changes (as percentages) in these variables in the NTG and control subjects with a linear mixed-effects model and evaluated correlations between these changes with Spearman’s rank correlation coefficient.
Results
The interaction term between the NTG group (reference, control group) and the 4-min protocol step (reference, baseline) significantly affected the changes in MT, nailfold capillary diameter and PA (β = -9.51%, P = 0.017, β = -20.32%, P = 0.002; β = + 18.06%, P = 0.017, respectively). The change in MT was positively correlated with the change in nailfold capillary diameter, and negatively correlated with the change in PA (r = 0.39, P = 0.036; r = -0.40, P = 0.031, respectively).
Conclusion
NTG patients showed abnormal vasoconstriction in the ONH and nailfold and vasodilation in the facial skin in response to cold-water provocation.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Glaucoma, the second most common cause of blindness worldwide [1, 2], is characterized by progressive retinal ganglion cell death and associated visual field loss [3]. High intraocular pressure (IOP) is the only modifiable risk factor for primary open-angle glaucoma, but the existence of normal-tension glaucoma (NTG) indicates that high IOP is not the only risk factor for glaucoma development or progression. One suspected non-IOP risk factor is chronic blood flow (BF) impairment in the optic nerve head (ONH), which may be associated with abnormal vasoreactivity in response to external stimuli (e.g., the vasospastic response to cold stimulus) [4, 5].
Cold provocation testing (CPT) has been used to evaluate the role of vascular dysregulation in glaucoma in several studies. This technique elicits vasoconstriction by activating the sympathetic autonomic nervous system [6,7,8]. Most previous studies have combined CPT with nailfold capillaroscopy and reported excessive nailfold capillary constriction during testing in glaucoma patients [9,10,11]. The popularity of these methods may be due to the ease of access to the nailfold and suggestions that there is a relationship between systemic abnormal vasoreactivity, such as Raynaud’s phenomenon, and NTG [12, 13]. In addition, excessive constriction of nailfold capillaries following CPT has been found to be associated with faster visual-field defect progression in primary open-angle glaucoma patients [14]. This suggests that there may be a clinically significant relationship between BF in the nailfold capillaries and the eye. Nevertheless, there have been few reports in the field of ophthalmology that have investigated the vasospastic response of glaucoma patients in the retina, the rim of the ONH, and the retrobulbar region during CPT [15,16,17]. Thus, there is an unfortunate lack of data on the vasoreactive response to cold provocation in the deep areas of the ONH, which is believed to be the primary site of glaucomatous lesions. Against this background, we chose to use laser speckle flowgraphy (LSFG), an easy and reproducible method of measuring BF in the deep area of the ONH [18, 19], in addition to a nailfold capillaroscopy device [20, 21].
We also went a step further and examined facial skin BF dynamics, using a skin blood flowmetry device, because the vascular response to cold provocation (i.e., sympathetic stimulation) may be different in this region [22] and because the face is even more accessible than the nailfold or deep areas of the ONH. Unfortunately, we lack multimodal imaging data obtained during CPT. In fact, it remains unclear which area in the body is most suited for detecting abnormal vasoreactivity in NTG patients and which device would be most suitable for obtaining such data. Precise and reproducible measurements of regional differences in the response of the vasculature to CPT may lead to further understanding of the vascular component in glaucoma pathogenesis and the association with clinical findings. Thus, this study sought to establish a CPT protocol and compare vasoreactivity in NTG and healthy controls during CPT in the deep ONH, nailfold, and facial skin with recently developed imaging devices, including LSFG, nailfold capillaroscopy, and skin blood flowmetry, respectively.
Materials and methods
Subjects
This prospective study comprised 14 eyes of 14 NTG patients and 15 eyes of 15 control subjects who visited the Seiryo Eye Clinic, located in Miyagi, Japan, between August and November 2021. Informed consent was obtained from the subjects before the CPT was performed. This study followed the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Tohoku University School of Medicine (protocol number 2021–1-434). When both eyes satisfied the inclusion criteria, the left eye was selected for the analysis. NTG was diagnosed by a glaucoma specialist (N.T.).
The inclusion criteria for both groups were (1) age between 30 and 75 years, (2) cataract grade less than or equal to 2 on the Emery-Little classification [23], and (3) IOP ≤ 21 mmHg. An additional inclusion criterion for the control group was normal findings in slit-lamp, fundoscopy, and optical coherence tomography examinations. Additional inclusion criteria for the NTG group were (1) the presence of glaucomatous optic disc changes with corresponding visual field (VF) defects matching the Anderson-Patella criteria [24], (2) abnormally reduced circumpapillary retinal nerve fiber layer thickness (cpRNFLT), (3) a normal, open angle in a gonioscopic examination, and (4) mean deviation (MD) > -12 dB.
Subjects were excluded if they (1) had a history of ocular or systemic disease causing optic nerve damage, (2) had high myopia (axial length [AL] > 26.5 mm or spherical equivalent < -8 diopters), (3) had a history of intraocular surgery, (4) had a history of smoking within the previous 4 years, (5) were pregnant, or (6) had a history of discomfort during any kind of cold provocation. All subjects abstained from alcohol and caffeine for at least 6 h before the cold-water provocation.
Measurement of baseline clinical characteristics
Baseline clinical variables were measured before the CPT. Logarithmic minimum angle of resolution (logMAR) was used to represent best-corrected visual acuity (BCVA). IOP was measured with Goldmann applanation tonometry, AL was measured with the OA-2000 (Tomey Corporation, Aichi, Japan), cpRNFLT was measured with swept-source optical coherence tomography (DRI OCT; Triton, Topcon, Inc., Tokyo, Japan), and the VF was measured with the 24–2 program of the Humphrey Field Analyzer (Carl Zeiss Meditec, Dublin, CA, USA). Reliable results were obtained from all NTG subjects in VF testing (fixation errors < 20%, false positives < 33%, and false negatives < 33%) and OCT examinations (signal strength > 60). Blood pressure (BP) and pulse rate (PR) were conventionally measured in the brachial artery at the height of the heart (HBP-1300; Omron Colin Co., Ltd., Tokyo, Japan). Pupil dilation was performed with 0.4% tropicamide (Mydrin M; Santen Pharmaceutical Co., Ltd., Osaka, Japan). Mean blood pressure (MBP) and mean ocular perfusion pressure (MOPP) were calculated as follows: MBP = diastolic blood pressure (DBP) + 1/3 (systolic blood pressure [SBP]—DBP); MOPP = 2/3 MBP – IOP.
LSFG measurements and nailfold capillary imaging
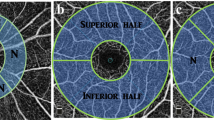
ONH BF was measured with LSFG. The principles of LSFG have previously been described in detail [25]. Briefly, this device measures the pattern of speckle contrast produced by the interference of a laser scattered by blood cells moving in the blood vessels. This study used the LSFG-NAVI device (Softcare Co., Ltd., Fukutsu, Japan). Mean blur rate (MBR), which is known to represent BF velocity, is the main LSFG variable and is expressed in arbitrary units. MBR images of the fundus are acquired continuously at the rate of 30 frames per second over a 4-s period and then averaged to produce a composite map of ocular BF. The accompanying analysis software can automatically divide the MBR map into the large vessel and tissue (capillary) areas of the ONH and determine specific values for each. The focus of this study was on tissue-area MBR (MT), because MT has been reported to represent BF in the deeper regions of the ONH [18, 19].
Nailfold capillaries were observed under a light microscope (Kekkan-Bijin; At Co., Ltd., Osaka, Japan) after application of mineral oil to reduce light reflection, as previously described [20, 21]. The observations were performed at the fourth finger of the left hand [26,27,28]. Capillary images were captured using the Capillary Analysis System (At Co., Ltd.). The images of the nailfold capillaries were numerically analyzed for their average length and diameter [20, 29].
Casio blood flowmetry, a novel method of measuring skin BF
Facial skin BF was measured with a skin blood flowmeter (Casio Computer Co., Ltd., Tokyo, Japan). This measurement is completed by simply placing the camera on the measurement site (in this study, the skin of the left cheek) for 30 s. Luminance data can be acquired from the image sensor 30 times per second. The principle of operation of this blood flowmeter is to measure skin BF via pulse wave extraction from the captured images, represented by pulse wave amplitude (PA). Hemoglobin in skin capillaries absorbs green light, and the luminance of the green component of light reflected by the skin thus changes with flux and reflux of skin blood perfusion. By capturing changes in the luminance of the minute green component of this signal with an image sensor, time-series data for luminance can be extracted.
As the skin blood flowmeter is a novel device for measuring skin BF, we first confirmed its reproducibility in this study. For this, we independently enrolled 12 healthy volunteers (45.6 ± 11.0 years, male to female ratio = 6:6). All subjects abstained from alcohol and caffeine for at least 6 h before the measurements. As shown in Supplementary Figure S1, at an initial visit, two sets of skin blood flowmeter measurements were obtained consecutively, at 10:00 a.m. (sets 1 and 2). At a second visit (between 1 to 7 days later), skin blood flowmeter measurements were again obtained at 10:00 a.m. (set 3), the examiner was changed, and a final measurement was obtained (set 4). The volunteers took 5-min rests between set 1 and set 2 and between set 3 and set 4. The coefficient of variation (CV) for the PA values was calculated to investigate the intrasession reproducibility (for sets 1 and 2), intersession reproducibility (for sets 1 and 3), and interexaminer reproducibility (for sets 3 and 4), following a method in a previous report [30]. We also checked whether skin blood flowmeter-derived PA correlated with laser speckle perfusion imager-derived BF, which has previously been used as a parameter to measure BF [31,32,33,34] in the same facial skin region.
Cold-water provocation test
The cold-water provocation test was performed as previously described [15, 16], between 1:00 and 5:00 p.m. in a dark, quiet room. The room temperature was kept at 20 °C. We prepared warm water at 40 °C and cold water at 4 °C. The cold provocation testing comprised 5 steps: baseline, warm water application, cold water application, 4-min post-cold immersion measurements, and 6-min post-cold immersion measurements. LSFG-derived parameters, BP, PR, skin blood flowmetry-derived PA, nailfold capillary diameter, and IOP were measured at baseline, 4 min, and 6 min. After the baseline examination, the subjects immersed their right hands into the warm water for 2 min, and then immediately immersed the same hand into the cold water for 1 min. The percentage changes in MT, PA, and nailfold capillary diameter versus baseline were calculated as follows:
% Change in X (t) = (X (t)—X (baseline)) / X (baseline).
(X = MT, PA, nailfold capillary diameter; t = baseline, 4 min, or 6 min).
X (t) indicates the value of MT, PA, or nailfold capillary diameter at each protocol step. Figure 1 shows representative images and the protocol schema. It was possible to complete each measurement, including MT, PA, nailfold capillary diameter, IOP, and BP/PR, within 30 s. Some measurements, such as BP, can be done concurrently with other tests. Thus, with efficient use of time and technique by the three experienced examiners, it was generally possible to complete a single time-point test in less than a minute. There were no instances where the test duration exceeded two minutes and overlapped with the next measurement time point. The protocol steps at which each parameter reached its peak (Fig. 2), calculated as the percentage changes in MT, nailfold capillary diameter, and PA, occurred at the 4,4,6-min protocol steps, respectively.

A Representative photographs of our testing protocol. From left to right: photographs of a subject immersing his right hand into 40 °C warm water and 4 °C cold water and undergoing LSFG measurement. B Testing protocol with five steps: baseline, warm water (2 min), cold water (1 min), and 4 min and 6 min after the cold-water immersion. During the test, LSFG measurements, BP, PR, skin pulse wave amplitude, nailfold capillaroscopy diameter, and IOP were recorded. The black circles represent measurement time points. Baseline LSFG measurements were repeated three times and averaged

Differences in the vascular response to cold-water provocation. The x-axis shows the protocol steps, and the y-axis shows the percentage change in the indicated parameters. Black circles with straight lines indicate variables from the NTG group and white circles with dotted lines indicate variables from the control group. The asterisks indicate the statistical significance of the interaction term between the indicated group and protocol step (linear mixed-effects model, *P < 0.05, **P < 0.01)
Statistical analysis
All data are shown as the mean ± standard deviation. Wilcoxon’s rank-sum test or Fisher’s exact test were used for group comparisons (i.e., control vs. NTG group). Multiple name-logistic regression analysis was used for group comparisons adjusting for potential confounding factors. An analysis of variance of linear mixed-effects model was used to see whether there was any change in BP, PR, IOP, or MOPP during the provocation testing, setting the “subject variable” as a random effect. A linear mixed-effects model was used to determine the statistical difference in percentage changes in MT, PA, and nailfold capillary diameter, setting the interaction term between “protocol step” (reference, baseline) and “group” (reference, control group) as fixed effects and setting the “subject variable” as a random effect. Spearman’s rank correlation coefficient was used to determine the correlation between the percentage change in MT and percentage change in nailfold capillary diameter or percentage change in PA, and between PA and laser speckle perfusion imager-derived BF parameters. We calculated the CV for PA to confirm its intrasession reproducibility, intersession reproducibility, and interexaminer reliability. All statistical analyses were performed with R software (version 3.2.5). The significance level was set at P < 0.05.
Results
Reproducibility of skin blood flowmetry-derived PA
Intrasession reproducibility, intersession reproducibility, and interexaminer reliability for PA were relatively high: the CV values were 7.3% ± 6.5%, 12.5% ± 7.0%, and 6.5% ± 4.8%, respectively. PA and laser speckle perfusion imager-derived BF showed a statistically significant correlation (r = 0.49, P = 0.007).
Comparison of clinical characteristics between groups
As shown in Table 1, lower cpRNFLT, lower MD, shorter nailfold capillary length, and thinner nailfold capillary diameter were observed in the NTG group (105.2 ± 13.7 vs. 75.3 ± 14.2, P < 0.001; -0.8 ± 1.2 vs. -3.0 ± 2.5, P = 0.003; 977.8 ± 265.4 vs. 592.9 ± 374.4, P = 0.004; and 29.0 ± 7.0 vs. 23.5 ± 5.1, P = 0.036, respectively). Other variables did not reach statistical significance (P = 0.087 – 0.930). Because of the multicollinearity between nailfold capillary length and nailfold capillary diameter, we created two multiple name-logistic regression models in which IOP, age, gender, and nailfold capillary diameter or nailfold capillary length were included as explanatory variables and the “group” variable (reference, control group) as the response variable. In model 1, nailfold capillary length was significantly shorter in the NTG group (0.992 [0.987—0.998], P = 0.009). In model 2, thinner nailfold capillary diameter was associated with the NTG group (0.754 [0.595—0.956], P = 0.020).
Changes in systemic variables during the CPT
No adverse events were observed during the provocation. As shown in Table 2, IOP increased during the CPT in the control group (P = 0.007); however, no systemic variables, including SBP, DBP, PR, MBP, and MOPP, changed significantly in either group (P = 0.086 – 0. 880).
Differences in the vascular response to cold provocation
As shown in Fig. 2, there was a statistically significant interaction term between the NTG group (reference, control group) and the 4-min protocol step (reference, baseline) against the percentage in change in MT (β = -9.51%, P = 0.017). There was a statistically significant interaction term between NTG group and the 4-min protocol step against percentage change in nailfold capillary diameter (β = -20.32%, P = 0.002). There were statistically significant interaction terms between the NTG group and the 4-min protocol step and the NTG group and 6-min protocol step against percentage change in PA (β = + 18.06%, P = 0.017; β = + 17.72%, P = 0.018, respectively).
Relationship among vasoreactivity parameters
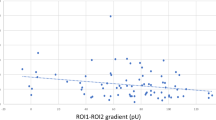
As shown in Fig. 3, the percentage change in MT was significantly positively correlated with the percentage change in nailfold capillary diameter (r = 0.39, P = 0.036) and negatively with the percentage change in PA (r = -0.40, P = 0.031) in the overall subjects.

The relationship between percentage change in MT and percentage change in PA or nailfold capillary diameter. The percentage change in MT was significantly correlated with the percentage changes in nailfold capillary diameter and in PA in the overall subjects (r = 0.39, P = 0.036; r = -0.40, P = 0.031, respectively)
Comparative visualization of healthy subject and NTG patient: LSFG images, nailfold capillary diameter and skin pulse wave alterations
Representative LSFG images, nailfold capillary diameter images, and graphs depicting skin pulse wave alterations during the protocol are presented in Fig. 4. The upper panels display a healthy subject with mild changes in MT, nailfold capillary diameter, and skin pulse wave alterations, while the lower panels exhibit an NTG patient with pronounced changes in these parameters.

Representative LSFG images, nailfold capillary diameter images, and graphs showing skin pulse wave alteration during the protocol. A-F The upper panels show a healthy subject with mild changes in MT, nailfold capillary diameter, and skin pulse wave alteration. G-L The lower panels show an NTG patient with excessive changes in these parameters. A, C, E, G, I, and K show representative baseline images; other images are after CPT. For better visualization of the representative images, we increased brightness by 9% and contrast by 50% for C, D, I, and J using PowerPoint (Ver. 2304, Microsoft Corporation, Redmond, WA, USA)
Discussion
In this study, we attempted to determine whether NTG patients had impaired vasoreactivity in response to cold stimulus, both systemically and locally in the eye. To do so, we established a CPT protocol combined with multimodal imaging that included LSFG, nailfold capillaroscopy, and skin blood flowmetry. We found different vasoreactive responses to cold provocation: there was a greater decrease in ONH-tissue BF and nailfold capillary diameter in NTG patients 4 min after the cold provocation and there was a greater increase in facial skin BF in NTG patients both 4 min and 6 min after the provocation. Additionally, we investigated the relationship between the percentage change in MT and the percentage changes in PA and nailfold capillary diameter. We found that the percentage change in MT was positively correlated with the percentage change in nailfold capillary diameter, but negatively correlated with the percentage change in PA. These results suggest that NTG patients might have abnormal vasoreactivity (i.e., they might have excessive vasoconstriction in the eye or nailfold and excessive vasodilation in the facial skin) in response to cold stimulus (i.e., sympathetic activation might occur).
We reconfirmed that there were nailfold capillary abnormalities in NTG patients at baseline. It has long been suggested that systemic vascular dysregulation may be involved in the pathophysiology of NTG [4, 35]. The nailfold capillaries have been the subject of research interest since the 1970s, possibly because of their easy accessibility and involvement in Raynaud’s phenomenon [36]. Although our study used different instruments and measured different parameters that were used in previous research, our finding that the nailfold capillaries were thinner and shorter in NTG patients is consistent with previous reports that nailfold capillary abnormalities were present in glaucoma patients [9, 37,38,39], indicating that we recruited a population of NTG patients with systemic vascular dysregulation.
During our CPT protocol, MOPP did not change in either the control or NTG groups, though IOP increased significantly in the control group. Considering that cold stress is considered to be a test of sympathetic nerve stimulation [22, 40, 41], which is thought to increase IOP [42], this result may be comprehensible. We also observed stable MOPP in the control subjects during CPT, despite incremental increases in IOP, which might have been due to sympathetic nerve activation and the tendency of BP to increase, though this effect did not reach statistical significance. The finding that IOP did not increase in the NTG group may be due to the possible effects of anti-glaucoma eye drops affecting the sympathetic pathway. Further investigation is needed to clarify this point. There is no consensus on how BP or IOP change during CPT, probably because past studies have used different CPT protocols, because of variations in BP response among individuals [43], and also because these measurements depend on the timing of the BP measurement. Kashima et al. reported that BP rose after 2 min, but then returned to baseline levels within 1 min [22]. In our protocol, the hemodynamics changes we observed in the ONH, nailfold, and facial skin were unlikely to have been due to changes in vital signs during and after the provocation, as there were no statistically significant changes in BP or MOPP.
In this study, the vascular responses of the ONH tissue and nailfold resembled each other, i.e., the capillaries in both these areas excessively contracted in NTG patients in response to CPT when compared with the control subjects. Previously, it was reported that CPT and nailfold capillaroscopy can be used to detect Raynaud’s phenomenon, which might be associated with NTG [12, 13, 36]. Our results support the idea that abnormal vasoreactivity in different body regions could be involved in the pathogenesis of NTG. Several reports have failed to show excessive contraction of the retinal or ophthalmic arteries [15, 17], while on the other hand, Gherghel et al. found that glaucoma patients showed a vasospastic response during CPT in the temporal ONH rim area [16]. Taken together with our results, the explanation for this discrepancy might be that capillaries originating from the short posterior ciliary artery can be affected by sympathetic excitation, because these arteries are innervated by autonomic nerves, while such innervation is absent or lacking in the retinal artery. Further investigation is needed to clarify this point in the future.
It is interesting to note that while the capillary hemodynamics of the ONH and nailfold were similar, facial skin BF showed opposite hemodynamics. In patients with Horner’s syndrome, the cheek on the side with sympathetic denervation shows diminished sweating and flushing [44]. Kashima et al. showed that facial skin BF increased in healthy subjects during CPT [22]. This suggests that the vasculature under the facial skin is innervated by the autonomic nervous system and dilates with sympathetic stimulation. The absence of such a response in the control subjects in this study may have been due to a shorter cold stimulus than that used by Kashima et al. (1 min vs. 2 min). Nevertheless, in the same condition, we found a stronger vasodilatory response in the NTG group. Regardless of whether sympathetic stimulation induces vasoconstriction or vasodilation in different body regions, we found excessive vasoreactivity in all of three regions in the NTG patients in this study. Furthermore, although ONH and nailfold observations are relatively easy to make, facial skin BF observations are even easier, in our experience. Thus, in the future, it might be possible to detect subjects with dysfunctional vasoregulation, and even glaucoma patients, simply by examining the facial skin BF reaction to CPT.
There are several limitations to this study. The most significant limitation is the small sample size, which was necessary for ethical reasons due to the burdensome nature of provocation testing. We chose the number of subjects by referring to previous studies that have used provocation testing; these studies generally included approximately 15 subjects per group [45,46,47]. The results in this study should be interpreted with great caution until we can verify them in a study with a larger sample size in the future. A second limitation is the potential bias arising from our study population. The subjects recruited in this study were not selected based on the presence of vasospastic abnormalities (e.g., having a history of cold hands), but the majority of open-angle glaucoma patients in Japan have normal-range IOP [48], meaning that they are more likely to have vascular abnormalities than the general population or high-tension glaucoma patients. In addition, it should be noted that we recruited only NTG patients with relatively mild visual field defects. This decision was made because if the patients had more severe glaucoma, the vessels might have been more atherosclerotic or even subject to drop-out [49,50,51], and we could not expect to clearly observe hyper-vasoreactivity. For this reason, we do not think that our results are generalizable to the overall population of patients with glaucoma. Third, we could not ask the NTG patients to discontinue the use of anti-glaucoma eye drops, again due to ethical considerations, so the differing vasoreactivity between the NTG and control groups might have been due to the effect of the eye drops. Indeed, only the glaucoma group received anti-glaucoma eye drops, so the difference in vasoreactivity might have been due to the presence or absence of eye drops. However, even when we divided the glaucoma group based on the use (n = 7) or non-use of β-blockers (n = 7), we did not observe a difference in percentage change in MT, nailfold capillary diameter, or PA (P = 0.443, P = 0.609, P > 0.999, respectively; Wilcoxon’s test). Thus, we still believe that the abnormality in vasoreactivity observed in the glaucoma patients was due to the presence or absence of glaucoma. In addition, since hyper-vasoreactivity was not only observed in the ONH but also in the nailfold and facial skin, we do not consider that the use of eye drops was a main cause. Furthermore, it is important to consider the potential influence of systemic vascular complications, such as diabetes mellitus. Thus, we added a history of diabetes mellitus (yes: 1; no: 0) and β-blocker use (yes: 1; no: 0) as explanatory variables in the linear mixed-effects models shown in Fig. 2 and confirmed that the results did not change. The results were as follows: the interaction term between the NTG group (reference, control group) and the 4-min protocol step (reference, baseline) significantly affected the changes in MT, nailfold capillary diameter, and PA (β = -9.51%, P = 0.017; β = -20.32%, P = 0.002; β = + 18.08%, P = 0.017, respectively). Taken together, we believe that the difference in vasoreactivity in different body regions is mainly associated with the presence of glaucoma. Fourth, it is unclear at what depth the blood flowmetry device measures BF in each area. This uncertainty might affect our conclusions, because autonomic nerve innervation might differ at different depths of the tissue. Further investigation is needed to clarify these points in the future with multi-center studies with large sample sizes. The fifth limitation is that we analyzed the correlation of vasoreactivity in different body regions in data from a combined group of controls and glaucoma patients. In this study, we observed abnormal vasoreactivity in glaucoma patients that was not present in controls. In this case, if we separated the two groups for analysis, the values for vasoreactivity might cluster into normal and abnormal categories. Particularly with a small sample size, this could artificially result in a conclusion that there was no correlation in regional vascular reactivity. We believe that the crucial point is the reversal phenomenon, whereby despite the influence of the presence or absence of glaucoma, vasoreactivity showed a positive correlation in some regions (e.g., the ONH vs. the nailfold capillaries) and negative in others (e.g., the ONH vs. the facial skin). Therefore, we consider it worthwhile to present the analysis of the overall data. Nevertheless, we also consider that we might find weak correlations within each group if we had a larger sample size; we are eager to perform such an investigation in the future.
In conclusion, we found that a subgroup of NTG patients showed excessive vasoconstriction in the ONH tissue and nailfold capillaries and excessive vasodilation under the facial skin in response to cold-water provocation; this dysfunctional vasoregulation was revealed by a combination of CPT and simultaneous multimodal imaging analysis of the optic nerve head, nailfold, and facial skin BF.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AL:
-
Axial length
- BCVA:
-
Best-corrected visual acuity
- BF:
-
Blood flow
- BP:
-
Blood pressure
- cpRNFLT:
-
Circumpapillary retinal nerve fiber layer thickness
- CPT:
-
Cold provocation testing
- CV:
-
Coefficient of variation
- DBP:
-
Diastolic blood pressure
- IOP:
-
Intraocular pressure
- logMAR:
-
Logarithmic minimum angle of resolution
- LSFG:
-
Laser speckle flowgraphy
- MBP:
-
Mean blood pressure
- MBR:
-
Mean blur rate
- MD:
-
Mean deviation
- MOPP:
-
Mean ocular perfusion pressure
- MT:
-
Tissue-area mean blur rate
- NTG:
-
Normal-tension glaucoma
- OCT:
-
Optical coherence tomography
- ONH:
-
Optic nerve head
- PA:
-
Pulse wave amplitude
- PR:
-
Pulse rate
- SBP:
-
Systolic blood pressure
- VF:
-
Visual field
References
Leske MC. Open-angle glaucoma – an epidemiologic overview. Ophthalmic Epidemiol. 2007;14(4):166–72.
Kingman S. Glaucoma is second leading cause of blindness globally. Bull World Health Organ. 2004;82(11):887–8.
Jonas JB, Aung T, Bourne RR, Bron AM, Ritch R, Panda-Jonas S. Glaucoma. Lancet. 2017;390(10108):2183–93.
Flammer J, Konieczka K, Flammer AJ. The primary vascular dysregulation syndrome: implications for eye diseases. EPMA J. 2013;4(1):14.
Kiyota N, Shiga Y, Yasuda M, Aizawa N, Omodaka K, Tsuda S, Pak K, Kunikata H, Nakazawa T. The optic nerve head vasoreactive response to systemic hyperoxia and visual field defect progression in open-angle glaucoma, a pilot study. Acta Ophthalmol. 2020;98(6):e747–53.
Flavahan NA. A vascular mechanistic approach to understanding Raynaud phenomenon. Nat Rev Rheumatol. 2015;11(3):146–58.
Kurysheva NI, Ryabova TY, Shlapak VN. Heart rate variability: the comparison between high tension and normal tension glaucoma. Epma j. 2018;9(1):35–45.
Victor RG, Leimbach WN Jr, Seals DR, Wallin BG, Mark AL. Effects of the cold pressor test on muscle sympathetic nerve activity in humans. Hypertension. 1987;9(5):429–36.
Gasser P, Flammer J. Blood-cell velocity in the nailfold capillaries of patients with normal-tension and high-tension glaucoma. Am J Ophthalmol. 1991;111(5):585–8.
Drance SM, Douglas GR, Wijsman K, Schulzer M, Britton RJ. Response of blood flow to warm and cold in normal and low-tension glaucoma patients. Am J Ophthalmol. 1988;105(1):35–9.
Usui T, Iwata K. Finger blood flow in patients with low tension glaucoma and primary open-angle glaucoma. Br J Ophthalmol. 1992;76(1):2–4.
Nicolela MT, Ferrier SN, Morrison CA, Archibald ML, LeVatte TL, Wallace K, Chauhan BC, LeBlanc RP. Effects of cold-induced vasospasm in glaucoma: the role of endothelin-1. Invest Ophthalmol Vis Sci. 2003;44(6):2565–72.
Alizadeh R, Vickers L, Hirunpatravong P, Romero P, Lin MC, Sharifipour F, Caprioli J. A phenotype of primary open-angle glaucoma with systemic vasospasm. J Glaucoma. 2018;27(11):987–92.
Guthauser U, Flammer J, Mahler F. The relationship between digital and ocular vasospasm. Graefes Arch Clin Exp Ophthalmol. 1988;226(3):224–6.
Chou WY, Liu CJ, Chen MJ, Chiou SH, Chen WT, Ko YC. Effect of cold provocation on vessel density in eyes with primary open angle glaucoma: An optical coherence tomography angiography study. Sci Rep. 2019;9(1):9384.
Gherghel D, Hosking SL, Cunliffe IA. Abnormal systemic and ocular vascular response to temperature provocation in primary open-angle glaucoma patients: a case for autonomic failure? Invest Ophthalmol Vis Sci. 2004;45(10):3546–54.
Rojanapongpun P, Drance SM. The response of blood flow velocity in the ophthalmic artery and blood flow of the finger to warm and cold stimuli in glaucomatous patients. Graefes Arch Clin Exp Ophthalmol. 1993;231(7):375–7.
Aizawa N, Nitta F, Kunikata H, Sugiyama T, Ikeda T, Araie M, Nakazawa T. Laser speckle and hydrogen gas clearance measurements of optic nerve circulation in albino and pigmented rabbits with or without optic disc atrophy. Invest Ophthalmol Vis Sci. 2014;55(12):7991–6.
Wang L, Cull GA, Piper C, Burgoyne CF, Fortune B. Anterior and posterior optic nerve head blood flow in nonhuman primate experimental glaucoma model measured by laser speckle imaging technique and microsphere method. Invest Ophthalmol Vis Sci. 2012;53(13):8303–9.
Nakajima T, Nakano S, Kikuchi A, Matsunaga YT. Nailfold capillary patterns correlate with age, gender, lifestyle habits, and fingertip temperature. PLoS ONE. 2022;17(6): e0269661.
Kamata Y, Iwamoto M, Muroi K, Minota S. Repeated local implantation of autologous peripheral blood mononuclear cells for the treatment of ischaemic digits in patients with connective tissue diseases. Rheumatology (Oxford). 2011;50(5):906–10.
Kashima H, Ikemura T, Hayashi N. Regional differences in facial skin blood flow responses to the cold pressor and static handgrip tests. Eur J Appl Physiol. 2013;113(4):1035–41.
Emery JM, Little JH. Phacoemulsification and aspiration of cataracts: surgical techniques, complications, and results. Mosby; 1979.
Anderson DR, Patella VM. Automated static perimetry. 2nd ed. Mosby; 1999.
Draijer M, Hondebrink E, van Leeuwen T, Steenbergen W. Review of laser speckle contrast techniques for visualizing tissue perfusion. Lasers Med Sci. 2009;24(4):639–51.
Cutolo M, Grassi W, Matucci Cerinic M. Raynaud’s phenomenon and the role of capillaroscopy. Arthritis Rheum. 2003;48(11):3023–30.
Lambova S, Hermann W, Müller-Ladner U. Capillaroscopic pattern at the toes of systemic sclerosis patients: does it “tell” more than those of fingers? J Clin Rheumatol. 2011;17(6):311–4.
Philip S, Najafi A, Tantraworasin A, Pasquale LR, Ritch R. Nailfold capillaroscopy of resting peripheral blood flow in exfoliation glaucoma and primary open-angle glaucoma. JAMA Ophthalmol. 2019;137(6):618–25.
Etehad Tavakol M, Fatemi A, Karbalaie A, Emrani Z, Erlandsson BE. Nailfold capillaroscopy in rheumatic diseases: which parameters should be evaluated? Biomed Res Int. 2015;2015: 974530.
Kiyota N, Shiga Y, Ichinohasama K, Yasuda M, Aizawa N, Omodaka K, Honda N, Kunikata H, Nakazawa T. The impact of intraocular pressure elevation on optic nerve head and choroidal blood flow. Invest Ophthalmol Vis Sci. 2018;59(8):3488–96.
Briers JD. Laser Doppler and time-varying speckle: a reconciliation. J Opt Soc Am A-Opt Image Sci Vis. 1996;13:345–50.
Forrester KR, Stewart C, Tulip J, Leonard C, Bray RC. Comparison of laser speckle and laser Doppler perfusion imaging: measurement in human skin and rabbit articular tissue. Med Biol Eng Comput. 2002;40(6):687–97.
Kashima S. Spectroscopic measurement of blood volume and its oxygenation in a small volume of tissue using red laser lights and differential calculation between two point detections. Opt Laser Technol. 2003;35(6):485–9.
Forrester KR, Tulip J, Leonard C, Stewart C, Bray RC. A laser speckle imaging technique for measuring tissue perfusion. IEEE Trans Biomed Eng. 2004;51(11):2074–84.
Flammer J, Haefliger IO, Orgül S, Resink T. Vascular dysregulation: a principal risk factor for glaucomatous damage? J Glaucoma. 1999;8(3):212–9.
Maricq HR, Downey JA, LeRoy EC. Standstill of nailfold capillary blood flow during cooling in scleroderma and Raynaud’s syndrome. Blood Vessels. 1976;13(6):338–49.
Shoji MK, Cousins CC, Saini C, Nascimento ESR, Wang M, Brauner SC, Greenstein SH, Pasquale LR, Shen LQ. Paired optic nerve microvasculature and nailfold capillary measurements in primary open-angle glaucoma. Transl Vis Sci Technol. 2021;10(7):13.
Rong X, Cai Y, Li M, Chen X, Kang L, Yang L. Relationship between nailfold capillary morphology and retinal thickness and retinal vessel density in primary open-angle and angle-closure glaucoma. Acta Ophthalmol. 2020;98(7):e882–7.
Pasquale LR, Hanyuda A, Ren A, Giovingo M, Greenstein SH, Cousins C, Patrianakos T, Tanna AP, Wanderling C, Norkett W, et al. Nailfold capillary abnormalities in primary open-angle glaucoma: a multisite study. Invest Ophthalmol Vis Sci. 2015;56(12):7021–8.
Freeman R. Assessment of cardiovascular autonomic function. Clin Neurophysiol. 2006;117(4):716–30.
Velasco M, Gómez J, Blanco M, Rodriguez I. The cold pressor test: pharmacological and therapeutic aspects. Am J Ther. 1997;4(1):34–8.
Feibel RM. Sympathectomy for glaucoma: Its rise and fall (1898–1910). Surv Ophthalmol. 2015;60(5):500–7.
Peckerman A, Saab PG, McCabe PM, Skyler JS, Winters RW, Llabre MM, Schneiderman N. Blood pressure reactivity and perception of pain during the forehead cold pressor test. Psychophysiology. 1991;28(5):485–95.
Drummond PD, Lance JW. Facial flushing and sweating mediated by the sympathetic nervous system. Brain. 1987;110(Pt 3):793–803.
Harris A, Zarfati D, Zalish M, Biller J, Sheets CW, Rechtman E, Migliardi R, Garzozi HJ. Reduced cerebrovascular blood flow velocities and vasoreactivity in open-angle glaucoma. Am J Ophthalmol. 2003;135(2):144–7.
Hosking SL, Harris A, Chung HS, Jonescu-Cuypers CP, Kagemann L, Roff Hilton EJ, Garzozi H. Ocular haemodynamic responses to induced hypercapnia and hyperoxia in glaucoma. Br J Ophthalmol. 2004;88(3):406–11.
Kiyota N, Shiga Y, Suzuki S, Sato M, Takada N, Maekawa S, Omodaka K, Maruyama K, Kunikata H, Nakazawa T. The effect of systemic hyperoxia on optic nerve head blood flow in primary open-angle glaucoma patients. Invest Ophthalmol Vis Sci. 2017;58(7):3181–8.
Iwase A, Suzuki Y, Araie M, Yamamoto T, Abe H, Shirato S, Kuwayama Y, Mishima HK, Shimizu H, Tomita G, et al. The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study. Ophthalmology. 2004;111(9):1641–8.
Chan KKW, Tang F, Tham CCY, Young AL, Cheung CY. Retinal vasculature in glaucoma: a review. BMJ Open Ophthalmol. 2017;1(1): e000032.
Suh MH, Zangwill LM, Manalastas PI, Belghith A, Yarmohammadi A, Medeiros FA, Diniz-Filho A, Saunders LJ, Weinreb RN. Deep retinal layer microvasculature dropout detected by the optical coherence tomography angiography in glaucoma. Ophthalmology. 2016;123(12):2509–18.
Kiyota N, Kunikata H, Shiga Y, Omodaka K, Nakazawa T. Ocular microcirculation measurement with laser speckle flowgraphy and optical coherence tomography angiography in glaucoma. Acta Ophthalmol. 2018;96(4):e485–92.
Acknowledgements
This work was supported by JST COI (grant number JPMJCE1303). The authors thank Mr. Tim Hilts for English editing of the manuscript and Mr. Takehiro Miya for technical support.
Funding
This paper was supported in part by JSPS KAKENHI Grants-in-Aid for Scientific Research (B) (TN; 26293372) and for Exploratory Research (TN; 26670751) and by JST COI (grant number JPMJCE1303). These funders had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication. This study was partly supported by Rohto Pharmaceutical Co., Ltd. This sponsor participated in data collection, provided technical support, and approved the manuscript.
Author information
Authors and Affiliations
Contributions
TN contributed to research design, management of the work, and writing the manuscript. NT and NK contributed to research design, data analysis, and writing the manuscript. HK, MY, TN, and YS contributed to data acquisition, research execution, and data interpretation. HA, MS, TT, TO, and TT contributed to data collection and provided technical support. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study adhered to the tenets of the Declaration of Helsinki, and the protocols were approved by the Clinical Research Ethics Committee of the Tohoku University Graduate School of Medicine (study 2021–1-434). Written informed consent was obtained from the subjects before the CPT was performed. No patient was individually identified in this study.
Consent for publication
All study participants provided written informed consent for the publication of any potentially identifying information or images.
Competing interests
Co-authors HA, MS, and TT are employed by Rohto Pharmaceutical Co., Ltd., a commercial company. Co-authors TO and TT are employed by Casio Computer Co., Ltd., a commercial company. TN receives financial support from Rohto Pharmaceutical Co., Ltd., and provision of study material equipment from Casio Computer Co., Ltd. There are no patents, products in development, or marketed products to declare. The other authors have no potential conflicts of interest associated with this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Takahashi, N., Kiyota, N., Kunikata, H. et al. Vasoreactivity of the optic nerve head, nailfold, and facial skin in response to cold provocation in normal-tension glaucoma patients. BMC Ophthalmol 23, 316 (2023). https://doi.org/10.1186/s12886-023-03059-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-023-03059-0